
Abstract
Objectives
To describe the support that patients reported receiving from family or friends (F/F) while participating in a self-care intervention for depressive symptoms; examine associations between patient-reported F/F support and use of self-care materials; and describe F/F perceptions of involvement in a subsample of F/F.
Methods
One hundred eighty-nine of 223 (85%) patients aged 40+ with chronic physical conditions and co-morbid depressive symptoms participating in a randomized self-care intervention trial, completed structured telephone surveys at three months about the F/F support received. Ten F/F participated in post study qualitative interviews on the support provided.
Results
30%, 44%, and 91% of patients reported overall F/F support with self-care, F/F involvement with the self-care intervention and emotional support, respectively. 61% felt positively and 10% felt negatively or conflicted with F/F support. F/F involvement in the self-care intervention was the only variable associated with patient use of self-care materials when examined alongside all F/F support variables (Proportional Odds Ratio = 1.21; 95% C.I. = 1.01, 1.45). F/F perceived less involvement in the self-care intervention than patients.
Discussion
Patients engaged in a self-care intervention for depressive symptoms use more self-care materials when they perceive F/F involvement in the intervention. Patients and F/F may perceive involvement differently and benefit from discussions about potential F/F roles.
Introduction
Supported self-care aims to activate patients with chronic conditions to develop strategies to monitor and manage symptoms, adhere to prescribed medications, cope with the impact of illness, and identify when to seek medical consultation. 1 This approach to chronic disease management is clinically sound and potentially cost-effective.2–4 It has been shown to be feasible, acceptable, and associated with improvement for patients managing depressive symptoms and co-morbid physical conditions.5–7
Self-care can be complex, and therefore, some patients engage family and friends (F/F) to help them make decisions about seeking medical attention, adhere to medical recommendations, and cope with their conditions.4,8–13 F/F encouragement and support may be particularly salient for those managing depressive symptoms, since motivation for eating well, staying active, and changing thinking patterns can be compromised by feelings of hopelessness and helplessness.14–17 In fact, social cognitive theory, the framework on which self-management is based, suggests that environmental factors such as F/F support have the potential to positively influence patient health behaviors. 18
Despite the role F/F may play in supporting patients’ self-care practices, relatively few studies have explored the relationship between F/F support and patients’ self-care adherence. Those that have, report some positive associations between F/F involvement in patients’ self-care practices and adherence to prescribed regimes for heart failure,8,19 diabetes, 20 and depressive symptoms.21,22 Roles found helpful include instrumental/tangible support to facilitate self-care, 22 appraisal support to assess when medical consultation is indicated, 19 and emotional support to encourage continued adherence to self-care regimes.8,21
Caution still exists regarding the role F/F may play in depressed patients’ self-care, where patients tend to report high incidences of negative experiences with F/F involvement compared to those who are managing physical conditions only.15,23 Indeed, negative or non-supportive F/F behaviors, when measured, have been associated with low illness self-efficacy, poor self-care adherence, and illness distress for patients managing heart failure or diabetes.23,24 Patients who appear most susceptible to negative forms of support tend to be those individuals with co-morbid depressive symptoms 23 and wives. 25
Despite awareness that F/F can have both positive and negative effects on patients’ self-care practices, we know relatively little about the type of support F/F provide to patients engaged in self-care to manage depressive symptoms. We similarly lack information about patients’ perception of support received, the relationship between F/F involvement and patients’ adherence to self-care regimes, and F/F’s desire or willingness to participate in patients’ self-care regimes for depressive symptoms.
In the context of a randomized trial comparing a telephone-based supported self-care intervention for depressive symptoms with a similar unsupported intervention, we sought to describe (1) patients’ perceptions of the type of support they received from F/F, (2) patients’ positive and negative experiences with F/F support, and (3) the relationship between perceived F/F support and patients’ use of self-care tools. In the qualitative component of the study, we explored F/F’s perceptions and experiences with the support they provided.
Methods
Patient data were derived from primary care adults with chronic physical conditions and co-morbid depressive symptoms participating in a single blind, pragmatic trial of a self-care intervention for depressive symptoms with no prescribed F/F role. Details of the interventions and methods have been reported elsewhere. 7 The intervention group received a toolkit comprising of informational and cognitive-behavioral tools in paper and audiovisual format and was offered telephone coaching; the control group received the toolkit only. Both groups also received a booklet for F/F that contained information about depression, and resources for F/F. The F/F booklet was the only material specific to F/F involvement. Patients in both study arms were left to decide if/when to share the booklet with F/F. The study protocol was approved by the St. Mary’s Hospital Center Research Ethics Board (file # MP-CHSM-11-030).
Sample and recruitment of patients
In 2012–2013, prospective participants completed self-referral forms in primary care settings in Montreal, Canada indicating that they were aged 40 or more, with at least one chronic physical condition (a doctor diagnosed condition lasting six months or longer including chronic pain) and a positive PHQ-2 screen for depression. 26 Potentially eligible patients were contacted by research staff to determine interest and further eligibility for the trial: a PHQ-9 score of 5 or more (indicating at least mild depression symptoms), 27 no suicidality, no current cognitive-behavior therapy, residing in the community, ability to read in either English or French, at most mild cognitive impairment (score of less than 10 on the 6-item Blessed Orientation-Memory-Concentration test),28,29 and no visual, hearing, or other impairment that would prevent them from using the tools or participating in telephone interviews.
A research assistant (RA) met eligible, interested individuals and invited the signing of the consent from. Consenting individuals were randomized individually to the intervention or control arm. 7
Sample and recruitment of family members/friends (F/F)
At six-month post-intervention follow-up, patients were invited to provide the name of one F/F aged 18 and over who provided tangible or emotional support to participate in an end-of-study qualitative interview. F/F identified were called by an RA who provided more information about the study. F/F willing to participate were sent a consent form and offered a telephone interview.
Measures
Patient measures
Patient characteristics
Socio-demographic variables included: age, sex, marital status, and level of education.30,31 Health variables included: the Health Survey Short Form-12 (SF-12), 32 and the Patient Health Questionnaire (PHQ 9) for depressive symptoms. The SF-12 physical component summary (PCS) score ranges from 0 to 100, a higher score indicating better physical health. 32 The PHQ 9 asks patients to indicate how often in the past two weeks they experienced each of nine depressive symptoms. Total scores ranging from 5 to 14 indicate mild to moderate severity and scores 15 or greater indicate moderately severe to severe depressive symptoms. 33
Patients’ perceptions of F/F support provided
Four measures were used to capture patients’ perceptions of F/F support provided. The Family Support for Self-Management Scale was used to capture overall F/F involvement in self-care. 23 Respondents are asked how often in an average week their F/F assisted with healthy eating, exercise, medication adherence, symptom monitoring, and management of medical care. Possible responses for each domain are never (0), rarely (1), some days (2), many days (3), and almost every day (4). Mean scores were calculated for each participant.
To represent F/F involvement in the self-care intervention, study participants were asked how often they were supported in the use of self-care materials. Possible responses included never (0), rarely (1), some days (2), many days (3), and almost every day (4).
To capture emotional support participants were asked (a) if they could identify a F/F who provided emotional support and (b) if the person providing emotional support was different than the person providing self-care support. Participants were coded as not receiving emotional support, receiving emotional support from the same person that helped with their self-care, or receiving emotional support from a different person.
Finally, to capture positive and negative experiences with F/F support, participants were asked 11 questions adapted from the work of Rosland et al., 23 exploring the frequency with which they felt positively (e.g. glad) or negatively (e.g. criticized) about F/F involvement, where each item was coded from never (0) to almost every day (4). In the previous study, 23 responses to each question were reported separately. For our study, we clustered items into sub-domains using a principle component analysis with varimax rotation. This analysis yielded three factors with eigenvalues greater than or equal to one, factor loadings of 0.40 or greater, 34 and clear conceptual distinctions: (1) negative experiences (nagged, criticized, argued, ignored, frustrated, and annoyed; Cronbach’s alpha coefficient 0.95); 35 (2) conflictual experiences (feeling guilty, confused or worried about over-burdening F/F; Cronbach alpha coefficient 0.66), and (3) positive experiences (glad, confident; Cronbach alpha coefficient 0.60). We calculated mean scores for the items comprising each factor to represent the extent to which participants experienced positive, negative, and conflictual support.
Self-care tool use
Use of the self-care tools was assessed by asking patients to identify how much they used each of the three core self-care tools and four supplemental self-care tools designed specifically for patients (excluding the F/F booklet). A score for total tool use was generated by summing the level of use for all seven tools ranging from 0 (never used any tools) to 13 (completed all tools).
Patients were also asked if they had distributed the F/F booklet. Possible responses were yes (1) or no (0). This tool was measured separately as its purpose was to provide patients with a tool to explain depression and self-care to F/F.
F/F measures
F/F perceptions of support provided
Qualitative interview guide
A semi-structured interview guide for telephone interviewing of F/F was developed by TS and revised by the research team. The guide aimed to elicit F/F experiences and involvement with patients’ self-care practices and the self-care intervention. F/F recommendations on the role F/F might play in the self-care intervention were also probed (see Appendix A for interview guide). Interviews were conducted by an RA in either English or French, and ranged from 13 to 35 mins in duration.
Data analysis
Quantitative data
Descriptive statistics were used to characterize patients, type of F/F support provided, and patients’ positive and negative experiences with F/F support. Chi-square and t tests were used to compare patient characteristics by study arm. Bivariate associations between patient characteristics, type of F/F support provided, and perceptions of support were tested using Chi-square analysis for categorical data, 36 one-way analysis of variance (ANOVA) for continuous data, 37 and one-way Kruskal–Wallis for skewed data. 38
Associations between type and perceptions of F/F support and patients’ self-care tool use and F/F booklet use were examined using ordered logistic regression and logistic regression, respectively. 39 Univariate and initial multivariable models were developed for each outcome adjusting for patient characteristics and study group (intervention versus control). Spearman correlation coefficients were calculated to measure the strength of associations among the F/F support variables (independent variables). A final multivariable model, including patient characteristics, study group, and all F/F support variables (6) was performed, and variance inflation factors (VIF) were also computed for each F/F support variable to assess potential collinearity. Variables with VIF greater than 3 and Spearman correlation coefficients greater than 0.60 were removed from the final multivariable models. A Likelihood-ratio test was performed to ensure that the odds ratio from the ordinal regression analysis was proportional across all values of the outcome. Quantitative data were analyzed using SAS version 9.4.
Qualitative data
All interviews were tape recorded, transcribed, and analyzed in three stages informed by the methods associated with thematic analysis. 40 In the first stage, a RA-coded interview data by placing excepts from transcripts into broad preliminary categories that matched the areas probed in the interview guide. The descriptive categories developed at this stage included: F/F descriptions of all support offered, F/F perceptions /experiences with support offered, the role F/Fs played in self-care intervention, the role F/F might play in self-care interventions. This initial coding structure revealed a trend toward minimal or lack of F/F involvement in the self-care intervention. To explore this trend further, the second stage of data analysis involved a comparison between F/F descriptions of involvement (qualitative data) and patient ratings (quantitative data). At this stage, discrepancies between F/F and patient reports were noted, and the theme F/F perceived less involvement in the self-care intervention than patient reports was developed. In the third stage of the analytic process, the descriptive categories developed in stage one were re-examined by TS using the constant comparison method. 41 More specifically, connections and patterns were sought to uncover how F/F talked about the support they provided, and what this could mean about their perceived or future involvement in the self-care intervention for depression. Themes developed at third stage included: Lack of Involvement Tied to Fears of Doing More Harm than Good; Emotional Support: Necessary but Complex and Joint Activities Identified as Helpful and Rewarding.
Results
Of 597 patients screened, 407 (68.2%) were eligible for study participation and 223 (54.8%) provided written informed consent and were randomized. Among those 223, 189 patients (85%) completed the three-month interview examining their self-care tool use and F/F support.
30 F/F were referred by patients, of whom 10 (33%) were reached and participated in the end-of study qualitative interview. Reasons for non-participation included: unreachable (16), deceased (1), too busy (2), refused (1). F/F interviews were conducted at study completion—six months to one year after associated patients completed their three-month interview.
Baseline characteristics of patient sample by study arm (n = 189).
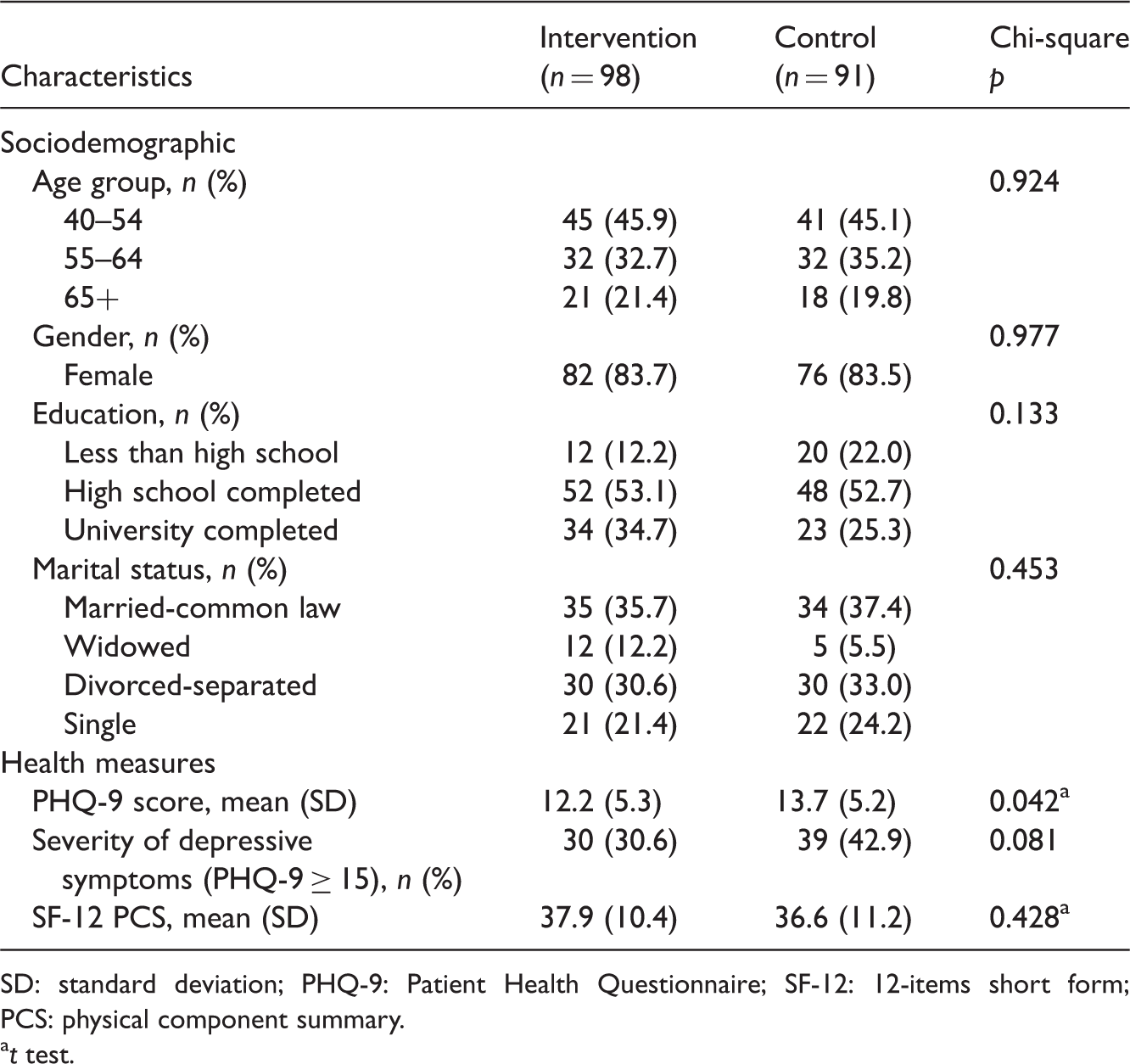
SD: standard deviation; PHQ-9: Patient Health Questionnaire; SF-12: 12-items short form; PCS: physical component summary.
t test.
Patients’ perceptions of F/F support provided and patient characteristics
Patients’ perceptions of F/F support provided and self-care tool use at three months (n = 189).
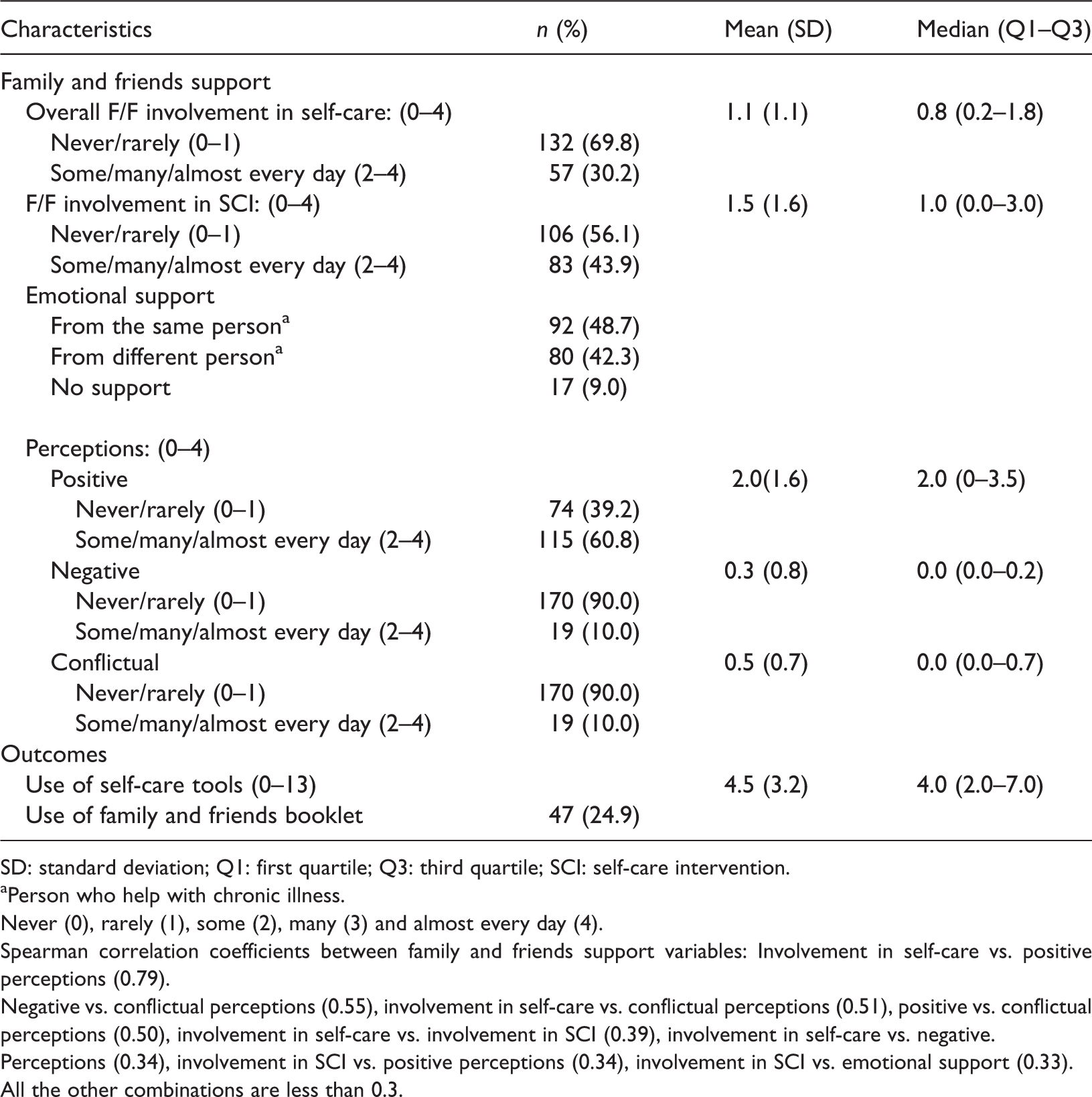
SD: standard deviation; Q1: first quartile; Q3: third quartile; SCI: self-care intervention.
Person who help with chronic illness.
Never (0), rarely (1), some (2), many (3) and almost every day (4).
Spearman correlation coefficients between family and friends support variables: Involvement in self-care vs. positive perceptions (0.79).
Negative vs. conflictual perceptions (0.55), involvement in self-care vs. conflictual perceptions (0.51), positive vs. conflictual perceptions (0.50), involvement in self-care vs. involvement in SCI (0.39), involvement in self-care vs. negative.
Perceptions (0.34), involvement in SCI vs. positive perceptions (0.34), involvement in SCI vs. emotional support (0.33).
All the other combinations are less than 0.3.
Association between patient characteristics and patients’ perceptions of F/F support provided (n = 189).

SD: standard deviation; PHQ-9: Patient Health Questionnaire; SF-12: 12-Item Short Form; PCS: physical component summary; SCI: self-care intervention.
1 Characteristics with two categories, t test was performed, with more than two categories, one-way ANOVA was performed.
2 Chi-square test was performed.
3 Kruskal–Wallis test was performed.
Person who help with chronic illness.
Patients’ perceptions of F/F support provided and self-care tool us
Associations between patients’ perceptions of F/F support provided and self-care tool use at three months (n = 189).
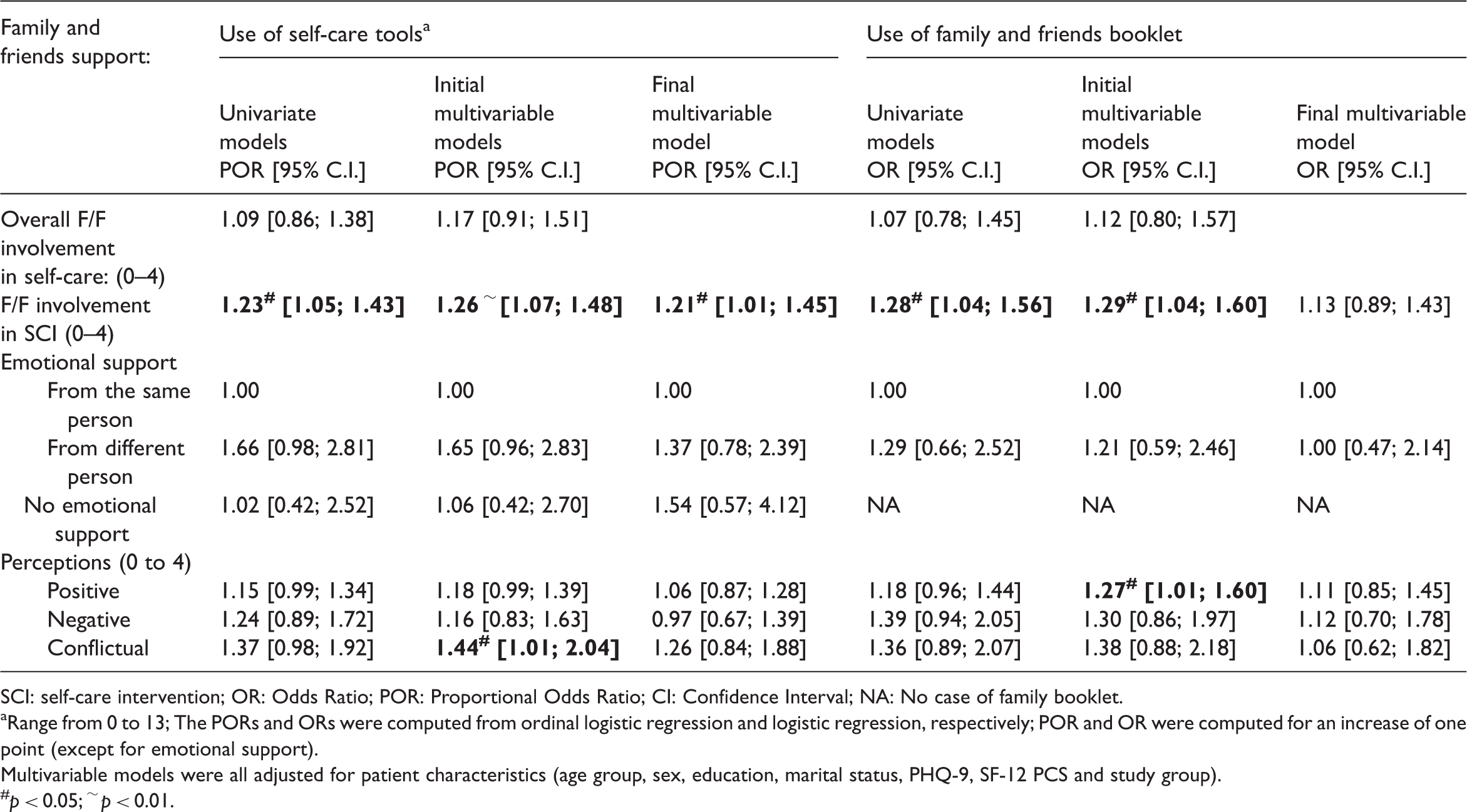
SCI: self-care intervention; OR: Odds Ratio; POR: Proportional Odds Ratio; CI: Confidence Interval; NA: No case of family booklet.
Range from 0 to 13; The PORs and ORs were computed from ordinal logistic regression and logistic regression, respectively; POR and OR were computed for an increase of one point (except for emotional support).
Multivariable models were all adjusted for patient characteristics (age group, sex, education, marital status, PHQ-9, SF-12 PCS and study group).
#p < 0.05; ∼ p < 0.01.
The first analysis explored unique relationships between overall F/F involvement in self-care, F/F involvement in the self-care intervention, emotional support, positive, negative, and conflictual perceptions of support and patient self-care tool use while adjusting for patient characteristics. In this analysis, F/F involvement in the self-care intervention and conflictual feelings about F/F support were both significantly associated with more self-care tool use. However, a Variance Inflation Factor of > 3 for overall involvement in self-care, combined with a high correlation coefficient between overall involvement in self-care and positive perceptions resulted in the removal of overall involvement in self-care from the final multivariable model. A final multivariable model, which explored the combined effect of all remaining F/F support variables shows that only F/F involvement in the self-care intervention was associated with self-care tool use for depressive symptoms, with a one point increase in involvement associated with a 21% increase in tool use.
The second analysis explored unique relationships between overall F/F involvement in self-care, F/F involvement in the self-care intervention, emotional support, positive, negative, and conflictual perceptions of support, and F/F booklet distribution while adjusting for patient characteristics. In this analysis, F/F involvement in the self-care intervention and positive experiences with F/F support were both significantly associated with F/F booklet distribution. However, after removal of overall self-care support (as per above), a final multivariable model which explored the combined effect of all remaining F/F support variables shows no significant associations with F/F booklet distribution.
Results of qualitative interviews with F/F
Demographics of F/F who participated in qualitative interviews
Three friends, four spouses, two daughters, and one sister participated in F/F qualitative interviews. Nine of 10 were women. Six were supporting patients in the control arm of the study. Nine were linked to patients who reported discussing the self-care tools with them, and seven were linked to patients who reported getting their assistance with self-care materials some days or more.
F/F perceived less involvement in the self-care intervention than patient reports
While seven F/F interviewed were identified by patients as having been involved in the self-care intervention some or most days, only two F/F saw themselves as involved in the self-care intervention. One wife describes watching the video with her husband, and comments that this helped her to remind him of certain aspects of the illness. She stated, “We sat down and watched the video together… There are certain things that I picked up and was able to remind him of.” A friend helped a patient work through the work book providing her with some structure around the support she was offering. She stated, “it was a guide to help talk to her and encourage her it was a guide I could use.”
Lack of involvement tied to fears of doing more harm than good
F/F described their lack of involvement as tied to concerns that self-care should be a private matter and worry that getting involved could harm their F/F. As one daughter stated, “I don’t know I really feel this is something he has to do on his own… if his family is pushing him it would make him withdraw more.” A friend stated, “she could have invited me to be involved if she wanted me to be” [translation].
Most F/F suggested that their apprehensions could have been addressed if they had the opportunity to discuss potential involvement with patients or a self-care coach. As one spouse stated, “but maybe, if someone had called me and said how you can use these tools or how you can encourage him to use them, that would have been good.” Another spouse stated, “it would have been good if someone from the beginning asked him if he wanted someone involved in helping him and had a meeting with him and that person, that would have been very constructive” [translation].
Emotional support: Necessary but complex
All F/F provided general support to their F/F on a weekly and sometimes daily basis. As one wife stated, “…I try to listen and hear what he’s going through and I try to give him perspective, my more optimistic perspective.” Similarly, a daughter said, “Yes, if she wants to talk, I will listen” [translation].
Many F/F could recount moments when support was not easily provided or readily received. One wife noted how her efforts at encouragement were experienced by her husband as non-supportive. She stated, “… and he feels I’m always interrupting, but I try my best, um I try to just stay calm and be supportive as much as possible.” A sister who also noted her sibling’s negative reactions toward her gestures of support stated, “I need to try and stay even. I’ve learnt how to control my emotions a little more so I don’t react as much, but there are times when it’s harder I guess.” Finally, a daughter whose father doesn’t readily share his emotions stated, “It is kind of a thing you have to pick up on. It is hard because he tries to hide it.” When overtures of emotional support were met with resistance, agitation, or avoidance F/F described feeling “insignificant,” “useless,” “helpless,” and “ripe with self-doubt” wondering how and if at all they can help their relatives feel better. Perhaps as a consequence many F/F were reticent to get involved in the self-care intervention without a formal role or direction ascribed to them.
Joint activities identified as helpful and rewarding
While some F/F struggled with the provision of emotional support most found it easier and rewarding to provide practical support such as assistance with shopping, meal planning, medical visits, and recreational activities. In these instances, F/F appraised their assistance as “helpful” and “mutually beneficial.” When done alongside patients, these tasks could also serve as a form of connection, distraction, and pleasure. As one wife stated, “last summer we bought bikes because my husband’s neurosurgeon told him it was a good activity for his back. We really like it.” Another friend commented that she enjoys “taking her [friend] out and getting her mind off of things.” A daughter whose father tends to hide his emotions said she “enjoys going shopping with [her father] to keep him company.”
Discussion
Summary of main findings
In this mixed-methods study, we explored the role F/F play in a self-care intervention offered to individuals with depressive symptoms and co-morbid chronic physical illnesses, the relationship between patient characteristics, perceptions of F/F support provided, and use of the self-care tools. A third (30%) and just under half (44%) of patients reported overall F/F involvement in self-care and F/F involvement in the self-care intervention and almost all patients (91%) reported receiving emotional support. Patients generally felt that the support they received from F/F was positive (61%), with only 10% reporting experiences of negative or conflictual support. Patients in a marital relationship reported the highest levels of overall F/F involvement in self-care and more positive perceptions. Patients with poorer physical health reported more overall F/F involvement in self-care in general and the self-care intervention in particular and patients with more severe depressive symptoms reported less emotional support.
When adjusting for patient characteristics and examining the combined effect of F/F support, only F/F involvement in the self-care intervention was associated with patient use of self-care tools, and no variables were associated with F/F booklet distribution.
The combined quantitative and qualitative data highlighted discrepancies between patient reporting of F/F involvement and F/F perceptions of involvement in the self-care intervention, with patients generally reporting more perceived F/F involvement than F/F. Reasons for non-involvement seemed driven by fears of doing more harm than good and uncertainties regarding patients’ preferences for F/F involvement.
When F/F described the general support, they provided to patients for self-care, they expressed more difficulties providing emotional support to patients, and more pleasure supporting patients in behaviorally oriented self-care practices such as going out, conducting errands, and engaging in joint physical activities.
Interpretation and prior literature
On average, patients in this study reported infrequent exposure to negative or conflictual F/F support and frequent exposure to positive support. For example, our patients reported less negative/conflictual support and similar levels of positive support than Rosland al.,'s 23 sample of patients with heart failure and diabetes. This is somewhat surprising given that patients with depressive symptoms tend to express more frustrations with F/F support than patients with physical conditions only.15,23 It is possible that some of the observed differences with Rosland et al.,'s sample can be attributed to how perceptions of support were calculated (a sum score of a number of items in our study and high endorsement of only one item in theirs). It is also possible that the context from which our studies were drawn (an intervention setting versus a natural setting) accounted for some of these differences. For example, our self-care intervention may have provided patients with opportunities to elicit positive support from F/F such as engagement in beneficial activities.
The one point increase in F/F involvement associated with the 21% increase in the use of self-care tools was an important finding. While some patients may experience guilt or uncertainty about the involvement of F/F, patients with depressive symptoms appear to use more self-care materials when they report F/F involvement with a self-care intervention. This finding builds on our previous work which documents bivariate positive associations between F/F involvement in a self-care intervention and patient use of behaviorally oriented self-care tools. 22
The combined qualitative and quantitative findings suggest that patients may have interpreted F/F involvement in a self-care intervention differently from F/F. More specifically, some F/F who had been identified as involved by patients did not see themselves as actively supporting patients in the self-care intervention. It is possible that patients considered F/F involvement in activities or general emotional support/encouragement to be a form of support with the self-care intervention, while F/F did not. Future research would benefit from examining what patients consider to represent F/F involvement in a self-care intervention, as this information may be particularly salient for directing practice.
Qualitative data provided some insights into F/F experiences with support provided. F/F described the provision of general emotional support as an important but complex aspect of their role. Janevic et al. 42 similarly uncovered that F/F who provide illness support to patients with depression and co-morbid physical conditions can experience their role as challenging. These combined findings suggest that an examination of F/F involvement in a self-care intervention must consider F/F experiences alongside patient outcomes.
Our qualitative findings also suggested that F/F found joint activities such as exercising together, going on outings, and assisting with errands enjoyable and rewarding. Previous research in diabetes self-care has suggested that F/F participation in healthy activities can positively impact patients’ adherence to self-care regimes and satisfaction with care. 43 Findings from our study indicate that engaging in these types of activities may also benefit F/F.
Limitations
This study has several limitations. First, the study measure of F/F involvement in the self-care intervention was a global one that did not ask patients to report on the receipt of specific types of F/F support with the self-care intervention (e.g. help formulating goals, encouragement, participation in activities that supported healthy behaviors). This makes it difficult to identify how patients understood F/F involvement in the self-care intervention, and what types of F/F involvement may be helpful to patients with depressive symptoms (which may differ from patients with chronic physical conditions). It also makes it difficult to interpret differences between patients’ and F/F reports of involvement. Second, the F/F perceptions captured in this study were based on a small self-selected sample of F/F whose experiences may not be transferable to others engaged in supporting patients with a self-care intervention for depressive symptomatology. These qualitative results should be considered exploratory. Third, discrepancies between patient and F/F reports of support with the self-care intervention may be due in part to recall bias on the part of F/F as they were interviewed six months to one year after patients were asked about F/F involvement. Fourth, the analyses linking tool adherence to F/F support were cross-sectional; causality cannot be inferred.
Implications for clinical practice and future research
Our study findings suggest that patients engaged in a self-care intervention for depressive symptoms may benefit from F/F involvement in the self-care intervention. Our findings further suggest that F/F may welcome such involvement, especially if their role includes engagement in mutually beneficial activities. However, given our global measure of F/F involvement in the self-care intervention our study did not capture the actions, gestures or sentiments patients perceived to constitute F/F involvement in the self-care intervention. Future research should account for this limitation by developing and testing measures aimed at capturing the type and frequency of specific self-care intervention support (e.g. help with goal formation; participation with joint activities; overall encouragement of tool use) from the perspective of both patients and F/F.
While our study examined the relationship between F/F involvement in a self-care intervention, and patient use of self-care materials no prescribed role was developed to guide F/F involvement. Given that F/F involvement in the self-care intervention appeared to benefit patients, and F/F seemed to welcome more direction and feedback, future research should explore the impact of a more prescribed F/F role on patients and F/F. This could include developing and testing self-care interventions that encourage patients and F/F to discuss care expectations together, and negotiate a role for F/F. Encouraging this form of dialogue has been found to be of benefit to F/F, health providers, and patients managing health conditions.4,10,23,44–48 In light of the positive findings from this study, examining the impact of a prescribed role for F/F for patients engaged in a self-care intervention for depressive symptoms appears warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fonds de la Recherche du Québec—Santé (FRQS) [grant #16384] May 2009—April 2013. Erin Strumpf was supported by a Chercheur Boursier Junior 1 from the Fonds de la Recherche du Québec—Santé (FRQS) and the Ministère de la Santé et des Services sociaux du Québec. Maida Sewitch was supported by a Chercheur Boursier Junior 1 from the Fonds de la Recherche du Québec—Santé (FRQS).