
Abstract
Objective
To assess the effect of a participatory group-based education programme for individuals with type 2 diabetes, Next Education.
Method
In a quasi-experimental study, individuals with type 2 diabetes were recruited from 14 Danish municipalities with a patient education programme. Eight municipalities using Next Education were intervention sites; six control sites used usual group-based education programmes. Data were collected through questionnaires at baseline and at 3 and 12 months after programmes ended. Changes in quality of life (EQ-5D-5L), diabetes-related emotional distress (PAID-5), physical activity, diet, foot care and sense of coherence (SOC-13) were assessed in generalised linear mixed models.
Results
At baseline, 310 participants (52.6% females, mean age 62.5 years [SD = 10.7] and a mean duration of type 2 diabetes of 6.9 years [SD = 8.4]) participated in Next Education (n = 234) or group-based education (n = 76) at control sites. Compared with participants at control sites, participants at intervention sites had significantly larger sense of coherence scores at 3 (9.4%, p = 0.03) and 12 (9.8%, p = 0.02) months of follow-up. Other measures did not differ significantly between groups.
Discussion
It is likely that person-centeredness and high degrees of user participation at the intervention sites improved sense of coherence among Danes with type 2 diabetes.
Introduction
Patient education and support play a crucial role in good disease management in individuals with type 2 diabetes (T2D). 1
Person-centred education seeks to empower patients by putting their needs and experiences at the centre of attention. Supporting patients in making informed decisions has been shown to be more effective in improving self-management skills than information-only educational approaches. 2 Moreover, studies show that group-based patient education programmes based on dialogue, development of self-management skills and empowerment are effective, compared with information-only programmes. 3 Group-based patient education has the potential to promote participation and facilitate group interaction, and has the advantage of providing social modelling and problem-based learning. 4 A recent systematic review and meta-analysis of controlled trials found that group-based patient education has been associated with improvements in HbA1c and other diabetes-related outcomes such as body weight, triglycerides and diabetes knowledge when compared with usual care, waiting list control or individual intervention. 5 However, group-based education has also been tested in other settings with various results in relation to lifestyle habits and psychosocial factors.6–8
Next Education (NEED), a participatory group-based patient-centred education programme for individuals with chronic illness, was developed in 2010 and feasibility tested in 2012. 9 NEED is based on the idea that dialogue and participation in patient education are necessary to improve psychosocial issues such as sense of coherence (SOC), meaningfulness, self-management skills and health-promoting behaviours. 2 SOC is a construct that has been associated with improvements in health and health behaviours. 10 SOC has three dimensions: Comprehensibility (I am confident that events in my life occur in an orderly, predictable manner and that I can make sense of these events and predict what may happen in the future); Manageability (I believe these events are within my control and that I have what I need to handle them); and Meaningfulness (Things in my life are satisfying, interesting and worth caring about). Having a strong SOC is important for individuals with T2D because it can enable them to cope better with the challenges of their disease and keep a positive outlook. 11 Furthermore, findings from a previous study have suggested an indirect path from SOC to improved glycaemic control. 12
NEED includes two theoretical models: The Balancing Person 13 and The Health Education Juggler, 14 and 24 dialogue tools in four categories: (1) reflection and experience; (2) motivation and goals; (3) knowledge and learning; and (4) body and senses. The Balancing Person describes individuals with chronic illness as constantly balancing physical, practical, social, and psychological challenges in their lives. 13 In addition, the model describes four health educational meta-needs to address these challenges in patient education: SOC, clarity, timeliness and connectedness. Consequently, NEED was designed, planned and implemented with the intention to promote a balanced life focused on the person rather than the illness. 13 The Health Education Juggler describes different roles health educators must master and use interchangeably during group education. The Balancing Person and Health Education Juggler models are described in further detail elsewhere.13,14
A feasibility study of NEED showed that the toolkit supported health educators in promoting person-centred patient education and enabled interaction and activity among participants as a means to obtain well-being and sustainable behaviour change. 9 However, the success of the tools depended to a large extent on the presentation, interpretation and skills of the health educator. 2 An evaluation among individuals with T2D showed that they experienced high levels of participation and increased their knowledge about diabetes after participation in NEED. 15 These patterns were confirmed in a quantitative analysis, in which participants who used NEED were more likely to rate patient education as ‘very good’ or ‘excellent’, compared with participants in group-based patient education at control sites. 15
However, we wanted to explore the effects of NEED further based on outcomes relevant to individuals with T2D receiving diabetes education. The objective of this study was to investigate to what extent participation in NEED was associated with improved psychosocial and lifestyle outcomes among individuals with T2D.
Methods
Study design
A quasi-experimental design was used to assess the effect of NEED, which was already in use in many Danish municipalities. Municipalities were eligible to participate in the study if they met inclusion criteria as an intervention or control site (see Figure 1). Intervention sites met three criteria: (1) 10 or more participants were enrolled in NEED group-based patient education for individuals with T2D; (2) NEED was used in the majority of education sessions (i.e. at least 50% of the time); and (3) participants used NEED at least 4 times.
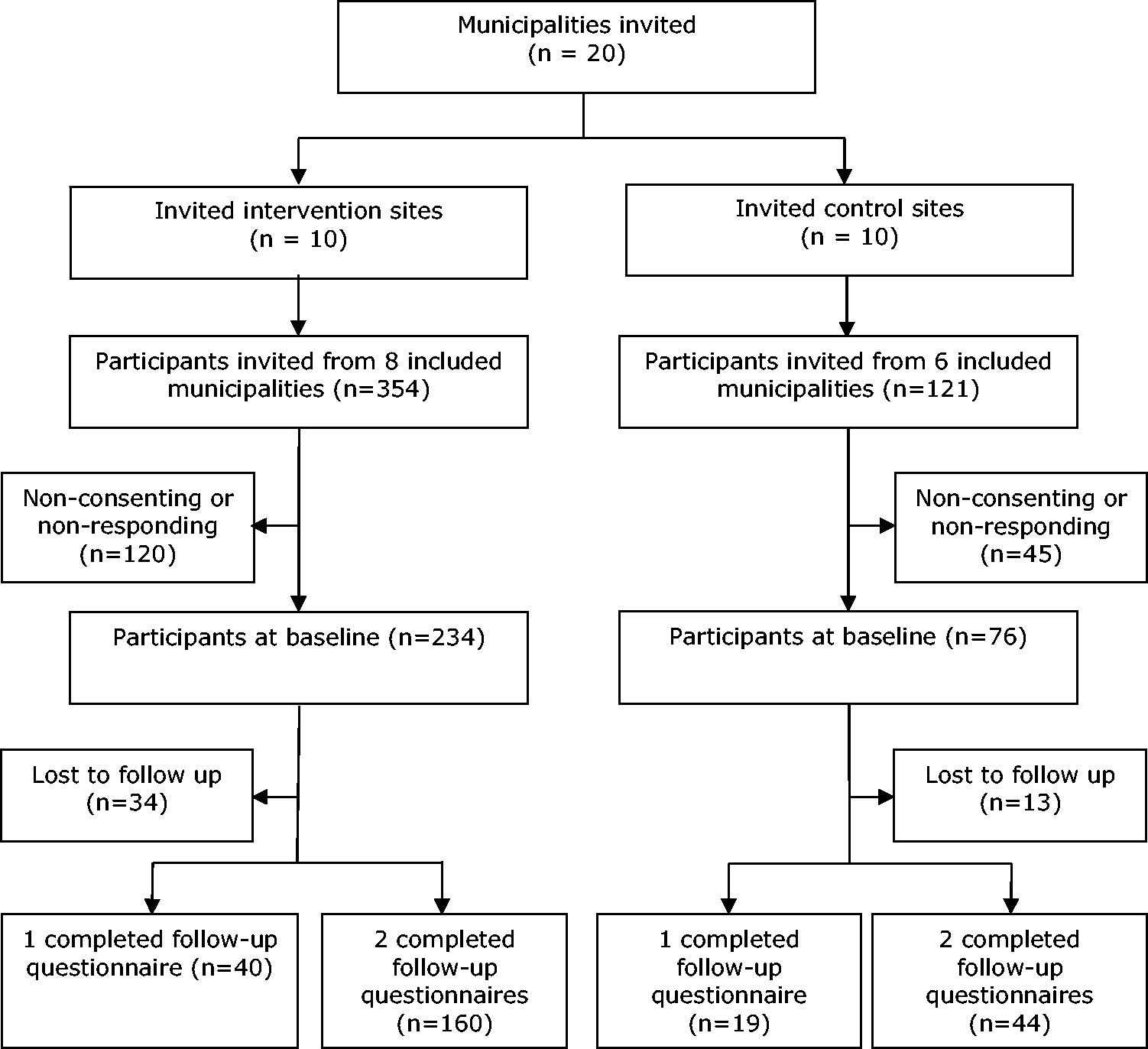
Participant flow diagram.
Control sites met the following criteria: (1) 10 or more participants were enrolled in group-based patient education for individuals with T2D during a 6-month period; (2) NEED had not been used before the study began in January 2013; (3) there was no planned use of NEED during the study period; and (4) participants used usual group-based patient education at least 4 times.
Individuals with T2D were invited to participate when they enrolled in patient education programmes at participating municipalities, as either an intervention or a control site. NEED embraces physical, practical, social and psychosocial aspects of living with a chronic illness and has a core focus on enabling participants to obtain a balanced life. Consequently, we focused on psychosocial outcomes related to aspects captured by NEED. The often-used measure HbA1c was unavailable in the municipal settings as it was impossible to derive HbA1c measures from participants’ general practitioners due to administrative and legal issues in Denmark at the time.
The intervention
NEED was delivered by specially trained health care professionals as a group-based patient education programme at intervention sites. 15
A step-by-step guide that allowed variation and adaptation to specific groups and health educators accompanied the NEED toolkit. The focus of the education was to tailor education to the needs of the specific group of participants. Consequently, the educational content and focus of NEED varied to some extent across educational groups; however, the focus was psychosocial issues and behaviour change. At control sites, participants were offered group-based patient education programmes that did not include the use of NEED but may have included other tools and methods to facilitate interaction, person-centeredness and social learning.
Outcome measures
Information on psychosocial outcome measures was collected before participation in patient education and at 3 and 12 months after completion of the programmes, using questionnaires developed at a specialist diabetes clinic in Denmark that included well-established and validated generic and disease-specific scales. Quality of life was assessed by the EQ-5D-5L. 16 Possible scores range from −0.624 to 1, with 1 indicating a high level of quality of life. Diabetes-related emotional distress was measured by the 5-item Problem Areas in Diabetes (PAID-5) scale. 17 Possible scores range from 0 to 20, with 0 indicating a low level of diabetes-related emotional distress. The Summary of Diabetes Self-Care Activities (SDSCA) scale was adapted to assess physical activity, diet and foot care. 18 SDSCA items assessing physical activity were used without alteration. The diet-related SDSCA item was adapted to recommendations from the Danish Ministry of Environment and Food (e.g. to eat six pieces of fruit/vegetables per day). Foot care was measured by a single item (“How many times within the last seven days did you check your feet?”) instead of two items. 18 Possible scores for all SDSCA items ranged from 0 to 7, indicating the number of days the activity had been performed within the previous seven days. SOC was measured by the 13-item sense of coherence scale (SOC-13). 11 Possible scores for each item ranged from 0 to 7; the total scale score ranged from 0 to 91, with 91 indicating a strong SOC.
Participants returned baseline questionnaires at the start of the first patient education session and returned follow-up questionnaires by mail. Participants who did not return follow-up questionnaires within two weeks received a mailed reminder that contained another copy of the questionnaire.
Control variables
Binary variables measured participants’ sex and the presence or absence of co-morbidities and a cohabitating spouse. Continuous variables assessed age and duration of T2D in years and body mass index (BMI) in kg/m2. Categorical variables included socioeconomic position, measured by educational level and categorised as primary education alone, short vocational courses, extended vocational training, <3 years of tertiary education and ≥ 3 years of tertiary education. Weekly alcohol consumption was measured as the number of standard drinks at a usual week and categorised as 0, <2, 2–7, 8–14 and ≥15, with the latter corresponding to the recommended maximum weekly intake by the Danish Health Authority. 19 Use of diabetes medication was measured by three categories: no medication, oral hypoglycaemic medication (blood glucose-lowering tablets) or injections (insulin or other injections); participants who used both oral hypoglycaemic medication and injections were categorised as using injections. Contact with friends was categorised as daily or almost daily, once or twice a week, once or twice a month and rarely or never (i.e. less than once a month). We included information on health promotion expenditures per inhabitant and degree of urbanisation in participants’ municipalities of residence.20,21 Degree of urbanisation was assessed by seven criteria defined by the Danish Business Authority and included four types of municipalities: urban, semi-urban, rural and remote. 21 Data on municipalities were obtained from publicly available national databases. 20
Statistical analyses
Baseline differences between participants at intervention and control sites were assessed by t-tests and Chi-square tests for continuous and categorical variables, respectively. We identified factors important for loss to follow-up by a backwards search in a logistic regression model that included all control variables and outcomes (i.e. EQ-5D-5L, PAID-5, physical activity, diet, foot care and SOC-13) assessed at baseline. We used linear mixed models to assess changes over time in the outcome measures among participants at intervention sites compared with those at control sites while controlling for dependencies in the data (i.e. multiple observations per participant and control variables measured at municipality and participant levels). A participant random effect controlled for repeated observations on the same participant, and a municipality random effect controlled for within-municipality correlations. Baseline data on sex, age, socioeconomic position, BMI, duration of T2D, alcohol consumption, diabetes medication, comorbidity, spousal cohabitation and contact with friends were included in the model as fixed effects to adjust for potential confounding.
All statistical tests were performed with a significance level of 5%. Statistical analyses were performed using IBM SPSS Statistics 20.
Ethical considerations
Participation in the study was voluntary and participants gave informed written consent to participate in the study. Participation in the diabetes education did not depend on consent to study participation. The study was approved by the Danish Data Protection Agency (SDC-2017018, I-Suite: 05861).
Results
On the basis of the inclusion criteria, 10 eligible municipalities were invited to participate as intervention sites among which eight accepted; 6 of 10 eligible municipalities agreed to participate as control sites. A single municipality with several parallel classes agreed to participate as both intervention and control site. A total of 475 Danish individuals with T2D were invited to participate in the study; 310 agreed to participate and returned the baseline questionnaire, yielding a response rate of 65.3%. Of all participants, 234 (75.5%) were enrolled in patient education programmes at intervention sites and 76 (24.5%) were enrolled in programmes at control sites. Among participants at both types of sites, 204 (65.8%) returned both follow-up questionnaires, 59 (19.0%) returned one follow-up questionnaire and 47 (15.2%) did not return either follow-up questionnaire. Participants who completed follow-up (i.e. returned both follow-up questionnaires) had lower socioeconomic position (p = 0.045) and were more likely to use oral hypoglycaemic medication (p = 0.02) and to come from semi-urban municipalities (p = 0.04). When examining participants who were lost to follow-up, higher BMI was associated with lower rates of answering both questionnaires (p = 0.005). Participation in NEED was not associated with the likelihood of complete follow-up.
Participants had an average age of 62.5 years (standard deviation [SD] = 10.7) and 52.6% (n = 163) were females (Table 1). Their mean duration of T2D was 6.9 years (SD = 8.4). Baseline use of diabetes medication (p = 0.02) and contact with friends (p = 0.04) differed significantly between participants at intervention and control sites. Participants at intervention sites were more likely to use oral hypoglycaemic medication than participants at control sites, who were more likely to use injections or no medication. Contact with friends was more frequent among participants in the control sites compared with participants at the intervention sites.
Baseline characteristics of participants.
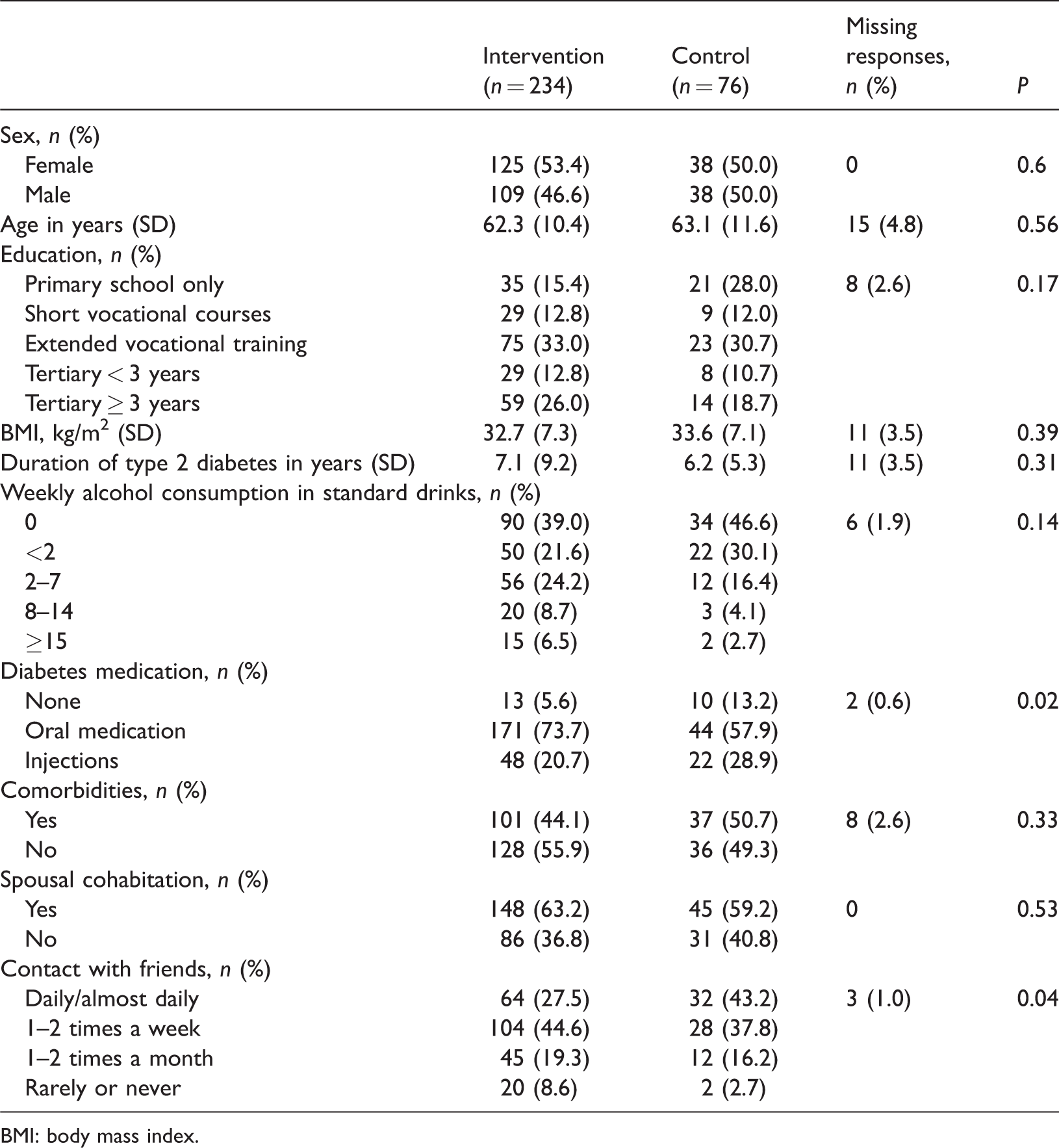
BMI: body mass index.
Compared with participants at control sites, participants at intervention sites had a significant larger increase in SOC-13 score at 3 (9.4%, p = 0.03) and 12 (9.8%, p = 0.02) months of follow-up (Table 2). We found no statistically significant differences in quality of life, diabetes-related emotional distress, physical activity, diet or foot care between participants at intervention and control sites.
Differences in mean scores among participants at intervention sites compared with participants at control sites.
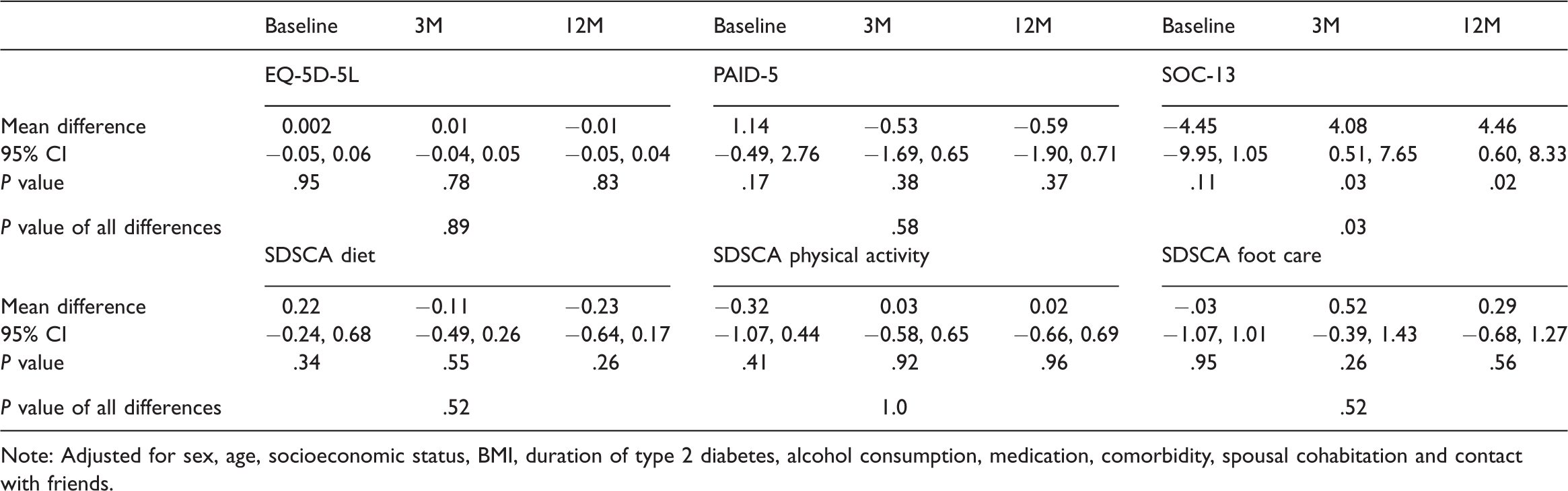
Note: Adjusted for sex, age, socioeconomic status, BMI, duration of type 2 diabetes, alcohol consumption, medication, comorbidity, spousal cohabitation and contact with friends.
Discussion and conclusion
Discussion
Compared with participants in usual group-based patient education at control sites, participants who enrolled in NEED programmes had significantly improved scores for SOC at 3 and 12 months of follow-up. Thus, the study suggests a sustained improvement in SOC following the intervention.
NEED embraces physical, practical, social and psychological aspects of a life with a chronic illness and has a core focus on enabling participants to experience a balanced life by connecting the past, present and future and by focusing on the person rather than the disease. 13 The core mechanisms of NEED embrace the concept of SOC, so it is not surprising that our main finding relates to this concept. Indeed, we find it plausible that participation in NEED is associated with an improved SOC, although other factors may have also contributed to the improvement we observed. It has previously been suggested that a combination of mechanisms related to NEED, including person-centeredness, dialogue and group processes, explained improvements among participants who used NEED. 15 Qualitative data from that study showed that participants in patient education programmes appreciated sharing experiences and exchanging knowledge with others in similar situations. 15 Likewise, evidence from the feasibility study of NEED 9 suggested that group processes contributed to creating a sense of community among participants in NEED programmes, and it has been previously found that individuals with a chronic illness value meetings with peers. 22 In the study reported here, it is likely that similar group processes and mechanisms, such as person-centeredness and dialogue, may explain the improved SOC among participants at intervention sites. None of the previous studies we identified as investigating the effects of group-based patient education explored the association between group-based patient education and SOC. Other psychosocial outcomes (quality of life, 6 diabetes-related emotional distress,6–8 and mental health7,8) have been previously investigated. Only one of these studies 7 found an association between group-based education and improvements in a psychosocial outcome (i.e. mental health).
Our study has several strengths. First, NEED was tested in real-life settings among its intended users (i.e. health educators and individuals with T2D). Thus, there was no discrepancy between the study setting and the settings where NEED is intended to be used. Second, a broad sample of individuals with T2D was included, supporting the generalisability of our findings. Third, our outcome measures included well-known, validated generic and disease-specific scales10,16–18 that reflected the concepts of NEED. Fourth, our robust statistical method attempted to account for missing responses, attrition and cluster effects in the data. Finally, the study design used both intervention and control sites and repeated measurements, which may have reduced confounding and information bias. A better balance between number of participants from control sites and intervention sites would, however, have resulted in even higher statistical power.
Several limitations deserve mention. We did not conduct a randomised controlled trial, which may have introduced bias. To reduce potential selection bias, we included control variables at the level of municipalities. Furthermore, participants at intervention and control sites seemed to be well matched at baseline; only the use of medication and contact with friends differed significantly between participants at the two types of sites. However, if contact with friends had positive impact on patient education outcomes and was more frequent among participants at control sites, any potential selection bias in this study would contribute to an underestimation of the effect we detected and cannot explain improvements in the intervention group. Participants being treated with oral medication were overrepresented in the intervention group. Accordingly, the main statistical models were adjusted for baseline use of medication to avoid potential bias.
The difficulties of conducting pragmatic intervention studies in primary care settings are well recognised; 23 they often have a relatively low ability to detect effects of interventions because patients are usually in earlier or milder disease stages, compared with patients in specialised care settings. 24 Likewise, NEED is a person-centred participatory patient education programme intended to be tailored to the actual groups of participants; therefore, the educational content and focus of NEED may vary between the individual sites, 15 which may contribute to difficulties in detecting effects on specific lifestyle outcomes. This explanation is supported by a previous study which found that NEED participants had varying perspectives on whether participation in NEED improved lifestyle habits. 15 Finally, we did not assess within-group changes in outcome measures over time, and therefore we cannot exclude the possibility that group-based patient education has beneficial effects regardless of the programme used.
Conclusion
Use of the participatory group-based patient education programme NEED focused on psychosocial issues and behaviour change was associated with sustained improvements in SOC among individuals with T2D, compared with usual group-based patient education approaches. Participants from the intervention sites experienced a sustained improvement in SOC at 3 and 12 months of follow-up. Lack of detectable differences between intervention and control sites in other outcomes may be attributed to low statistical power of the study or equivalently beneficial effects of NEED as well as other group-based patient education programmes.
Footnotes
Acknowledgements
We would like to express our sincere thanks to the participating municipalities, including educators and participants for offering their time to interviews and questionnaires. We acknowledge Jennifer Green, Caduceus Strategies, for editorial assistance.
Authors’ contributions
All authors contributed to the study design. LANC and AKH analysed the data and drafted the manuscript. RASP, IW, VS, and KO critically revised the manuscript for important intellectual content and all authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.