
Abstract
Background
Physical inactivity is a major factor in the development of many chronic illnesses, including hypertension. Evidence highlighting links among physical activity participation and psychosocial constructs such as self efficacy, social support and perceived barriers among hypertensive patients in the Nigerian population is scarce. This study explored the associations between physical activity and each of self efficacy, social support and perceived barriers.
Methods
Two hundred and twelve patients receiving treatment in two tertiary health institutions located in Ekiti State, Nigeria were surveyed cross-sectionally. Physical activity level, self efficacy, social support and perceived barriers were measured with the International Physical Activity Questionnaire, Exercise Self-Efficacy Scale, Medical Outcomes Social Support Scale and Exercise Benefits and Barrier Scale respectively.
Results
Level of physical activity was significantly associated with self efficacy (rs = 0.67, p < 0.01, = 0.45) and social support (rs = 0.80, p < 0.01, = 0.64), with most participants (56.1%) being physically inactive. However, no association was found between physical activity level and perceived barriers (rs = 0.07, p > 0.01, = 0.005).
Conclusion
Most of the hypertensive patients presented with low levels of physical activity. Physical activity was associated with psychosocial constructs including self efficacy and social support but not with perceived barriers.
Introduction
Hypertension (HTN) is a medical condition in which the blood pressure of an individual is chronically elevated to or above 140/90 mmHg or when there is a reported use of antihypertensive medication. 1 This condition is a very serious public-health challenge in both developed and developing countries. 2 In an analysis of worldwide data in the year 2000, Kaerney et al. estimated the global prevalence of HTN in adults to be about 972 million. 3 They further predicted that this figure would have increased to 1.56 billion by the year 2025. In sub-Saharan Africa, prevalence rates of 36.6%, 29.4% and 24.6% have been reported in Nigeria, Ghana and Cameroon, respectively.4−6 This high prevalence may be due to the fact that Africans have difficulty in adopting lifestyle modifications which could reduce the risk of developing HTN. 7 These lifestyle modifications include weight control, reduced alcohol intake, no smoking and increased physical activity. 8
Physical activity (PA), defined as any energy-expending bodily activity produced by skeletal muscles, 9 has been identified as an important panacea for both the prevention and management of chronic illnesses such as HTN.10,11 Being physically active has been found to reduce the risk of HTN. 11 Thus accumulation of moderate PA on most, if not all, days of the week has been recommended as an exercise treatment for HTN. 10 This gives credence to the recommendation by the World Health Organization that every individual should engage in adequate levels of PA throughout their lives to benefit their health. 12 This recommendation is supported by evidence that PA reduces the systolic blood pressure of hypertensive individuals. 10 The World Health Organization therefore prescribed that everyone should engage in at least 30 minutes of moderate PA daily. 12 In spite of evidence that PA helps to prevent and treat HTN, people are still unable to achieve the recommended levels of PA. 13 Psychosocial constructs have been shown to influence the achievement and maintenance of PA behaviour in healthy adults.14-16 Therefore, the PA of people with HTN cannot be simply explained without considering the influence of psychosocial factors. 14
The Social Cognitive theory of Bandura, a theory hinged on psychosocial constructs, posits that constructs such as self-efficacy, social support and perceived barriers can be key mediators and moderators of lifestyle behaviour. 17 Ayotte et al., in a study of chronically ill middle-aged and older Caucasians, reported that people with higher self-efficacy perceived fewer barriers and reported more PA than people with lower self-efficacy. 14 Literature to support that these psychosocial constructs have influence on achieving the recommended level of PA in hypertensive patients in the Nigerian population are not readily available. This study was therefore conducted to determine whether any association exists between PA and each of self-efficacy, social support and perceived barrier in hypertensive patients receiving treatment in some tertiary health institutions in Ekiti State, South-west Nigeria.
Procedure
This study was a cross-sectional survey of hypertensive patients in the two tertiary hospitals in Ekiti State, South-west, Nigeria. Ethical approval was sought and obtained from the Ekiti State Hospital Research Ethics Committee (UTH/A67/2011/03/005). Participants were a convenience sample of patients managed exclusively for HTN in the 6 months before the study. HTN was defined using either the criteria of blood pressure ≥140/90 mmHg or self-reported use of antihypertensive medication. 1 Participants were recruited from the HTN, medical outpatients and physiotherapy clinics of the hospitals.
All consenting patients who met the inclusion criteria and were seen within the data collection period participated in the study. Inclusion criteria included being managed for HTN only, not presenting with additional disabling conditions such as blindness and amputations, and willingness to fill the informed consent forms. Participants were delimited to those who could read and write English. A total of 250 patients were eligible based on the set criteria and these were subsequently approached for recruitment. Twenty-two of the prospective participants declined, while the rest consented to participate in the study. The data of 16 of the participants could not be utilised in the analysis as they were incomplete.
The aims and procedure of the study were explained to prospective participants before they were eventually recruited and a written informed consent was obtained from each participant prior to their participation in the study. Socio-demographic data such as age, gender, occupation, level of education and marital status were then documented for each participant. The duration of diagnosis of HTN was thereafter extracted from the medical records of the participants.
The International Physical Activity Questionnaire (IPAQ), an internationally developed self-administered questionnaire, was used to assess the PA of the participants. It was administered and scored based on stipulated criteria. 18 The amount of social support available to the participants was measured using the Medical Outcomes Study (MOS) Social Support Survey. The instrument is a 19-item scale developed by Sherborne and Stewart. 19 It has been demonstrated generally that social support is an important influence on health, well-being and exercise.20−23 In spite of this, the majority of exercise-based studies have limited their focus to the contributions of domain-specific social interactions to PA participation, ignoring the contribution of general social support. Lachman and Weaver, 24 however, opined that it is better to use generalized measures in establishing relationships between predictor variables and health and well-being outcomes rather than showing such relationships with domain-specific measures because significant relationships using generalized measures would apply to multiple domains of functioning. The use of the MOS Social Support Survey (a generalized measure) could therefore have the added benefit of promoting health behaviours and outcomes in addition to exercise, which could lead to more comprehensive health interventions. The instrument consists of four separate social support subscales and an overall functional social support index. A higher score for an individual scale or for the overall support index indicates more support. Each item is scored on a 5-point Likert scale and the scores indicate the degree to which the respondent agrees or disagrees with the item question (1 = none of the time, 5 = all of the time). The minimum possible score is 19, which indicates low social support and the maximum possible score is 95.
The Exercise Self-Efficacy questionnaire (ESE) developed by Bandura was used to assess the PA-specific exercise self-efficacy of the participants. 25 The scale is a self-administered questionnaire used as a measure of the confidence in one's ability to persist with exercise in various situations representing the areas of negative affect, resisting relapse, and making time for exercise. The barrier component of the Exercise Benefits and Barriers Scale (EBBS) was used to measure the barriers to PA of the participants. 26 This component consists of 14 items categorized into four subscales: exercise milieu; time expenditure; physical exertion and family discouragement, which are rated on a 4-point Likert-type scale. The score on the barrier scale is inversely proportional to the barriers perceived. The maximum score is 56 while the minimum score is 14. Obtained scores for the ESE and EBBS were divided by the total possible score and multiplied by 100 to obtain a percentage score while the MOS Social Support Survey score was transformed to a 0−100 scale using the following formula: 100 × (observed score – minimum possible score)/(maximum possible score- minimum possible score). 19
Data analysis
Data analysis was conducted using the SPSS Version 16 (SPSS Inc, Chicago, IL, USA). Spearman’s rank correlation was used to determine the association between PA levels and each of exercise self-efficacy, social support and perceived barriers of respondents. Spearman’s rank correlation was also used to determine the association between the duration of diagnosis of HTN and the PA levels of respondents. Standard multiple regression analysis was thereafter used to determine the comparative influence of each psychosocial construct on the physical inactivity of the participants.
Results
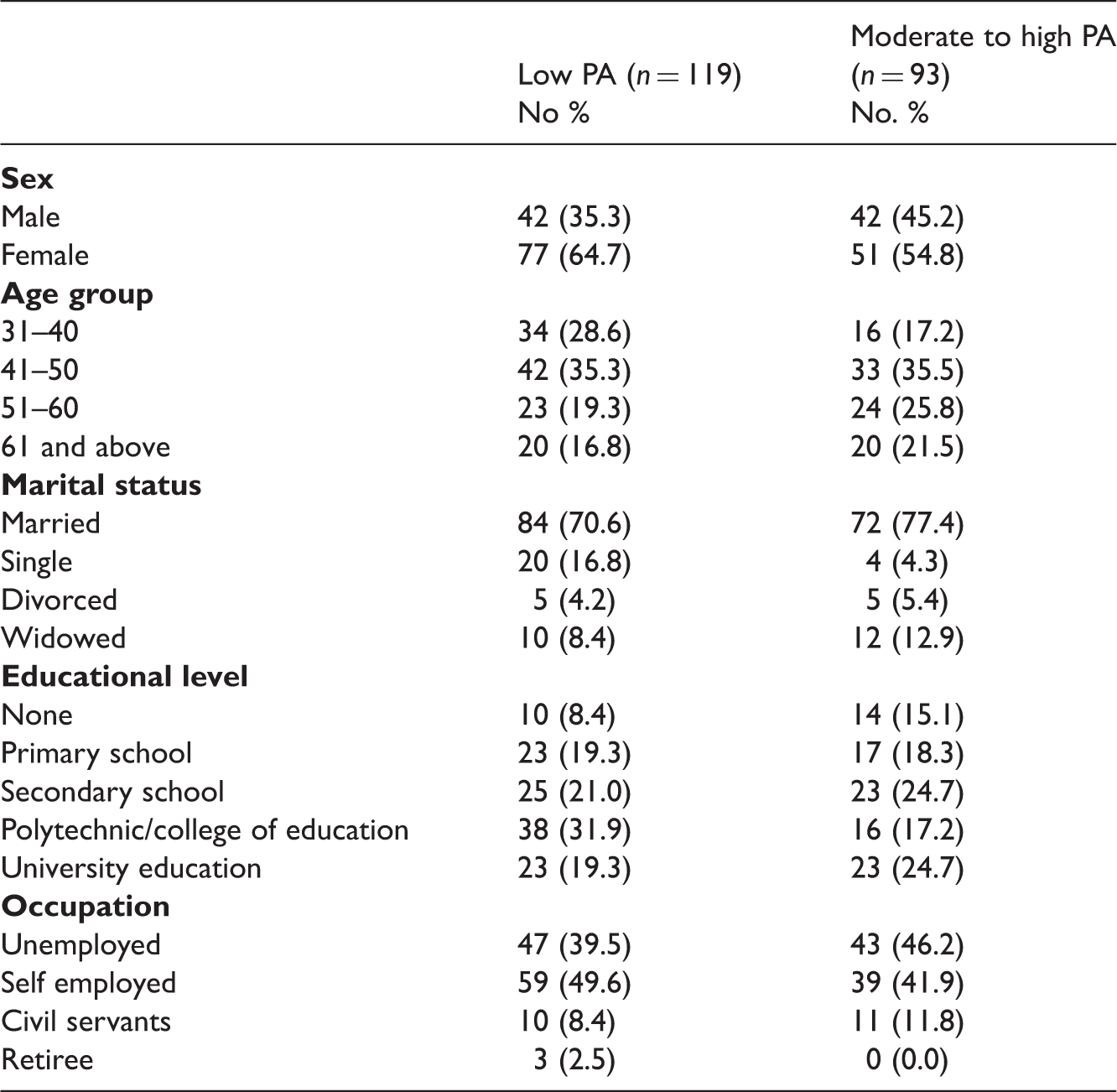
Physical activity levels of participants based on socio-demographic characteristics
Spearman’s correlation between physical activity levels and each of self efficacy, social support and perceived barriers
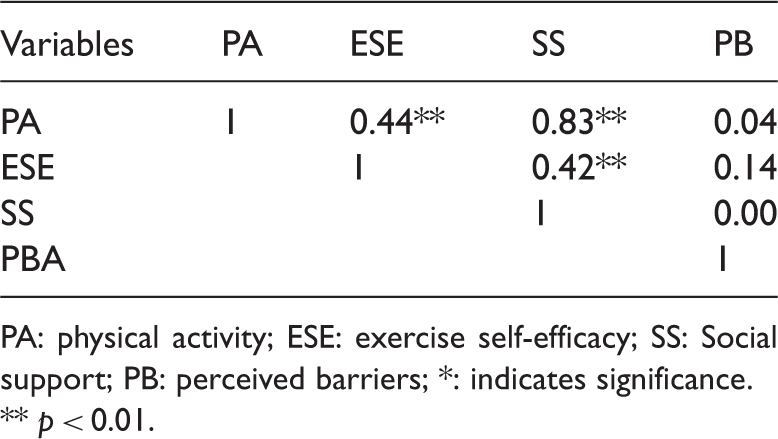
PA: physical activity; ESE: exercise self-efficacy; SS: Social support; PB: perceived barriers; *: indicates significance.
p < 0.01.
Standard multiple regression analysis showing the influence of each of social support, self efficacy and perceived barriers on physical activity
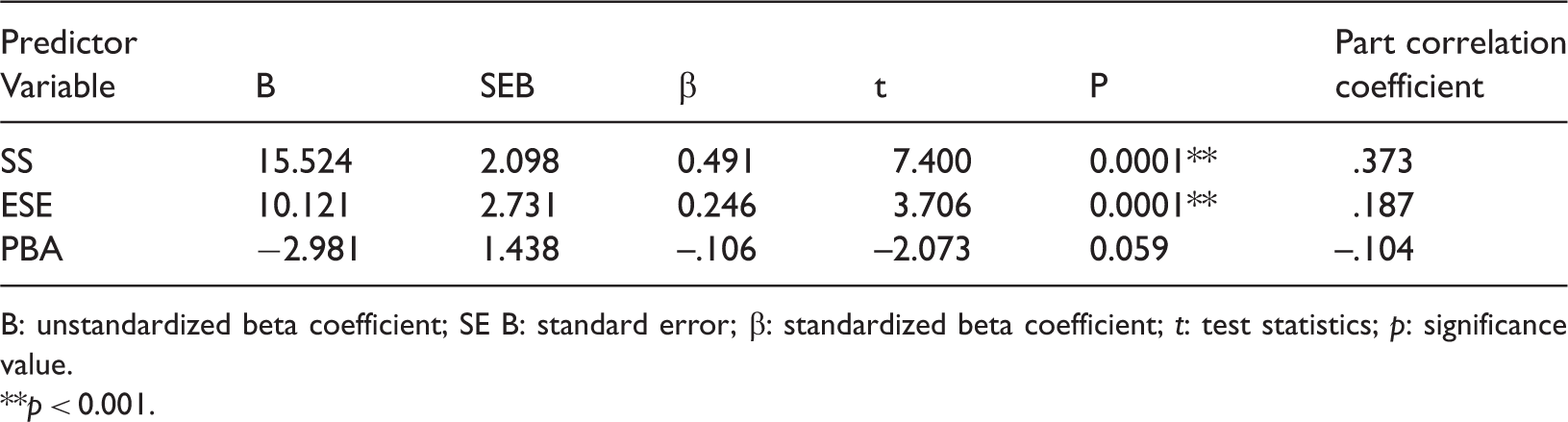
B: unstandardized beta coefficient; SE B: standard error; β: standardized beta coefficient; t: test statistics; p: significance value.
p < 0.001.
Discussion
The high level of physical inactivity reported by more than half of the participants in this study is similar to that found by Ahmed et al. who, in a study on compliance to antihypertensive drugs, salt restriction, exercise and control of systemic HTN, reported low PA level by 76.4% of the participants. 27 This may not be unconnected with the low level of awareness about prevention and treatment of HTN in this part of the world. 28 There is a need for the general populace to embrace lifestyle modifications which may help to reduce the risk of developing HTN. To achieve this, researchers have continued to carry out studies to find different ways to increase PA as a result of the high levels of reported physical inactivity among the chronically ill. 17 One way of doing this is to conduct studies that will enable the characterization of the various life factors that may influence PA with the aim that the outcome of such studies will serve as a guide to the effective promotion of PA among patients with chronic illnesses.
The present study examined the influence of self-efficacy, social support and perceived barriers on the PA levels of hypertensive patients. Direct links were observed between the PA levels and each of self-efficacy and social support of the study participants. The reason why some of these psychosocial variables were linked with PA is unknown. It is however known that hypertensive patients are often faced with a myriad of challenges vis-a-vis medical management, difficulty in maintaining life roles and managing negative emotions such as fear and depression. 29 These may affect the patients’ belief in themselves and in their ability to adopt and maintain the recommended levels of PA. 30 When social support is provided for such individuals to enable them overcome these challenges, they can feel disparaged, nagged or guilty about receiving help. 30
The findings in this study suggest that the availability of social support from loved ones may assist in self-management behaviours, while patients are also expected to take self-management actions requiring adequate levels of self-efficacy in order to achieve desired health outcomes. 31 It is therefore important to ensure that there is a paradigm shift on the part of social support givers to also endeavour to motivate and facilitate healthy behaviour in their patients rather than shouldering all illness care tasks on the patient’s behalf. 32 It has also been suggested that the self-efficacy of support givers with respect to helping the patients should not be ignored. 33 These findings are consistent with a growing body of evidence supporting an association between PA and each of self-efficacy and social support.14−16
No significant association was observed between PA levels and perceived barrier. This is contrary to the findings of Sternfeld et al. who reported a negative association between perceived barriers and the likelihood of being physically active. 16 A major difference, however, between this study and that of Sternfeld and colleagues is that their sample was drawn from an apparently healthy population of ethnically diverse women who were members of a large health maintenance organization while this study recruited patients diagnosed with HTN. Studies reporting the role of barriers in adopting and maintaining PA behaviours have been inconsistent and the role of changes in barriers possibly affecting decisional balance is unclear. 34
Based on the observation that PA was associated with self-efficacy and social support, the present study further examined the comparative influence of the psychosocial variables on PA using the standard multiple regression analysis. It was discovered that the psychosocial variables had combined influence on the PA of the participants, explaining almost half of the variance in the participants’ PA. However, more than half of their PA profile may have to be attributed to other variables that were not accounted for in the study. It was assumed that other variables, such as motivation for instance, may have had considerable influence on the PA of the participants. Out of the three psychosocial variables, it was however discovered that self-efficacy and social support had significant contributions to the observed PA of the participants, with social support having the dominant influence. Research has shown that social support is an important factor that influences regular engagement in PA.15,35 According to Bandura, 36 the social environment (of which social support is a part) could either facilitate or hinder health behaviour change. For instance, positive social support from friends or family members may enhance an individual’s health behaviour (an example of which is PA participation). One of the ways in which social support impacts on participation in PA is through its influence on self-efficacy. Those who receive more support are more likely to increase their self-efficacy beliefs,36-38 which increases the likelihood of them being physically active. 36 Lack of social support can be a major barrier to PA participation by individuals, regardless of their level of PA. 39
Limitations
Notwithstanding the findings made, this study was confronted with some basic limitations. The reliance on self-reported information for PA, though obtained through a validated questionnaire, is one limitation that readily comes to the fore. A second limitation is that no random samples were drawn; data was collected only from patients receiving treatment in two tertiary hospitals. The implication of this is that the results obtained herein may not exactly represent the situation with hypertensive patients who do not receive treatment in the hospitals. The correlational nature of this study is the third limitation in that causal relationships could not be inferred from the study.
Conclusion
The results show a low level of PA among a group of Nigerian patients with HTN and suggest that self-efficacy and social support were associated with this low level of PA. Social support appears to play a superior role in explaining the PA of the patients. This implies that the likelihood of engaging in adequate levels of PA by hypertensive patients will increase through the provision of adequate psychosocial support, especially in an enabling environment where social support is readily available.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicting of Interest
The authors declare that there is no conflict of interest.