
Abstract
Ovarian torsion is a surgical emergency in which twisting of the ovarian vascular pedicle leads to ischaemia. Although an uncommon diagnosis in prepubescent girls, prompt recognition of this condition is essential in order to prevent ovarian necrosis, which can have long-term consequences in terms of fertility. Transabdominal ultrasound is the recommended imaging modality for diagnosing ovarian torsion; however, given the limited availability of paediatric-trained sonographers, patients may not obtain the necessary imaging in a timely manner. Point-of-care ultrasound performed by emergency department personnel has emerged as a useful adjunct to clinical examination and one that can help expedite specialist involvement. We describe two cases of prepubescent ovarian torsion presenting to our Paediatric Emergency Department, where point-of-care ultrasound played a key role in diagnosis and expediting definitive surgical management.
Introduction
Ovarian torsion occurs due to the twisting of the ovarian vascular pedicle, causing ischaemia to the ovary and/or the fallopian tube (adnexal torsion). Although it is an uncommon and often unsuspected cause for acute lower abdominal pain in prepubescent female patients, ovarian torsion requires prompt recognition and timely management. We describe two cases of prepubescent girls presenting to our Paediatric Emergency Department (PED), where both were identified to have ovarian torsion using point-of-care ultrasound (POCUS).
Case 1
A 7-year-old girl was brought to the PED by her mother after complaining of right iliac fossa pain for approximately 12 hours. The pain was described as stabbing and colicky in nature, severe enough to cause her to buckle over. Her parents reported that she appeared pale during episodes of pain. She had one episode of vomiting. There was no history of fever, diarrhoea, or urinary symptoms. She had no significant past medical or surgical history, and she had not yet attained menarche. On examination, she was haemodynamically normal but appeared slightly pale and lethargic. Abdominal examination revealed a soft, non-distended abdomen with guarding in the suprapubic region and right iliac fossa. There was no rebound tenderness, and Rovsing’s sign was negative. Urinalysis was negative. She was given analgesia and observed in PED for 2 hours during which time her pain completely resolved, and she tolerated oral intake. She was subsequently discharged with safety-netting advice. She re-presented to PED the following day with worsening right-sided abdominal pain and three episodes of vomiting. On examination, she had right iliac fossa tenderness without rebound tenderness. Blood tests were undertaken with the following results: Haemoglobin: 137 g/L; white cell count: 12.83 × 109; neutrophils: 9.79 × 109; platelets: 486 × 109/L; CRP: <0.6 mg/L; ESR: 2 mm/h.
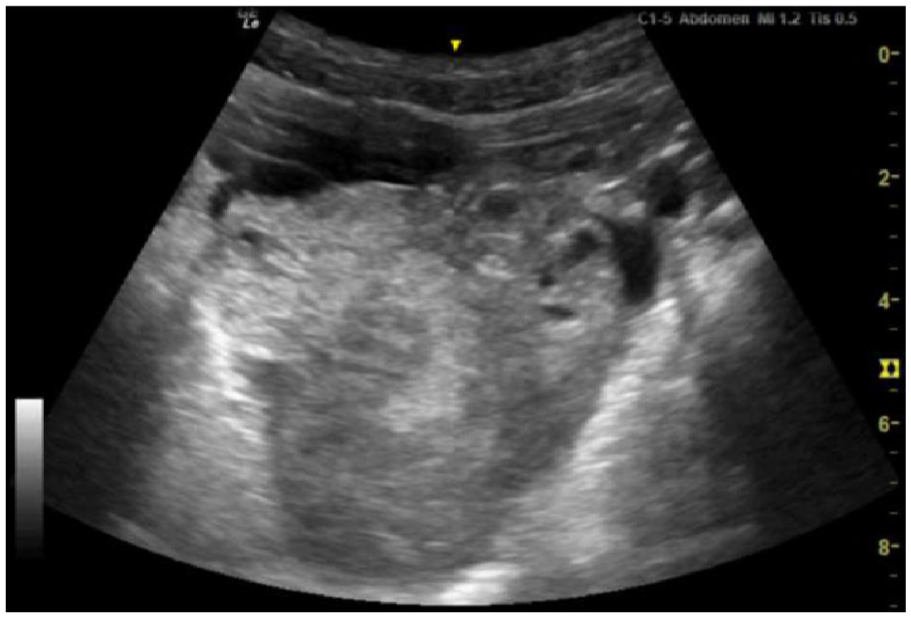
Two of the authors undertook POCUS as demonstrated in Figures 1 to 4. This demonstrated a moderate amount of free fluid in the pelvis. The urinary bladder was displaced and partially obscured by the right ovary, which was unusually located in the midline and markedly enlarged, measuring approximately 5.5 cm × 3.7 cm. The ovarian follicles were prominent and peripherally displaced, with the largest follicle measuring 0.9 cm. Colour Doppler flow could not be appreciated within the right ovary; however, no pedicle was visualised to assess for a whirlpool sign. The left ovary was significantly smaller, measuring 1.56 cm × 1.3 cm and relatively homogeneous in echotexture with only tiny follicles visible and with preserved colour flow on Doppler. The right lower quadrant appeared unremarkable aside from approximately five lymph nodes, all <2 cm in diameter, with normal architecture. The appendix was not visualised; however, there were no secondary signs of appendicitis, and regional bowel loops were unremarkable. The POCUS findings were consistent with acute right ovarian torsion.
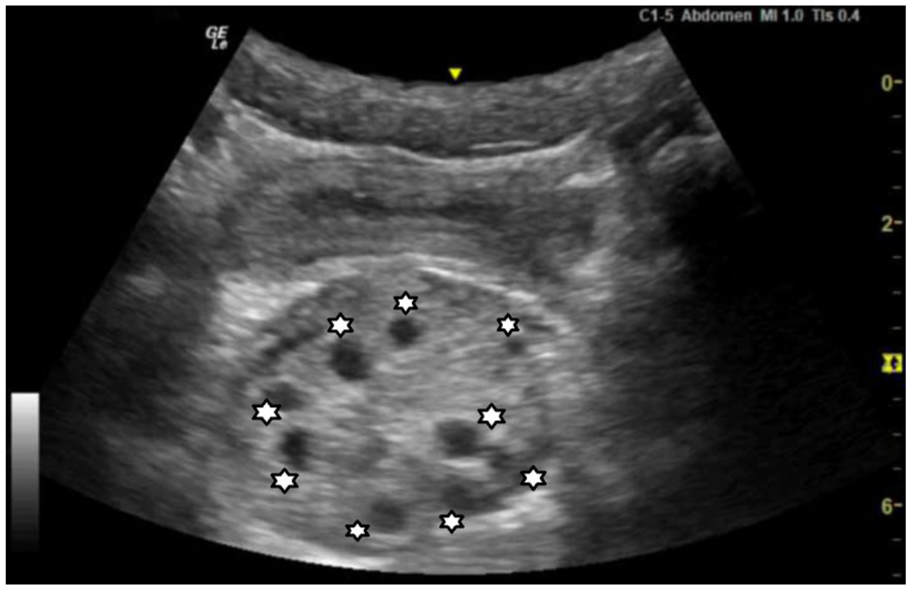
POCUS image of the mid pelvis using the curvilinear 5–12 MHz probe in the transverse orientation.
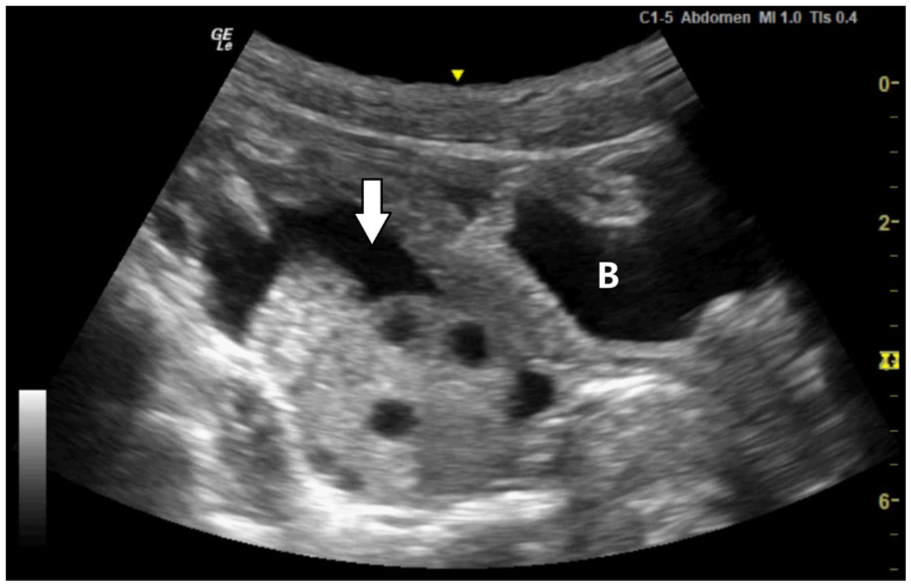
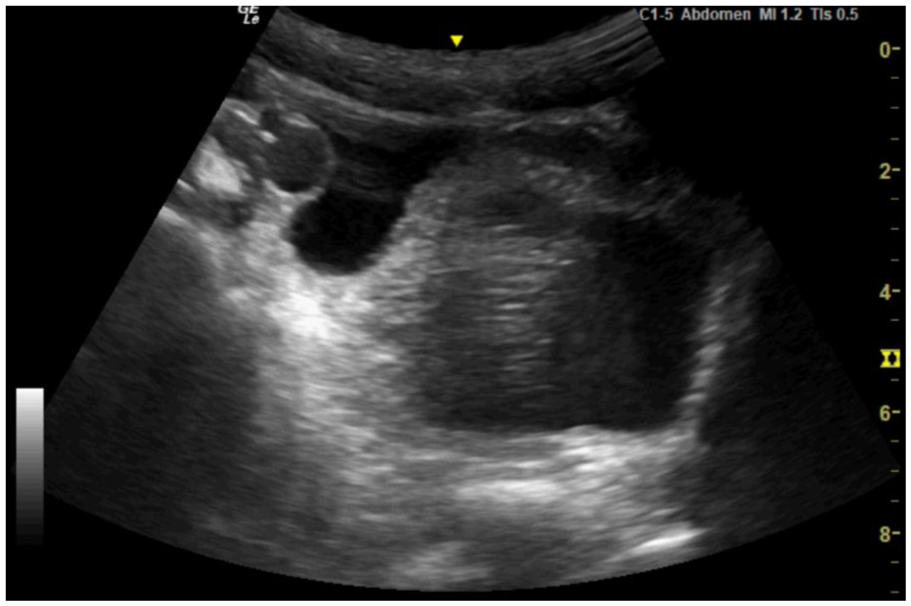
POCUS image of the pelvis using the curvilinear 5–12 MHz probe in the longitudinal orientation.
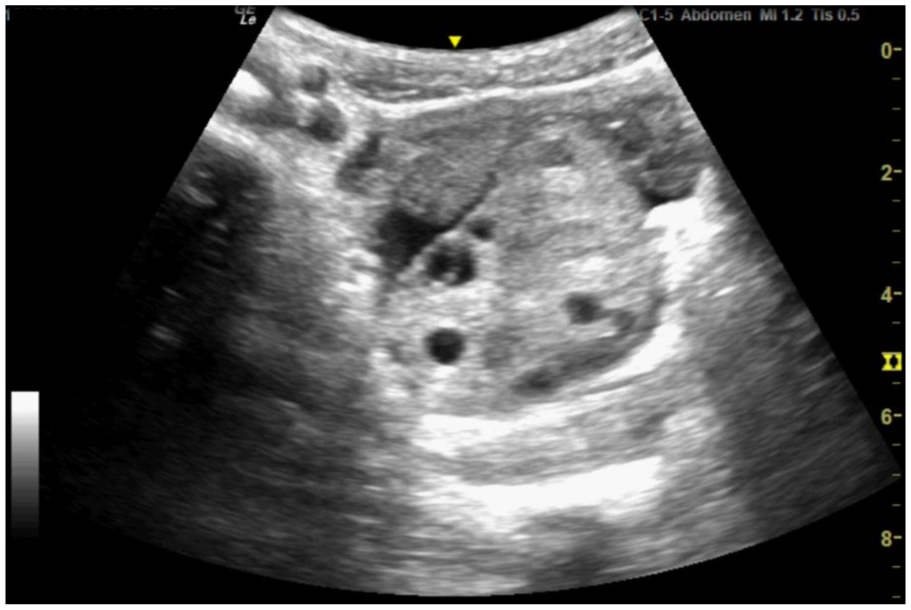
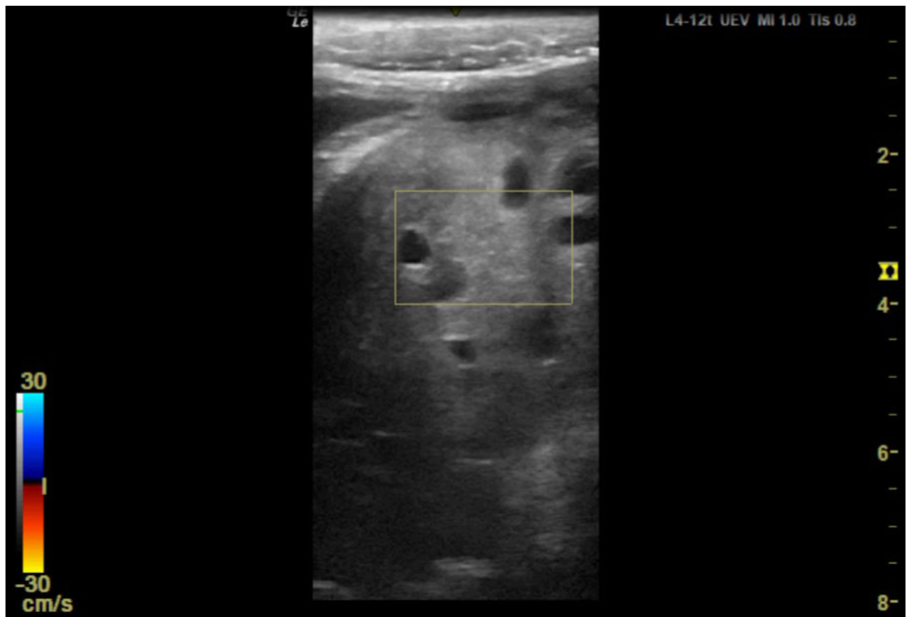
POCUS image of the lower pelvis using the curvilinear 5–12 MHz probe in the transverse orientation.
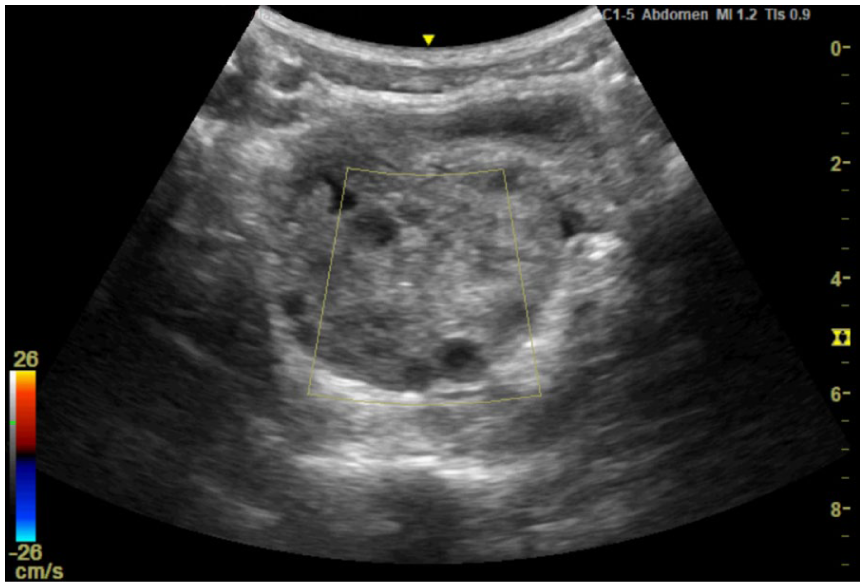
POCUS image of the lower pelvis using the curvilinear 5–12 MHz probe in the transverse orientation, which shows an enlarged ovary with absence of internal flow on colour Doppler.
Radiology performed an ultrasound, which confirmed acute torsion of the right ovary with an enlarged volume of 27.5 mL and a normal left ovary (volume: 6.7 mL).
The child was transferred to the tertiary paediatric surgical centre, where she underwent laparoscopic evaluation, revealing adnexal torsion on the right side. This was un-torted with visible improvement in the colour of the tube and ovary. Her tumour markers (alpha-fetoprotein and beta HCG) were normal. She was discharged home the following day with a plan for a repeat ultrasound in 6 weeks to assess the recoverability of the ovary.
Case 2
An 8-year-old girl was brought to the PED after complaining of progressive right-sided abdominal pain in the preceding 48 hours. She had multiple episodes of non-bilious vomiting but denied fever, diarrhoea, or urinary symptoms. Her past medical history was unremarkable. She had not yet attained menarche. On examination, her abdomen was soft, non-distended, with tenderness in the right iliac fossa without guarding. There was no rebound tenderness, and Rovsing’s sign was negative. Urinalysis was negative.
One of the authors undertook a POCUS (see Figures 5–8), which demonstrated a moderate to large amount of free fluid in the pelvis with none elsewhere. A very large heterogeneous mass was evident in the right lower quadrant, with the presence of circular anechoic regions suspicious for ovarian follicles. The left ovary was visualised to be small with a homogeneous echotexture in comparison and appeared normal, other than the presence of some large follicles. High-frequency POCUS images provided greater clarity of this structure; colour Doppler did not demonstrate any internal flow. Based on the size, position, morphology, Doppler findings, and comparison with the contralateral ovary, an ovarian torsion was suspected.
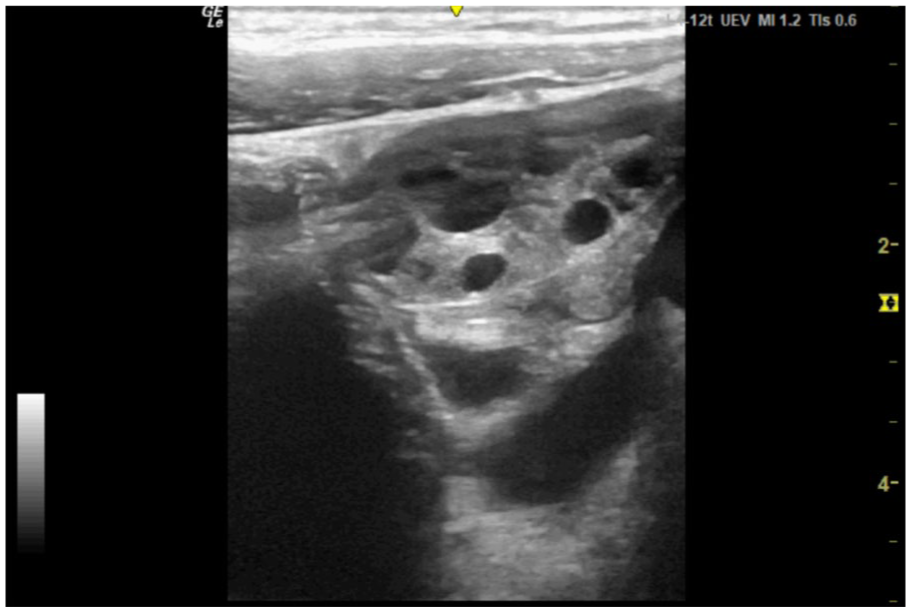
POCUS image of the lower pelvis using the curvilinear 5–12 MHz probe in the transverse orientation, which shows a very large heterogeneous mass with the suggestion of small follicles within its periphery.
POCUS image of the lower pelvis using the curvilinear 5–12 MHz probe in the transverse orientation, showing a moderate amount of free fluid.
POCUS image of the right lower pelvis using the high-frequency linear 12–16 MHz probe.
POCUS image of the left lower pelvis using the high-frequency linear 12–16 MHz probe.
The child was taken to the theatre where she had right ovarian torsion of 520° associated with a large right haemorrhagic ovarian cyst, likely to be the lead point for torsion. Her left ovary appeared healthy. The right ovary was detorted and appeared to be salvageable. She will be followed up with an outpatient ultrasound scan to assess the recovery of the ovary and to see whether the haemorrhagic cyst has resolved.
Discussion
Often overlooked as a cause for abdominal pain in prepubescent females, ovarian torsion remains an important diagnosis to exclude, given the impact on the viability of the affected ovary and hence the child’s fertility.
In the paediatric population, ovarian torsion has an estimated incidence of 5 per 100,000 with an average age of 14.5 years, although some studies suggested a lower median age. 1 One study found that 4% of females presenting to the PED with acute abdominal pain were diagnosed with ovarian torsion. 2 Another retrospective review demonstrated a bimodal age distribution with the largest number of cases (16/97) in the less than 1-year age group and the other peak at 12 years. 3 Ovarian torsion has been described in infants as young as 6 weeks, where the presenting symptoms may be non-specific. 4 Owing to the non-specific presentation of ovarian torsion, delayed diagnosis has been reported in up to 30% of cases. 5
Management options include ovarian detorsion, detorsion with oophoropexy, and oophorectomy. Traditionally, oophorectomy was often performed when the ovary appeared ischaemic or haemorrhagic; however, there is evidence that supports ovarian preservation in the paediatric population due to the ovary’s reparative capacity. 6 The precise duration of vascular compromise required to cause irreversible damage remains uncertain, but the ovary’s dual blood supply may provide some protection to vascular injury. 6 The ovary is supplied both by the ovarian artery, which reaches the ovary via the lateral infundibulo-pelvic ligament (suspensory ligament of the ovary), and the ovarian branch of the uterine artery, which reaches the ovary from the medial side via the ovarian ligament. This dual supply from different directions may explain the increased recoverability of the ovary when compared to the testis in testicular torsion. Ovarian viability decreases with increasing time from symptom onset to surgical detorsion, which emphasises the importance of timely diagnosis and early intervention to salvage the organ. 6
For paediatric ovarian torsion, clinical signs and laboratory findings have been demonstrated to not be sufficiently reliable in making or excluding the diagnosis. 7 Transabdominal ultrasound is the imaging modality of choice for patients with suspected adnexal/ovarian torsion. 8 Abdominal and pelvic POCUS is performed similarly to formal radiology scanning, predominantly using the curvilinear 5–12 MHz probe, with greater detail if necessary, being identified using the high-frequency 12–18 MHz linear probe. Before undertaking standardised abdominal views at the right and left upper quadrants looking for free fluid, the pelvis is assessed in a systematic manner in both longitudinal and transverse planes using gentle pressure. The ovaries should be appraised for their size, echotexture, and follicle distribution before using colour Doppler. Doppler settings should be optimised for low velocity flow by using a low pulse-repetition frequency (PRF), a low wall filter, and a small sample gate to maximise sensitivity to reduced venous and arterial perfusion. This is particularly important as normal arterial or venous flow does not exclude torsion, and absent or reduced venous flow may be the earliest haemodynamic abnormality.9,10
Multiple sonographic findings have been studied, and although there are a number of suggestive findings, none alone are pathognomonic. The most reliable are as follows: abnormal position of the effected ovary, for example, in the midline, in the pouch of Douglas or superior to the uterus, enlargement of the affected ovary (>4 cm or more), the “string of pearls sign” whereby stromal oedema and venous congestion may displace fluid into peripheral follicles, the follicular ring sign referring to perifollicular hyper-echoic prominent margins 1 to 2 mm in thickness observed all around the small antral follicles of the torted ovary and oedema of the ovary with heterogeneous parenchyma and increased echogenicity of the stroma.9 –11 As highlighted above, reduced flow on colour Doppler due to impaired arterial or venous flow may be present, but preserved flow does not exclude torsion. Another sonographic sign that may be evident is the “Whirlpool sign,” which represents the coiled vascular pedicle and appears as a para-ovarian structure with multiple concentric rings often alternating in echogenicity, typically located between the uterine fundus and ovary. 9 This can be difficult to identify and was not evident during the two cases we describe. Other non-specific signs include the presence of pelvic free fluid. Ultrasound may also show ovarian conditions predisposing to torsion, such as ovarian cysts/masses. The “double bladder” sign is observed when a midline ovarian cyst represents what appears to be a second bladder on ultrasound. This does not diagnose torsion per se, but in a clinical context may represent a clue pointing towards torsion, for example, in association with pelvic pain. 5 In a reported case series, medialization of the torted ovary was present in 34% of cases. 12
In their systematic review and meta-analysis, Wattar et al. 13 found that ultrasound has a sensitivity of 0.79 (95% confidence interval (CI) = 0.63–0.92) and specificity of 0.76 (95% CI = 0.54–0.93) for the detection of adnexal torsion. With the addition of colour Doppler findings, there was a slight but non-significant improvement in sensitivity (0.80, 95% CI = 0.67–0.93) and specificity (0.88, 95% CI = 0.72–1.00). From the same review, but a smaller number of studies, magnetic resonance imaging (MRI) showed a sensitivity of 0.81 (95% CI = 0.63–0.91) and specificity of 0.91 (95% CI = 0.80–0.96). CT scanning showed similar diagnostic accuracy, but from a small number of studies, and a meta-analysis was not possible.
Garde et al. 14 looked at the diagnostic accuracy of individual ultrasonographic signs. An adnexal mass and presence of pelvic fluid showed poor diagnostic accuracy, while the presence of ovarian oedema, the whirlpool sign, and decreased or absent ovarian colour Doppler flow have good specificity but moderate sensitivity for detecting adnexal torsion. In a separate review, the whirlpool sign showed a sensitivity of 0.82 (95% CI = 0.78–0.86) and a pooled specificity of 0.81 (95% CI = 0.70–0.90). 15 The presence of Doppler arterial flow does not rule out torsion 16 and has low sensitivity but high specificity. 17 Preserved flow on colour Doppler may be a result of intermittent torsion or collateral blood supply. Asymmetric sizes of the ovaries may indicate the presence of torsion; an ovarian volume ratio of >2.5 has been shown to have a high sensitivity and specificity for torsion in pre-menarchal girls. 18 The finding of an asymmetrically enlarged ovary is of particular importance in this age group because many causes of an enlarged ovary in adults (endometrioma, tuboovarian abscess, ectopic pregnancy) are uncommon in children. Unilateral ovarian enlargement in the setting of acute pelvic pain should always prompt concern for ovarian torsion in girls.
A 7-year retrospective case–control study sought to evaluate the predictive value of individual sonographic signs and found that ovarian size alone could not be used to rule out torsion, with ovarian torsion being present in ovaries that were less than 20 mL in volume. They too highlighted the best predictor of ovarian torsion as volume ratio (relative to the unaffected ovary) with a value of >15 showing the strongest association with surgically confirmed torsion. 19
The literature regarding POCUS for adnexal torsion in paediatric patients is largely confined to case reports and case series.20,21 In one prospective adult study, transvaginal POCUS identified both ovaries in approximately 80% of patients. 22 While radiology-performed ultrasound has a 97%–98% visualisation rate for the ovaries, 23 this demonstrates that POCUS for ovarian torsion is feasible in the emergency department. This is important as access to paediatric ultrasound is limited, particularly out of hours. CT scanning is readily available but has similar diagnostic accuracy while irradiating the patient while MRI scanning has limited availability, is expensive, time-consuming, and formal reports can be difficult to obtain. POCUS on the other hand is quick, easily repeatable as symptoms develop, and well tolerated by paediatric patients. POCUS examinations for both cases were performed by one of the authors, a Consultant in Paediatric Emergency Medicine with more than 7 years of ultrasound experience, including postgraduate qualifications in Medical Ultrasound. All scans were conducted according to a defined departmental protocol.
In both of our cases, POCUS, performed while the child was in the PED, played a key role in the recognition of ovarian torsion, which enabled prompt, definitive management and ensured positive outcomes for each. From these cases, the authors have taken away that clinical context and sonographic features taken together can help guide decision-making in this time-critical condition, and that the only thing needed to consider ovarian torsion as a potential differential diagnosis is the presence of an ovary.
Conclusion
Prepubescent ovarian torsion is uncommon, challenging to diagnose clinically, and may be easily overlooked. This mini-case series supports the potential role that POCUS may play as an adjunct imaging tool, which can be valuable in helping to identify ovarian torsion, even in prepubescent girls. Further studies would be helpful to evaluate the role of POCUS for this purpose in the wider clinical context.
Footnotes
Acknowledgements
None.
Ethical considerations and consent statement
Informed consent was provided by those who are authorised to do so for all images used. No patient identifiable information was visible.
No specific approval from the NHS Research Ethics Committee was deemed to be required for the publication of this article, as it related to routine patient care only.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
N/A.
Permission from patient(s) or subject(s) obtained in writing for publishing their case report
Consent was obtained for the use of images in this manuscript from those authorised to provide it, in this case, given that the subjects were minors, this was from those with parental responsibility.