
Abstract
Purpose:
This study aimed to evaluate the effects of dietary composition, physical activity, and body mass index on gallbladder recovery time following food consumption and to identify alternative scan preparation strategies for patients unable to fast before abdominal ultrasound.
Methods:
A quasi-experimental study involving 26 participants was conducted using four ultrasound sessions under different conditions: consumption of each dietary item with and without moderate physical activity. Gallbladder wall thickness and volume were measured hourly following standardised ultrasound protocols. Measurement reliability was assessed using the intraclass correlation coefficient on 30 randomly selected scans reviewed by two independent observers.
Results:
Recovery time significantly varied among meal types (χ²(2) = 18.42, p < .001), with wholemeal bread yielding the fastest and yogurt the slowest recovery. Physical activity significantly enhanced wall recovery (p = 0.002) but did not affect volume (p = 0.317). Body mass index showed no significant effect. Moderate and excellent intraclass correlation coefficients were achieved for gallbladder wall thickness (0.52) and volume (0.88), respectively.
Conclusion:
Wholemeal bread and postprandial physical activity serve as effective alternatives for ultrasound preparation when assessing gallbladder wall recovery. These findings promote patient-specific ultrasound protocols to improve diagnostic efficiency and comfort.
Background
The gallbladder plays a vital role in the biliary system, facilitating digestion by storing and concentrating bile produced by the liver. 1 Ultrasound is the preferred imaging modality for evaluating gallbladder anatomy and function due to its non-ionising nature, real-time capability, cost-effectiveness, and wide accessibility. Indeed, abdominal and pelvic ultrasound examinations account for approximately 69% of all general practitioner referrals in Central Switzerland between 2004 and 2018, 2 underscoring its central role in clinical practice. Optimal visualisation of the gallbladder requires that it be adequately distended at the time of scanning. This is typically achieved through fasting for at least 6 hours before the examination, during which only clear fluids are allowed. 3 Fasting ensures that the gallbladder reaches a fully distended state, minimising the effects of recent food intake on wall thickness, lumen size, and overall morphology. Such preparation is crucial for accurate assessment, as changes in gallbladder volume and wall thickness are closely associated with various pathological conditions, including cholecystitis, biliary dyskinesia, and gallstone disease. 4 However, adherence to fasting protocols may not always be feasible. Patients with gastrointestinal disorders such as gastritis or duodenal ulcers, diabetics requiring regular meals, or individuals on medication schedules that necessitate food intake may struggle to comply with fasting requirements. 5 In such cases, incomplete gallbladder distention during imaging can compromise diagnostic accuracy, leading to inconclusive results, misinterpretation, or the need for repeat examinations. These challenges not only delay diagnosis and increase healthcare costs but also subject patients to unnecessary anxiety and inconvenience.
Given these limitations, it is clinically valuable to understand the factors influencing gallbladder recovery time following food consumption that is the duration required for the gallbladder to regain adequate distention suitable for diagnostic imaging. Previous studies have demonstrated that recovery time can vary substantially based on dietary composition, the amount and type of fat ingested, and individual physiological differences such as body mass index (BMI) and metabolic rate. 6 Physical activity level may also play a role, as exercise influences gastrointestinal motility and bile flow dynamics. Despite these potential interactions, the combined influence of diet, BMI, and physical activity on gallbladder refilling and recovery time remains underexplored. 7 Therefore, this study aims to evaluate the effects of dietary composition, physical activity, and BMI on gallbladder recovery time after meal ingestion and to identify potential alternative preparation strategies for patients unable to undergo standard fasting before abdominal ultrasound. Establishing evidence-based guidance on optimal recovery intervals and preparation methods may enhance diagnostic reliability, reduce scan rescheduling, and improve patient-centered imaging protocols in clinical practice.
Materials and methods
Participants
This quasi-experimental study was conducted in the ultrasound laboratory of one of the local university. Participants were recruited from undergraduate students of the university using convenience sampling. The study protocol was conducted in accordance with the Declaration of Helsinki and received ethical approval from the university research ethics committee. Written informed consent was obtained from all participants prior to enrollment. A total of 26 healthy university students were included, all of whom had no personal or family history of biliary system disease, food allergies, or medical conditions that would limit physical activity. Participants with the presence of systemic illness, a history of abdominal surgery, or non-compliance with fasting requirements were excluded. Participants were categorised into BMI groups according to the World Health Organization classification. 8
Image acquisition
All participants underwent four scanning sessions on separate days, each with different meal and varying in-between scan activities. The sessions were as follows: Day 1 – two boiled eggs (grade B) without physical activity; Day 2 – two slices of wholemeal bread without physical activity; Day 3 – 400 g natural yogurt (full fat) without physical activity; and Day 4 – 400 g yogurt (full fat) combined with a 1000-step walk over 10 minutes in between the hourly scan. Step counts were verified using the Strava® mobile application to ensure compliance with the activity protocol.
On the scanning day, participants underwent a 6-hour fast with allowance for clear fluids only. Baseline measurements were acquired at the beginning of the ultrasound examination with participants positioned supine and both arms raised to optimise subcostal imaging. Gallbladder wall thickness was measured at the anterior wall, and gallbladder volume was automatically calculated from the maximum longitudinal length obtained in the long-axis plane and the maximum transverse width and anteroposterior diameter obtained in the short-axis plane (Figure 1). Following this initial assessment, participants were instructed to consume the meal supplied by the researcher. Participants underwent hourly ultrasound assessments until either the gallbladder wall thickness decreased below baseline values and the gallbladder volume exceeded baseline measurements, or the sixth hour was reached, whichever occurred first. All ultrasound examinations were performed using an ultrasound scanner (RS8S, Samsung Medison, South Korea) equipped with a CA1-7S convex array transducer operating at 1.0–7.0 MHz. Each participant underwent three measurements by a single operator, from which the mean and median gallbladder wall thickness and volume were derived. To ensure observers’ reliability, gallbladder wall thickness and volume were independently rescanned and measured by a second operator on 30 scan sessions randomly selected from the total dataset of 26 subjects. Both operators were blinded to each other’s results.
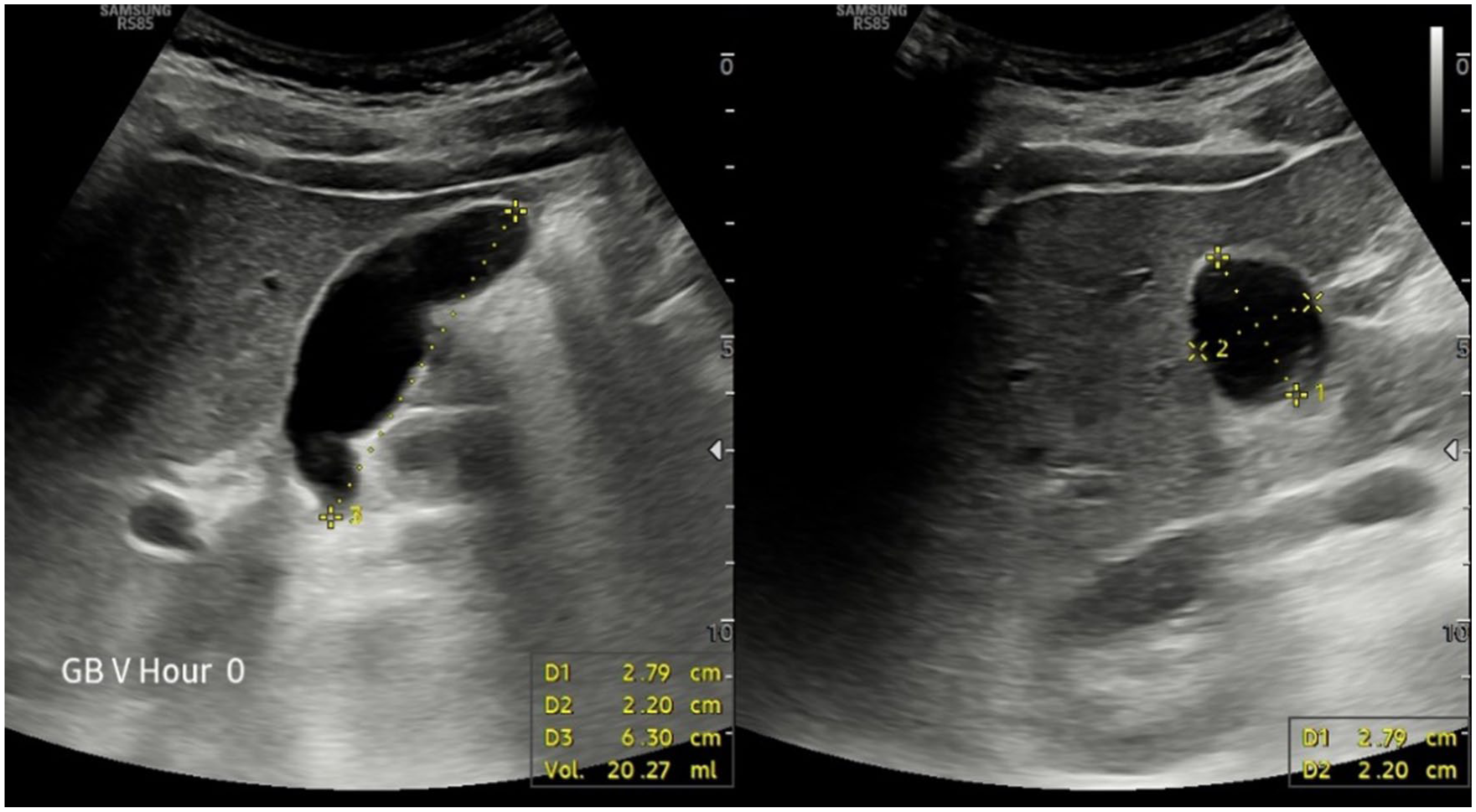
Gallbladder image appearance in the images used to collect the volume measurement (a) longitudinal view to collect the length of the gallbladder. (b) Transverse view to collect the height and the width of the gallbladder.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics version 29 (IBM Corp., Armonk, NY, USA). Descriptive statistics were expressed as means and standard deviations. Data normality was assessed using the Shapiro–Wilk test. The Friedman test was used to compare gallbladder recovery times among the three dietary conditions, followed by the Wilcoxon signed-rank post hoc test for pairwise comparisons. The Wilcoxon signed-rank test was also used to compare recovery times between minimal energy and physical activity conditions. The intraclass correlation coefficient (ICC) was calculated to determine inter-observer agreement. Reliability was interpreted using the following thresholds: poor (<0.5), moderate (0.5–0.75), good (0.75–0.9), and excellent (>0.9). A General Linear Model (GLM) analysis was conducted to examine the combined effects of dietary type, activity level, and BMI on gallbladder recovery time. Statistical significance was set at p < 0.05.
Results
Demographic and baseline characteristics
A total of 26 healthy undergraduate students (age range = 23–24 years), comprising 8 males and 18 females, were assessed. The BMI distribution was as follows: underweight (n = 5), normal weight (n = 11), overweight (n = 5), and obese (n = 5).
Effect of different dietary components on gallbladder recovery time
For gallbladder wall recovery, the Friedman test indicated a statistically significant difference in the time required for the gallbladder wall to return to its distended state across the three meal types, χ²(2) = 13.136, p = 0.001. This finding suggests that at least one meal produced a notably different recovery time compared to the others.
Post hoc analysis using the Wilcoxon signed-rank test was conducted to identify which meal pairs differed significantly. The greatest difference was observed between yogurt (mean = 4.5 hours) and wholemeal bread (mean = 3.5 hours) (Z = −3.402, p < 0.001). A significant difference was also found between boiled eggs (mean = 4 hours) and wholemeal bread (Z = −2.185, p = 0.029). However, no significant difference was observed between boiled eggs and yogurt (Z = −1.893, p = 0.058) (Figure 2).
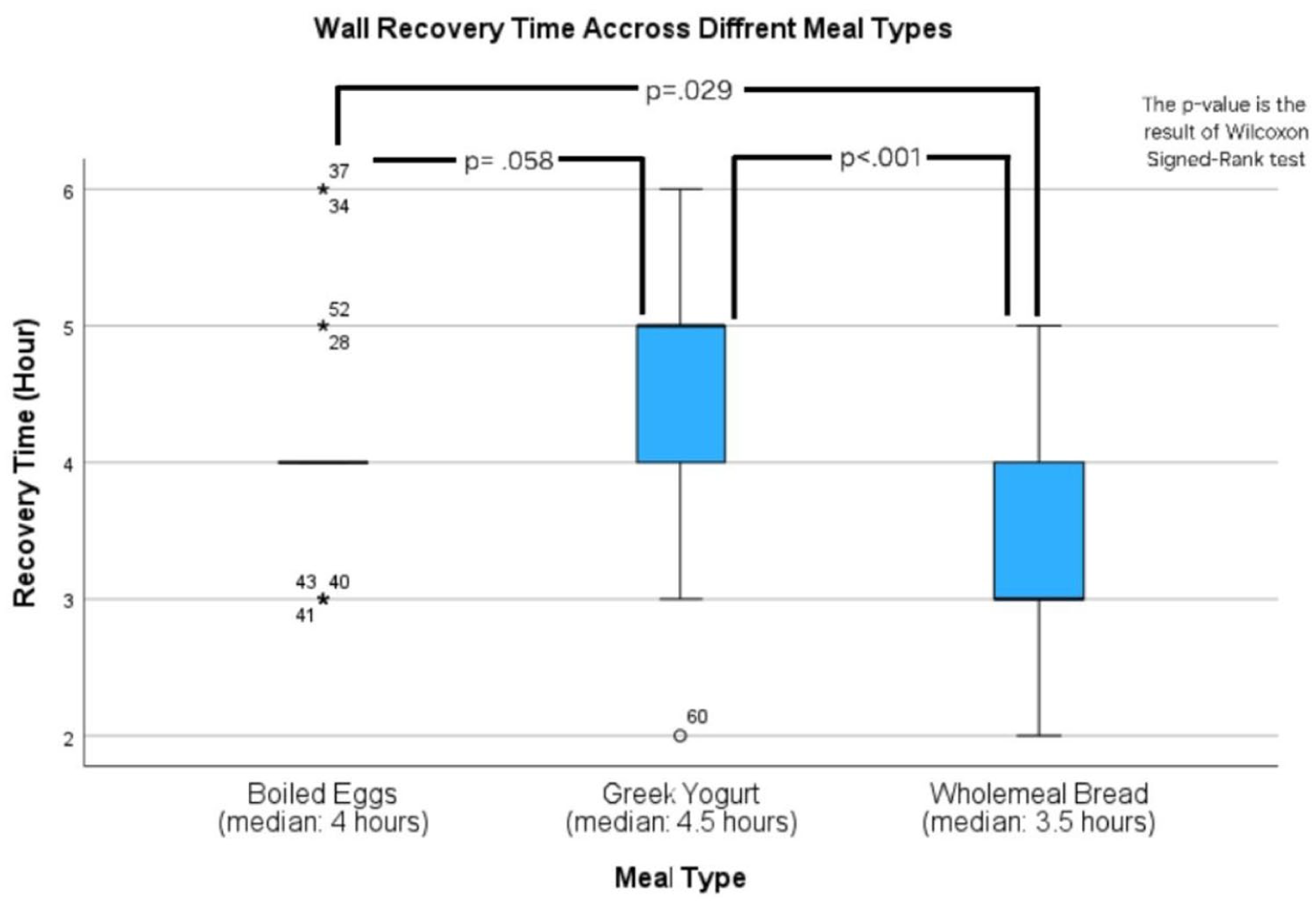
Box plot comparing the wall recovery time taken following three meal types: boiled eggs, Greek yogurt, and wholemeal bread.
The Friedman test demonstrated a statistically significant variation in gallbladder volume recovery time across meals, χ2(2) = 7.063, p = 0.029. A post hoc test showed a significant difference between yogurt (mean = 4.3 hours) and wholemeal bread (mean = 4 hours) (Z = −2.206, p = 0.027), and the other two pairs – boiled eggs (mean = 4.2 hours) and wholemeal bread (Z = −1.598, p = 0.110) and boiled eggs and Greek yogurt (Z = −0.864, p = 0.387) – both show no differences (Figure 3).
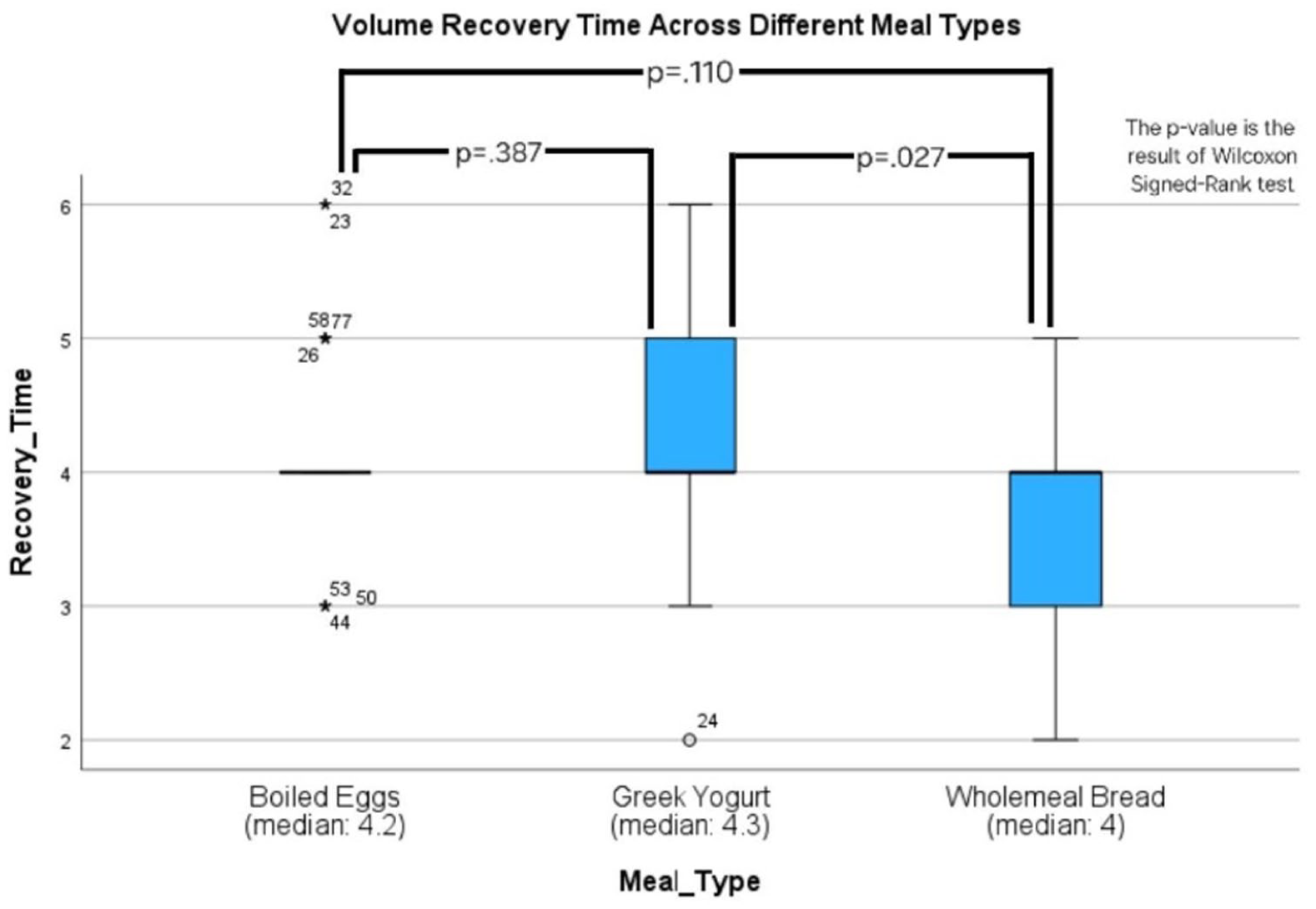
Box plot comparing the volume recovery time taken following three meal types: boiled eggs, Greek yogurt, and wholemeal bread.
Assessing the impact of physical activity on gallbladder recovery after food consumption
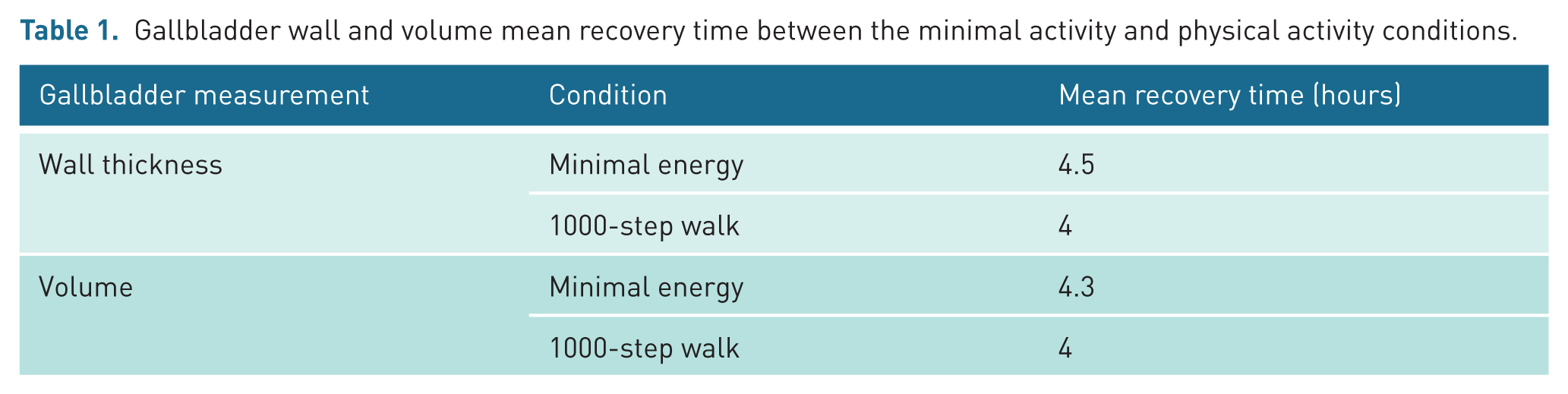
Table 1 shows the gallbladder wall and volume mean recovery time between minimal energy and physical activity (1000-step walk in 10 minutes hourly). The Wilcoxon Signed-Rank test was used to compare gallbladder recovery time, measured by wall thickness and volume separately, between the physical activity and minimal activity conditions. For the gallbladder wall, the test showed that physical activity showed a statistically significant difference in gallbladder wall recovery (Z = −2.751, p = 0.006). However, the gallbladder volume did not elicit a statistically significant difference where Z = −1.430, p = 0.153.
Gallbladder wall and volume mean recovery time between the minimal activity and physical activity conditions.
Comparing the impact of different dietary component, physical activity, and BMI variation
GLM revealed that both physical activity level and dietary component significantly influenced gallbladder wall recovery time (Activity: F(1,99) = 4.153, p = 0.044, η² = 0.040; Meal: F(1,99) = 4.768, p = 0.031, η² = 0.046). Participants engaging in minimal physical activity while consuming yogurt exhibited significantly longer recovery times compared to those who performed physical activity (p = 0.003, mean difference = 0.788). Yogurt led to the most extended recovery duration (mean = 4.269, Std = 0.132), followed by boiled eggs (mean = 4.038, Std = 0.187), with wholemeal bread resulting in the shortest recovery time (mean = 3.462, Std = 0.187). Among dietary components, yogurt resulted in longer recovery time compared to wholemeal bread (p = 0.002, mean difference = 0.808), while no significant differences were observed between yogurt and boiled eggs. The BMI covariate did not significantly affect gallbladder wall recovery time (p = 0.137), and no interaction effect was found between activity and meal type. The overall model explained 16% of the variance in recovery time (adjusted R² = 0.126), supporting the influence of both activity level and dietary component on gallbladder function.
For gallbladder volume recovery, GLM analysis revealed that meal type significantly influenced the recovery time (Meal: F(1,99) = 6.989, p = 0.010, η² = 0.066), representing a moderate effect size, while physical activity level did not yield a significant effect (Activity: F(1,99) = 0.280, p = 0.598, η² = 0.003), indicating a negligible effect size. Among dietary components, yogurt led to the most extended recovery duration (mean = 4.250, Std = 0.109), followed by boiled eggs (mean = 4.192, Std = 0.154), with wholemeal bread resulting in the shortest recovery time (mean = 3.615, Std = 0.154). Yogurt resulted in significantly longer gallbladder volume recovery time compared to wholemeal bread (p = 0.002, mean difference = 0.808), while no significant differences were found between yogurt and boiled eggs. No interaction effect was detected between meal type and activity level, and BMI did not significantly influence gallbladder volume recovery (p = 0.381). The overall yogurt counted for approximately 12% of the variance in recovery time (adjusted R² = 0.081), supporting the role of dietary composition, particularly yogurt versus wholemeal bread, in modulating gallbladder volume recovery.
Reproducibility of gallbladder wall and volume measurements
For the gallbladder wall, a moderate level of agreement was discovered, where the average ICC was 0.54, with a 95% confidence range of .238–.751 (F(29,29) = 3.612, p < 0.001). As for gallbladder volume, an excellent level of agreement was discovered with the average ICC was 0.88, with a 95% confidence range of 0.765–0.941 (F(29,29) = 15.347, p < 0.001).
Discussion
This research aimed to determine which meal type, wholemeal bread, boiled eggs, and yogurt, promotes the quickest gallbladder recovery, as determined by gallbladder wall thickness and volume. Our results showed that dietary composition and physical activity both showed significant associations with gallbladder recovery time following food intake. Notable differences in recovery across the assigned test meals were also observed, with some foods requiring longer recovery periods than others. Although BMI did not contribute significantly to these variations, the influence of dietary type and post-meal physical activity highlights the need to consider these factors when preparing patients for abdominal ultrasound examinations. Despite the operator-dependent nature of ultrasound, the consistency of the measurements obtained in this study supports the reliability of the methodological approach.
Gallbladder wall thickening is a common finding that can be associated with a wide range of benign and malignant conditions, making accurate interpretation essential for appropriate clinical management. Because a substantial proportion of gallbladder carcinoma cases initially present with wall thickening, early and precise risk categorisation is crucial. Ultrasound remains the primary imaging modality for evaluating suspected gallbladder disease, as it provides excellent visualisation of the gallbladder wall and is highly effective for measuring wall thickness. 9 Therefore, establishing which of the three meal types of wholemeal bread, boiled eggs, or yogurt optimally accelerates gallbladder recovery, based on wall thickness and volume parameters, is necessary for understanding postprandial gallbladder dynamics.
Studies have demonstrated that dietary fat is the strongest stimulus for cholecystokinin (CCK) release, which subsequently promotes gallbladder contraction and delays refilling, while protein can stimulate CCK release to a lesser extent, and carbohydrates generally have a minimal stimulatory effect on gallbladder motility. 10 In the present study, differences in gallbladder wall thickness and volume recovery time were observed across the three meal types, with yogurt eliciting the longest recovery time and wholemeal bread the shortest. These variations are likely attributable to differences in dietary fat content and their physiological effects on gallbladder motility. According to the nutritional composition of the diet, the yogurt used in the study contained 3.6 g of fat per 100 mL, grade B eggs provided approximately 5.3 g of fat per egg, and wholemeal bread contributed less than 1.5 g of fat per slice. As wholemeal bread is predominantly carbohydrate-based, with modest protein and minimal fat, this nutritional profile explains its association with the shortest recovery time. This finding is consistent with previous studies demonstrating that higher fat meals prolong gallbladder contraction through sustained CCK release, whereas lower fat meals permit earlier gallbladder refilling.11,12 The significant difference between eggs, which are protein- and fat-dominant, and wholemeal bread is also in line with reports indicating that protein- and fat-containing foods trigger greater gallbladder contraction than high-fibre, low-fat carbohydrate sources. 13 By contrast, eggs are protein- and fat-dominant, while yogurt represents a more balanced macronutrient mix. The absence of a clear difference between the yogurt and egg meals aligns with studies suggesting that meals with relatively similar fat-to-protein ratios may produce comparable CCK-mediated gallbladder motility. 14 Thus, although yogurt was linked to the longest recovery time, the difference compared with eggs was not statistically significant. Importantly, although the meals in the present study were not designed as high fat challenge meals, the findings demonstrate that even moderate differences in fat content can influence postprandial gallbladder kinetics. However, not all studies align; some authors have reported comparable gallbladder responses following protein-rich meals, suggesting that non-lipid macronutrients may also elicit meaningful CCK-mediated effects. 15 Such inconsistencies in the literature may be attributable to variations in caloric density, meal composition, viscosity, and gastric emptying rates, all of which influence hormonal release and gallbladder motility. 16 Collectively, the present findings reinforce the importance of standardising pre-scan dietary instructions in both research and clinical settings, as variations in meal type can introduce significant physiological variability into gallbladder measurements. 17
The differing effects of physical activity on gallbladder wall thickness and volume recovery suggest that these two parameters may respond to postprandial physiology through distinct mechanisms. The significant improvement in wall recovery following physical activity is consistent with evidence that light to moderate movement enhances gastrointestinal motility, accelerates hormonal clearance, and improves splanchnic circulation, which collectively facilitate faster relaxation of the gallbladder wall. 18 In contrast, the absence of a corresponding effect on gallbladder volume aligns with a study indicating that volume refilling is primarily driven by ongoing CCK decline and hepatic bile secretion rate processes that may be less sensitive to short-term physical activity. 7 A possible explanation is that activity may influence muscular relaxation of the wall more rapidly than it alters the actual rate of bile replenishment, resulting in early wall recovery without measurable changes in total volume.
The combined GLM findings indicate that both dietary composition and physical activity exert meaningful but distinct influences on gallbladder recovery, with meal type consistently emerging as the stronger determinant. BMI had no significant effect on recovery frequency in either model, indicating that short-term gallbladder responsiveness may be driven more by immediate meals and behavioral inputs than by baseline anthropometric variance. This is in contrast to previous research that linked obesity to reduced gallbladder motility, 19 and it might be due to sample homogeneity or the use of BMI as a covariate rather than an independent variable. The analysis considered BMI as a covariate, which may have statistically controlled for its significance, resulting in an underestimation of its real physiological impact on gallbladder motility. Another possible reason for the differences in BMI is that it may not always accurately represent a person’s real body fat or fat distribution. The sample may have had similar BMI ranges or body types, making it challenging to spot apparent variation in gallbladder function. Recent research suggests that novel metrics, such as relative fat mass, may be more effective in demonstrating how body fat affects gallbladder health.20,21
For patients who can’t fast before an abdominal ultrasound, such as those with metabolic disorders, strict medication schedule, or vulnerable groups like children and older adults, this research provides useful alternatives to improve the quality of gallbladder imaging by allowing patients to eat wholemeal bread and take part in moderate activity (like walking about 1000 steps in 10 minutes per hour) may still produce clear and accurate results. These habits helped speed up wall recovery without noticeably affecting image quality. In fact, many standard gallbladder scans focus on wall assessment, and with proper technique, wall thickness can still be evaluated reliably even if the patient has eaten, especially when factors like pseudothickening are considered. 22
The inter-observer reliability of gallbladder measurements obtained using the Samsung RS85 Prestige system demonstrated moderate to excellent agreement between the two observers. The moderate reliability observed for gallbladder wall thickness is consistent with previous ultrasound research showing that thin, highly compressible structures frequently yield lower reproducibility due to minor variations in probe pressure and insonation angle. 23 In contrast, gallbladder volume demonstrated excellent agreement, reflecting the advantage of assessing larger, well-defined anatomical boundaries, which are less sensitive to operator-dependent variability. These findings align with prior studies reporting similarly higher ICC values to assess the consistency of gallbladder polyp measurements obtained through transabdominal ultrasound, both when repeated by the same observer and when performed by different observers, as well as to identify factors that may influence this measurement reliability, particularly when using high-performance scanners such as the Samsung RS85. 24 The reliability demonstrated in our study therefore supports the robustness of the measurement protocol and reinforces the expected pattern in abdominal ultrasound reliability literature, where volumetric indices consistently outperform linear wall measurements in reproducibility.
This study has several limitations. First, the participants were limited to young, healthy adults, which may restrict the generalisability of the findings to other age groups or individuals with underlying medical conditions. Second, the relatively small sample size may have reduced the statistical power of the study. In addition, gallbladder volume was calculated using an ellipsoid formula derived from manually measured gallbladder length, width, and anteroposterior dimensions, which may not fully represent the actual gallbladder volume. Future studies should include a larger sample size and a wider age range and employ true volumetric gallbladder measurement techniques to improve accuracy and external validity.
Conclusion
This study demonstrates that patients require only approximately 3.5 hours of fasting prior to gallbladder ultrasound when consuming wholemeal bread, which is notably shorter than the standard recommendation of 6 hours. The reduced fasting requirement reflects the low-fat content and carbohydrate-dominant profile of wholemeal bread, which facilitates earlier gallbladder recovery. Furthermore, combining wholemeal bread intake with physical activity may potentially shorten the fasting duration even further. These findings highlight a practical approach to patient preparation that improves comfort and compliance without compromising diagnostic efficiency, thereby contributing to enhanced patient care in routine ultrasound practice.
Footnotes
Acknowledgements
Not applicable.
Ethical considerations
Ethics Committee of Universiti Teknologi MARA, Faculty of Health Sciences, Universiti Teknologi MARA, Selangor, Malaysia (MECID No: FERC/FSK/MR/2024/00254).
Contributors
M.M., S.S.L., and A.I.A. contributed to conception and design. M.M. and S.S.L. contributed to acquisition of data. M.M., S.S.L., and A.I.A. contributed to analysis and interpretation. S.S.L. and A.I.A. contributed to drafting the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Not applicable.