
Abstract
Objective
The European Reference Network on Rare and Complex Connective Tissue and Musculoskeletal Diseases involves health care providers (HCPs) from 8 European countries and 7 patients’ representatives of European Patient Advocacy Groups. The objective was to evaluate current practice and unmet needs for patient education (PE) in Europe.
Methods
A questionnaire was sent to HCP members asking about the PE practices and another, to enquire about their needs, was sent to patients’ associations in the different countries.
Results
The questionnaire was completed by 33 HCPs. Half had no specific staff members dedicated to PE. For HCPs with dedicated staff, 83.3% (n = 11) considered that care providers were insufficient to meet patients’ needs. Most of HCPs would like to see the practice of PE standardized. Sixty eight percent (n = 1093) of patients suffering from connective tissue diseases completed the questionnaire had never heard about PE. Most of them were interested in taking part in a PE program.
Discussion
Our survey revealed a strong interest in PE among patients and HCP and heterogeneity of practice. PE appeared important for both HCPs and patients. An online course for medical students in Europe will be developed in partnership with EULAR to respond to these unmet needs.
Introduction
A chronic disease can be defined as a systemic impairment that is evolving slowly and is not curable at this time. This implies that patients will have to deal with their disease for a couple of years or more and need a clear understanding of their disease to allow them to manage it more effectively. Chronic diseases represent the major share of the disease burden in Europe and are responsible for 86% of all deaths. 1 They have repercussions on several aspects of life. In physical terms, they can cause motor impairment, 2 and from a psychological perspective, they can cause anxiety and depression. 3 They can also affect family and social relationships, generating stress and tension. 4 From an economic point of view, chronic disease has a huge impact in terms of the employment rate of persons with long-standing health issues. 5 At the 2011 New York Conference of the United Nations high level meeting on noncommunicable disease prevention and control, a report was requested from the World Economic Forum and the Harvard School of Public Health to assess the economic cost of chronic diseases: it was estimated at $2 350 billion a year. The report concluded that chronic diseases are among the major global threats to economic development. 6
These repercussions are equally valid for rare and complex connective tissue and musculoskeletal diseases (rCTDs). Collectively, autoimmune diseases are estimated to afflict over 7% of the general population.7 The ERN ReCONNET (European Reference Network on Rare and Complex Connective Tissue and Musculoskeletal Diseases) involves health care providers (HCPs) from 8 EU countries: Belgium, France, Germany, Italy, The Netherlands, Portugal, Romania and Slovenia, and 7 patients’ representatives of European Patient Advocacy Groups (ePAGs). 8 rCTDs have a major impact on patients and society because of their burden of morbidity and mortality. Specific goals of the ReCONNET network activities are to increase empowerment and engagement of patients in the management of their disease; to improve and acquire new knowledge on these conditions; to identify standard, costeffective and sustainable pathways for the management of rCTDs. These missions meet the objectives of patient education (PE). The aim of PE is to help patients with a chronic disease to improve their quality of life and the way they manage their disease. PE was defined in 1998 by the World Health Organization. 9 PE introduces the notion of self-management in collaboration with medical staff, helping patients to cope with their chronic disease and establish better communication with others, including in society and in a hospital setting. PE programs have the dual goal of improving competence of patients as well as providing healthcare providers with specific communication strategies aimed at understanding patients’needs and empowering them. PE is a tool that also reduces the cost of managing a chronic disease. 10 According to the Agency for Healthcare Research and Quality, “patients who have a clear understanding of their after-hospital care instructions […] are 30% less likely to be readmitted or to visit the emergency department than patients who lack this information”. 11 PE is not only beneficial to improve patient satisfaction, it also has a financial impact.
PE can be performed in four steps: educational diagnosis, development of a personalized program, implementation of this program and evaluation of the skills acquired. The aim of an educational diagnosis is to identify processes used by the patient to cope with the chronic disease; the patient’s needs, resources and difficulties; and the skills he/she needs to acquire. This information then serves as the basis for developing a personalized program. 12
The aim of our study was to obtain a clear overview of current PE practice and unmet needs in European countries, by conducting a survey based on two questionnaires, one sent to HCPs and the other to patients in the corresponding countries.
Methods
A questionnaire in English designed using Google Forms® was made available to HCPs, members of ERN ReCONNET, specialized in rare and complex connective tissue and musculoskeletal diseases, for a month in May 2018, asking them and their medical staff about their current PE practice in their department. Another questionnaire, for patients, was sent to ePAGs for translation into the relevant languages. The questionnaire, in the appropriate language version, was then sent to patients’ associations in the different countries and spread to their members, for six months between August 2018 and January 2019. To be eligible, these patients had to be over 18 years old and had to be affected by a rare and complex connective tissue and musculoskeletal diseases: systemic sclerosis, mixed connective tissue disease, idiopathic inflammatory myopathies, antiphospholipid syndrome, undifferentiated connective-tissue disease, IgG4 related diseases, relapsing polychondritis, systemic lupus erythematosus, Sjögren syndrome, Ehlers-Danlos disease, vasculitis, autoinflammatory disease, primitive immunodeficiency disease. For HCPs and patients, PE was defined as: “a way of helping patients with a chronic disease to manage their life in the best possible way. PE is a continuous process and is an integral and ongoing part of patient caregiving. The purpose of PE is to help patients acquire and maintain the skills they need to take responsibility for their own care and develop their capacity to adapt on a daily basis and so improve their quality of life.”
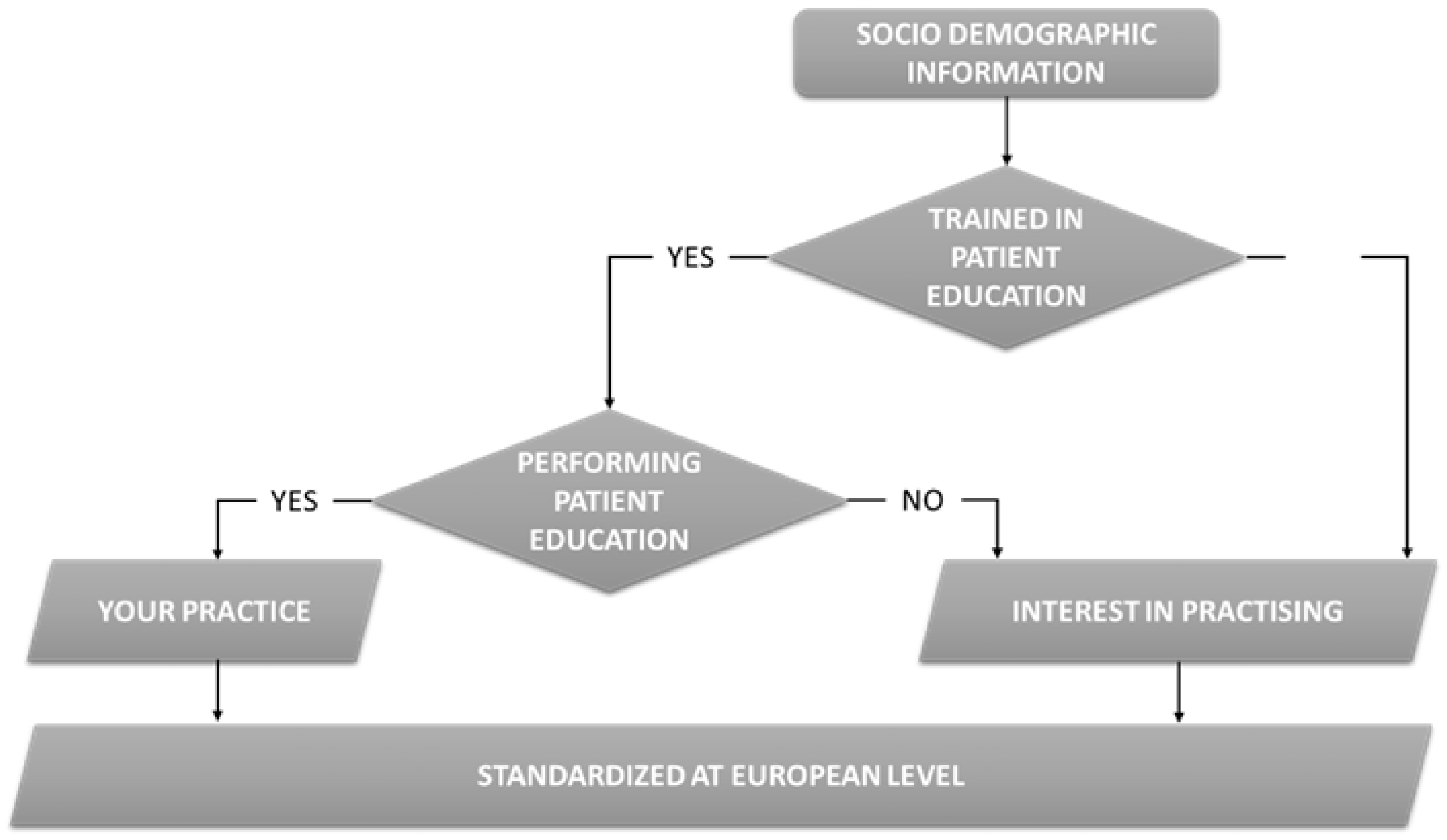
Flow diagram for the survey of HCPs.
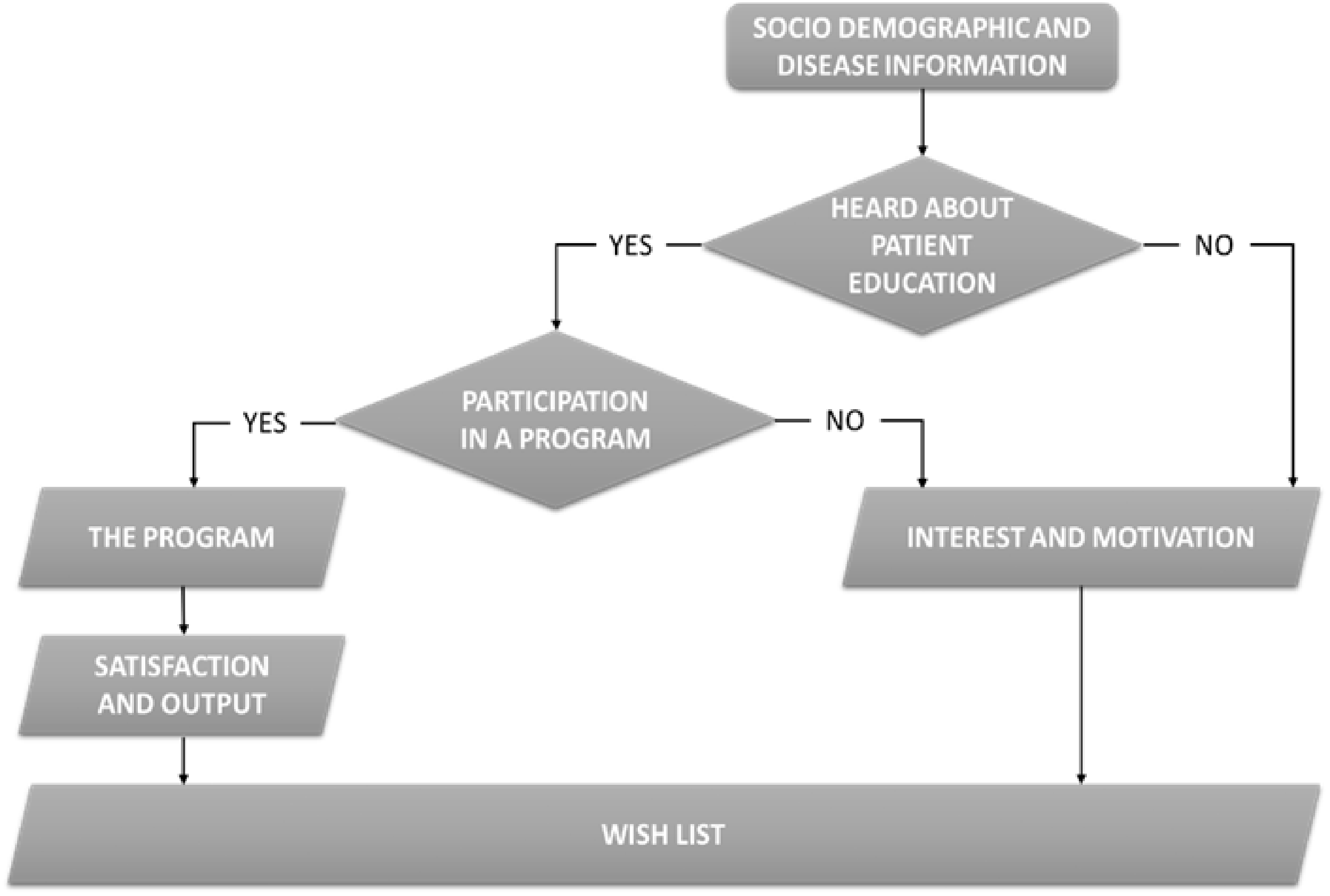
Flow diagram for the survey of patients.
Results
Regarding their PE experience, 58% (n = 19) had no specific staff members dedicated to PE. Thirty-six percent (n = 12) were already trained in PE and 6% (n = 2) had no clear vision of PE practice in their department. In departments with staff trained in PE, 67% (n = 8) had specific PE programs for patients with systemic sclerosis, systemic lupus erythematosus, Sjögren’s syndrome, vasculitis and primary immunodeficiency disease. Among people trained, a majority of nurses (100%, n = 12) were trained in PE, also physicians (75%, n = 9), dieticians (58%, n = 7), psychologists (58%, n = 7) and expert patients (33%, n = 4). They received training of 70 hours (35%, n = 5), 40 hours (21.4%, n = 3) or held a PE University Diploma (35.7%, n = 5). Provision of PE was individualized (25%, n = 3), grouped (25%, n = 3) or mixed (50%, n = 6) (Figure 3).
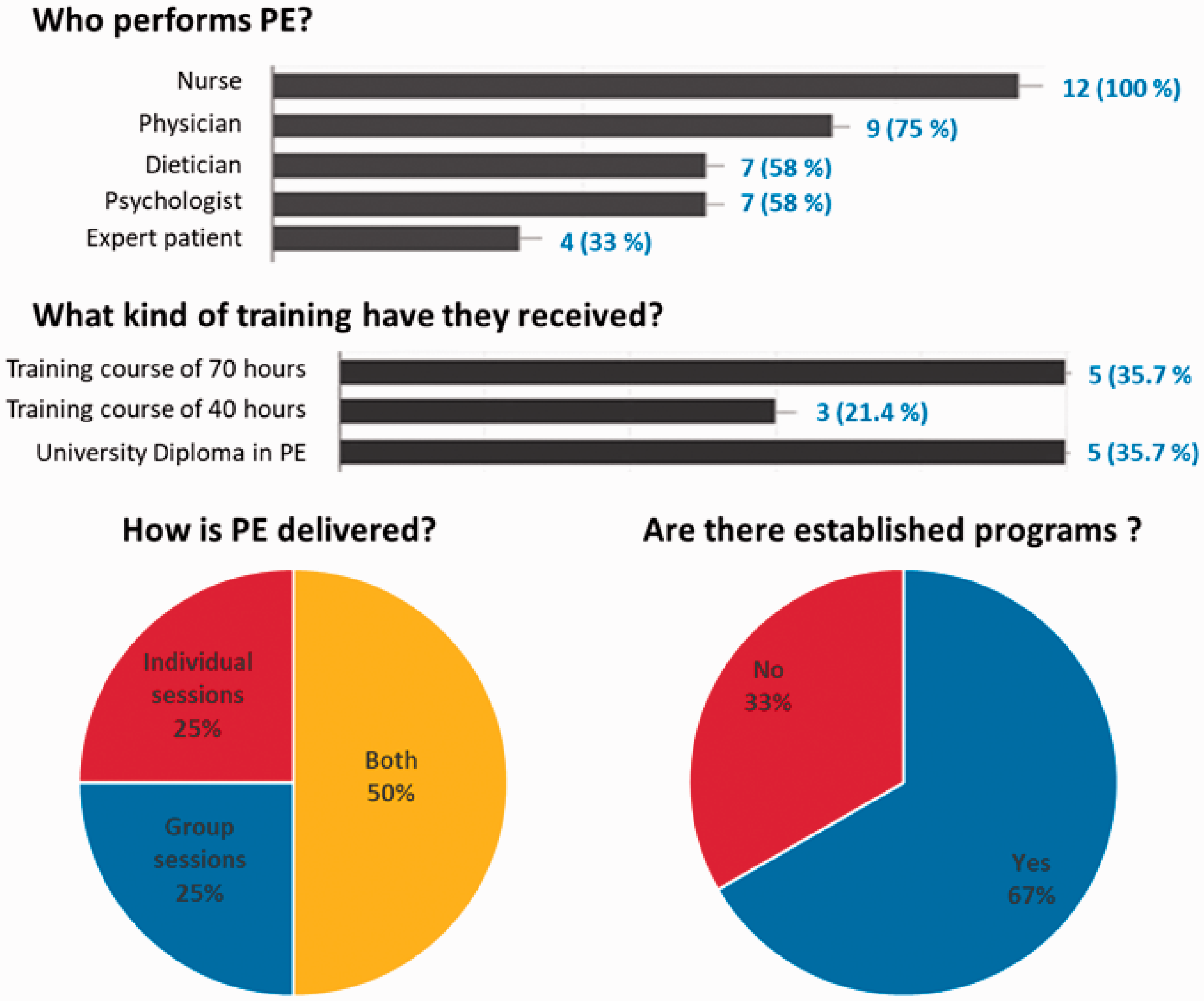
Overview of PE provision in HCPs with trained staff.
HCPs members estimated that they spent at least 2 half-days per month (74,9%, n = 9) organizing sessions of PE.
For HCPs with dedicated staff for PE, 83.3% (n = 10) estimated that the number of care providers were insufficient to meet patients’ needs.
Regarding HCPs who did not have staff trained in PE, they were all interested in receiving PE training (100%, n = 19).
Among HCPs, irrespective of whether they already had dedicated staff for PE, 88% (n = 29) wanted to see the practice standardized at European level.
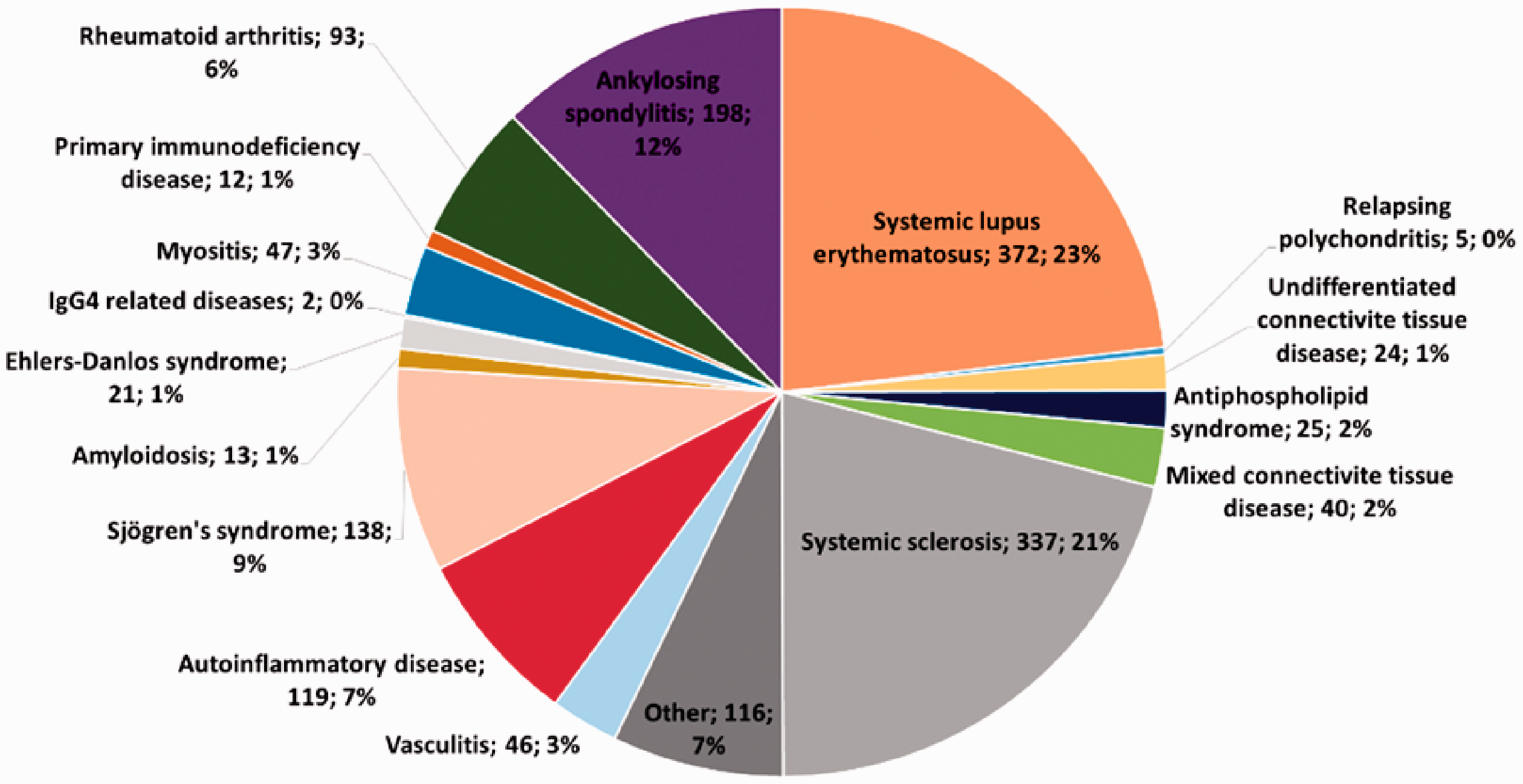
Distribution of patients’ diseases.
Sixty-eight percent (68%, n = 1093) of patients had never heard about PE and 74% of them (74%, n = 808) were interested in taking part in a PE program. Among the patients who had already heard about PE, 32% (n = 164) had been invited to take part in a program and 57% (n = 94) of them actually took part in the proposed program. For this category of patients, they had heard about it mostly from their specialist center (31.6%, n = 29), a patient association (25.8%, n = 24), the internet (25.3%, n = 23) or their general practitioner (9%, n = 8). These proposed programs were mostly for patients with systemic sclerosis (25.4%, n = 16), systemic lupus erythematosus (23.8%, n = 13) and rheumatoid arthritis (20.6%, n = 12). PE was provided in group sessions (82%, n = 77), individual sessions (9%, n = 9) or mixed sessions (9%, n = 8). Ninety percent (n = 85) of patients expressed high levels of satisfaction with the overall program, which focused on several topics (Figure 5).
Topics covered during PE programs.
A majority of patients indicated that the PE program had helped them improve their knowledge of the disease (76%, n = 72). They had also had the opportunity to share their experience of the chronic disease with other patients or directly with their own family (71%, n = 67) and with the healthcare provider (59%, n = 56). The benefits they reported included learning about care and prevention techniques (48%, n = 46), having a better understanding of their treatment (48%, n = 45), feeling more autonomous in the overall management of their disease (n = 40) and feeling less anxious after sessions (42%, n = 40).
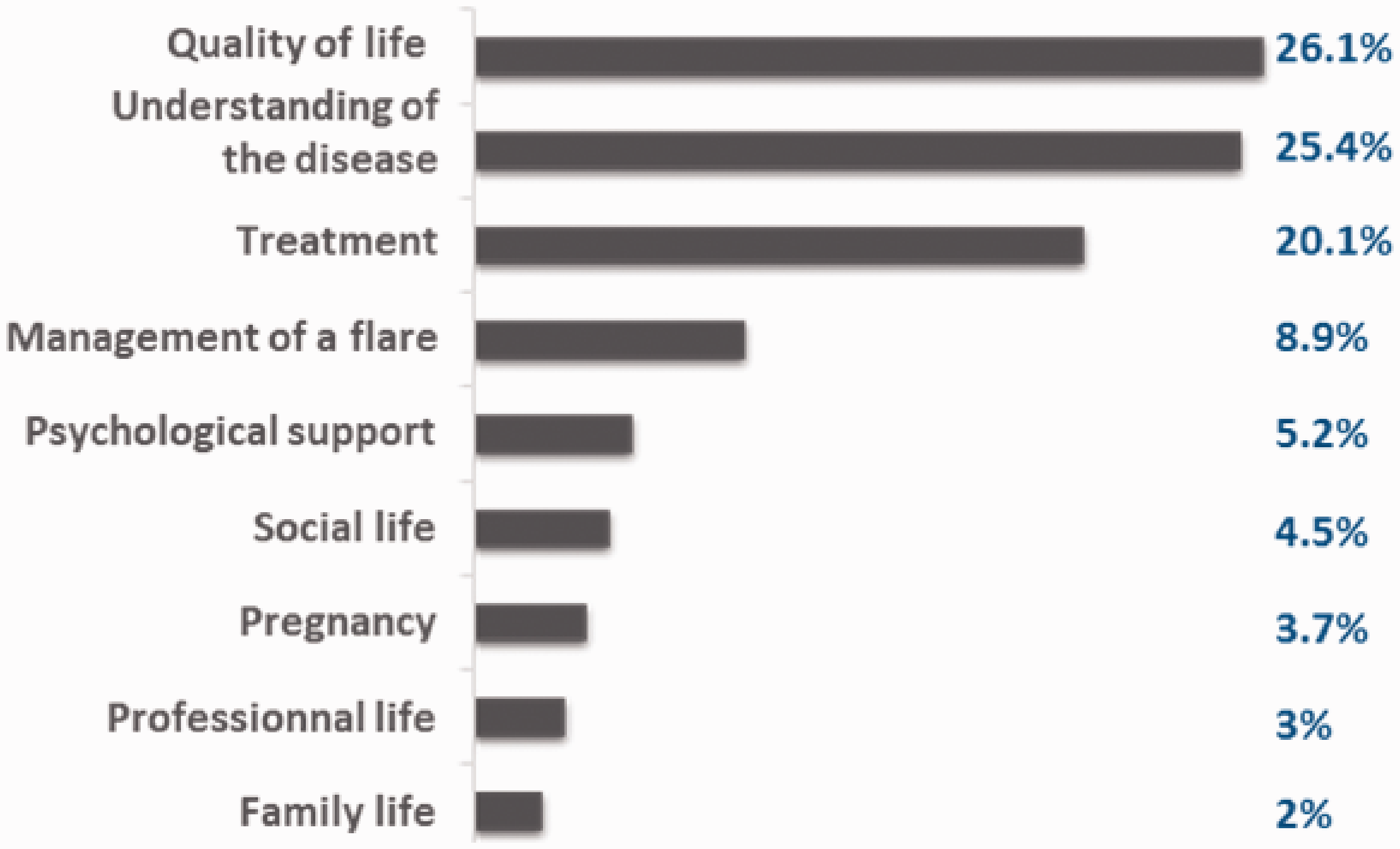
Finally, when all respondents answered the open ended question about their priorities concerning PE, they expressed the need for better knowledge of how to deal with the disease in daily life (55%, n = 882), of treatments (54%, n = 866), of administrative aspects for recognition of their disease (46%, n = 745), of the disease itself and its symptoms (46%, n = 734) and of the impact on their social and family life (44%, n = 711), as well as information on well-being and nutrition (34%, n = 547) and the opportunity to exchange experiences with other patients (38%, n = 604).
When statistics comparisons were made between rCTDs, no difference were found in the percentage of participation to a program or in the benefits of the program.
Discussion
Our study brings to light unmet needs relating to PE provision, as expressed by patients with rCTDs and by their HCPs. To our knowledge, this is the first study to present this dual approach to HCPs’ and patients’ needs relating to PE, especially in case of a rCTDs. Our study demonstrates that both parties have expectations in terms of PE and reveals substantial needs for PE provision around Europe. HCPs expect to receive training in PE and most patients would like to participate in a PE program, showing convergence of needs. This is a major finding, illustrating a convergence between needs and determination. Patients who are able to take a proactive role in their own care, need to understand their chronic illness and work to prevent or minimize its potential complications. PE appears as a good practice to achieve shared decision making, improve understanding and adherence, motivate and encourage self-management. 13 EULAR has established recommendations for the practice of PE for people with inflammatory arthritis. 14
The results of this study show that the practice of PE is still not generalized among rheumatologists, with only 52% of responders having medical staff trained in PE. One of the possible explanations for this result could be the lack of available training and disparities in Europe. Five important factors are identified in the development of PE: research and evidence based standards; the organization of care in the country; training and methodological support; professional values and acknowledgment; funding and the place of PE in health policy. 15
In order to answer this question, it would be interesting to explore HCPs barriers to the provision of PE in their country. Development of PE cannot be done without government will. It may be a gateway to access to care. Regarding the interest shown by HCPs in the practice of PE, there is clearly a need for the development of better communication techniques in the field of health care in Europe. HCPs have the possibility of using the Internet for PE, but they will first need to acquire new skills and knowledge to incorporate this technology into their practice. 16 An online course on PE is due to be developed with four modules to acquire the level of expertise to allow the professional exercise of PE as well as the conduct and animation of project of PE. This online course will be developed to enhance skills in educating patients suffering from rheumatic and musculoskeletal diseases. These four modules will be considered as a formation of 15 hours of e-learning. They will be followed by a concrete application in a service already practicing PE with a defined program. A PE program emphasizes an approach centered on the mobilization of a patient’s resources and the sharing of solutions between peers. This encourages HCPs to acknowledge patients’ expertise and to consider them as a valuable resource for other patients. 17 This leads to the concept of an ‘expert-patient’, a patient who has acquired solid knowledge about his/her illness over time, promoting dialogue with the medical team. 18
In our study, a majority of responding patients (68%) had never heard about PE but most of them were interested in taking part in a program (74%). Our questionnaire was applied in various European countries and the results highlight similar needs among patients with rare and complex connective tissue and musculoskeletal diseases in Europe. Nevertheless, this study showed also a glaring lack of information about PE. Considering Belgium, 16% (n = 30) of patient already had heard of PE while in Slovenia, 63,3% (n = 152) of patient already had heard of it (Figure 6). For patients who had already followed a program, the topics covered were wide-ranging, confirming that PE is a continuous process that requires permanent adaptation related to the evolution of the disease and the experience of its management by the patients themselves, and their own wishes. 19 Patients were mostly glad to have participated in a program. It has already been proved that PE and patient satisfaction are positively related to patient empowerment. 20 The World Health Organization defines empowerment as “a process through which people gain greater control over decisions and actions affecting their health” and this should be seen as both an individual and a community process. 9 Individual empowerment focuses on developing a positive self-concept or personal skills. For an empowered community, individuals and organizations collectively use their skills and resources to meet their respective needs. 21 It is equally relevant to focus on individual empowerment but also on organizational empowerment in the context of health-promoting hospitals. 22 When asked about their PE ‘wish list’, patients reported a need for help with physical concerns and activities of daily living. These findings are consistent with previous research that found impaired health-related quality of life in patients with systemic lupus erythematosus. 23
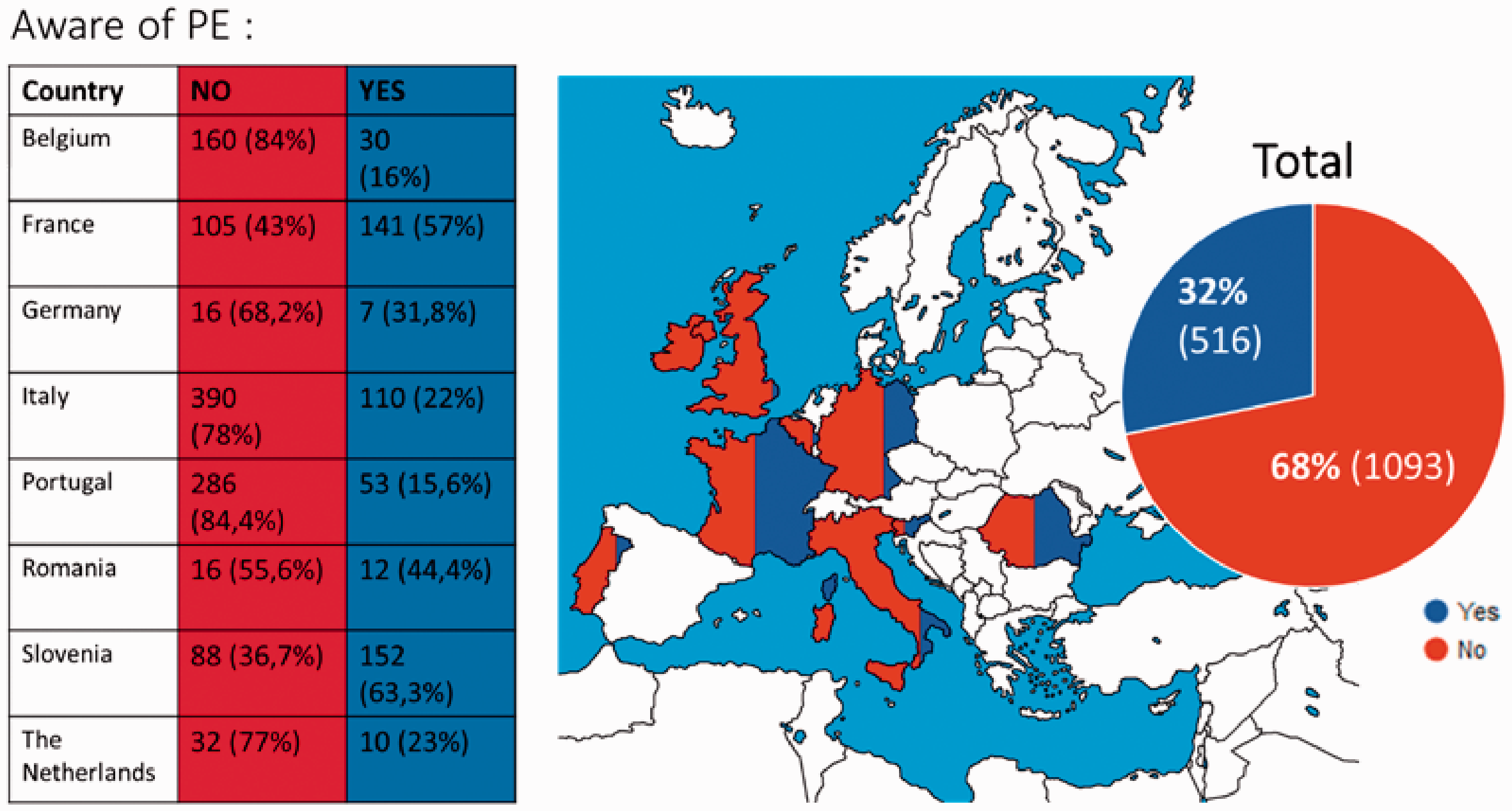
Country inequality of the spread of PE information.
Our study has several limitations. Most of the respondent patients were women, and even if most autoimmune diseases are more frequent in women, 24 this prevents us from extrapolating our findings to unmet needs among men as it has been showed that gender have to be considered for personalized practice of PE. 25 The two questionnaires were based on multiple-choice questions, which limited our ability to consider the potential variety of answers given the personalized nature of PE. Future interventional studies are needed to evaluate a generalized program and to assess the efficacy of a unified program for rare and complex connective tissue and musculoskeletal diseases in Europe.
Conclusion
Our survey revealed a strong interest in PE among patients and HCPs. It appears that current limitations on PE could be overcome if the provision of training were to be generalized or at least rendered more accessible. Our study provides an overview of PE practice in a range of European countries. Our survey of unmet needs in PE reveals heterogeneity of current practice among HCPs and also a strong demand from patients to acquire practical knowledge. This multi-scale study could be the starting point for expanding PE via Patient Associations and health care professionals. With this in mind, an online project to generalize practice of PE in Europe is currently underway.
Footnotes
Acknowledgements
ERN ReCONNET is one of the 24 European Reference Networks (ERNs) approved by the ERN Board of Member States. The ERNs are co-funded by the European Commission. The content of this publication represents the views of the authors only and it is their sole responsibility; it cannot be considered to reflect the views of the European Commission and/or the Consumers, Health, Agriculture and Food Executive Agency (CHAFEA) or any other body of the European Union. The European Commission and the Agency do not accept any responsibility for use that may be made of the information it contains.
Contributorship
MMF and EH built surveys. AC, CF, IG, JG, VG, AV were ePAGs, in charge of the spreading of the questionnaire in Europe. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not required by authors’ institution because the research methods are minimal risk and participation was voluntary.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ERN-ReCONNET is funded by the European Union’s Health Programme (2014–2020).
Guarantor
Meryem-Maud Farhat.
Informed consent
Potential participants were provided with information about the study purpose and the voluntary nature of participation. Informed consent was thus implied by completing and returning the questionnaire.
Trial registration
Not applicable.