
Abstract
Objective
The overall aim of this study was to examine, among individuals living with severe asthma, the role of perceived competence in achieving their goals.
Methods
Qualitative research methods were used to conduct in-depth semistructured interviews. Interviews were video and/or audio recorded, transcribed and analyzed inductively and deductively, informed by the self-determination theory construct of perceived competence. Thirty-six face-to-face interviews, lasting 1.5–4 h, were conducted across Australia.
Results
Feeling competent to achieve asthma goals played a role in participants’ ability to achieve broader goals. Their desire to achieve their broader goals was strongly driven by their perceived ability to master managing their condition, which at times required more than medical strategies. Two main themes were discerned from the analysis: (1) learning how to look after yourself: self-care is important and (2) reaching an agreement with severe asthma: being at one with the illness.
Discussion
This study highlighted the influence of perceived competence on self-management and goal achievement in severe asthma. Healthcare providers could explore patients’ perceived competence to set and achieve goals, as a self-management strategy. Future research should consider these findings when developing and implementing patient-driven, self-management interventions for those living with severe asthma.
Introduction
Competence is argued to be an important characteristic of ‘motivational drive’,1,2 towards long-term conditions/chronic disease self-management and promoting goal setting. A key construct of self-determination theory is competence. The theoretical underpinnings of competence suggest that strengthening an individual’s ability to self-manage their chronic illness provides them with a sense of mastery and effectance, that is need to interact effectively with one’s environment, when responding to the complex challenges of achieving goals.1,3,4 The term ‘competence’ is defined as a self-belief in one’s ability or capability to perform an activity or achieve goals. 5 Within the healthcare literature, ‘perceived competence’ has been described as an individuals’ perceived ability to carry out their own self-care routines in order to manage their disease.6,7 In asthma self-management, some studies have described competence in narrow terms as the confidence to accurately interpret symptoms and follow through with appropriate self-care.8,9
Asthma is a chronic condition that affects approximately 330 million people worldwide with an estimated total healthcare cost in Australia approaching $27.9 billion a year.2,10,11 While most people can effectively manage their asthma with treatment, between 3% and 10% of people with asthma experience uncontrolled symptoms despite being on high-dose treatment and are therefore classified as having severe asthma.11,12 Severe asthma accounts for high morbidity and is estimated to contribute to half the healthcare costs associated with asthma.13,14 A Canadian report identified the annual cost per patient with severe asthma to be 10 times more than for those with mild to moderate asthma and suggested that a broader paradigm of asthma management was needed. 14
Much of the applied research on self-management of asthma focuses on clinical concepts such as improving lung function, symptom management and use of action plans and medications. 15 In the past few years, there has been a great deal of research conducted into patients actively participating in their care and the benefits of self-management. One integral part of managing a chronic condition is setting goals.16–19 The effect of goals upon behaviour has received much empirical attention.20,21 Goal setting is defined as the process by which people set themselves goals and are motivated to work towards achieving them and has been recognised as an effective technique to help facilitate health-related behaviours and self-management.22–24 However, there is a no published research around goal setting and achievement among those living with severe asthma.
Research has shown that strengthening a patient’s sense of perceived competence improves self-management, 25 quality of life26,27 and satisfaction with patient–clinician goal setting and goal achievement.6,7 This has been found across a range of chronic conditions including type 2 diabetes, 6 respiratory 25 and cardiovascular disease.25,27 However, despite the push for enhancing both patient and physician perceived competence to improve health outcomes,7,25,28 it is important to note that people’s illness perceptions play an important role in influencing goal-setting behaviours. 29 Understanding illness experiences is key to uncovering the day-to-day physical, psychological and emotional challenges, people face to preserve their sense of competence to live well with their condition.
The increasing importance and popularity of strategies to support patient competence in healthcare,7,30 combined with the paucity of studies of how people with severe asthma live with their condition,31,32 highlights the need for research in this area. Thus, the overall aim of this study was to examine the role of perceived competence in achieving goals when living with severe asthma, based on in-depth interviews with adults with this condition.
Methods
A qualitative interpretative approach was chosen for this study because it can provide rich and deeply nuanced insights. 33 The research protocol was approved by the University of Sydney Human Ethics Committee (HREC 2015/934).
Patient recruitment
Participants were invited by their general practitioner (GP) or respiratory physician to take part in the study if they were 18 years or older and diagnosed with severe asthma by a specialist respiratory physician according to international guidelines. 12 The aim was to include participants from different ethnicities, geographical locations and sociodemographic backgrounds; interviews were offered in English, French or Arabic. All participants were provided with an information pack by their GP or respiratory physician and were asked to sign a consent form and complete a reply form if they agreed to take part in the interview.
Data collection and analysis
The data were collected between October 2016 and August 2018. In-depth face-to-face interviews were conducted in the participants’ homes, or elsewhere if preferred. Participants were asked to tell their own story from the point when they first noticed they had breathing problems. To begin with, they were encouraged to talk about their experiences of living with this condition, with as little interruption as possible from the interviewer. The interview schedule was initially developed from a systematic review of the literature and provided a guide for discussion. 31 Prompts included questions about how they managed their condition and their goals. For this study, goals were defined as personal objectives 34 and desired outcomes. 35 An overview of the questions asked during the interview is included in Appendix 1.
Trustworthiness was ensured through respondent credibility, transferability, dependability and reliability.36–38 During later stages of data collection, the constant comparison method of analysis was applied to continuously compare the experiences of participants and subsequent revision of the coding template.39,40 Following each interview, field notes were written to initiate reflection. Interviews were audio and/or video recorded and transcribed verbatim. The transcribed data were then read several times, and in addition, the recordings were listened to once more to ensure the accuracy of the transcription. The transcripts were initially coded by the interviewer (DE) using NVivo software and were read by all authors of the research team. The researchers have experience in qualitative research (LS, KR and HR) and in the clinical aspects of severe asthma (HR).
A hybrid process of thematic analysis was used to interpret the data. 41 This incorporated both a data-driven inductive and SDT informed deductive approach. The theoretical frame of SDT’s construct of competence informed the template of codes as a means of organising text for subsequent interpretation.2,4 The initial stage of coding involved constructing a coding framework with reference to competence, personal abilities, capabilities and goals. Initial codes were grouped into categories according to similarities. Analysis and comparison across and within the categories were conducted to develop themes. This meant stepping into complex territory, in which the process of interpretation required a higher level of abstraction. 42 Interpretation of the data is inevitably affected by the interviewer’s own values, beliefs, experiences and biases.43,44 To counter potential biases data analysis was first carried out by DE and then independently checked by three other experienced researchers (LS, HR and KR). Pseudonyms have been used to protect the anonymity of the participants.
Results
Participants
Thirty-six interviews were conducted. A total of 19 women and 17 men, aged between 17 and 74 years, participated. All participants spoke fluent English and most agreed to be video recorded. The interviews were 81–235 (mean 147) mins in length. Sociodemographic characteristics are summarised in Table 1.
Characteristics of the participants (n = 36).
Findings
Analysis revealed that perceptions of goal setting and perceived competence to manage severe asthma were inextricably linked. It was apparent that the success of achieving broad life goals depended on meeting asthma goals (Figure 1). Achieving asthma goals was of prime importance to participants, mainly because these goals focused on basic physiological tasks such as breathing. Feeling competent to achieve asthma goals played a role in their ability to accomplish broader life goals such as being able to travel or spending more quality time with their family. Participants’ ability to achieve their asthma goals was strongly driven by their desire to master self-management of personal health. Two themes were discerned: (1) ‘learning how to look after yourself’: self-care is important (see Table 2) and (2) ‘reaching an agreement with severe asthma’: being at one with the illness (see Table 3).
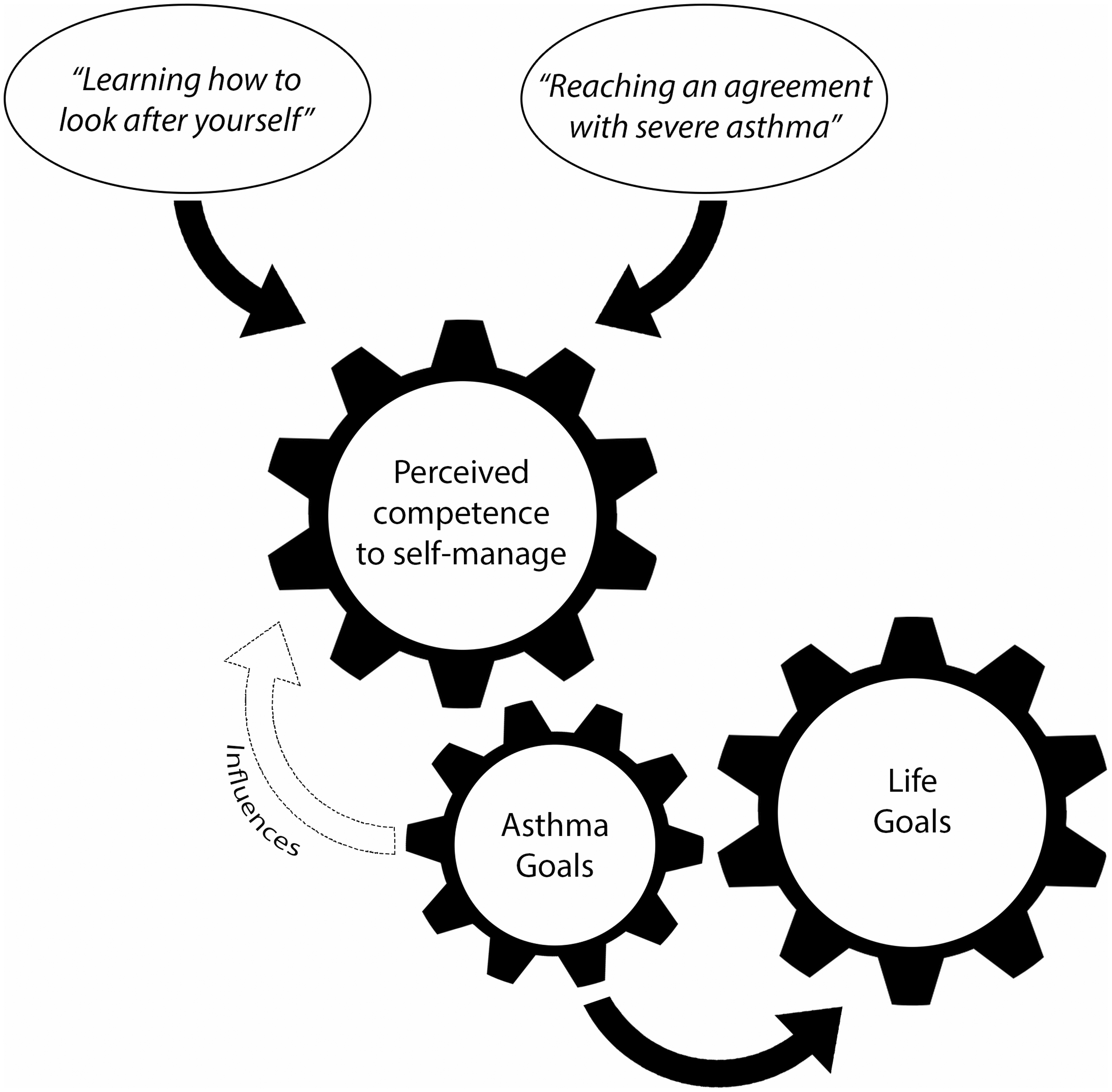
Conceptual diagram of the role of competence in self-management and goal achievement.
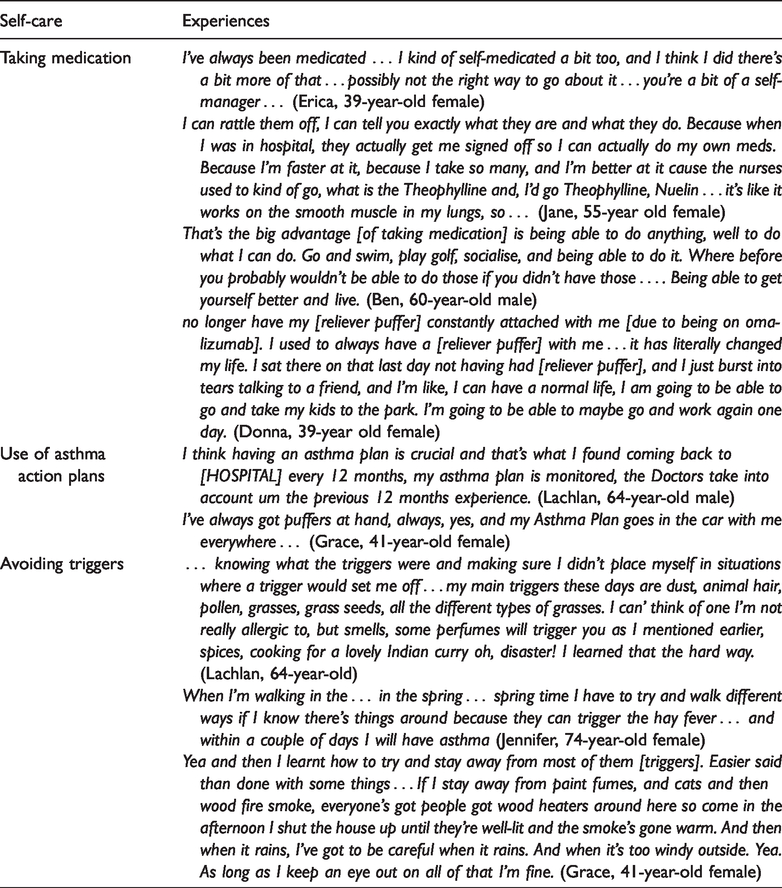
Additional quotes for ‘learning how to look after yourself’: self-care is important.
Additional quotes for ‘reaching an agreement with severe asthma’: being at one with the illness.
Theme 1: ‘Learning how to look after yourself’: self-care is important
Feeling competent in achieving personal asthma management goals was valued and deemed an important enabler to achieving asthma goals. Taking medications was perceived to give people with severe asthma a sense of effectance in managing their asthma. Medications such as salbutamol (an inhaled quick-reliever medication, e.g. Ventolin™) and/or oral corticosteroids (prescribed for short-term treatment of serious attacks, and, for some patients, used long-term to help prevent serious attacks albeit with potentially serious side-effects) at times provided a sense of security and necessity to accomplish their goals. For example, Jane reported that her reliever inhaler was on her at all times irrespective of what she was doing that day: … the rules [her personal rules] are I have to have the [reliever] puffer and spacer in my hands all the time, if I get up to move. So, if I get up from a bed to go to the toilet I have to carry the [reliever], the spacer. (Jane, 51-year-old female) … I've got backups … I've got them at my mum's, I've got them in the car, I have them at home. If I go to the doctor’s, she's already got them set anyway … she knows that I'll panic about it and all the rest of it. (Teresa, 39-year-old female) I will admit that … I'm talking a lot because I’m up the Prednisone to make sure that I'm able to do this [the interview] because normally for me talking this long just, it wouldn’t happen … (Jeff, 35-year-old male)
While asthma medications, particularly oral corticosteroids, have side effects that can be serious, this did not appear to limit participants’ decisions to alter the dose or stop their treatment. For example, Chris reported that prednisone has ‘destroyed’ his eyes, nose, thinned his skin and given him the shakes; yet he continues to take more to manage his asthma to achieve his asthma goals of feeling in control: I said before, it’s [severe asthma] a life changing thing, a life controlling thing … I hate being out of control … I probably wrecked me [sic] life … taking too much Prednisone … I take lots of medication, more than I need … I’m very fearful of having another real severe attack again. (Chris, 66-year-old male) [Omalizumab] made a huge difference to my life … I could go most of the day without having to use [reliever puffer]. It was absolutely incredible. I had to remind myself to take it with me … It's made a huge difference mentally as well as physically, feeling like you can participate in more things … (Charlotte, 52-year-old female) … [I want] it [breathing] not to hurt … I had it [biological therapy] once a month. I only had two and I had four exasperations [sic] yeah … like this new fantastic drug that works on everyone didn’t work so now we’re trying this other drug … (Jane, 51-year-old female) You're merely attempting to manage a potentially debilitating, and-and a potentially fatal disease … preferably have an effective asthma plan that, you know, will work from a specialist that you adhere to strictly on a day to day basis. But, with it's not a thing that's designed to inconvenience you. It's something that will help you to maintain a normal, average lifestyle. (Freddy, 64-year-old male)
Theme 2: ‘Reaching an agreement with severe asthma’: being at one with the illness
In addition to being adherent to treatment and relying on their asthma action plan (self-care), participants expressed that they required more than medical strategies to feel competent to self-manage. They felt they needed to be more self-aware of their illness. For some, competence was expressed as their ability (1) to self-manage and (2) to feel at one with their illness. This required transitioning from focusing on their needs as defined by the illness, to learning how to understand their body and integrate the illness into the context of their lives and broader goals.
Perceived competence to self-manage
Participants described the experience of ‘owning their body’ as a crucial component to being at one with their illness and feeling competent to self-manage to achieve their broader life goals: I would be defined by my asthma if I didn’t respect the fact it is part of my life and I didn’t do anything to look after it. It would then dominate my life, because I would then be getting sick, so you find the things that work for your asthma and you get on and live life as anyone else does. It just so happens you’ve got asthma. (Lachlan, 64-year-old male) I don’t understand asthma … it’s a bit depressing, Don’t want to admit it but … . everything’s just a struggle … there’s been a lot of changes but it’s all out of, out of my control. There’s nothing that I can do to, to fix it [fixing his asthma and being able to breathe] … (Archie, 58-year-old male) Sometimes I could be just sitting in a conversation and I’ll suddenly think, gosh, but I just don’t do anything, and I hope it’ll pass and usually it does. Because the worst thing you can do is panic. That’s what I’ve learnt … it’s always mind over matter and you’ve just got to try to be calm all the time … (Sara, 71-year-old female) … stress can actually trigger asthma, so again, if you can calm down through meditation and meditation doesn’t have to be sitting quietly going “ohm” with your fingers like that … just taking yourself away from that position of stress or the thing that’s triggering you … (Ben, 60-year-old male) I was hurting [after going to the gym] and we were stopping because of my asthma playing up or my muscles were going wrong … I think it’s a big part of the fact that it’s my body getting stronger, but it’s also the condition going well “we know you’re getting stronger, but-” it’s sort of working against it … Sometimes I push myself too far, because I know “I know I can do it!”. (Jeff, 35-year-old male) I'm a very stubborn woman and I like to do things myself … I was cooking and I was yeah. I said no I feel great. He'd [carer] been gone an hour or an hour and a half or something and I thought geez I'm not well so I went to bed … I lay down and the next thing bang I was down and I had no-one. I couldn’t ring for help; I couldn’t do anything. (Jane, 51-year-old female) I feel that the condition impacts my life goals on how quickly I can achieve the goals that I set out and how fast I can actually knock off each individual item … which is very frustrating, because I know I’m physically capable of doing it, it’s just [my] asthma … (Jeff, 35-year-old male)
Perceived competence to feel at one with their illness
Being in and out of hospital due to the unpredictable nature of severe asthma at times eroded participants’ perceived competence to manage their condition. For some, being admitted to hospital on a regular basis left them feeling defeated by their condition. So, the constant challenge of being unable to predict the next exacerbation left them feeling unable to understand their body and accomplish goals. Donna’s life goal was to complete a degree at university but her uncontrolled asthma prevented her from achieving it at that time: … that [asthma] limited me to what I wanted to do because I had to face the embarrassment of that [breathlessness] … also, by the time you did something, you were exhausted, running with sweat, because you’ve had so many asthma attacks … I pretty much was in and out of hospital … I wouldn’t have the attendance required because of my hospitalisations and also there were days I wasn’t going to be well enough … (Donna, 39-year-old female)
Time since diagnosis emerged as a defining influence in achieving goals and perceived ownership of their body. Narratives of perceived competence to self-manage also varied depending on participants’ illness trajectory and their life context. These experiences varied from inherently describing a loss of competence to developing a sense of competence by learning how to master challenging situations given their previous experience. A perceived loss of competence was prominent among those diagnosed with severe asthma for fewer than 10 years. Archie described that before being diagnosed with severe asthma, he used to compete in weight lifting competitions. Since his diagnosis, he has struggled to maintain his physical activity and as a result described a loss of competence: … instead of doing, ah doing the gym and we were really fit and my son and I were right into it, now it’s just go do the basic in the gym just to stay, so you don’t lose all your muscle and, because you can’t do the cardio and physical work anymore … I’ll sit, sit on the couch and next thing I’m back at, falling asleep again … it’s just a struggle just, just to get through the next hour … (Archie, 58-year-old male) I couldn’t do all the things I wanted to do, particularly socialising, partying. You just learn what your limitations are, and you work around it … you learn quickly and if you want to, you cannot listen to your body and its needs or you’ll cause enormous problems, I don’t want to do that, I didn’t want to do that and why would anyone? So, as I said, you get to know your body with something like asthma. (Lachlan, 60-year-old male)
Discussion
The purpose of this study was to examine the role of perceived competence in achieving goals among individuals living with severe asthma. To the authors’ knowledge, this study has provided the first insights into the role of perceived competence in self-management and goal setting for people with severe asthma. Overall, our findings revealed that the success of achieving competence in life goals depended on meeting asthma goals.
The need to feel competent in self-management was a necessary driving force for goal setting and achievement. Interviewees who reported diminished feelings of competence in managing severe asthma felt unable to set and achieve asthma and broader life goals. These findings parallel Ryan and Deci’s proposal that an individual’s competence can facilitate intrinsic motivation, while diminished feelings of competence serve to restrict it. 45 Studies reporting on patients perceived competence and goal setting have focused on designing and implementing strategies to enhance patient competence to self-care in order to improve health outcomes.9,30,46 For the participants in our study, however, one of the key components to feeling competent to manage their condition was their ability to self-care, including taking medications. Research pointing to poor medication adherence has often been published in the asthma literature, with rates of poor adherence among patients ranging between 30% and 70%47,48. Much of the research focuses on identifying ways to improve adherence to therapy for those living with asthma.49–51 However, our study shows that those living with severe asthma have expressed being adherent to treatment and at times taking a higher-than-recommended dose of their medications (salbutamol and/or oral corticosteroids were specifically mentioned) despite experiencing serious side effects. Novel monoclonal antibody therapies have been shown to have a positive impact on health-related quality of life for patients with severe asthma.52,53 Our findings suggest that for many patients these medications enabled them to accomplish their broader life goals; but a couple of patients reported adverse effects from biological therapy that thwarted their ability to achieve even their asthma goals. Another self-care behaviour reported in the literature is the use of asthma action plans. Several studies have reported that asthma action plans tend to be under-used by patients with asthma or not offered by healthcare providers.8,54,55 In contrast, our study participants with severe asthma reported that having an asthma action plan enhanced their sense of competence to manage their condition.
While research has shown that, for patients’ living with symptoms such as breathlessness, feeling able to manage their symptoms was influenced by their coping style and help-seeking behaviours. 56 Our findings, however, have highlighted another key component to feel competent in managing symptoms. For people living with severe asthma, being able to manage their condition was influenced by their ability to feel a sense of psychological ownership over their condition. Participants expressed the importance of being able to integrate the illness into their lives and feel at one with their illness. Psychological ownership has not been studied extensively in the healthcare literature. Feeling at one with their condition has been described as a complex state comprising self-awareness, thoughts and beliefs. 57 Sensations of fear and panic contributed to the disruption of the sense of bodily ownership. Participants described having to enlist strategies to reduce the potency of their negative emotions and develop their sense of bodily ownership. The experience of owning an illness is rooted in the idea of control. 57 The time since being diagnosed emerged as a defining influence in perceived control of their body. Those who have lived with this condition for more than 10 years reported being able to understand their body emotionally and physically with greater acuity. Looking at the narratives of people’s experiences of living with severe asthma, through the lens of competence, potentially furthers our understanding of the psychological efforts required to manage this condition.
Strengths of the study include its rigorous qualitative methodology, including the use of a theoretical frame of reference, and incorporating both an inductive and deductive approach to analysis. In addition, the authors discussed the analysis to compare and challenge individual interpretations. The authors frequently discussed the analysis to compare and challenge individual interpretations. A limitation of this study is that our participants did not encompass the ethnic diversity in the Australian population but had a similar Caucasian predominance as the Australian Severe Asthma Web-based Database, in which 85% of patients registered were Caucasian. 58
Practice implications
For people living with severe asthma, the need to feel competent to achieve asthma goals was a necessary driving force to achieve broader goals. Healthcare providers should discuss with their patients what goals are important to them and their perceived ability to achieve these goals. This can be used to understand how people living with severe asthma manage their condition and their level of perceived competence. For example, perceived competence may affect how people take their medication, interpret their symptoms and communicate with their healthcare providers. This may provide insight into the psychological impact of living with this condition. In light of these findings, therapeutic guidelines could be reviewed to include more holistic self-management strategies. This study supports the need for deep reflection on the current practice of caring for patients with severe asthma. Identifying patient perceived competence for achieving asthma goals has the potential to unravel unmet psychological and emotional needs. Future research should consider these findings when developing and implementing patient-driven self-management interventions for those living with severe asthma.
Conclusion
This study has advanced our knowledge in understanding the complex dynamics of patient perceived competence in self-management and ability to achieve goals. Our study has shown that the success of achieving goals depends on patients’ perceived competence to manage their illness. Given that the majority of research aimed at developing policy and practice for severe asthma describes the need to promote self-management, our findings suggest that this is broader than the conventional concept used in the asthma literature. In addition to symptom management and adherence to treatment, self-management also includes the ability to achieve psychological ownership of the illness.
Footnotes
Acknowledgements
We would like to thank all participants and the healthcare providers involved in recruitment.
Contributorship
LS, HKR and DE designed the study. DE conducted the data collection. The initial coding was undertaken by DE, LS and KR. All authors were involved in the finalising work of the analyses, and DE made the final write-up of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The research protocol was approved by the University of Sydney Human Ethics Committee (HREC 2015/934).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded through a Seed Grant from the National Health and Medical Research Council Centre for Research Excellence in Severe Asthma, Australia.
Guarantor
DE
Informed consent
Written consent was obtained from patients for their anonymised information to be published in this article.