
Abstract
Objectives
This study explores perceptions of US Veterans Affairs (VA) and non-VA healthcare providers caring for Veterans with heart failure (HF) regarding Veteran knowledge and motivations for dual use, provider roles in recommending and coordinating dual use, systems barriers and facilitators, and suggestions for improving cross-system care.
Methods
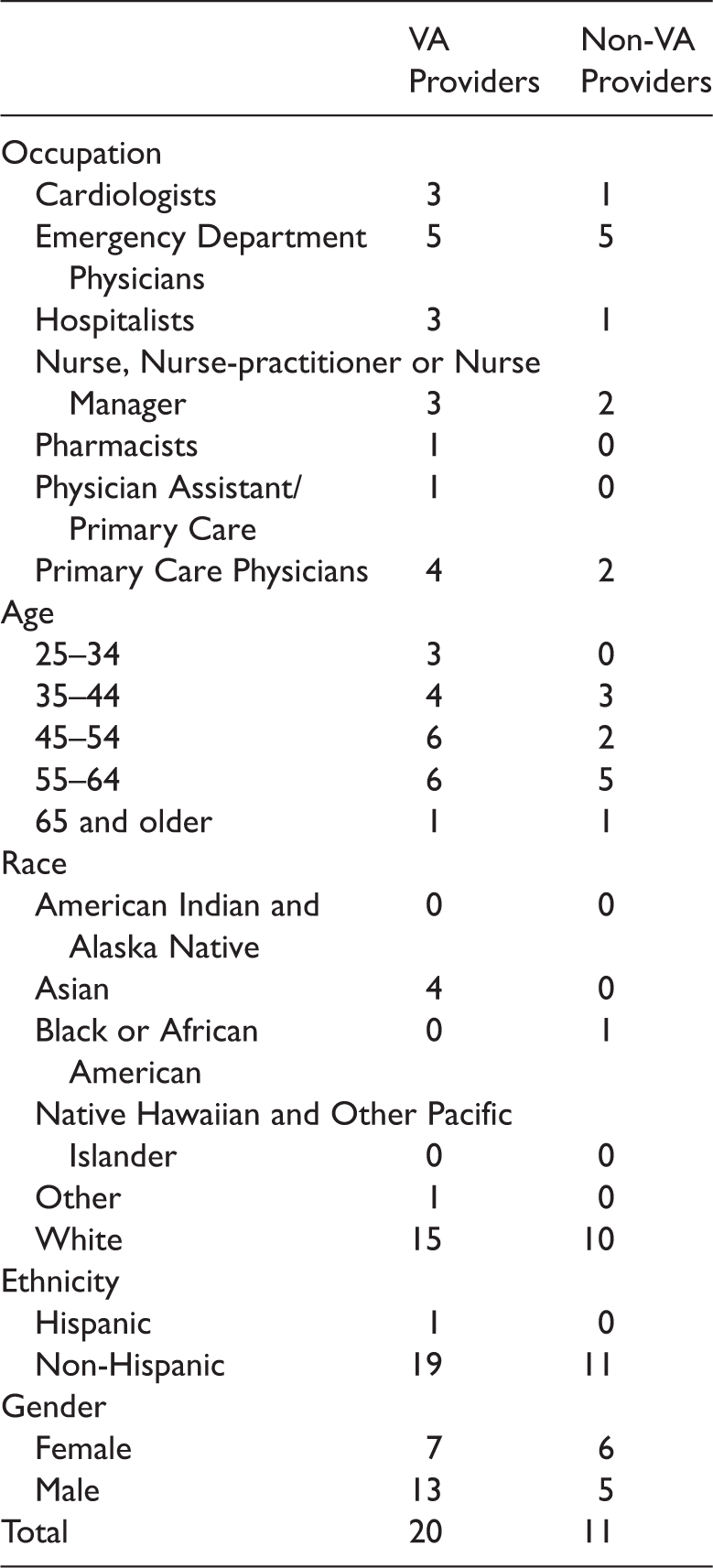
Twenty VA and 11 non-VA providers participated in semi-structured interviews, which were analyzed using parallel qualitative content and discourse analysis.
Results
VA and non-VA providers described variable HF knowledge and self-management among Veterans, and both groups described the need for improved education addressing medication adherence, self-care, and management of acute symptoms. Both groups described highly limited roles for providers in shaping choices surrounding dual use. VA and non-VA providers had significantly different perceptions regarding the availability, quality, and effectiveness of VA HF services. Multiple non-VA providers expressed frustration with and difficulty in contacting VA providers, accessing records, and making referrals into the VA system. Suggestions for improved care focused on patient education and care coordination.
Discussion
Dual healthcare system use for Veterans is increasingly common. Similarities and contrasts in perceptions of VA and non-VA providers are instructive and should be incorporated into future policy and program initiatives.
Introduction
Heart Failure (HF) is a highly prevalent chronic medical condition prone to frequent acute exacerbation that currently affects an estimated 6.5 million U.S. adults. 1 Heart failure causes approximately 1.1 million hospitalizations and 3.4 million ambulatory care visits each year at an estimated annual cost of $30.7 billion. 2 Among patients hospitalized for HF, almost one quarter (i.e., 23.8%) are seen in an emergency department (ED) within 14 days of hospital discharge, and one-fifth (20.7%) are readmitted within 30 days of hospital discharge. 3 Approximately half of all HF patients die within five years of diagnosis, and one in one deaths have included HF as a contributing cause. 4 Heart failure is also highly prevalent in the Veteran population, where it is a frequent cause for hospital admission and one of the most frequent causes of unplanned hospital readmission. 5
For most Americans, health care is scattered across multiple providers and health care systems. While care across settings is often necessary and desirable, emerging evidence suggests that such fractured care can be less efficient and less safe.6–9 Within the U.S. Veterans Health Administration (VA), dual healthcare system use (dual use) occurs when Veterans enrolled for VA care also receive care from non-VA providers or healthcare facilities, and it is particularly common. Weeks and colleagues examined dual use for cardiovascular disorders among Veterans enrolled in VA care in New York State and found that younger Veterans relied solely on VA hospitals for 41% of their care, while older Veterans relied solely on VA hospitals for only 27% of their care. 10 Among Medicare HF patients rehospitalized within 30 days, studies estimate that 19% are readmitted to a different hospital the second time around. 11 Also, a recent study of Veterans with HF found significantly higher rates of ED visits, hospitalizations for HF, and hospital readmissions among dual users as compared to single-system users. 12 Thus, the VA population is a reasonable one in which to study the phenomenon of cross-system care using HF as a model chronic disease.
The reasons for cross-system care, or dual use, are complex and include patient, provider, and systems-level drivers. Dual use is important in the VA given recent passage of the Veterans Access, Choice, and Accountability Act of 2014 (VACAA), which has significantly increased the care of Veterans in non-VA systems, including an expected expansion of non-VA hospitalizations. 13 This line of investigation is also timely given active Center for Medicare and Medicaid Services (CMS) programs focused on improving hospital care quality and to promoting population health management. These actions include penalties related to all-hospital 30-day readmission rates and ongoing Accountable Care Organization (ACO) demonstration projects. 14 Thus, examination of cross-system care is relevant both in VA and also outside the Veterans Health Administration as well.
To date, most studies of dual use have been retrospective studies using administrative data.6,15–19 While a few studies have assessed drivers of dual use from the patients' perspective, 20 we are aware of no studies that assess drivers of dual system use from the perspective of providers in both VA and non-VA settings. In order to address this gap in knowledge, we performed a qualitative research study with a group of VA and non-VA providers as a source of information to better understand different providers' perspectives regarding Veteran knowledge and motivations for dual use, provider roles in recommending and coordinating dual use, systems barriers and facilitators of dual use, and suggestions for improving systems of care.
Methods
Ethics approval
Initial human subjects' protection approval was obtained from the Department of Veteran Affairs (VA) Central Institutional Review Board (CIRB), followed by review from the local VA Research and Development (R&D) Committee. The first CIRB approval (12 January 2013) was followed by approved Continuing Reviews (10 March 2014, 10 March 15 and 10 March 16) as part of a larger mixed methods study.
Study participants
Characteristics of study participants.
Semi-structured interviews
Interview guide.
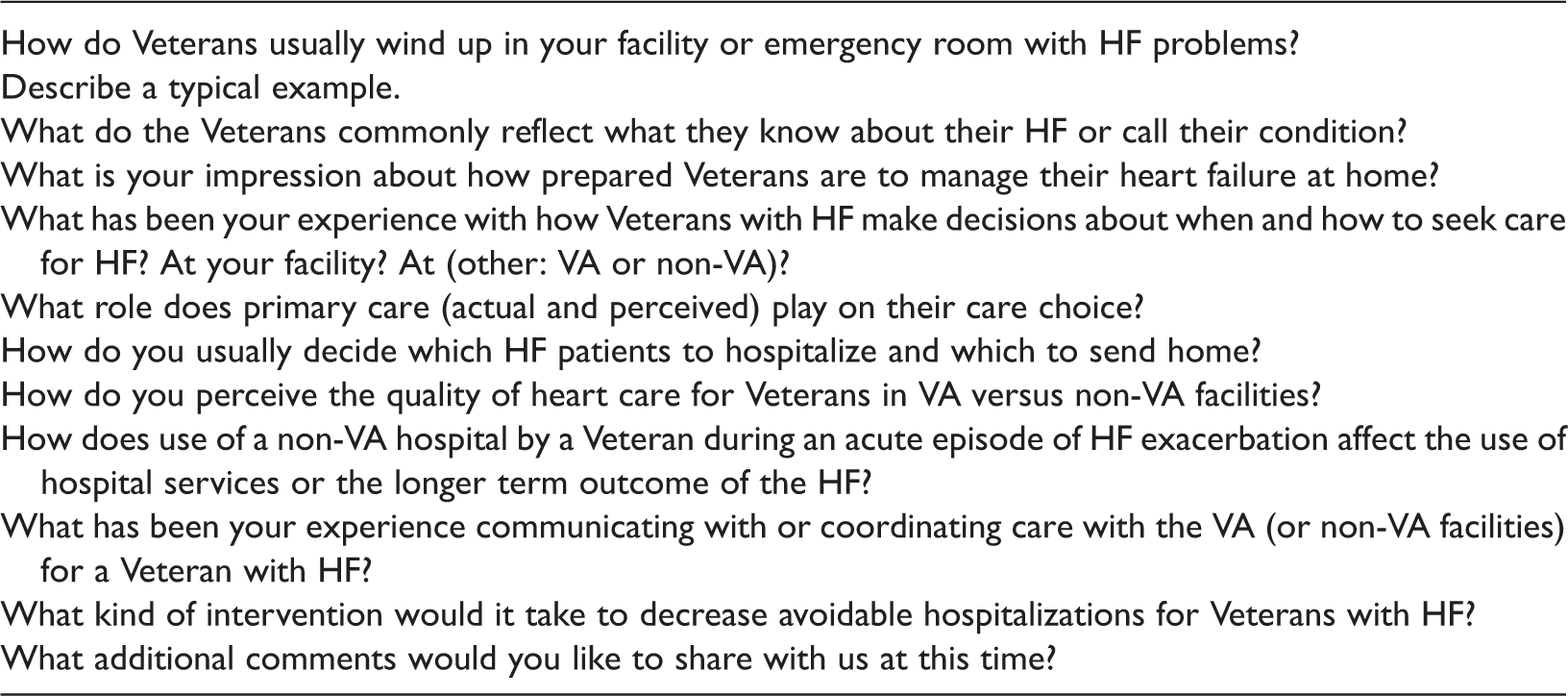
VA: Veterans Affairs; HF: heart failure.
In keeping with an approach developed for sociological methods, inter-rater agreement was negotiated by consensus using a matrix that standardized the units of text between the two parallel qualitative methods used by the coders: qualitative content analysis and discourse analysis. 24 This approach to inter-rater agreement emerges from an approach to qualitative data analysis that uses principles of inductive reasoning that support the parallel development of code types for a negotiated consensus for data analysis and interpretation. 25
Data analysis
Each cohort of provider interviews was coded separately into perceptions of VA providers and non-VA providers by a coder using qualitative content analysis and a second coder using discourse analysis. Our choice to combine content analysis in parallel with discourse analysis warrants some discussion. Hsieh and Shannon explain that qualitative content analysis “is defined as a research method for the subjective interpretation of the content of text data through the systematic classification process of coding and identifying themes or patterns.” 26 In that classification, our approach is considered summative content analysis (pp.1283–1284), as it goes beyond quantifying content in the text to examining its context as part of its interpretation. As summarized by Schreier, content analysis in quantitative research is usually considered a method for data collection to be counted, while in qualitative research content analysis counts as a method for data exploration and analysis. 27 This method organizes and elicits meaning from the data collected and draws conclusions from a process of examining the context of what was said, establishing categories and compiling results. 28
Though there are a variety of approaches to discourse analysis, we used the type of discourse analysis that focuses on ways of speaking and that incorporates pragmatics, or an emphasis which takes into consideration the contexts surrounding the speakers from which inferences and references are drawn. 29 In this type of discourse analysis, coding identifies categories of language used in interviews that denote how the speakers think about their world, how they position themselves, the footing or stance they take in relation to themselves, others and actions they take, and choices in speaking that signal identity, beliefs, and attitudes. As an example, for the code “positioning”, in examining transcripts line by line, pronoun use and exclusions frequently identified how providers positioned perceptions about themselves and the Veterans. In referring to Veterans as “they,” Veteran HF decisions were portrayed as internally related to listed symptoms, with little reference to conditions at home, resources, family, or contextual factors in which symptoms escalated and decisions were made. By contrast, in referring to Primary Care or hospital services, providers used “we” to describe the array of services offered, even when the services were inaccessible or not their service, positioning themselves as extensions of the institution.
Examples from discourse analysis.
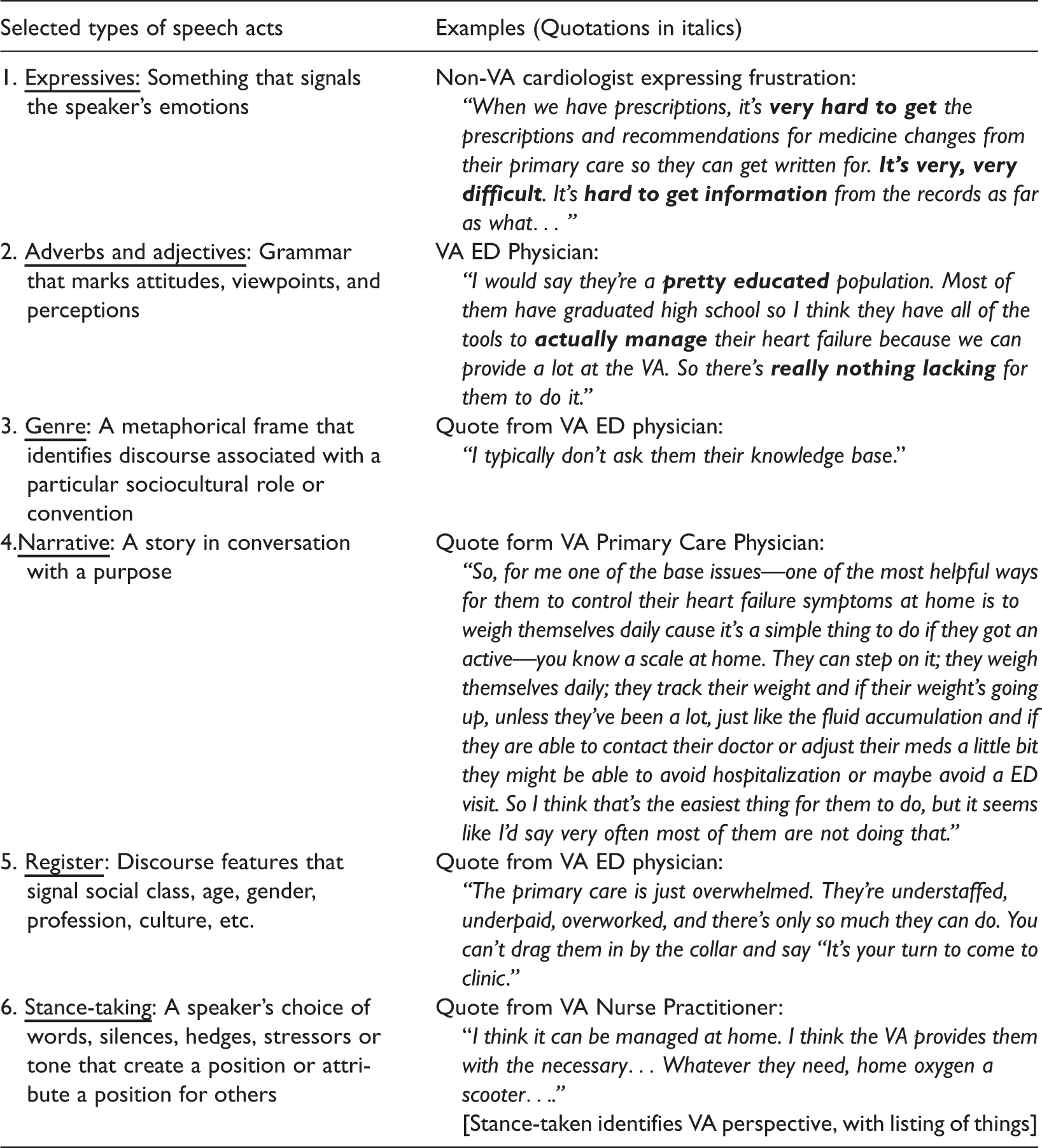
VA: Veterans Affairs; HF: heart failure; ED: emergency department.
Key themes related to dual system use as articulated by VA and non-VA healthcare providers.
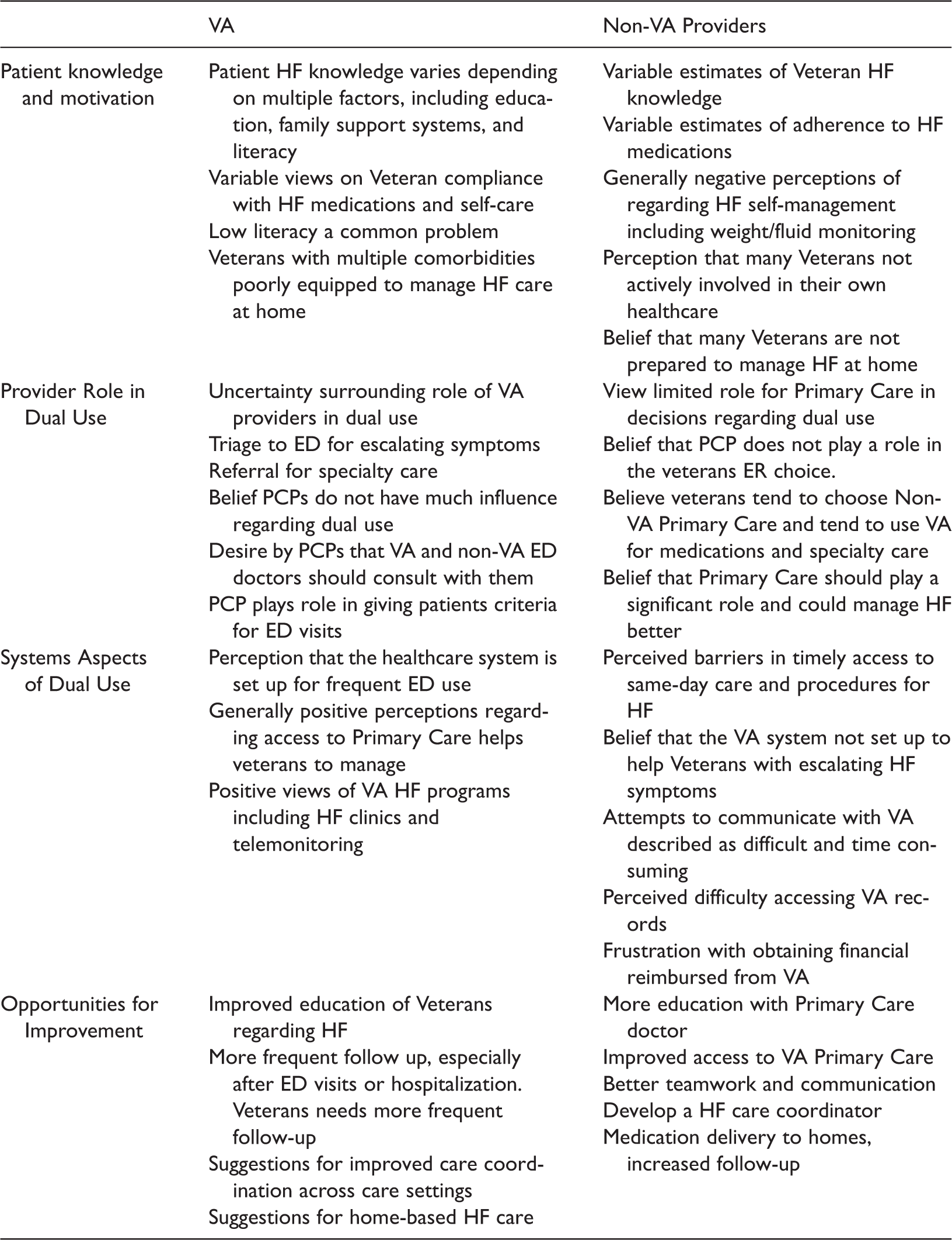
VA: Veterans Affairs; HF: heart failure; ED: emergency department.
Results
Overall, VA and non-VA providers had similar ranges of perceptions regarding Veteran knowledge of HF and their motivations for dual use. Providers in both groups endorsed that the status of Veterans' understanding of their HF condition was highly variable. For instance, a VA primary care physician stated, “I would say they're a pretty educated population. Most of them have graduated high school so I think they have all the tools to actually manage their heart failure….” By contrast, a VA nurse practitioner stated, “Well, they are typically well
Both VA and non-VA providers expressed uncertainty in identifying the role they or their colleagues played in initiating or coordinating dual system use. For instance, when asked what role primary care providers played in choice of site of care for Veterans with heart failure, several interviewees asked for clarification or stated they did not understand the question. One typical VA provider responded, “…I don't think primary care plays a lot of roles.” Once clarified, several VA and non-VA primary care providers described examples limited to triage in acute exacerbation and referral for specialized procedures (regardless of site). However, one non-VA emergency provider noted that Veterans themselves seemed to use services across systems selectively: When it comes to needing prescription refills and things like that they're going to go back to the VA so they can get the medications paid for, of course. And probably more serious problems that require subspecialty care, they'll probably go back into the VA, but the [community] primary care physicians play a significant role in their care.
This role uncertainty regarding dual use suggested areas of communication between services managing the same Veterans with HF that would benefit from support and enhanced coordination. Though non-VA providers also saw little current role for primary care in improving the process of HF care, they were more likely to recommend that primary care providers should be more involved. For the most part, both VA and non-VA providers perceived the decision to hospitalize a Veteran with HF with escalating symptoms to be a matter of clinical symptoms and lab test results, with little reference to the Veteran's role in decision-making, resources, their fears or feelings.
A third area explored in interviews with VA and community providers related to systems aspects of dual use. VA providers voiced overall satisfaction with care coordination, the availability of cardiology and nurses available for education, and appreciation for the VA Care Coordination Home Telehealth (CCHT) service that is frequently used to monitor Veterans with HF.32,33 For instance, one VA primary care physician said: We also have Telehealth here at the VA which is pretty responsive, if they get patients enrolled quickly, and [we] monitor them through the phone system… I think that when patients get to be end-stage or need palliative care, I think the VA is good about getting them on hospice when needed. I think, for the most part, I haven't had a lot of problems with my heart failure patients in the VA.
While VA providers tended to believe that the VA system offered a variety of resources to meet the needs of Veterans with HF, non-VA providers offered a different perspective about VA care. Non-VA providers often felt Veterans accessed community healthcare because of difficulties accessing VA primary care or getting timely appointments for related services. One community emergency physician opined, “I think they need to have efficient, easy access to see their doctor in clinic. A nurse to follow them would be outstanding.” To some degree, these concerns unmasked lack of awareness of available VA services since the VA Medical Center serving the catchment area for this provider's ED actually did have a nurse-practitioner-led heart failure follow up clinic. Other community providers described difficulty communicating with the VA as time-consuming and frustrating. One community nurse-practitioner working in primary care stated: It is extremely frustrating. You can call, and they might call you back. Or they might not call you back. If they're on vacation, no one's covering them. And the Veterans unfortunately are staying in the hospital for many more days than what might be needed just because we can't get hold of someone to do the care that's needed or we can't get a hold of someone. So, we really struggle with contacts.
Some community providers described difficulty coordinating medications and other treatments with VA. “When we have prescriptions, it's very hard to get the prescriptions and recommendations for medicine changes from their primary care so they can get written for. It's very, very difficult,” referring to difficulty managing without access to VA medical records. Additional comments focused on difficulty obtaining VA medical records, arranging follow up testing in VA, and occasionally in obtaining reimbursement from VA for services.
Finally, patterns emerged regarding providers' recommendations for changes to improve cross-system healthcare. The most common recommendations from both VA and community providers focused on improving patient education for HF management. According to one VA emergency physician, “Well, compliance. Anything that would improve compliance and education so the patient does understand.” Many VA providers also recommended better follow-up and use of current services, such as the care Home-based Primary Care which features visiting nurses, 34 and more use of the CCHT. Both groups of providers called for more care coordination for Veterans receiving cross-system care. A comment by one community nurse-practitioner summarizes this theme: “I definitely think if we could work together as a team and do more of a team approach for the patient it would be much better. More clear communication between providers would be better.”
Discussion
Our study is one of the first to explore the perceptions of healthcare providers who collaborate in the care of patients receiving treatment across healthcare systems, and it is the first to specifically explore HF care. We observed several areas of concordance in views expressed by VA and non-VA providers. For example, both sets of providers described varied experiences in the level of HF knowledge and self-management among Veterans. Providers in both groups felt that improved patient education addressing medication adherence, self-care, and management of acute symptoms is warranted, but there was no consensus on who should provide this education. Both VA and non-VA primary care providers perceived they had limited roles in shaping choices or Veteran decision making surrounding dual use. Seemingly missing were descriptions of advanced planning or intentional counseling regarding site of care and acknowledgement of the role to be played in care coordination. Our interviews uncovered striking differences in perception between VA and non-VA providers regarding the availability, quality, and effectiveness of VA HF services. Finally, multiple non-VA providers expressed frustration with and difficulty in contacting VA providers, accessing records, and making referrals into the VA system.
As discussed above, few prior studies have qualitatively analyzed provider perceptions of cross-system care, although a few studies designed to evaluate aspects of cross-system care within the context of the Veterans Choice Program were recently commissioned by the VA Quality Enhancement and Research Initiative (QUERI), which are ongoing. Previously, Kramer and colleagues conducted focus groups with providers in the Veterans healthcare system and the Indian Health Service (IHS) who shared care for Veterans dually enrolled in both systems. 35 In patient interviews, they observed that, in addition to financially based decision making, patients deliberatively chose healthcare services in given systems based on available services matched to their health needs. Similar to our findings, both VA and IHS providers described poor communication and coordination of care across systems. Providers in both systems noted that dual use prolonged visits given the need to identify potential conflicts in treatment and/or duplication of services, perceptions that we also captured. Authors described the need for care coordination and a corresponding need to identify which primary care provider was “primary.” Such determinations can be even more complex in VA-community interactions given the wealth of community providers without linkages to each other or to the VA.
This dilemma is pertinent given that both groups of providers in our study described patient education as desirable, but frequently inadequate. The question becomes, “Who should provide patient education including guidance on heart failure self-management and sick day care?” A fairly robust literature exists documenting the value of personalized care planning for a variety of chronic diseases. Coulter and colleagues analyzed 19 studies enrolling over 10,000 patients with diseases including diabetes, hypertension, mental health conditions, and one study in heart failure patients, and their meta-analysis concluded that personalized care planning leads to improvements in physical and psychological health status and in self-management when compared to usual care. 36 In heart failure, Shearer and colleagues observed improved ability for heart failure self-management among patients receiving a nurse-led, telephone-delivered intervention that included personalized care planning and patient empowerment. 37 Similar interventions have been found effective as well, though more intensive care management interventions may be more potent in reducing hospitalization and hospital readmission in HF. 38 Our findings highlight this area of confusion among providers, and the need to reach clarity about care leadership and patient education in future programs designed to improve the safety of cross-system care. It may also be useful to explicitly solicit patient preferences and discuss site of care decisions as a component of patient education and care planning.
Comments by both VA and community providers regarding barriers in access to information across systems are particularly relevant. While electronic systems for health information exchange (HIE) show great promise, they also face significant barriers and have been largely underutilized in the U.S. to date. 39 Many with VA have called for informatics-based approaches, such as HIE to gaps in care. 40 Within the past five years, the VA piloted and disseminated consumer-initiated health information exchange within My Health eVet, the VA's patient-facing electronic health record (EHR) through a feature called the Virtual Lifetime Electronic Record. 41 In a small pilot trial, Veterans trained to access a “Continuity of Care Document” (CCD) and prompted to share their CCD with non-VA care providers were significantly more likely to do so as compared to control patients. 42 However, the uptake of this form of HIE nationally and its effectiveness on patient outcomes are as-yet unclear. Far more complex than information exchange is the issue of care coordination across systems. Several studies of dual use document duplicative testing and prescribing practices as well as higher rates of hospitalization and even higher mortality among dual users.43–45 Many of these risks could be mitigated through improved care coordination. Recognizing the potential negative unintended consequences of dual use, the VA Office of Community Care is currently piloting initiatives specifically designed to coordinate care when Veterans are seen by community providers. 46 Such efforts are needed and should be rigorously evaluated to ensure efficacy, scalability, and spread.
Certain limitations should be acknowledged regarding our study. First, we interviewed healthcare providers from three separate VAMCs and healthcare organizations across two Southern states, so our observations may not be generalizable nationally. Second, our sample lacked significant racial/ethnic diversity relevant to the population at large, and it is unclear the extent to which our sample reflects predominant racial/ethnic distributions among physicians practicing in our geographic region. Third, because we interviewed a variety of healthcare providers in VA and non-VA systems, we may not have achieved full thematic saturation for any given discipline, so view these perspectives as an initial exploration. We were also not able to get perspectives of all potentially relevant provider disciplines. Instead, we were able to garner a broad-based set of perspectives from key provider groups in VA and the community, an approach meant to generate hypotheses rather than demonstrate significance. Fourth, our study focused on dual system care for Veterans with heart failure. Thus, while there may be parallels to dual use in other chronic conditions, such as asthma, COPD, diabetes, or cancer, care should be taken in extrapolating our observations to other populations. Finally, it is important to note that qualitative themes emerging from this work will benefit from further empirical testing using quantitative methods to further validate the observations.
In summary, findings from this study have clear implications within the VA system where a priority has been placed on better understanding the dynamics of VA care provided in community settings. In August 2017, the VA will pass an important milestone with the sunset of the Veterans Access to Care and Accountability Act (VACAA) which authorized marked increases in non-VA care among Veterans. It is not yet clear which programs will modify or replace VACAA, but possibilities include extension of contract care similar to the Veterans Choice Program, VA-coordinated care that more closely resembles earlier VA programs, or possibly voucher systems as proposed by some advocacy groups. 47 In every case, patient and provider input should be key factors in designing policies and systems of care. Our findings have implications outside the VA as well. Seventy-eight percent of hospitals received penalties for higher than expected hospital readmission rates for one or of five target conditions in 2016 under the CMS Hospital Readmission Reduction Program. 48 Among primarily outpatient primary care and specialty providers and groups, the recent Medicare Access and Chip Reauthorization Act (MACRA) mandates expanded merit-based incentive payments (MIPS) and alternative payment models (APMs) that will focus both groups more heavily on episodes of care and/or longitudinal care across settings.49–51 These imminent program changes would benefit from attention to the perspectives of VA and community providers as well as the Veterans making decisions about care.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by VA Health Services Research and Development (IIR 12-331, Axon-PI).