
Abstract
Objectives
Chronic disease accounts for 70% of U.S. deaths, with suboptimal nutrition an important, preventable risk factor. Food insecurity is a contributor to poor nutrition. Food pantries are a regular source of groceries for the food insecure and an ideal place for nutrition literacy programs. Supporting Wellness at Pantries (SWAP) is a stoplight nutrition ranking system based on 2015–2020 Dietary Guidelines, but has only been implemented in urban areas. Rural communities experience higher rates of poor health and food insecurity.
Methods
This study implements SWAP at a food pantry in a rural community with high rates of food insecurity and chronic disease. Food was sorted into “green,” “yellow,” and “red” items on color-coded shelves, with green foods the most accessible, and signage explaining the sorting was displayed. Surveys measured whether clients found SWAP helpful in choosing nutritious foods, particularly for households with chronic diseases.
Results
Clients reported that it was significantly (p <.0001) easier to choose items low in salt, sugar, and fat. The benefits of SWAP extended outside the pantry by increasing confidence in choosing nutritious foods while grocery shopping.
Discussion
SWAP can be an effective tool for improving nutrition literacy among food insecure rural residents with chronic illnesses.
Keywords
Background
Food insecurity is a major determinant of health and disease, including chronic non-communicable diseases (NCDs),1,2 which account for approximately 70% of deaths in the United States. Food insecurity is linked with suboptimal nutrition, identified as the most important preventable NCD risk factor. 3 In 2019, 10.5% of all households in the U.S. were affected by food insecurity. 4 However, food insecurity is not distributed proportionally across the American population. Rural residents—one in five Americans—have historically faced health and food access issues at rates much higher than their suburban and urban counterparts; 4 while 63% of U.S. counties are rural, rural counties represent 79% of counties with the highest rates of food insecurity. 5
Rural residents also have higher rates of diet-related NCDs like hypertension and type 2 diabetes, 6 and are more likely to have multiple chronic conditions. 7 As the burden of NCDs continues to grow, from both a quality-of-life and healthcare cost perspective, practitioners increasingly argue that prevention in the form of adequate nutrition is both the most cost-effective and practicable approach to reducing the impact of NCDs. 8 Unfortunately, educating individuals on nutrition and diet modification will only go so far; if foods are not accessible, affordable, or available, then disease-prevention efforts will not be effective.
Distance between food stores is often greater, and ability to travel to these stores more difficult, in rural spaces; road conditions, lack of adequate infrastructure or public transportation, and fuel prices can be barriers to commuting long distances for food. 9 Minimal population density in rural areas can contribute to poor availability of food choices when shopping, as rural stores may not keep vast varieties and quantities of foods on shelves if fewer people will be coming through the doors. 10 In general, food stores in areas with high rates of poverty tend to stock foods that are less nutritious but more filling or energy dense; this is a prime example of the lack of availability of nutritious foods—even when “food” more generally is available—that food insecure populations can face.11,12 Rural households have also historically experienced lower incomes and higher rates of poverty. 13 Rural residents tend to be older due to out-migration of the younger population, and are more likely to find themselves in poorer financial situations, as there is often less economic stimulation and lower educational attainment in rural areas. 9 Further, food prices are sometimes higher in rural areas due to geographic isolation. 9 Thus, even when there are food stores in rural areas, the food may not be affordable.14,15
In face of this limited access to affordable, nutritious food, many households rely on food assistance such as food banks and pantries, organizations that directly serve communities by providing free food to those in need. 16 Together, food banks and pantries serve more than 45 million Americans annually. 17 Although these organizations are intended as an emergency provisioning system, most food pantry clients utilize them month-to-month. 17 Because of this great demand, and difficulty obtaining donations, the traditional focus of the food pantry system is providing users with an adequate quantity of food, with less attention paid to nutritional quality. 18 However, these organizations have the potential to address suboptimal nutrition in other ways, including via health education, disease screenings, cooking classes, and other programs.19,20 These efforts may be especially important because individuals who frequently visit food pantries face higher levels of hypertension and/or diabetes than the general population. The majority of food pantry users have at least one household member with hypertension, while about 30% report a household member with diabetes. 18
One such initiative is the Supporting Wellness at Pantries (SWAP) system, designed to integrate within local food pantries to encourage healthful living. 17 The SWAP system utilizes a stoplight approach to encourage clients to choose nutritious options when shopping in food pantries. 15 A unique component of SWAP is its focus on educating food pantry staff/volunteers on how to determine the nutritional quality of foods, in addition to educating food pantry users. The SWAP system was developed by Dr. Katie Martin and a team of nutritionists at St. Joseph University in collaboration with Foodshare, a food bank in Hartford, CT. Martin et al. implemented SWAP in six urban food pantries in the Northeastern U.S.; major pantry stakeholders reacted very positively, with most survey respondents indicating that they like the system and found it easy to use from an administrative standpoint. 15
However, prior to this study, SWAP has not been implemented in any rural food pantries. Since food insecurity and NCDs disproportionately affect rural areas, it is important to evaluate whether SWAP would also be beneficial in rural areas. Using the stoplight system to “make the healthy choice the easy choice,” rural food pantries could increase self-efficacy in choosing nutritious foods while they provide direct food assistance. This study is an implementation of the SWAP system at a food pantry in a rural county with high rates of food insecurity and NCDs in North Carolina. The food insecurity rate in the county is 15%, 21 higher than national and state rates, while the poverty rate is 18%. 22 This county also experiences mortality due to NCDs, including heart disease and diabetes, at higher rates than in North Carolina overall. 23
Methods
This study was a pre-post implementation assessment of introducing SWAP at a rural food pantry, approved by the Institutional Review Board at Campbell University. At the study site food pantry, clients must prove county residence annually and show a photo ID during each visit. There are no other restrictions on use of the pantry. The aims of this study are to assess food pantry staff willingness to employ the SWAP system, evaluate client perceptions of the SWAP system, and determine whether clients, particularly those affected by chronic diet-related diseases, found the system helpful to them in choosing foods low in saturated fat, salt, and sugar. Given the positive feedback to the program in urban areas, it was expected that staff/volunteers at this rural pantry would be open to the program due to the ease of use, and that clients would also respond positively and find the system helpful.
Pre-surveys, originally designed and used by the creators of the SWAP program, were administered to food pantry clients in the week prior to implementation of the SWAP system. At the time, the pantry was open three weekdays and one weekend day per week for five hours each day; the survey was administered during all five hours on all four of these days. All clients who entered the food pantry during these hours were eligible to complete the survey. During checkout, clients were asked if they were willing to participate in a short survey about their use of the food pantry. If interested, they were asked to confirm that they were over 18 years of age and read a verbal consent document; if consent was given, clients were given a paper copy of the survey to fill out. Pre-surveys asked about clients’ awareness of current nutrition signage at the pantry, whether the pantry helps them to choose foods low in sugar, salt, and fat at the pantry, perceptions of volunteer knowledge of healthy foods, and whether the pantry helps clients choose healthy foods when shopping at the grocery store; these questions were scored in a 5-point Likert scale, with 1 being “strongly agree,” and 5 being “strongly disagree.” This scoring system was used to reduce potential for left-side or acquiescence bias. The survey also included yes/no questions regarding whether anyone in each participant’s household has diabetes or high blood pressure. No other demographic data were collected.
After collection of pre-surveys was complete, volunteers and staff at the pantry assisted in implementing SWAP after business hours over two days. The amount of sodium, sugar, and saturated fat of each canned good, dry good, dessert, and grain item available at the pantry was evaluated, and each food assigned as green (“choose often”), yellow (“choose sometimes”), or red (“choose rarely”) based on the SWAP guidelines. On each shelving unit, green foods were assigned the top shelf, yellow foods the middle, and red foods the bottom. Shelves were color coded using colored masking tape along with labels provided in the free SWAP toolkit. Additional inventory unable to fit on the front-of-house shelving was sorted into green, yellow, and red groups and placed on color-coded shelves in the storage areas of the pantry, to allow pantry staff and volunteers to quickly restock shelves according to the SWAP system. Pantry staff and volunteers were trained in using the SWAP toolkit to determine a food item’s category and where to place it. They were also educated on the impact SWAP could have on clients’ health outcomes, for example how high sodium foods can contribute to high blood pressure. This enabled staff and volunteers to explain to clients why certain foods were categorized in certain ways, which may help clients understand which foods should be monitored or avoided if they have certain medical diagnoses. Finally, signage explaining the stoplight system was placed around the food pantry; prior to this, there was no nutrition signage in the pantry.
A week after implementing SWAP, post-surveys were administered during the same time periods as the pre-survey, all five hours on each of the four days the pantry was open that week. The post-survey assessed clients’ awareness of the new system, their perceptions of whether it helped them choose foods low in sugar, salt, and fat, and whether clients had anyone in their household with diabetes or high blood pressure. The post-survey included an additional question not on the pre-survey, “how do you feel about the stoplight nutrition signs in the pantry?” Pre- and post-surveys were not paired. At this food pantry, clients can visit once per week; therefore, participants may have filled out one or both surveys. While serving as a volunteer, the lead author engaged in informal conversations with clients and staff. Limited qualitative feedback on the SWAP system and ease of implementation was also collected by writing notes documenting this feedback immediately after shifts.
Data were analyzed using R version 3.2.2. 24 Scale scores for each question were computed from each Likert scale question, reversed such that 1 indicated a negative “strongly disagree” response while 5 indicated a positive “strongly agree” response, and compared between pre- and post-implementation surveys using unpaired t-tests, with a significance level of p < 0.005. Percentages of survey participants that had at least one household member with either diabetes or hypertension were calculated. Analyses were also stratified by the presence of a household member with diabetes, high blood pressure, or both to assess the potential role of SWAP in chronic disease management.
Results
The pre-survey was completed by 198 participants and the post-survey by 195 participants. Because the survey was administered during normal business hours while clients were being served and checked out, it was not feasible for staff and volunteers to track the number of people who declined the survey, though it is estimated that approximately 5–10% of clients chose not to participate. Unpaired t-tests revealed a significance between average pre- and post-survey scores for six of the seven corresponding questions; the results of the t-tests are shown in Table 1. The average score improvement between pre- and post-survey questions was a half point on a scale of 5; noticeability and visibility of nutrition education signage at the pantry showed the greatest improvement with a score increase of over a full point. On the post-survey, 40% of participants reported someone in their household with diabetes, 55% with high blood pressure, and 34% with both diabetes and high blood pressure.
Evaluation of pantry nutrition supports before and after implementation of SWAP nutrition stoplight rating system in a rural food pantry.
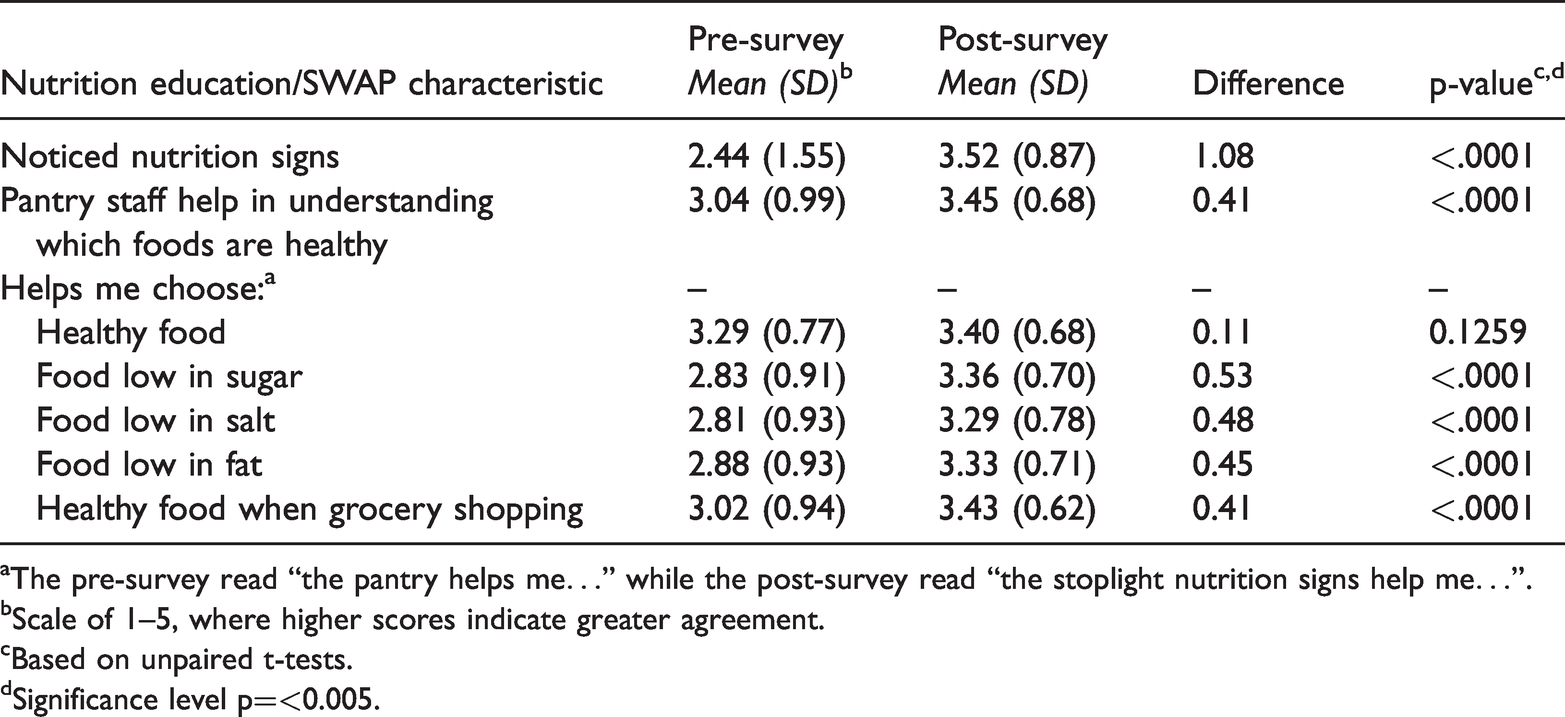
aThe pre-survey read “the pantry helps me…” while the post-survey read “the stoplight nutrition signs help me…”.
bScale of 1–5, where higher scores indicate greater agreement.
cBased on unpaired t-tests.
dSignificance level p=<0.005.
One question on the post-survey did not correspond with a question on the pre-survey; this was a question assessing how well clients liked the new SWAP nutrition signage overall. Nearly all (95%) participants provided positive feedback about the SWAP system; the rest gave a neutral response (“Not sure” how they feel about the stoplight nutrition signs).
Participants in households where someone has diabetes reported a significantly higher score on the question “The stoplight nutrition signs help me choose food that is low in salt” compared to households without diabetes (0.32, p < 0.005). Similarly, participants in households with both diabetes and high blood pressure scored higher on the same question (0.29, p < 0.005). These results are shown in Table 2.
Post-survey scores regarding whether SWAP signs helped rural food pantry clients locate foods low in sugar, salt, and fat by presence of chronic conditions in household.
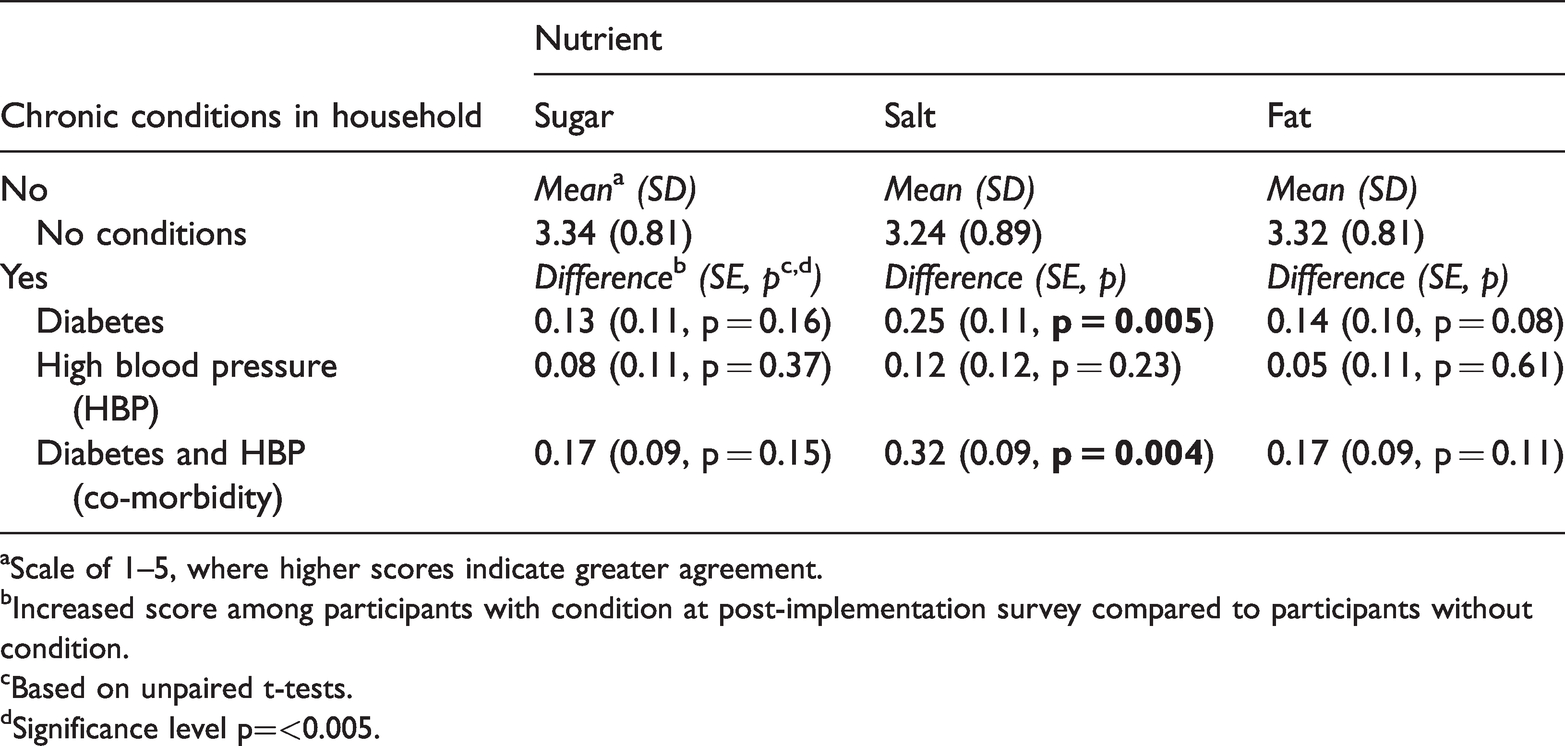
aScale of 1–5, where higher scores indicate greater agreement.
bIncreased score among participants with condition at post-implementation survey compared to participants without condition.
cBased on unpaired t-tests.
dSignificance level p=<0.005.
Participants with diabetes and/or high blood pressure did not report significantly different scores on any other questions, including those about the helpfulness of SWAP in choosing foods low in sugar or fat.
Most clients reported informal positive feedback while filling out, or after turning in, their post-surveys. The most common feedback was that the SWAP system made it much easier to quickly locate foods recommended for clients’ chronic medical conditions, especially regarding foods low in sodium and high blood pressure. While feedback from clients was positive, feedback from staff and volunteers at the pantry was mixed. The food pantry is staffed by only a small number of paid, regular employees; the majority of the workers are volunteers, some temporary and others long term. Due to this unique staffing situation, the pantry greatly depends on the long-term volunteers for operations. In general, the paid staff and newer volunteers were much more willing to implement the SWAP system, while the longer-term volunteers were reluctant to make major changes in operations. For example, one volunteer was concerned that the SWAP protocol was too complicated for everyone to understand and was reluctant to “buy in” to the SWAP process. Many volunteers were used to stocking the shelves certain ways and did not want to have to learn a new process. However, both paid and volunteer staff appreciated the setup in the storage room that made it easier to restock shelves in accordance with SWAP once the initial organization was complete.
Discussion
This project aimed to evaluate the feasibility and perceptions of the SWAP nutrition education system at a rural food pantry. Volunteer commitment to the SWAP system was an unexpected, though minor, obstacle to implementation. Paid staff and shorter-term volunteers were supportive. Once the system is in place, it is easy to maintain, which could reduce volunteer concerns about the program. Clients expressed overwhelming support and positivity regarding the SWAP system, supporting previous research.17,25 Given that this was a small pilot study, however, several areas for tailoring the program depending on food pantry context were identified.
Many contextual factors might affect food pantry clients’ assessments of nutritional education interventions. For example, because the study site food pantry relies partially on donated foods, the quantity and types of foods can vary daily, which could influence program perceptions. Much of the food donated to the food pantry was categorized as yellow or red, leaving the green shelf looking sparse and unappealing, with limited variety. Further, prior to implementation, staff members at the pantry were purchasing foods based on client popularity or what they perceived to be healthy. To promote increased availability of green foods, the SWAP team developed a “Healthy Food Donation List” that recommends certain items over others (e.g. dried or no-salt added canned beans instead of standard canned beans). Moving forward, this list can be handed out as part of an outreach effort to potential donors, and used to direct purchasing foods for inventory, to increase availability and acceptability of green foods at the study site pantry.
Additionally, food insecure households may be more focused on providing energy-dense foods to keep family members full, instead of paying attention to “healthier” options. This highlights the importance of tailoring educational materials to meet the specific needs and concerns of the people utilizing the food pantry. For example, informal conversations with study site food pantry clients revealed that many are particularly aware of and concerned about sodium, and liked learning that rinsing canned vegetables would significantly reduce the amount of sodium in the food. This easy practice that anyone can do at home could bring some lower-category canned goods in line with higher-category nutrient compositions, and help offset instances where green foods are less readily available at the pantry.
Previous research demonstrates that the SWAP system is feasible and popular in urban food pantry settings; this study extends that research into a rural area with positive results. The study is limited by being a small pilot at only one pantry, and focuses on client and staff/volunteer feedback rather than assessing changes in behavior or health outcomes. Future research should explore whether SWAP has an impact on behavioral and nutritional and health-based endpoints, such as by tracking changes in chosen foods, dietary recalls, in-depth qualitative feedback, assessing changes in grocery shopping behavior, or measuring clinical data. Additionally, food preferences, household size, distribution of NCDs in the household, and other contextual factors that vary among different populations in different locations should be taken into consideration and used to tailor the program to best fit the needs of a given pantry’s client base. Finally, some experts recommend that programs like SWAP increase the sodium threshold of canned vegetables specifically, to ensure more of these foods end up on green shelves, encouraging greater consumption of vegetables. 26 Future studies should explore the benefits of using the stricter vs. more relaxed guidelines.
In rural communities, where food insecurity is often alarmingly high, food pantries can be strategically placed and utilized to combat food insecurity. Food pantries also have the potential to minimize the effects of diet-related NCDs by encouraging clients to choose food based on their nutritional value. While a small pilot, this study demonstrates the continued potential of SWAP as an effective tool for this purpose by increasing clients’ self-efficacy in choosing foods low in sodium, sugar, and saturated fat while at the pantry, and in choosing healthy foods when grocery shopping. The SWAP toolkit is free, accessible for pantry staff and volunteers, and intuitive for clients to understand. More food pantries should be encouraged to implement SWAP in an effort to provide nutrition education to the community alongside their primary efforts to reduce food insecurity.
Footnotes
Acknowledgements
We thank Dr. Katie Martin (Executive Director, Foodshare Institute for Hunger Research & Solutions) for contributing the Supporting at Wellness at Pantries signage, educational materials, and survey instruments for use in this study, as well as for her guidance and encouragement in bringing SWAP to our study site.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Institutional Review Board at Campbell University, reference number CUIRB-IRB00009201.
Informed consent
Verbal consent was collected.
Guarantor
LM
Contributorship
JH collected the data, performed data analysis, and prepared the first draft of the manuscript; LM performed data analysis and provided substantive revisions to subsequent drafts of the manuscript.