
Abstract
Objectives
People with chronic illness are particularly dependent on navigating and using the health care system. This requires navigational health literacy (HL-NAV). The article aims to examine the distribution and predictors of HL-NAV in a sample of chronically ill individuals.
Methods
Data of 1,105 people with chronic illness from the general population in Germany were collected in December 2019 and January 2020. HL-NAV was assessed by 12 items (score 0–100). Bivariate and multiple linear regression analysis were performed.
Results
HL-NAV score was 39.1 (SD 27.3). In bivariate analyses, HL-NAV was lower among chronically ill persons aged 65 or above, with low education, limited functional health literacy, low social status, financial deprivation, poor social support, multiple chronic conditions, and an illness duration of 6–10 years. In multivariate analyses, advanced age, lower education, less functional health literacy, lower social status, and less social support remained associated with lower HL-NAV.
Discussion
The results underline the importance of promoting HL-NAV among people with chronic illness. Strategies should aim at strengthening individual competencies taking into account the social and situational factors but also at reducing the demands placed on chronically ill people by providing user-friendly and trustworthy information on the health care system along the illness trajectory.
Introduction
Chronic illnesses create an urgent need for health care, which becomes more extensive and multilayered during the illness trajectory,1–3 necessitating the involvement of numerous health professions and health care providers from different sectors of the health care system. 4 However, it is challenging to navigate the health care system and find the right place at the right time to best address the given individual health situation,5–8 since health care systems in many countries, including Germany, are characterized by high complexity, a lack of transparency, and fragmentation.9–11 To successfully navigate the health care system, users, and especially those who are chronically ill, need navigational health literacy (HL-NAV).
The term “health literacy” generally refers to “people's knowledge, motivation, and competences to access, understand, appraise, and apply health information in order to make judgments and take decisions in everyday life concerning health care, disease prevention, and health promotion.” 12 As this definition of health literacy is rather general, it is difficult to draw practical conclusions for specific contexts in which health information needs to be managed. Thus, there has been a growing trend toward context-specific conceptualizations and measures of health literacy13,14 such as medication, coronavirus-related, and digital health literacy.15–17 Following this development, HL-NAV can be understood as “people's knowledge, motivation, and skills to access, understand, appraise, and apply the information and communication in various forms necessary for navigating health care systems and services adequately to get the most suitable health care for oneself or related persons.” 18
To date, knowledge about HL-NAV in general, but especially in Germany, is scarce. Only a few studies have addressed parts of the abovementioned HL-NAV conceptualization. Rudd et al. 19 included literacy tasks regarding rights and responsibilities, application for insurance and other coverage plans, and informed consent for procedures as “systems navigation” among the five health literacy activities on the Health Activities Literacy Scale (HALS). However, the HALS is based solely on a functional understanding of health literacy, and the resulting score does not distinguish between its different activities. Osborne et al. 20 operationalized “navigating the health care system” as one of nine sub-dimensions of their Health Literacy Questionnaire (HLQ), referring to the ability to find out about services and support, and to advocate within the health care system on one's own behalf. Navigation sub-scores showed an association with some demographic and also illness-related characteristics.21–23 However, it does not explicitly refer to the core focus of health literacy, which is managing health information. 12 For a detailed description of the HL-NAV concept, instruments, and studies, see Griese et al. 18
Thus, the topic was included in the International Health Literacy Survey 2019–2021 (HLS19) administered by the World Health Organization (WHO) Action Network on Measuring Population and Organizational Health Literacy (M-POHL) in which general and specific health literacies were measured in up to 17 countries in the wider WHO region of Europe. 24 Germany participated in the HLS19 with the Second Health Literacy Survey for Germany (HLS-GER 2). 25
This article provides a partial analysis of the HLS-GER 2 data on HL-NAV among people with chronic illness.
Purpose
The purpose of this article is to examine HL-NAV among people with chronic illness. Specifically, the following questions are addressed: (1) How is HL-NAV distributed in a sub-sample of chronically ill individuals from the general population in Germany? (2) What population groups among people with chronic illness show comparatively low HL-NAV? (3) What are the predictors of HL-NAV according to the integrated model of health literacy? 12
Methods
Participants and data collection
For these analyses, HLS-GER 2 data were used. The HLS-GER 2 is a representative quantitative cross-sectional survey measuring general and specific health literacy as well as important co-variables in Germany's general German-speaking population aged 18 and above. Data were collected from December 2019 to January 2020 using paper-assisted personal interviews (PAPI). Sampling points in administrative regional units (NUTS2 level), considering population density, were randomly selected. In the respective areas, respondents were recruited using a community-based quota sampling approach, with a quota for gender in combination with age, household size, and education. Participants provided verbal informed consent, which the interviewers verified and documented. Ethical approval for this study was obtained from the Ethics Committee of Bielefeld University (No. 2019-103). A total of 2,151 persons from the general population participated in the HLS-GER 2. The response rate in this study was 63.4%. For this study, data from 1,105 participants reporting at least one chronic illness or long-term health problem (≥6 months) were filtered from the unweighted main dataset.
Measures
HL-NAV. HL-NAV was measured with a newly developed instrument, the HLS19-NAV.18,24 It includes 12 items asking participants to indicate on a 4-point Likert scale (from 1 = very difficult to 4 = very easy) how easy it is to access, understand, appraise, and apply information about navigational issues in the health care system. The answers were dichotomized for analysis (i.e. “easy” and “very easy” combined), summed, and scaled to a unified metric (0–100). The calculated index thus indicates the percentage of items that were answered with “easy” or “very easy,” where a higher score indicates higher HL-NAV. The instrument was successfully applied and validated in eight different countries (including Germany). 24 The instrument's internal consistency for the presented sample can be rated as high, with a Cronbach's α of 0.873.
Socio-demographic and economic characteristics
Age, gender, educational level, functional health literacy (FHL), social status, financial deprivation, and migration background were included. Educational level was assessed using the International Standard Classification of Education 2011 (ISCED-11), which describes the highest educational attainment acquired across nine levels. 26 For descriptive analyses, levels 0–2, 3 and 4, and levels 5–8 were classified as a low, medium, and high educational level, respectively. FHL was measured using the Newest Vital Sign (NVS) test 27 This performance-based measurement assesses basic literacy and numeracy skills using a food label. The NVS score is within the range of 0–6 and is calculated based on the number of correct answers. Scores were grouped into three categories (0–1 = high likelihood of limited FHL, 2–3 = possibility of limited FHL, 4–6 adequate FHL). To assess social status, participants were asked to rate their position in society, where 1 indicates the lowest position and 10 indicates the highest position. 28 Values in the ranges 1–4, 5–7, and 8–10 were classified as a low, medium, and high social status, respectively. The extent of financial deprivation was measured according to responses to three questions (How easy or difficult it is to (1) afford medication if needed? (2) afford medical examinations and treatments, if needed? (3) pay all bills at the end of the month?), which were answered on a 4-point Likert scale ranging from “very easy” to “very difficult.” Financial deprivation was assumed if the responses to at least two out of three questions were “difficult” or “very difficult.” Migration background was established if respondents or at least one parent were born outside of Germany.
Social support
Social support was assessed as a situational determinant of health literacy. 12 Therefore, the Oslo-3 Social Support Scale (OSSS-3) was used. 29 The scale comprises three items on the perceived availability of social support (size of primary support group, interest and concern shown by others, and ease of obtaining practical help). Score ranges from 3–14, and values within the ranges 3–8, 9–11, and 12 and higher are considered to represent poor, moderate, and strong social support, respectively.
Variables related to chronic illness
The number of chronic diseases was measured by asking participants about their specific disease(s) based on a list of 26 possible responses (25 frequent health problems and an open option (supplemental material)). Multiple answers were possible, and the number of diseases was counted. In addition, illness duration was assessed. To perform descriptive analyses, the number of chronic diseases was grouped into three categories (1, 2, 3 + diseases) and illness duration was grouped into four categories (<1, 1–5, 6–10, >10 years).
Data analysis
Data were analyzed using IBM SPSS Statistics 25. Descriptive statistics were used to describe sample characteristics, HL-NAV mean scores, and degree of difficulty concerning the HL-NAV information tasks. To identify subgroups with comparatively low HL-NAV, deviations from the total sample's (DM) HL-NAV mean score were computed for each subpopulation. In addition, single population groups’ mean scores were compared using analysis of variance (ANOVA). Subgroups of chronically ill patients were labeled as having low HL-NAV if they had significantly lower HL-NAV mean scores than at least one other subgroup and simultaneously had a lower mean score than the total sample of people with chronic illness. A Bonferroni-adjusted post hoc test was used to adjust for multiple comparisons. Finally, the predictors of HL-NAV were tested using multiple linear regression. All variables were included in the regression model, as previous studies have already proven their theoretical and empirical relevance.
Results
Sample characteristics and distribution of HL-NAV scores of people with chronic illness from the HLS-GER 2 study are presented in Table 1. Overall, the mean HL-NAV score was 39.1. The largest deviations from the total sample's mean score were found in participants with a low level of education (DM: −11.8), a high likelihood (DM: −9.6) or possibility (DM: −4.9) of limited FHL, poor social support (DM: −8.0), low social status (DM: −7.5), an illness duration of less than one year (DM: −9.0) or a duration of 6–10 years (DM: −6.2), financial deprivation (DM: −7.9), aged 65 or above (DM: −3.2), and those with multiple chronic diseases (DM: −2.4).
Sample characteristics and distribution of HL-NAV score.
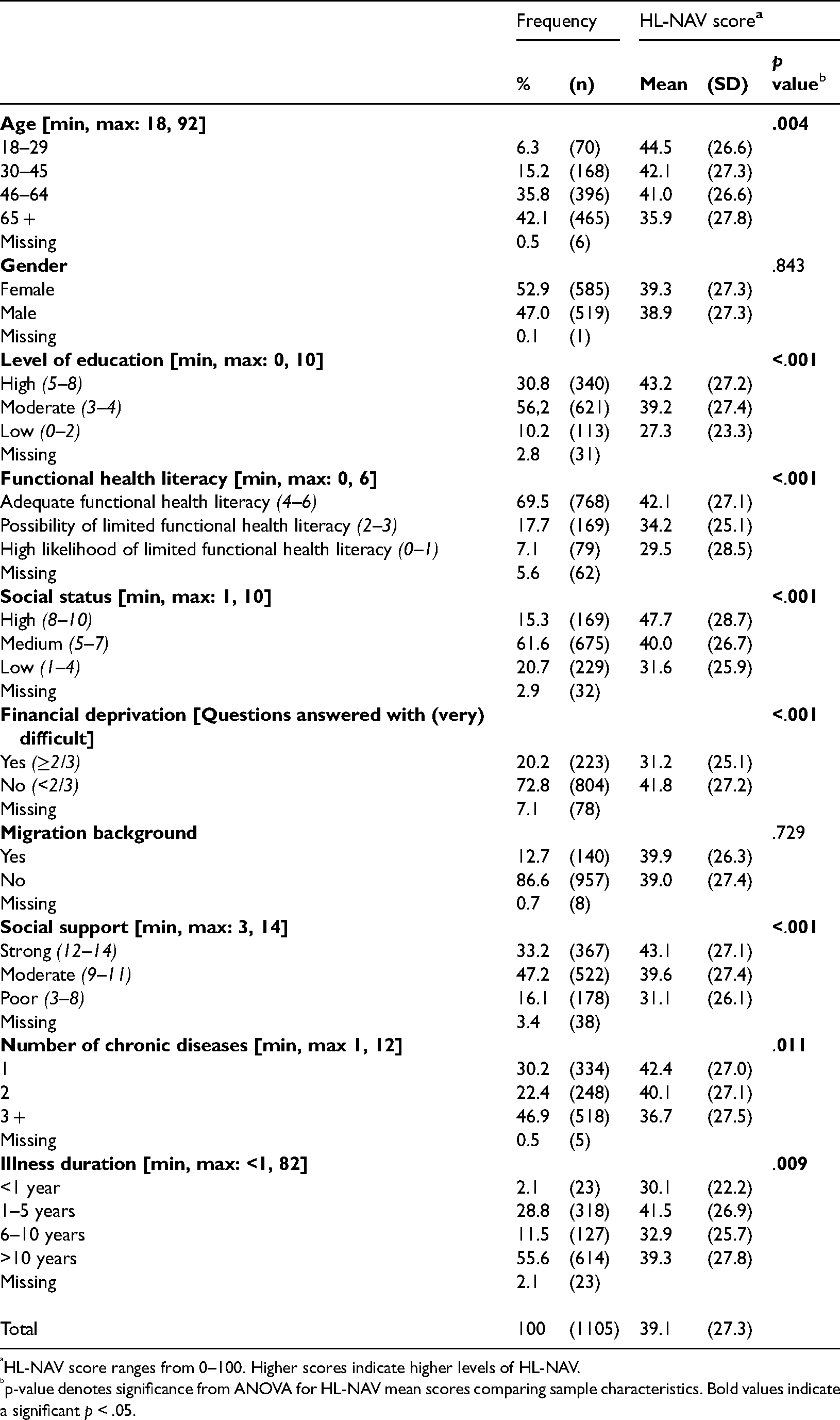
HL-NAV score ranges from 0–100. Higher scores indicate higher levels of HL-NAV.
p-value denotes significance from ANOVA for HL-NAV mean scores comparing sample characteristics. Bold values indicate a significant p < .05.
Regarding subpopulation groups, post hoc analysis (Table 2) indicated significantly lower HL-NAV scores in chronically ill patients aged 65 years or above (mean: 35.9) compared to participants aged 46–64 years (mean: 41.0). Significantly lower HL-NAV was also found in participants with a low educational level (mean: 27.3) compared to those with a high (mean: 43.2) or moderate (mean: 39.2) educational level. For FHL, the lowest HL-NAV was observed in participants with a high likelihood (mean: 29.5) or possibility (mean: 34.2) of limited FHL compared to those with adequate FHL (mean: 42.1). Significant differences were found between all social status groups, with the lowest mean score in participants with a low social status (mean: 31.6). HL-NAV was also lower in participants experiencing financial deprivation (mean: 31.2) than in those without (mean: 41.8) financial deprivation, as well as in participants with poor social support (mean: 31.1) compared to those with moderate (mean: 39.6) or high (mean: 43.1) social support. Regarding chronic illness, participants with three or more chronic diseases (mean: 36.7) had a significantly lower mean score than those with only one disease (mean: 42.4). HL-NAV was also lower in participants with an illness duration of 6–10 years (mean: 32.9) than in those who had lived 1–5 years (mean: 41.5) with chronic illness.
Results of Bonferroni corrected post hoc tests for multiple comparisons (ANOVA).
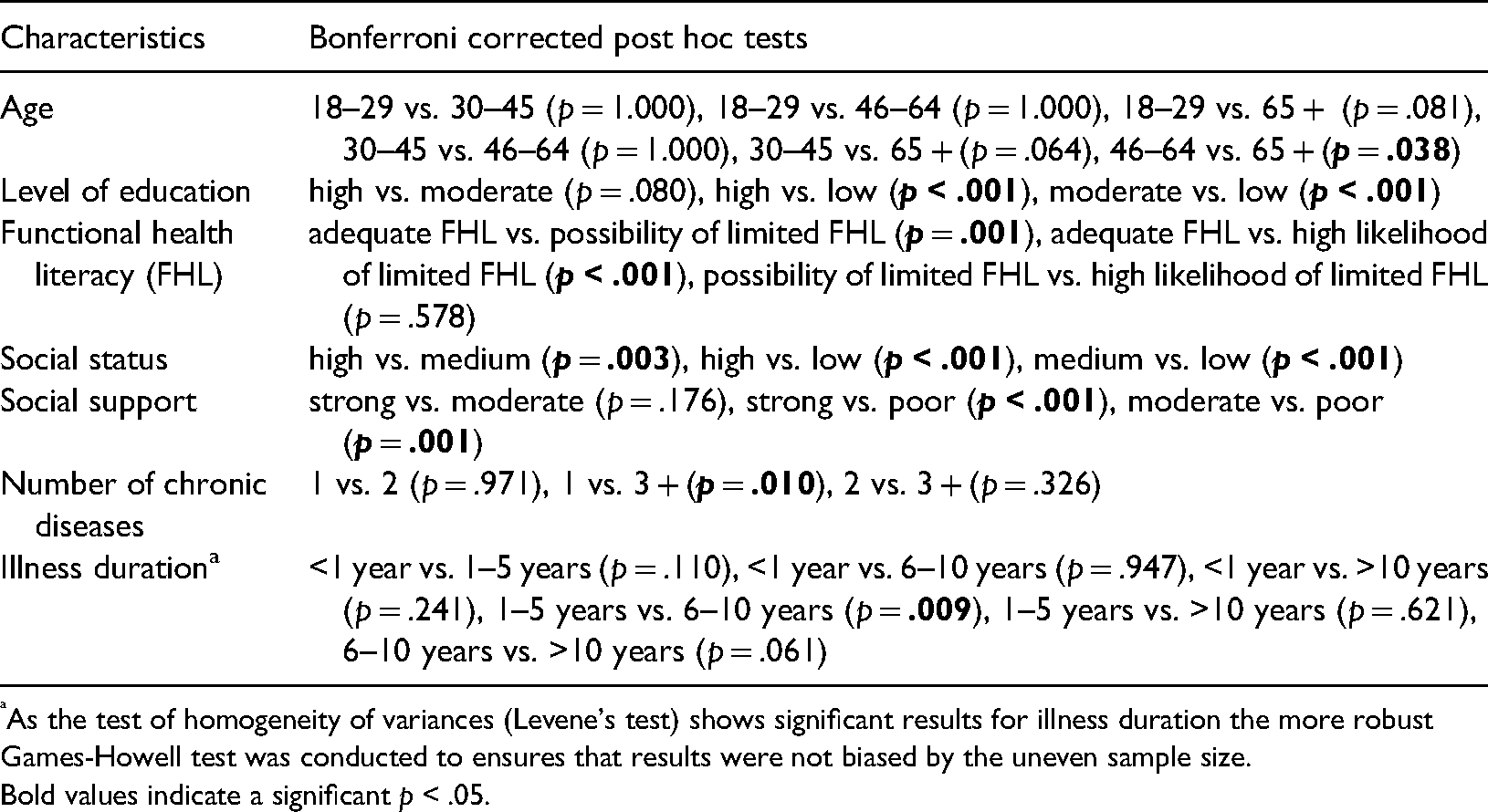
As the test of homogeneity of variances (Levene's test) shows significant results for illness duration the more robust Games-Howell test was conducted to ensures that results were not biased by the uneven sample size.
Bold values indicate a significant p < .05.
verall, HL-NAV information tasks were considered predominantly challenging: 11 out of 12 tasks were rated as “difficult” or “very difficult” by at least half of all participants. The degree of perceived difficulty (“difficult” and “very difficult”) ranged from 74.6% to 29.7% in the total sample (Table 3). Chronically ill persons aged 65 and older consider it difficult to judge whether a particular health service will meet their expectations and wishes in terms of health care (77.0%). Participants with a low educational level (90.3%), a low social status (82.5%), and those experiencing financial deprivation (83.9%) found it challenging to find out about their rights as a patient or user of the health care system. Identifying support options that may help one orientate within the health care system was rated the most difficult by participants with a high likelihood of limited FHL (83.5%). Understanding information about ongoing health care reforms that might affect health care was rated as the most difficult task for participants with poor social support (80.8%), multiple chronic diseases (75.2%), and an illness duration of 6–10 years (81.1%).
Percentage of perceived difficulties on the HL-NAV items.
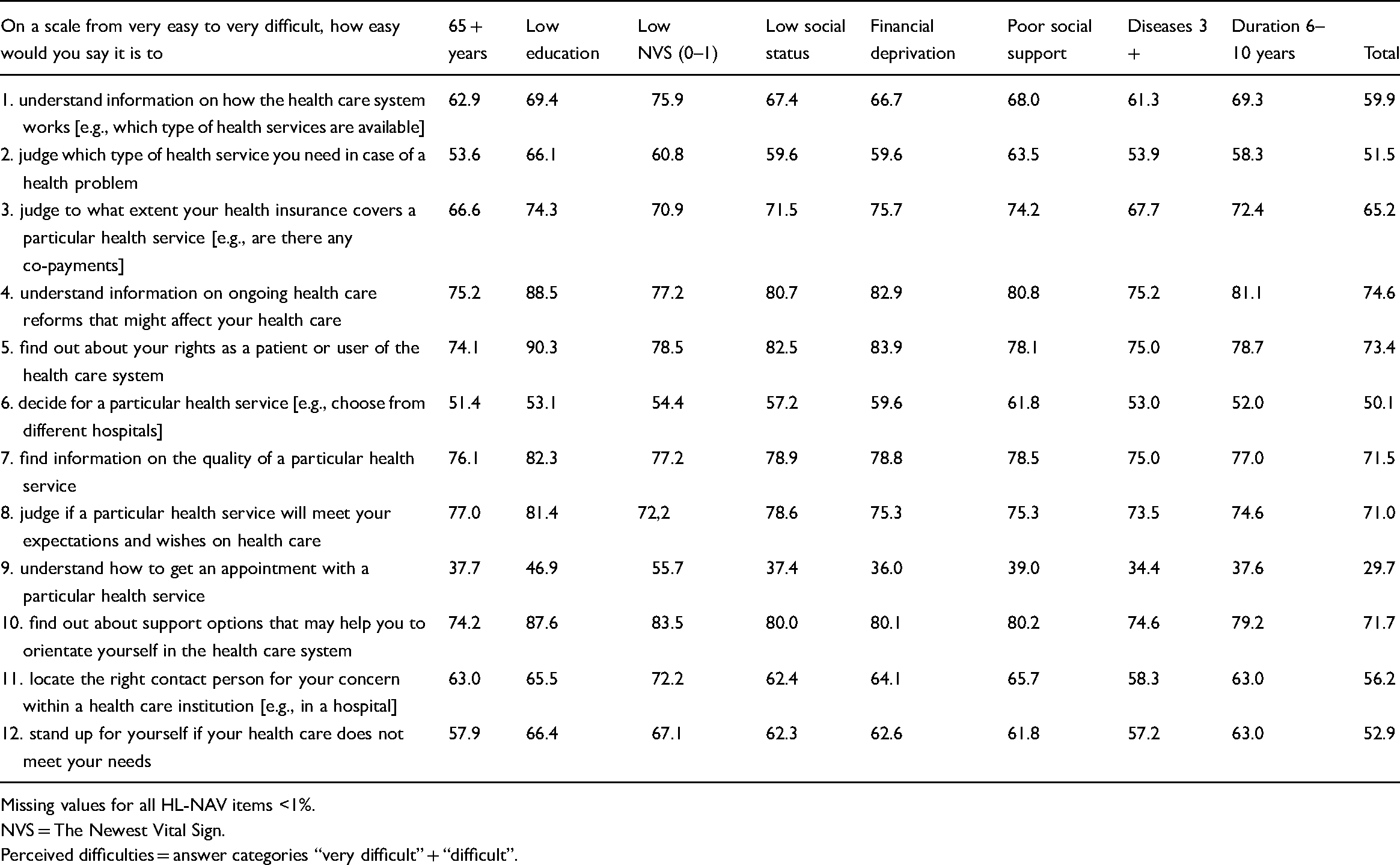
Missing values for all HL-NAV items <1%.
NVS = The Newest Vital Sign.
Perceived difficulties = answer categories “very difficult” + “difficult”.
In multiple linear regression (Table 4), a higher HL-NAV score was associated with lower age (p = .001), a higher level of education (p = .039), higher FHL (p = .003), a higher social status (p < .001), and stronger social support (p = .032). The strongest predictors were social status (β = 0.15), followed by age (β = −0.11), FHL (β = 0.10), education (β = 0.07), and social support (β = 0.07). The model does not show an independent effect on financial deprivation, the number of chronic diseases, and illness duration. The overall model's explained variance was small, with an adjusted R-squared value of 0.095.
Predictors of HL-NAV in multiple linear regression.
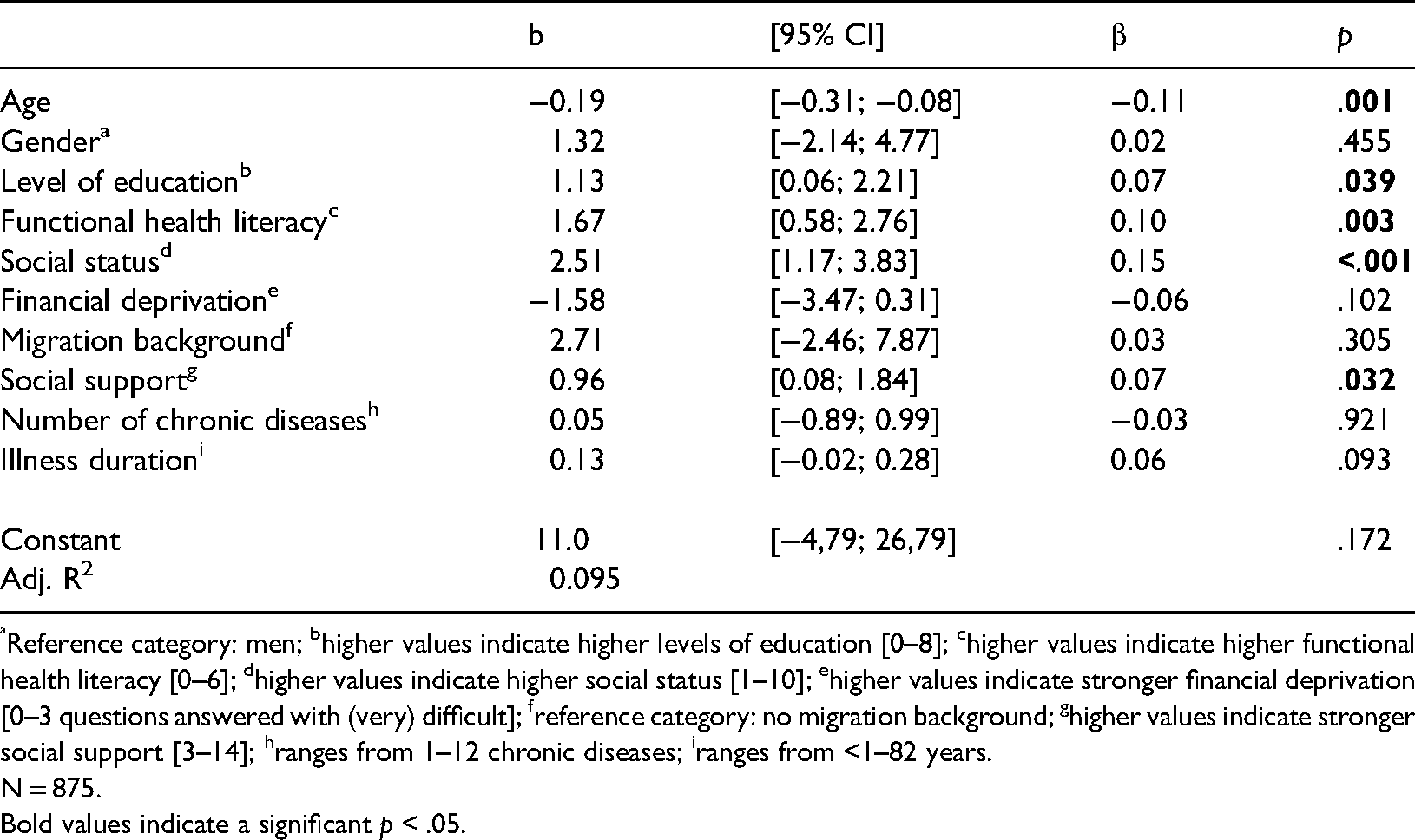
Reference category: men; bhigher values indicate higher levels of education [0–8]; chigher values indicate higher functional health literacy [0–6]; dhigher values indicate higher social status [1–10]; ehigher values indicate stronger financial deprivation [0–3 questions answered with (very) difficult]; freference category: no migration background; ghigher values indicate stronger social support [3–14]; hranges from 1–12 chronic diseases; iranges from <1–82 years.
N = 875.
Bold values indicate a significant p < .05.
Discussion
The analysis provides empirical knowledge of HL-NAV among people with chronic illness in Germany. The key finding was that large portions of chronically ill individuals showed low HL-NAV scores (mean score: 39.1); on average, 61% of all HL-NAV items were rated as “difficult” or even “very difficult.” Thus, their HL-NAV is lower than other health literacies measured in the HLS19 such as general, digital, and communicative health literacy. 24 Therefore, dealing with information about navigating the health care system seems inherently more challenging than other areas in which information has to be managed.
HL-NAV in people with chronic illness is also slightly lower than that in Germany's general population. 24 This confirms a longstanding topic of discussion: The complex health care system, its numerous organizations, and its procedures, which often lack transparency, not only represent a “black box" 30 for many users but also present challenges for people with chronic illness in terms of accessing, understanding, appraising, and applying information about the health care system. This result is surprising because qualitative studies have indicated that people with chronic illness are intensive health care system users who could be expected to be familiar with its realities.31,32 Apparently, the opposite seems to be the case: The chronically ill experience most navigation-related information tasks as difficult. A reason might be that they realize the barriers and challenges associated with receiving the right health care. Furthermore, with the increased complexity of the health care situation, for example, in old age or in the presence of multiple chronic conditions, the need to manage information becomes more extensive, while at the same time, individual resources required to deal with these challenges decrease due to illness and functional limitations.33,34 In this regard, Beauchamp et al. 21 have also referred to the high number of health care providers involved and the resulting “overwhelming” amount of information that people suffering from multiple chronic conditions have to process.
The results also show that HL-NAV is subject to a social gradient. Social determinants already known for general health literacy25,35,36 have been widely confirmed for HL-NAV among people with chronic illness. Thus, an independent relationship has been established between HL-NAV and age, education, FHL, and social status. The effect of financial deprivation in the bivariate analysis vanishes after controlling for other variables. This shows that it is important to design and provide information in such a way that it can also be processed by patients with a low educational level and a low social status, as well as by those with limited literacy. This might help to reduce social inequalities in health, as health literacy acts as a mediator between socio-economic status and negative health outcomes. 37
Another relevant finding was that multivariate analyses found no association between HL-NAV and the duration of chronic illness. Although it is not possible to draw conclusions about the development of HL-NAV over time due to the cross-sectional design, it is hypothesized that HL-NAV is dependent on the illness trajectory and not the mere duration of illness; that is, it is less pronounced in critical phases and periods of uncertainty due to the high requirements placed on the chronically ill during those phases. 3 The relationship between the dynamics of chronic illness trajectories and health literacy should be addressed in further research.
Furthermore, it should be highlighted that social support is related to HL-NAV. This is in line with findings underscoring the importance of this resource for dealing with chronic illness.38,39 There is also evidence that people who receive poor social support are more likely to have lower health literacy.40–42 Therefore, strengthening or expanding existing support systems, for example, through more patient navigation initiatives in Germany, may also help to overcome information barriers to navigating the health care system. Moreover, informal support networks, which are critical to chronic disease management, should be given greater support in promoting HL-NAV.
Finally, it should be noted that HL-NAV is not an isolated competence. HLS19 findings show a moderate association between general health literacy and HL-NAV, pointing to important overlaps between concepts, while simultaneously demonstrating that HL-NAV and general health literacy are not congruent. Therefore, strengthening general health literacy may also prove beneficial for HL-NAV, but HL-NAV goes beyond general health literacy. 24 Strengthening other related capacities, such as engaging with health providers and health professionals’ communicative skills, may also have a positive effect on HL-NAV. The same is assumed for digital health literacy, since navigation-related information and services supporting health care system navigation are largely available online.
Strengths and limitations
In this study, a new instrument for measuring HL-NAV was applied to a relatively large sample of chronically ill patients for the first time. However, there are some limitations that need to be addressed. First, no direction of causality can be seen because of the study's cross-sectional design. Furthermore, although our sample reflects general trends in the distribution of chronic illness in the general population, 43 it does not claim to be representative of people with chronic illness in Germany. It can also be assumed that people with a higher level of interest in health topics were more likely to participate in the survey than those with less interest. However, the community-based sampling approach and personal interviews assured the participation of vulnerable population groups in this study. In addition, HL-NAV was self-assessed in this study. Self-reported difficulties do not automatically mean that tasks cannot be managed in the long term or that the respondents’ personal capabilities are low. Rather, the measurement tool's relational characteristic 44 needs to be considered. This means that personal competencies and structural deficits in information provision within the German health care system were assessed simultaneously. A further limitation is that migration background in this article includes people with and without migration experiences from different countries. Indicators such as the language spoken and culture-related aspects 45 may play a more important role in processing health information than the general operationalization used in this study. In addition, disease type was not considered in the analysis. However, navigation requirements may be highly diverse and disease-specific. This needs to be considered in future research on HL-NAV. Given the overall explained variance of only 9.5%, the identification of additional important determinants of HL-NAV, such as the characteristics of the health care system and its information structures, will be of importance.
Practical implications and conclusions
The results indicate that there is a need to strengthen HL-NAV at all levels of the health care system. In the past, many efforts were made to expand the range of information and counseling services available in Germany. However, these services, as the results indicate, seem to be widely unknown to the chronically ill or difficult to identify. The same applies to information about patient rights and participatory decision making (e.g. on the quality of health services). These issues should be considered in further efforts to strengthen HL-NAV among people with chronic illness. To achieve this, developing target group-specific strategies to strengthen personal HL-NAV is recommended, tailored to consider the social, demographic, and situational contexts of people with chronic illness. At the same time, it is important to reduce the demands placed on the chronically ill with low HL-NAV by providing more guidance and support for navigating the health care system and its related information structures. To this end, it may be useful to invest in health literacy health care systems and organizations (OHL) as well as in more low-threshold accessible, easily understandable, and quality-assured information about the health care system along the entire illness trajectory.
Supplemental Material
sj-doc-1-chi-10.1177_17423953211073368 - Supplemental material for Navigational health literacy among people with chronic illness
Supplemental material, sj-doc-1-chi-10.1177_17423953211073368 for Navigational health literacy among people with chronic illness by Lennert Griese, Doris Schaeffer and Eva-Maria Berens in Chronic Illness
Footnotes
Acknowledgements
The presented study was conducted at Bielefeld University, Germany. The authors would like to thank Prof. Dr. Jürgen Pelikan, leader of the International Coordinating of HLS19, and the members of M-POHL who were involved in preparing the international study.
Contributorship
LG and DS conceived the article and wrote the first draft of the manuscript. EB was involved in reviewing and editing the manuscript and gaining ethical approval. All authors approved the final version of the manuscript.
Ethical Approval
Ethical approval for the underlying study was obtained from the Ethics Committee of Bielefeld University (No 2019-103).
Informed Consent
Participants provided verbal informed consent for their data to be used for scientific purposes.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the German Federal Ministry of Health (Bundesministerium für Gesundheit (BMG)) ( grant number: chapter 1504 title 54401, ZMV I 1-2518 004 (HLS-GER 2).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.