
Abstract
Objective
Mental illness is highly prevalent among people living with HIV. Poor mental health is linked to HIV disease progression, making the treatment of mental illness alongside HIV essential. While the benefits of exercise on the physical health of people living with HIV are well established, the effect of exercise on mental health in this population is less examined. Therefore, this study aimed to conduct a systematic literature review of the effects of exercise on mental health in people living with HIV.
Methods
A search of electronic databases (PubMed, Web of Science, PsycINFO) through 30 November 2016 was completed. The methodological framework for scoping studies was used to conduct the review process. RISMA guidelines were used to report the results.
Results
The search resulted in 2273 articles and 52 were determined to be relevant. After review of the full text of potentially relevant studies, 24 studies were included for the analysis.
Discussion
Both aerobic and resistance exercise have independent and combined positive effects on various indicators of mental health in people living with HIV. Major limitations include high attrition rate, small sample size, and poor study designs. Higher quality studies with more diverse populations such as women, older adults, and transgender individuals are required.
Introduction
Globally, 36.7 million people were living with human immunodeficiency virus (HIV) at the end of 2015 and, in 2015, approximately 2.1 million people became newly infected. 1 HIV infection can now be considered a chronic condition in countries where antiretroviral therapy (ART) is available and accessible to people living with HIV (PLWH). In fact, the HIV mortality rate dropped by 94% from 1996 to 2006 in countries with high rates of access to ART; 2 and a study of HIV-infected adults in the United Kingdom has shown that this life expectancy improvement is mainly attributed to CD4+ cell count restoration and viral load suppression achieved through ART adherence. 3 Optimal ART adherence not only increases the life expectancy of PLWH, but also decreases the HIV transmission risk dramatically.4,5
As a chronic condition, HIV is often accompanied by a high prevalence of co-occurring mental illness. For example, in the United States, it is estimated that 16% of those with HIV have a comorbid anxiety, while up to 36% may have comorbid depression.6–8 In fact, in the United States, the prevalence of depression is estimated to be three times higher among PLWH compared to their seronegative counterparts. 9 Similarly, studies conducted with newly diagnosed HIV-infected adults from South Africa 10 and Cameroon 11 show that 55% and 63% of the patients were suffering from depression, respectively. These high rates of depression are particularly concerning because negative affective states have been linked to poor medication adherence and the clinical progression of the disease.12–14 More specifically, a meta-analysis of cross-sectional studies, which examined the association between depression treatment and ART adherence, reported that the odds of ART adherence is 83% better for those being treated for depression. 14 Moreover, a review of longitudinal studies conducted from 1990 to 2007 indicated that poor mental health was associated with higher viral load levels, a decline in CD4+ cell count, and an increased risk of mortality. 13
Although the specific biological mechanisms involved in these relationships are currently unknown, it is clear that disease progression is impacted by negative affective states and depressive symptoms. As such, there is a strong rationale to investigate interventions that are designed to improve mental health in PLWH. Exercise may be one such intervention as some recent evidence suggests. Specifically, a recent meta-analysis on the effect of aerobic exercise on the health of PLWH found significant improvements in quality of life and depressive symptoms. 15 However, another meta-analysis was inconclusive on the effect of resistance exercise on mental health of PLWH. 16 Importantly, both meta-analyses were limited to randomized controlled trials and exercise interventions that were carried out at least three times per week for at least 4 weeks.15,16 Therefore, the purpose of this paper was to further investigate the effects of aerobic and resistance exercise on mental health outcomes in PLWH by identifying and critically reviewing any published study to date. In order to demonstrate the scope of the studies conducted so far, the studies in this review were not limited by study design (i.e. both randomized controlled trials and quasi-experimental), or level of exercise frequency, intensity, or duration.
Methods
Eligibility criteria
The inclusion criteria were determined prior to the literature search. Studies had to include the following: (a) participants were people living with HIV/AIDS, (b) exercise (i.e. resistance, aerobic exercise or combined) was used as an intervention, (c) at least one mental health outcome was measured pre-to-post intervention, and (d) published in English. Both experimental and quasi-experimental designs were included. We also included interventions that combined aerobic or resistance exercise with other movement modalities (e.g. Tai Chi) or nonexercise modalities (e.g. pharmacological interventions or nutritional interventions). The methodological framework for scoping studies was used to conduct the review process. 17 PRISMA guidelines were used to report the results. 18
Search strategy
A systematic review of published (i.e. in print and online) studies testing the effects of exercise on mental health of PLWH was conducted. An electronic database literature search through 30 November 2016 was conducted using “PubMed”, “Web of Science”, and “PsycINFO”. The keywords used for the search were (“hiv” OR “aids”), (“exercise” OR “physical activity” OR “aerobic” OR “resistance” OR “walk”), (“mental health” OR “depression” OR “depressive symptoms” OR “quality of life” OR “mood” OR “fatigue” OR “anxiety”) and the syntax was adapted for each database accordingly. A manual search through the references of the review articles was also conducted to include all the relevant literature.
Data extraction and synthesis
The information related to study eligibility was extracted by one reviewer. In case of any uncertainty about whether an article met the inclusion criteria, the article was discussed by the coauthors to determine exclusion or inclusion in the review. The following information was extracted for each included study: (a) characteristics of the participants; (b) characteristics of the exercise intervention (e.g. type, frequency, intensity, duration); (c) characteristics of the control condition; (d) type of outcome measured (e.g. depressive symptoms, mood, anxiety, quality of life); (e) the instruments administered to measure the outcomes; (f) study design; and (g) program attrition rate (i.e. the percentage of participants who dropped out). Formal assessment of risk of bias was not included due to variability in study design and the limited number of studies meeting the inclusion criteria. 19
Results
The search resulted in 2273 articles. After excluding duplicates across the databases and articles that clearly did not match the inclusion criteria, 52 were determined to be relevant. Of these, 24 studies were eligible and are included in this review. The search procedure and study selection methodology are shown in Figure 1, and the participants’ characteristics, study designs, and outcomes are presented in Table 1. Characteristics of the intervention and control group are presented in Table 2. The results are categorized by mode of the exercise interventions.
The search procedure and study selection methodology. Participants’ characteristics, study designs, and outcomes. RCT: randomized controlled trial. NR: not reported. AE: aerobic exercise group; RE: resistance exercise group; CON: control group; EX: exercise group; QOL: quality of life. POMS: profile of mood states. CES-D: Center for Epidemiological Studies-Depression Scale. Characteristics of the intervention and the control group. The total time is the time of each session excluding warm-up and cool-down. MHR: maximum heart rate; HRR: heart rate reserve; LT: lactate threshold; RM: repetition maximum; bpm: beats per minute; None: no control group; Nonexercise: the control group did not participate in any sessions and were asked to continue with their activities of daily living; NR: not reported.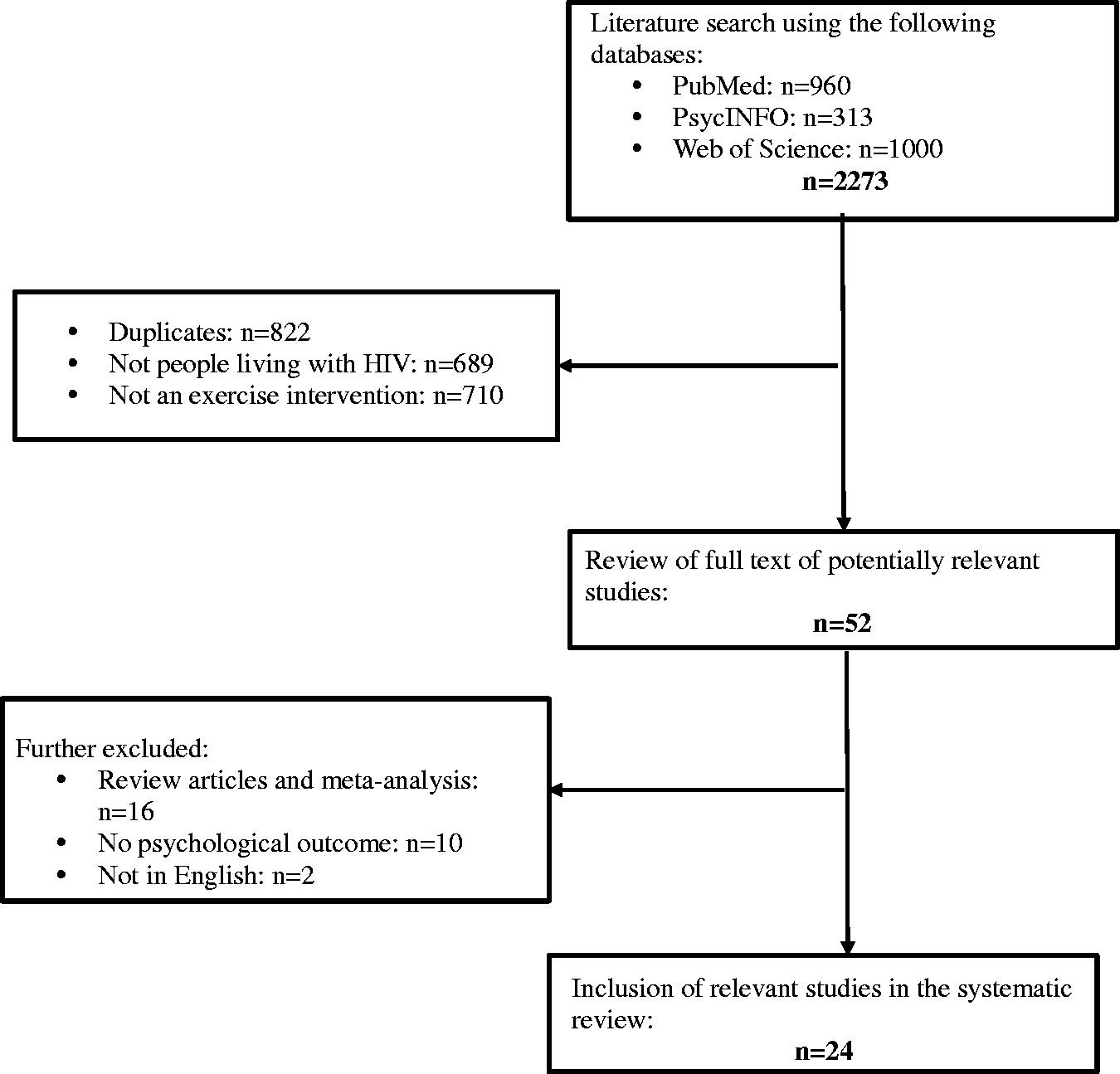


Aerobic exercise interventions
Nine studies20–28 examined the effect of aerobic exercise on mental health of PLWH. Researchers tested both continuous and interval exercise at different intensities. Three studies20,21,26 examined interval aerobic exercise and the other six22–25,27,28 tested continuous aerobic exercise. The intensities tested were low,21,27 moderate,20,23,24,26–28 and vigorous.21,22,24–26 Interventions ranged from 5 weeks 20 to 24 weeks,21,27 with the duration of each exercise session lasting between 20 min 23 and 60 min.24,27 Exercise frequency was three times per week across all experiments except for one study, 28 which had the participants exercise once per week at the research site and three times at home.
Four studies23,24,27,28 measured quality of life (QOL), four20–22,26 measured depressive symptoms, two20,21 measured levels of anxiety, and one 25 measured affect, life satisfaction, and self-efficacy.
Two studies20,22 used the profile of mood states (POMS), 29 one study 21 used the general health questionnaire, 30 and one 26 used the Montgomery–Asberg 31 to measure the anxiety and depressive symptoms. Additionally, the Center for Epidemiological Studies-Depression Scale (CES-D) and the Beck Depression Inventory (BDI)32,33 were used to measure the depressive symptoms. 22 Affect was measured 25 with the Positive And Negative Affect Schedule (PANAS), 34 life satisfaction with the Satisfaction With Life Scale (SWLS), 35 and self-efficacy with the Physical Self-Efficacy Scale (PSES). 36 QOL was measured 24 with a subset of a QOL questionnaire, 37 the Sickness Impact Profile (SIP), 38 the Medical Outcome Study in HIV-infection (MOS-HIV), 39 the Duke Activity Status Index (DASI),23,40 the World Health Organization Quality of Life (WHOQOL),27,41 or the Medical Outcome Survey 36-item Short-Form Health Survey (SF-36).28,42
The findings of these studies are mixed while the majority of the studies show significant improvement in one mental health outcome. In one study, 20 seropositive controls scored significantly higher in anxiety and depressive symptoms at the 1-week post HIV status notification when compared to the seropositive exercisers. Other researchers22,25 reported significant improvements in the depressive symptoms, significantly higher positive mood, higher life satisfaction, and lower negative mood in the exercise group when compared to the control group. However, in two other studies,21,26 the researchers reported no significant change in anxiety and depressive symptoms. Out of the four studies that measured QOL, one 23 reported significant improvement only in the health subscale of QOL in the exercise group compared to the control. Two27,28 reported significant improvement in the overall QOL domain in the exercise group compared to the control. The other one 24 reported significant improvement in QOL for both exercise groups compared to the control with no significant differences between the exercise groups (i.e. vigorous vs. moderate intensity).
On the whole, aerobic exercise seems to be beneficial for mental health of PLWH. However, when drawing conclusions from these results, it is important to consider the shortcomings of the current body of research. First, the attrition rate varies across the studies. Specifically, the attrition rate ranged from 3% in two studies25,27 to 76% in another study. 21 Second, participants were 100% men in two studies,20,25 and between 40% and 96% men in other studies.21–24,26–28 Third, two studies21,26 did not have a control group and the contact time in the control group was not matched in two other studies.23,25 Lastly, only one study 22 controlled for HIV disease stage and balanced the groups based on a number of potentially confounding variables (e.g. social support, perceived stress, anti-depressant use, and HIV-related symptoms).
Resistance exercise versus aerobic exercise interventions
There is only one study 25 that tested the effects of resistance versus aerobic exercise. In this study, 25 mental health status was compared between aerobic exercise, resistance exercise, and an unsupervised stretching control group. The aerobic exercise group exercised continuously at moderate to vigorous intensity, while the resistance exercise group completed progressive resistance exercise. Affect, life satisfaction, and self-efficacy was compared between groups pre- and post-intervention. Results indicated that both the aerobic and resistance exercise groups had significantly higher positive affect, higher life satisfaction, and lower negative affect when compared to the stretching control group, with significantly greater improvements found in the aerobic group. Of note, the participants were all men and there were more participants diagnosed with AIDS in the resistance exercise group compared to the aerobic group.
Resistance exercise interventions
There are four studies25,43–45 that examined the effect of resistance exercise on mental health of PLWH. All of these studies reported administering progressive resistance exercise. One study 44 had two resistance exercise groups. In this study, 44 one group used resistance bands and initiated the exercise protocol at 1 set of 25 repetitions to fatigue and progressed to 2–3 sets of 8–12 repetitions to fatigue. The other group used bodyweight (i.e. no resistance band) and performed the same exercises in a group setting. Another study, 43 progressed the participants from 1 set of 15 repetition maximum (RM) to 3 sets of 12 RM. Lox et al. 25 had participants complete 3 sets of 10 RM throughout the intervention. One study, 45 however, has not reported the details of the resistance exercise protocol. The frequency of the exercise sessions were three times per week in two studies,25,43 and six times per week in another. 44 The length of the interventions were 1225,44,45 to 16 weeks. 43
Three studies measured QOL.43–45 One study 25 measured mood, life satisfaction, and physical self-efficacy. QOL was measured through the WHOQOL, 41 the Euro QOL-5 Dimensions, 46 and the SF-36. 42 Two studies,43,45 reported significant improvement in QOL for the exercise group compared to the control group, while Hamid et al. 44 reported no significant differences in QOL between the two exercise groups. Additionally, Lox et al. 25 reported significant improvement in mood and life satisfaction for the exercise group compared to the control.
Of note, two studies did not have a control group,43,44 and the contact time in the control group was not matched in one study. 25 Except for one study 43 with perfect attendance, the attrition rate ranged from 3% 25 to 60%. 45 Participants were 100% men in two studies,25,44 73% men in one, 43 and 29% in the other. 45
Combined aerobic and resistance exercise interventions
There are six studies47–52 that combined aerobic and resistance exercise. The aerobic exercise protocols tested were low, 47 moderate,48–51 and vigorous. 52 The duration of aerobic exercise sessions were between 20 49 and 45 min. 52 The resistance exercise protocols were mostly initiated at 50–60% of 1 RM and progressed to 80% of 1 RM.49–51,52 One study, 47 however, used resistance bands and one study 48 maintained the resistance at 12 RM during the entire intervention. The frequency of the sessions were 247–50 or 351,52 times per week. All studies compared combined aerobic and resistance exercise with a control group only, except for one study, 47 which had two exercise groups (i.e. combined aerobic and resistance exercise and a group performing Tai Chi movements) and a control group.
Three studies47,51,52 asked the control group not to participate in any sessions and to continue with their activities of daily living. Other studies had participants attend an AIDS-related support group, 50 attend sessions which included reading books, talking, watching television, or participating in other sedentary behaviors, 48 or attend an unsupervised walking program and a monthly forum. 49
Two studies47,48 measured mood. Four studies47,49,50,52 measured QOL. Additionally, Galantino et al. 47 measured spirituality, Fillipas et al. 49 measured self-efficacy, and Rojas et al. 50 measured psychological well-being. Jaggers et al. 48 measured psychological distress, self-reported HIV symptoms (e.g. insomnia, pain, fatigue) and salivary cortisol, and Gomes et al. 51 measured life satisfaction. Mood was measured with the brief POMS (POMS-30). 53 QOL was assessed with the MOS-HIV 39 and a QOL questionnaire developed for Spanish speakers undergoing treatment for drug addiction. 54 Spirituality was measured with the Spirituality Well-being Scale (SWB), 55 and self-efficacy was measured through the General Self-Efficacy Scale. 56 Self-reported HIV symptoms were measured with the HIV Symptom Distress Scale (SDS), 57 psychological stress was measured with the Perceived Stress Scale (PSS), 58 psychological well-being was measured through the Symptom Checklist Revised (SCL-90), 59 and life satisfaction was measured through the Life Satisfaction Index. 60
Except for one study, 52 which did not report significant differences between groups, all others show significant improvement in mental health status. Three studies47,49,50 reported improvement in QOL for the exercise group compared to the control group. Specifically, improvements are reported in emotional well-being, physical strength, energy, overall health, and cognitive function subscales of QOL.49,50 Additionally, Fillipas et al. 49 reported significant improvement in self-efficacy in the exercise group compared to the control group. Jaggers et al. 48 reported a significant reduction in the depressive symptoms and mood disturbances as well as significant decrease in salivary cortisol levels in the exercise group. Interestingly, the control group scored significantly higher in perceived stress post intervention, suggesting a protective role of exercise against stress. 48 Significant improvements in life satisfaction are also reported in the exercise group compared to the control. 51
Three studies47,49,50 had participants exercise in groups, and two studies50,51 did not conduct random assignments. Moreover, in one study 51 the control group comprised both the waitlist and the nonadherent participants in the exercise group. Participants were 100% men in three studies,47,49,52 and between 59% to 76% men in others.48,50,51 The attrition rate ranged from 12% 49 to 47%. 48
Combined exercise and nutritional supplementation/counseling interventions
There are four studies61–64 that combined exercise and nutritional supplementation or counseling. In one, 61 participants were randomized to 14 weeks of either whey protein supplementation group (1.0 g/kg/day of whey protein), progressive resistance exercise group, or combined whey protein supplementation and progressive resistance exercise group. Prior to the intervention, participants attended a 6-week pre-intervention assessment period to serve as their own control. In another one, 62 researchers tested the effect of a weight loss program on psychological parameters in a 12-week longitudinal study.
Two other studies63,64 tested the effect of combined aerobic exercise with counseling compared to a control group. In one, 61 the exercise protocol was progressive resistance exercise. In the other, 62 the exercise protocol was a combination of aerobic and progressive resistance exercise and participants attended group nutrition education classes once a week as well. In the studies with aerobic exercise intervention,63,64 participants either had to complete moderate intensity aerobic exercise three times per week combined with counseling once a week 64 or had to attend an hour gym class three times per week combined with nutritional counseling once per month. 63
QOL was measured through the MOS-HIV 39 and the SF-36.42,61–63 Both the Brief Symptom Inventory (BSI) 65 and the BDI 32 were used to measure the depressive symptoms.62,64 The 5-item SWLS 35 measured overall happiness, and the 13-item Sense of Coherence Scale 66 was used to measure individual’s beliefs regarding the fairness, manageability, and meaningfulness of their circumstances. 62
All of the studies61–64 indicated significant improvement in the mental health status with exercise. Specifically, Agin et al. 61 reported that the progressive resistance exercise group showed significant improvement in subscales of physical activity, vitality, and general health perception of QOL and the combined resistance exercise and whey supplementation group significantly improved on the social functioning subscale of the QOL. Interestingly, there was a significant decline in the physical activity subscale of QOL for the whey protein supplementation group. Engelson et al. 62 reported that QOL scores significantly improved in all the dimensions measured, except for general mental health on SF-36 and anxiety subscale on BSI. Aweto et al. 64 reported significant improvement in the depressive symptoms for the exercise group while there was no change for the control group. Finally, Ogalha et al. 63 reported significant improvement in general health, vitality, and mental health subscale of SF-36 in the exercise group compared to the control group.
Importantly, attrition rate ranged from 10% 63 to 36%. 62 One study 62 did not have a control group and the contact time in the control group was not matched in two other studies.63,64 Participants were mostly women in three of these studies (i.e. 100% in two,61,62 and 70% in another.) 64
Combined exercise and pharmacological treatment
There are two studies67,68 that looked at the effect of combined exercise and testosterone treatment. The first one 67 used a four-group double-blind randomized controlled trial design. The groups were (1) placebo, no exercise; (2) testosterone replacement, no exercise; (3) placebo combined with progressive resistance exercise; and (4) testosterone combined with progressive resistance exercise. Testosterone treatment was 100 mg per week of testosterone enanthate. In the second study, 68 participants were randomized to either a nutrition intervention (i.e. increased caloric intake to 50 kcal/kg/day and increased protein intake to 1.6 g/kg/day) with placebo pills, a nutrition intervention with 10 mg of oxandrolone twice daily, or a nutrition intervention with progressive resistance exercise.
Both studies67,68 used progressive resistance exercise. Both the frequency of the sessions (i.e. three times per week) and the length of the interventions (i.e. 16 weeks in the first one 67 and 15 weeks in the second one 68 ) were similar.
In the first study, 67 QOL was measured through a nonspecified self-report questionnaire including multi-item measures of physical functioning, general health perception, emotional well-being, and cognitive and sexual functioning. In the second one, 68 QOL was measured through the subscale of physical functioning from SF-36. 42
The findings of these two studies are mixed. Bhasin et al. 67 did not report any significant differences in QOL measures, while Shevitz et al. 68 reported significant improvement in QOL in the combined nutrition intervention and resistance exercise group pre- to post-intervention with no difference between the groups. Attrition rate was also different across these studies. Bhasin et al. 67 had an attrition rate of 20% while Shevitz et al. 68 had an attrition rate of 6%. Participants were mostly men in these two studies (i.e. 100% men in one 67 and 70% men in the other). 68
Discussion
The effects of both aerobic and resistance exercise on mental health have been tested, with positive results shown independently for each type of exercise, at different intensities, and when they are combined. Importantly, no adverse effects were reported with exercise in this population. These results are also supported by the recent meta-analytic research on the beneficial effects of aerobic exercise with PLWH 15 and other meta-analysis on the effect of exercise on mental health with the general population. 69 However, it would be difficult to draw a detailed exercise recommendation for improvement of mental health from the reviewed studies due to limitations of the current body of research.
Many of the studies had a small sample size and were inadequately powered. For example, sample size ranged from 15 43 to 160. 45 Many experiments also reported a high level of attrition with seven studies reporting more than 30%.21,26,28,44,45,48,62 Unfortunately, it is not clear why some studies experienced such high attrition, but it could be attributable to the exercise protocol (i.e. frequency, intensity, duration, and type), lack of remuneration, or logistical barriers, such as scheduling or access. The high attrition rate clearly biases these findings because it is unknown if the results found to date only represent a unique subset of PLWH who completed the study’s requirements.
Another limitation is the quality of the reviewed studies. Six21,26,43,44,62,68 of these studies did not have a control group and two studies50,51 did not perform random assignment. These potential threats to internal validity of the experiments make it difficult to draw inferences from the results or link the outcome to the intervention. 70 For instance, during the course of the intervention, a change in an unobserved variable such as progression of the HIV disease could have confounded the results. Also, lack of randomization can have detrimental effects on the outcome. Without random assignments, it is not clear if the groups were different in regards to the confounding variables related to physical activity behavior (e.g. self-efficacy) and, therefore, responded differently to the intervention.70,71 Moreover, the contact time between groups was not matched in five studies,23,25,49,63,64 and four studies44,47,49,50 utilized group exercise; while another used group nutrition classes. 62 Given the well-known effects of social support on mental health,72,73 it is not clear if the positive effects shown were an independent effect of the exercise, a consequence of social support by other participants, or a combination of those effects.
The current studies are also limited by the sampled population characteristics. Participants were aged between 30.5 to 46.2 years and mostly men living with HIV. In fact, only four studies45,61,62,64 were on average mostly women (i.e. 85% women). Six studies20,25,44,47,49,52,67 were only men (i.e. 100% men), and the majority of the participants (i.e. >50%) were men in 12 other studies.21–24,26,28,43,48,50,51,63,68 Considering that women, transgender individuals, and older adults living with HIV are under-represented in the current research, it is imperative that future trials consider including all genders and age groups. Additionally, many studies did not acknowledge whether or not participants were seeking mental health treatment, or whether there were baseline differences with respect to stages of HIV disease. This is clearly problematic given that poor mental health might be confounded with symptoms of physical illness related to HIV and neuropsychological impairment. 74
Finally, nearly half of the research included in this review has been conducted more than 10 years ago, during which important gains have been made in the advancement of HIV treatment and care. It is unlikely that the results of a study examining the psychological benefits of exercise more than 10 years ago would be easily replicated now. More importantly, these studies may represent a different sample of PLWH compromising their generalizability to the current population of PLWH.
Recommendations for future research
The current body of work suffers from several consistent methodological limitations. Despite this, there is a clear rationale to continue to examine exercise as a tool to help with mental health symptom management (e.g. depressive symptoms, anxiety, and components of QOL) for PLWH, as most of the studies show significant improvement in these symptoms. Importantly, one recent study with seronegative individuals living with depression reported that the majority had an interest in participating in an exercise program for symptom management and mood enhancement. 75 Although these preferences need to be reexamined with seropositive individuals, it seems that an individualized exercise program might be a viable approach for improving mental health.
Future studies should use intent-to-treat analysis in order to include all the randomized participants in the final analysis, 76 and help with deeper understanding of the effectiveness of exercise interventions.76,77 The field can also benefit from future meta-analyses to help detect the bias in the current research and increase the precision of the results specifically with inconclusive or underpowered trials.78,79 Also, researchers should actively seek out and include more diverse populations such as women, transgender individuals, and older adults and account for confounding variables such as stages of HIV disease, baseline psychological profiles of the participants, and/or social support. Future research could also consider using activity monitors to minimize the burden of access to the research site for the participants. Finally, more adequately powered randomized clinical trials are required to fully understand the acute and long-term effects of exercise dose (e.g. intensity, frequency, volume) on mental health outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.