
Abstract
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is manifested by physical symptoms of breathlessness, fatigue and cough affecting sufferers in their activities of daily living particularly at times of exacerbation. Mental health problems co-occur in people with a diagnosis of COPD. Depression and anxiety have been described as the most common yet least-treated co-morbidities 1 and significantly impact on quality of life. 2 The prevalence of depression has been found to be as great as 42% and that of anxiety as high as 19% in those with stable COPD 1 and is high in comparison with other long-term conditions. 3 Additionally 25–50% of patients diagnosed with severe COPD and 19% of those with the mild to moderate form of the disease suffer from anxiety or depression.1,4– 6 Fear and anxiety, in particular panic disorder, 7 have been shown to be directly associated with episodes of breathlessness particularly during the night, 8 and dyspnoea has a significant influence on perceived burden of disease. 9 Women, older patients and those with greater depression scores have poorer physical functioning. 10 No study has yet shown anxiety or depression to be an independent risk factor for hospital readmission, but depression is possibly causally associated with exacerbation frequency and risk of hospital admission 11 and depressive symptoms with increased risk of mortality in COPD.12,13
In a focus group study of people with chronic bronchitis, Nicolson and Anderson 14 described the negative impact on self-esteem; participants thought of themselves as different to who they were before the onset of illness, which led to a sense of frustration and emotional decline. They also perceived themselves to be a burden and avoided contact leading to increasing social isolation. Other qualitative research has highlighted the importance of the perception of ‘control’ over symptoms 15 and the pervasive impact of dypsnoea on everyday life. 15 – 17 For a sample of patients with severe COPD, 18 quality of life was seen as mainly depending on family relationships, opportunities afforded locally for neighbourliness and freedom from fear, mobility and independence in the activities of daily living in addition to the absence or successful mitigation of symptoms of concomitant disease.
However, despite recommendations that mental health problems co-morbid with COPD should be more actively treated, 19 the mental health needs of people with COPD are notably poorly served, with both patient- and physician-level barriers to the detection and management of anxiety and depression. Patient barriers may include a lack of knowledge about depression and treatment options, stigma, reluctance to talk about emotional problems or the masking of mood symptoms by physical symptoms such as fatigue, decreasing exercise tolerance and dyspnoea.1,20 A small qualitative study of newly diagnosed patients with COPD in Sweden suggested that ‘shame’ for perceived self-inflicted disease may be a factor in failure to seek help. 21 This is echoed in the themes of ‘self-blame’ but also a resistance to being blamed by others (and thus avoidance of others’ gaze) described by the participants in Nicolson and Anderson’s study. 14
In this study, we aimed to try and understand how the un-met mental health needs of this group might be better served by health care services. We approached this by exploring the mental health needs of people living with COPD from four related perspectives which are integral to developing improved services and interventions for this group: what were they experiencing at present? What had they already accessed or received (‘expressed need’)? 22 What did they want which they had not already received? ‘(felt need’) and how might, from their perspective, their emotional needs be more effectively met by the National Health Service.
Methods
Study design
Qualitative study with in-depth interviews of participants.
Setting
Two community–based COPD clinics in Salford, Greater Manchester, United Kingdom.
Sample
Fourteen patients with a spirometry-confirmed diagnosis of COPD using the British Thoracic Society (BTS) guidelines, 23 attending a community-based COPD out-patient clinic, where a member of the clinical team (the Consultant Physician) had previously clinically identified associated emotional distress, were invited to participate. Those who gave informed written consent were recruited to be interviewed. All consents were collected and interview dates confirmed with the patients a week prior to the interview date. The sample was both a convenience sample (approaching those who were due to attend the clinic over a 10-week time period) and purposive (specifically recruiting a sample of those patients within this group with already known associated emotional issues). Selected patients were over the age of 16 but with no upper age limit. We excluded patients whom the clinician considered would be unable to carry out an interview without incurring undue distress because of breathlessness or other associated physical or psychological symptoms. Twenty-two patients were initially approached, seven refused and one withdrew consent after interview. Reasons were unwilling/insufficient time to stay for interview after their appointment with the physician and feeling too breathless to engage in an interview.
Ethics
Ethical approval was obtained from the North Manchester Local Research Ethics Committee with Research and Development approval gained from Salford Research and Development committee.
Interviews
Topic guide for interviews.
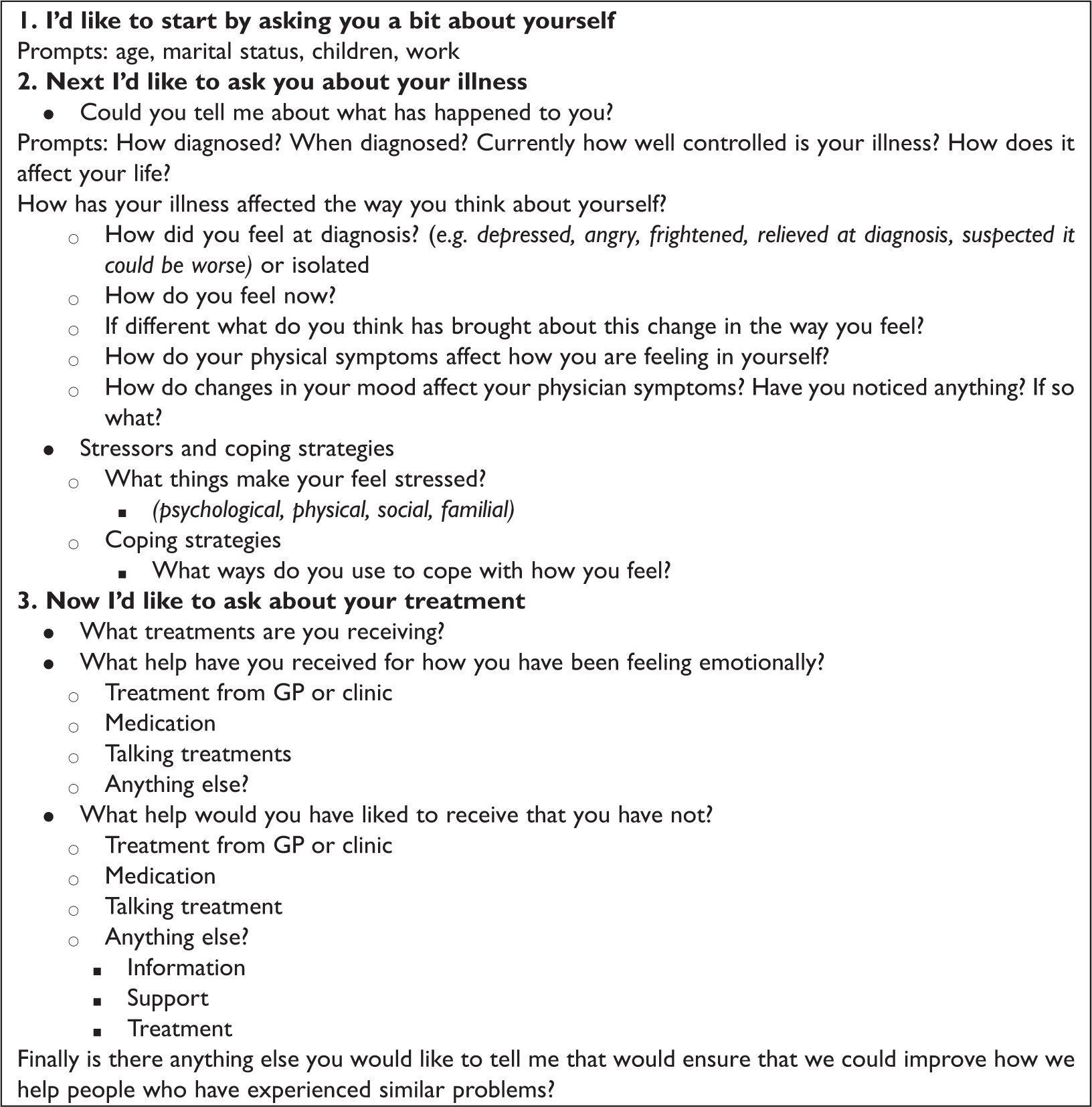
Participants were also asked about anything that, from their perspective, would be an effective addition to their treatment. They were asked to complete two standardised self-report measures of the severity of depression and anxiety (PHQ-9 and GAD-7).24,25 Information indicating the severity of the interviewee’s COPD as per the British Thoracic Society (BTS) classification 23 was also collected.
Analysis
Data were initially analysed concurrent with continuing data collection by development of a simple thematic coding template using MAXqda2 qualitative software; drawing on both the interview questions informed by the literature, and novel concepts emerging from the data, in construction of the template. Interviews were examined thematically across the whole dataset as well as in the context of each person’s interview, using a ‘constant comparative’ method, 26 developing from simple codes to concepts and emergent themes, feeding back developing ideas and questions into the interview process. The transcripts were discussed at length by the research interviewer [LE] and her supervisor [LG] during regular debriefing meetings, and both collaborated in each stage of development of the themes. No new themes were emerging from the data at the conclusion of the thematic analysis, and the researchers were satisfied that saturation had been achieved at this point. This analysis was then further developed by [LG] [supervisor] who utilized a Framework approach 27 to specifically develop and discern what constituted ‘met’ and ‘unmet needs’ in this dataset. This involved interrogating both the raw data and emergent themes from the initial thematic analysis to distil, interpret and structure findings in the light of the original research questions. A biopsychosocial taxonomy, 28 considering physical, psychological and social aspects of care, was employed in developing and populating frameworks with data. At each stage of the analysis, emergent concepts and ideas were developed and refined through discussion in the broader research team to include the respiratory physician and nurse and obtain feedback.
Results
Characteristics of participants
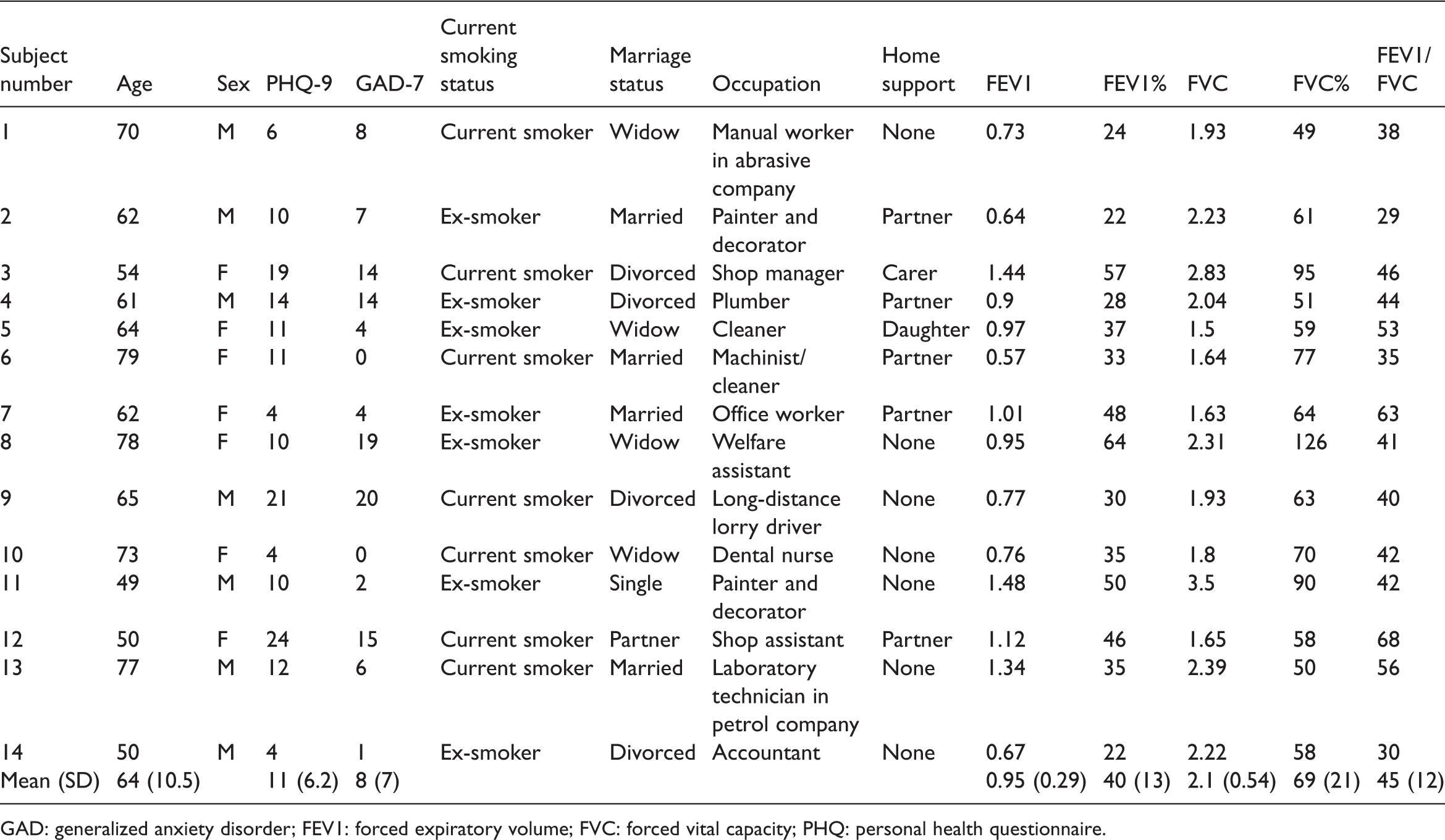
GAD: generalized anxiety disorder; FEV1: forced expiratory volume; FVC: forced vital capacity; PHQ: personal health questionnaire.
Experiencing the illness
Three main themes emerged which relate directly to the first research question – participants’ experience of the illness. First, a sense of changing identity as the disease challenged abilities, affecting confidence and self image. Second, the experience of social isolation, a consequence of experiencing physical limitations and emotional problems. Third, particular types of barriers the participants encountered acting as obstacles to coping, adapting and accessing treatments.
Changing identity
Almost all the participants experienced a change in and loss of their previous sense of who they were. This seemed to be a result of the disease changing the individuals’ abilities, independence and confidence levels, particularly in the presence of other people, and in comparison with their ‘past self’: They don’t look at you the same – you aren’t the person that you used to be. You are somebody else now – … . And I was walking behind these two people. and my chest was really bad so I was going like that (breathing really deep and raspy) and they were looking round at me like I was some kind of monster you know – because my chest was that bad. (SN 9) Sometimes, when I get out of the bath, sometimes M [carer] has to wipe me down, well most of the time really. She wipes me down … . I think it’s just you feel a bit degraded. It is like when it comes to me having to bend down – simple things. (SN 2)
The former had worked very independently as a long-distance lorry driver, and the latter had previously been a fit, active manual worker on a building site.
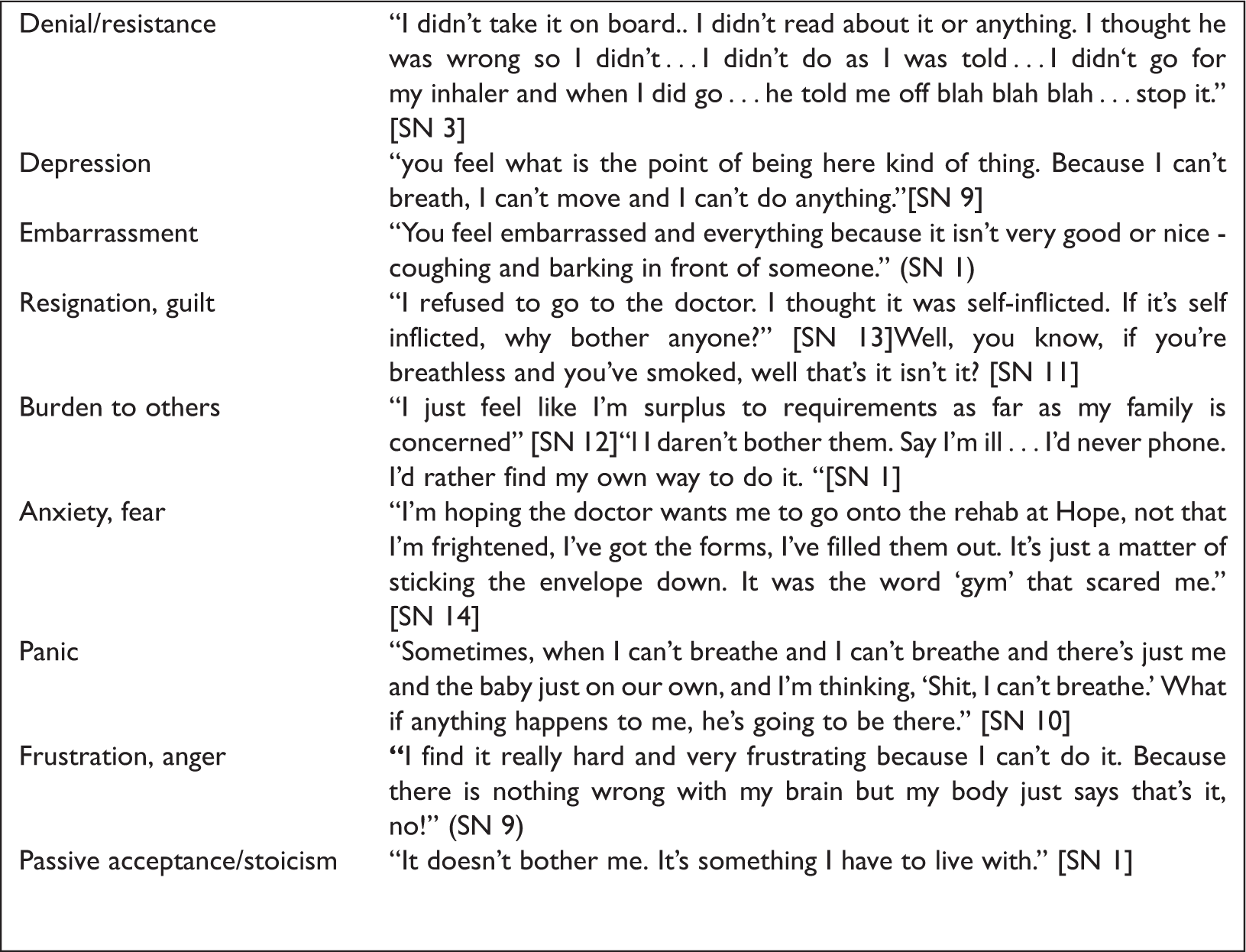
Emotional reactions to illness.
Isolation and fear of dependence
Isolation from others, both due to decreased capability, but also self-imposed isolation related to their mood, was common: I don’t see a fraction of the people I used to. (SN 13 former lab technician) [swearing] don’t want anyone to come anywhere near me. (SN 12 former shop assistant)
A majority of the interviewees expressed a sense of feeling they were a burden to and dependent on those around them. They described how they attempted to reduce their reliance on others which contributed further to social isolation because of their fear of dependence and being a burden. I don’t like relying on folk to come with me because I have always done things myself you know what I mean? I have never relied on people before me. They have always relied on me. But I just can’t do it now. I think I can but I can’t. (SN 8 former welfare assistant)
Several felt that nobody really understood what they were experiencing or how they were feeling which led to both a perceived and real distance between them and those that they had been close to. One woman who had been the manager of a shop said that her partner: … would never understand, people don’t. He tries to understand now, but he doesn’t, he doesn’t. That’s why I get so frustrated. I can be walking and he’ll be walking miles in front of me and I’ll go … and he’ll turn around and look at me and say ‘what’s wrong!?’ and I’ll say ‘For god’s sake.. nothing!?’ and I sit down and go … (SN 3)
Relationships came under pressure, as friends and family tried to support them and prevent the person with COPD from becoming depressed and thus more isolated. This sometimes changed the dynamics of relationships: That’s my own independence I don’t want to lose that … . Like my daughters will say why didn’t you phone when you were ill and all that. I think to myself – why should I? (SN 1 former manual worker)
Nevertheless, others also talked of how they found reassurance in being with people such as their family. They felt ‘safe’ in case their physical health started to deteriorate suddenly. They knew their family would instantly appreciate what was wrong with them and be able to do what was needed to help them. … the only thing I think of is … I know she is there … … at the moment now I feel quite alright, whether it’s because he’s here [referring to partner] constantly, I don’t know. [SN 10 former dental nurse]
However, they were aware that carers did not necessarily find it easy to provide this intensity of support, which contributed to and further compounded the sense of guilt that they felt.
Barriers to accessing care
Physical disability resulting from the illness itself functioned as a barrier to accessing care for several of the interviewees who talked about the practical barriers facing them in getting to clinics: I mean, if I was going to Hope Hospital instead, I would still go in a taxi because I don’t want to park across the road at Stott Lane and then have to walk to the hospital, but I could go through the door there and find one of the hostesses who’d find me a wheelchair and take me wherever I was going … but here you can’t even be dropped off at the door. I bet it’s a man designed it. [SN 11]
But this was also compounded by emotional barriers which were intimately intertwined-acceptance, despair and guilt and which might all serve to militate against seeking further external help. Many of the participants talked about reaching an acceptance that nothing could be done to alleviate the situation. In some, this seemed to have some adaptive aspects in terms of being able to cope more effectively, by employing the technique of downward social comparison
29
: It’s not only me that has got this, there are hundreds and hundreds of other people as bad as me. (SN 1)
But some statements of ‘acceptance’ seemed potentially to mask a sense of deeper resignation: If you get used to something, and you’ve had it so long, it’ll stop becoming an embarrassment, I’m sure. At this rate, in another two years time it won’t embarrass me because you become accustomed to it (SN 14).
And a desire not to be a burden to others: If you’re really bad you rely on other people a lot of the time which I don’t like, because you feel a nuisance, well I do. Or a bit of a burden like. (SN 2)
Further compounded by a belief in some that this was all due to a self-inflicted problem anyway: The reason I refused to go to the doctor . [was because] . . I thought it was self-inflicted. If it’s self-inflicted why both anyone? [SN 14]
For many interviewees, the focus was on finding their own ways of coping with their symptoms, particularly by ‘being positive’, resisting letting things get them down and simply bearing it: [its] my own fault through smoking … . so I have to deal with it. It’s not fair on other people. [SN 3] Well my attitude is, you know, don’t let it get into your head. If I were to allow this, what I have got, to get in to my head, I might as well get measured up. That’s how I look at it. I don’t let anything like this get on top of me. I’ll walk about even though it kills me. [SN 1]
These appeared however not only to serve as coping strategies but effectively as barriers to accessing emotional care: I don’t want to go through everything again and again plus the fact I can’t remember much … like you talk about when it first started … that is an age ago to me … so much has changed … a life time ago … umm … . No and I don’t want to think about it and I don’t want to think that far back. I just go day to day now … and take it how it comes … that’s the only way I can do it. [SN 7]
Experiencing treatment
Interviewees expressed mixed feelings about the treatment that they had received thus far in their illness. Some expressed little faith in further medication – either for their physical or psychological problems: Because over the last five years I’ve had more antibiotics and steroids than goodness knows what. You name it … I’ve had it. [SN 1]
And there was a general reluctance to take antidepressant medication. I didn’t feel like they were doing me any good so I stopped taking them. He doesn’t know about that though. [SN 3 referring to antidepressant medication] But I don’t think that makes much difference … . I don’t know whether it was any good or that but I just took it … . I’ve not took two. [SN 6 talking about fluoxetine]
However, where the participants had been able to engage with pulmonary rehabilitation this was viewed very positively, learning ways to cope with symptoms and getting support from others: … there are people there the same as me, you know. They’re not crying and I’m not crying. It helps to see others cope you know? And we are there together. [SN 4]
And where it had been accessed, psychological therapy was also viewed positively. She was such a lovely lady [the psychologist] … she seemed to understand. She never judged me or anything and she did say if I ever needed her again I just had to see my doctor and she would be there for me. [SN 3]
Unmet needs
There were however doubts expressed by several participants about whether it was actually possible to do anything further to help them, either physically or emotionally. This was unsurprising given the powerful and often negative emotional reactions that many of them were having to their illness as described above.
The possibility that talking therapy might help was viewed with some scepticism: Talking to other people isn’t going to give me a new set of lungs now is it? [SN 1] Talking about it gets on my nerves to be honest. [SN 7]
Others considered that they might benefit from a more supportive approach, and in particular the opportunity to share the burden of their illness with peers: I got a leaflet through from the doctors … it is like a 6 week course thing and it is with other people who have COPD and they are doing group therapies and all sorts of different things to do and activities so.. I think that would be pretty good because like I say you are not just helping yourself then. You would be helping other people [SN 9]
However this was balanced by a viewpoint expressed by others of simple resignation that there was nothing else that could be done, and no unmet needs to be met: They’ve helped me as much as possible and they’ve been very very good with me. [SN 3] You’ve got to sort your own way out of it, anyway, at the end of the day … . I think you’ve got to work your way through it yourself [SN 11]
There was also evidence in some interviews of a degree of ambivalence about expressing need. For example, early in his interview SN 1 talks about ‘feeling very down’ on some days but later counters this with ‘it doesn’t bother me, it’s something I have to live with.’ Similarly SN 6 says: I get down because I can’t do what I want to do’ but later adds ‘there’s no use moaning and groaning over it, what has happened has happened’.
Meeting unmet need
It was thus very difficult to facilitate discussion in the interviews of what might ensure that needs might be more effectively met. Many participants had difficulty in even acknowledging the existence of any unmet needs. As we noted above, there were instances in the interviews of where the apparent need for emotional support was met with ambivalence or rejected. Such rejection might in some people have been strongly related to their view of COPD itself as being self-inflicted and thus that their suffering was somehow ‘justified’. Thus, there was nothing that can be done to help them as noted above. In some instances, such barriers had been overcome by sensitive and flexible engagement by a therapist (as for participant SN 3 above). In other cases, engagement with treatment generally (but not focusing specifically emotional aspects of it) seemed to have been achieved by the provision of information about COPD in a clear and non-confrontational way. The way they’ve explained everything, about what the condition is, yes, brilliant. Really brilliant, because it makes you understand; I can understand what’s happened to my lungs and how it’s been affecting them and what’s affected it, yes … . … I’m very happy with all the help and the consideration I’ve had off everybody that’s been concerned. I’ve just had to learn to do what I’m told, for once. [SN 14]
Discussion
Interviews with participants with a diagnosis of COPD who had been identified by their consultant physician as suffering from associated emotional distress revealed three major themes that characterised their experience of the disorder: a sense of altered identity, social isolation and fear of dependence and barriers to accessing care. Although some had clearly accessed emotional support for their problems, and benefited from it, there was a sense of passive acceptance and resignation, compounded by the emotional concomitants of depressed mood such as despair and guilt. To this, for some, was added the impact of their belief in the disorder being essentially self-inflicted and thus something they would have to deal with themselves. All of these problems were further compounded by the negative views of the self and the future that are the recognised concomitants of depressed mood. Participants were thus largely unable to express whether or what their unmet needs for emotional care actually were, although for some their distress was clearly apparent and palpable.
During the analysis, it became apparent there was a need for health professionals to possess the necessary consultation skills to be able sensitively to negotiate with the patient in relation to denial and uncertainty about addressing emotional aspects of COPD.
Findings in relation to the published literature
A sense of altered identity in a similar group of patients (with chronic bronchitis) has previously been reported by Nicolson and Anderson. 14 This also echoes the work of Bury 30 in his description of biographical disruption in people who experience chronic illness. Previous research has also highlighted how a sense of being a burden to others can result in social isolation, 14 and the key role played by family and supporters in contributing to quality of life, 18 both of which were echoed in our participants. Downward social comparison, which we identified as a coping mechanism used by some subjects, may be important in militating against depression older people with chronic physical symptoms. 31 Our study adds to the literature by exploring how unmet needs for mental health care might, if at all, be addressed.
Clinical implications
There is undoubtedly evidence for the effectiveness of psychological interventions in COPD both in terms of the impact of pulmonary rehabilitation 32 and some evidence for brief cognitive behaviour therapy-based intervention in primary care. 33 However, given the barriers that our participants experienced in accessing care, we would suggest that care may need to be more assertive, using, for example, active case management methods and collaborative care models to engage people more effectively. 34
We would suggest that consideration might be given to how denial of the specifically emotional consequences of COPD and mixed feelings about the need for emotional help and support might also be addressed earlier in the course of the illness. This could be through provision of appropriately designed information and sensitive use of negotiation, before such attitudes become entrenched. This however needs to be done in a way that does not disrupt and indeed promotes normal adaptive coping mechanisms. It will also require improved training of clinicians in patient-centred approaches to exploring the meaning and impact on mental health of chronic illness and assessment of severity of associated anxiety and depression. We think this may be more effective if focussed within primary care, rather than in the specialist setting in which we recruited our sample. It was our perception that in this setting participants may be much more difficult to engage in such discussions because of the increasing chronicity and severity, not only of their physical disease, but associated mental health problems. However, this necessitates further research.
Strengths and limitations of the study
Our sample was necessarily small, given the time limitations of the research interviewer who was a medical student, but saturation of themes was achieved. Although the student was an inexperienced interviewer she was closely supervised and proved highly able to engage interviewees in difficult discussion. Presence of carers and family members may have limited some aspects of the interview (for example in completion of the questionnaires) but the interviews nevertheless proved to be highly insightful.
Conclusions
Provision of mental health care to people with COPD poses major challenges in view of the physical and particularly psychological barriers that they experience in being able to access care. We would suggest that innovative research and clinical care should be aimed towards development of skills, strategies and systems required to engage sensitively and negotiate needs for care, in a patient-centred manner, with people who do not necessarily see the need to ask for emotional support.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.