
Abstract
Objectives
This service evaluation explored the experiences of families receiving care in a paediatric chronic fatigue service. The evaluation aimed to improve service provision across paediatric chronic fatigue services more widely.
Methods
Children and young people aged 7–18 years (n = 25) and parents/carers (n = 25) completed a postal survey exploring experiences of a paediatric chronic fatigue service. Quantitative data were analysed descriptively, and qualitative data were analysed using thematic analysis.
Results
Most service usersand parents/carers (88%) agreed that the service met their needs, that they felt supported by staff, and most notably, a large portion (74%) reported the team increased their activity levels. A small number disagreed (7%) with statements relating to positive links with other services, ease of talking to staff and suitability of appointment type. The thematic analysis revealed three themes: help managing chronic fatigue syndrome, experience of professional support and accessibility of service. Families reported benefiting from increased understanding of chronic fatigue syndrome, learning new strategies, the team linking with schools, feeling validated and mental health support. Accessibility was a particular problem including the service location, setup of appointments and difficulty contacting the team.
Discussion
The evaluation presents recommendations for paediatric Chronic Fatigue services to improve service user experiences.
Chronic fatigue syndrome (CFS), also referred to as myalgic encephalomyelitis, is a complex, chronic medical condition characterised by debilitating fatigue, which is not secondary to exertion or significantly relieved by rest.1,2 Concurrent symptoms include post-exertional malaise, unrefreshing sleep or sleep disturbances and cognitive difficulties. 2 A diagnosis can be confirmed after three months of experiencing persistent symptoms that are not explained by another condition. 2 The prevalence rate is estimated to be 0.89% in children and adolescents. 3
Potential triggers for CFS include having a physical illness or experiencing a traumatic event.4,5 Children with CFS present differently from adults, for example, younger children are more likely to have sore throats and adolescents are more likely to have headaches and comorbid depression. 6 Children and young people with CFS experience social isolation, poorer school-related quality of life, difficulty attending school, bullying from peers, distrust from adults around them and higher levels of anxiety.7–11
The causes and pathophysiology of CFS are still poorly understood and because of this, there are strong and differing views about the management of CFS.2,12 The delayed publication of the revision of the 2007 version of the CFS NICE guidelines demonstrated the disagreement among professionals and CFS patient groups. 12 The new NICE guidelines shorten the timescale for diagnosis, enabling access to care earlier and highlighting people with CFS may have experienced a journey of disbelief and stigma.2,12 NICE 2 recommend children and young people with CFS should be referred to a paediatric CFS specialist team to develop a personalised care and support plan, including a plan for energy management and support to engage in education, social activities and hobbies.
Evidence suggests there are low rates (5%–8.3%) of full recovery for adults with CFS.13,14 The long-term outcomes for CFS in adolescents appear more promising, with one study finding 58.9% of adolescents recovered from CFS at follow-up. 15 The mechanisms underpinning differences in recovery rates are not well understood. It is thought that part of these differences may be associated with biology, for example, a younger person's body may recover quicker. Moreover, children face fewer barriers to making changes regarding their activity levels compared to adults who may have work and childcare commitments. A final consideration is the level of neuroplasticity of the brain during childhood, with Weyandt et al. 16 reporting that experience-dependent interventions were associated with notable neuroplastic changes among children and adolescents.
Access to CFS services decreased in the UK during the Covid-19 pandemic. Social distancing guidelines reduced the capacity for outpatient face-to-face appointments. Services unable to overcome these barriers experienced unpredictable referral rates and long waiting lists, see Purrington and Beail. 17 Therefore, several CFS services opted to introduce remotely delivered videoconferencing therapy. An evaluation of a specialist paediatric CFS team working in this way was previously completed by Haig-Ferguson et al. 18 This evaluation reported that service users experienced videoconferencing therapy predominantly positively, noting benefits such as improving accessibility and a sense of being more open online; however, challenges and concerns were also reported, for example, feeling anxious on screen and privacy issues.
In the post-pandemic era, CFS services continue to utilise a mixture of face-to-face, telephone and videoconferencing appointments to complete clinical contacts. The Institute of Medicine outlines aims for quality health care, including providing care that is respectful of, and responsive to, individual patient preferences, needs and values, and ensuring that patient values guide all clinical decisions. 19 Therefore, to further improve clinical outcomes for patients with CFS, it is imperative to understand the lived experience of this cohort. Subsequently, this service evaluation aimed to explore the views of children, young people and their parents/carers regarding their experience of a CFS service delivered by a paediatric CFS team.
Finally, it is also of note that in a recent clinical review paper that charted a 25-year perspective of paediatric CFS, Loades et al. 20 highlight a knowledge gap that calls for further qualitative research on the lived experiences of CFS interventions. Therefore, it is hoped that this evaluation will inform practices in wider paediatric CFS teams by providing an up-to-date, current perspective of the lived experiences of these services.
Methods
The service
The service is specialist paediatric CFS service based in the North of England. The multidisciplinary team includes a Consultant Paediatrician, three Occupational Therapists and a Clinical Psychologist. The team sees service users aged up to 18 years with CFS. The service has a regional catchment and referrals come from either Paediatricians or GPs. Clinics run weekly and involve an initial assessment with a Consultant paediatrician and an Occupational Therapist or Clinical Psychologist. Each clinic appointment lasts 1 h 45 min.
The assessment covers the service user's history and current situation. Information is gathered on symptoms relating to the diagnostic criteria for CFS and the impact on daily life. 2 A biopsychosocial model is used as a framework to understand changes to well-being and lifestyle. A diagnostic decision is usually made at the initial assessment.
Those given a diagnosis of CFS are offered an online workshop to learn about pacing, a self-management strategy to balance activities with rest. A post-workshop review is offered six weeks later exploring intervention options and motivation for engagement. After the review, a service user waits around three months to start treatment. They are placed on a waiting list for Energy Management with an Occupational Therapist. The Energy Management intervention consists of six sessions, usually a month apart, via video or face-to-face, covering a range of topics including activity scheduling, sleep hygiene and school liaison. Changes to energy patterns and activity routines are measured using activity diaries and energy scales.
In some circumstances, service users are offered six sessions with the Clinical Psychologist, with the option for another six sessions. The frequency of these sessions is dependent on the young person's preference. Outcome measures for these sessions vary according to the model used and goals set. The service uses therapeutic models including Acceptance and Commitment Therapy, the DNA-V (Discoverer, Noticer, Advisor & Values) model, Solution Focused Therapy and Motivational Interviewing techniques.
Following this package of care, service users are offered open access to the service for around three months before being discharged from the service. The team has a clear discussion with the family at the beginning of treatment regarding the remit of the service, particularly that the service offers guidance and support in learning how to manage energy and setbacks and are not able to offer ongoing long-term support. The typical service engagement duration is nine months to one year.
Design
A mixed quantitative and qualitative design was selected for the study to be more comprehensive. The quantitative element allowed an exploration of outcomes important to the stakeholders in a systematic way and the qualitative element provided access to the voice of the service users and provided an opportunity for open feedback.
Participants
All children, young people and their parents/carers currently receiving treatment from the paediatric CFS team were eligible to participate. Overall, 102 service users and 102 associated parent/carers were invited to take part. The age of the invited service users ranged from 7 to 18 years old. All service users met the criteria for CFS. 2
Context
Data was collected between April and May 2021, around one year following the start of the Covid-19 pandemic. Due to social distancing guidance, the service increased the use of remote communication methods, including pre-recorded videos rather than face-to-face workshops and offering appointments via telephone or video more frequently. To capture the views and experiences of the cohort of service users and families who had experienced this new service provision, service users currently open to the team were invited to take part. This enabled the most up-to-date information to be collected in terms of the service being offered and, therefore, contribute to a current and relevant evaluation.
At the time of data collection, Covid-19 guidance from the government was regularly changing and England's third national lockdown had recently ended. As the lockdown restrictions eased, limits on socialising indoors and outdoors were gradually reduced, and there was a phased reopening of schools yet work-from-home guidance remained in place. The experiences and views of participants were likely influenced by this and should be understood within this context.
Materials
All data was collected by two postal surveys which were developed by the paediatric CFS team: one for service users and one for parents/carers (see supplementary material one). The quantitative data was collected via Likert scales and tick boxes in response to closed-ended questions or statements. Qualitative data was collected via free text boxes in response to open-ended questions. The surveys included questions about experiences, including appointments, interactions with staff, the impact on their life and any difficulties. The Warwick Patient Experiences Framework, which identified key themes that are important to a high-quality patient experience, guided the creation of the questionnaire and so questions focus on the availability of the service, tailoring the service to meet the patients’ needs and preferences, communication format and delivery, appropriate information and support. 21 The surveys were anonymous and did not request demographic or identifiable information. Participants were provided with a pre-paid envelope to return the survey. Paper-based postal surveys were chosen over an online survey because evidence suggests this data collection method results in a higher response rate.22,23
Procedure
Participants had provided consent to be contacted by the team regarding service user feedback. When invited to take part via a letter, participants were informed that participation was voluntary and not taking part would not affect their care in anyway. Participants were informed their responses would be anonymous. A total of 102 service users and 102 parents/carers were sent a postal survey. Participants were given four weeks to respond to the survey.
Data analysis
Descriptive statistics were calculated to summarise the data set, including frequency and mode. Thematic analysis was used to identify repeated patterns within the written data, guided by Braun and Clark.24–26 The first author typed the written data into NVivo, a software program used for the analysis of unstructured text. The first author then read and re-read the text to familiarise themselves with it before coding segments. The first author generated themes, which were then reviewed and refined. The first author kept notes of any reflections on her own biases and experiences and the impact they may have on the process.
Ethical approval
The project was commissioned by the Clinical Psychologist within the paediatric Chronic Fatigue Team and approved by the Research Support Officer at The University of Sheffield. The project was classified as a service evaluation and was written up retrospectively; therefore, it did not require formal ethical approval from a recognised ethics committee. However, the project was granted approval from the Audit and Effectiveness Officer in the Trust and registered with the Quality and Standards Database and Trust's Clinical Audit and Effectiveness Programme.
Results
Sample
Out of 102 service users and 102 parent/carers, 25 service users and 25 of their parents/carers responded. Data on demographic information was not collected due to the anonymity of the survey.
Overview of service users and parent/carer responses
A total of 88% of service users and parents/carers agreed with the collection of statements provided regarding the service meeting their needs and feeling supported by staff; 7% of the sample communicated disagreement with certain statements, including links with other services, ease of talking to staff, ease of contacting the service and suitable appointment type; 74% of service users and parents/carers selected that the team increased their activity levels; 87% of service users and parents/carers would recommend the service to friends and family.
Parents’/carers’ answers for statements
The frequency of answers chosen for each statement and mode is shown in Table 1. As a Likert scale with categorical data was used, the mean and median have not been calculated.
Frequency and mode of answers chosen for statements.
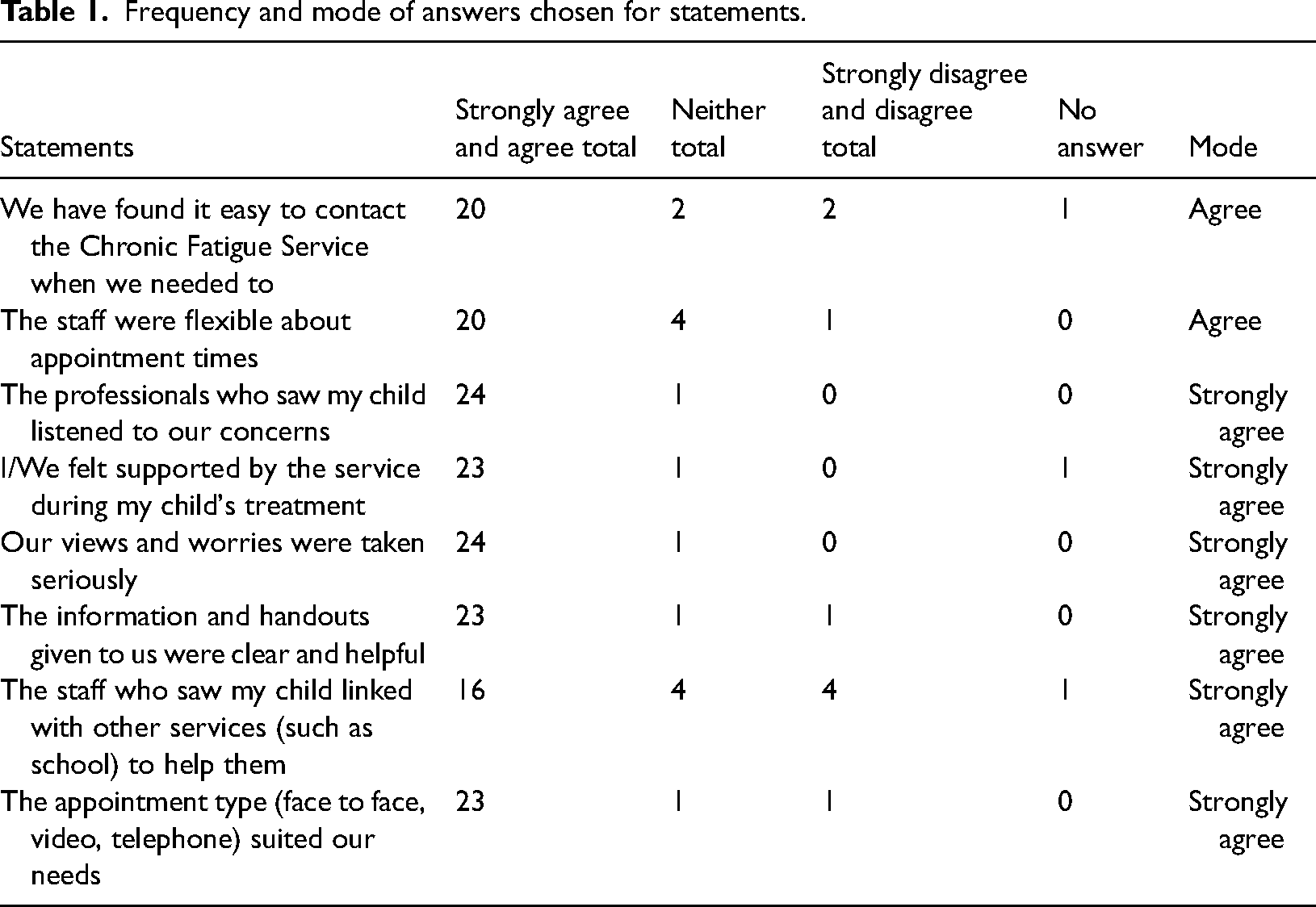
The results show that a large proportion of the answers for each statement was in the strongly agree and agree categories. Visual representations of the categories can be found in supplementary material two. One participant felt the question about linking with other services was not applicable because they lived out of area. Another participant said feeling supported during treatment and finding it easy to contact the service were not applicable. This may be because this service user was at the start of their journey with the team. Professionals listening to concerns, feeling supported and views taken seriously received the most strongly agree answers and did not receive any disagree answers, therefore, was a strength of the team.
Children's/young persons' answers for statements
The frequency of answers chosen for each statement and mode are shown in Table 2. As a Likert scale with categorical data was used, the mean and median have not been calculated.
Frequency and mode of answers chosen for statements experience.
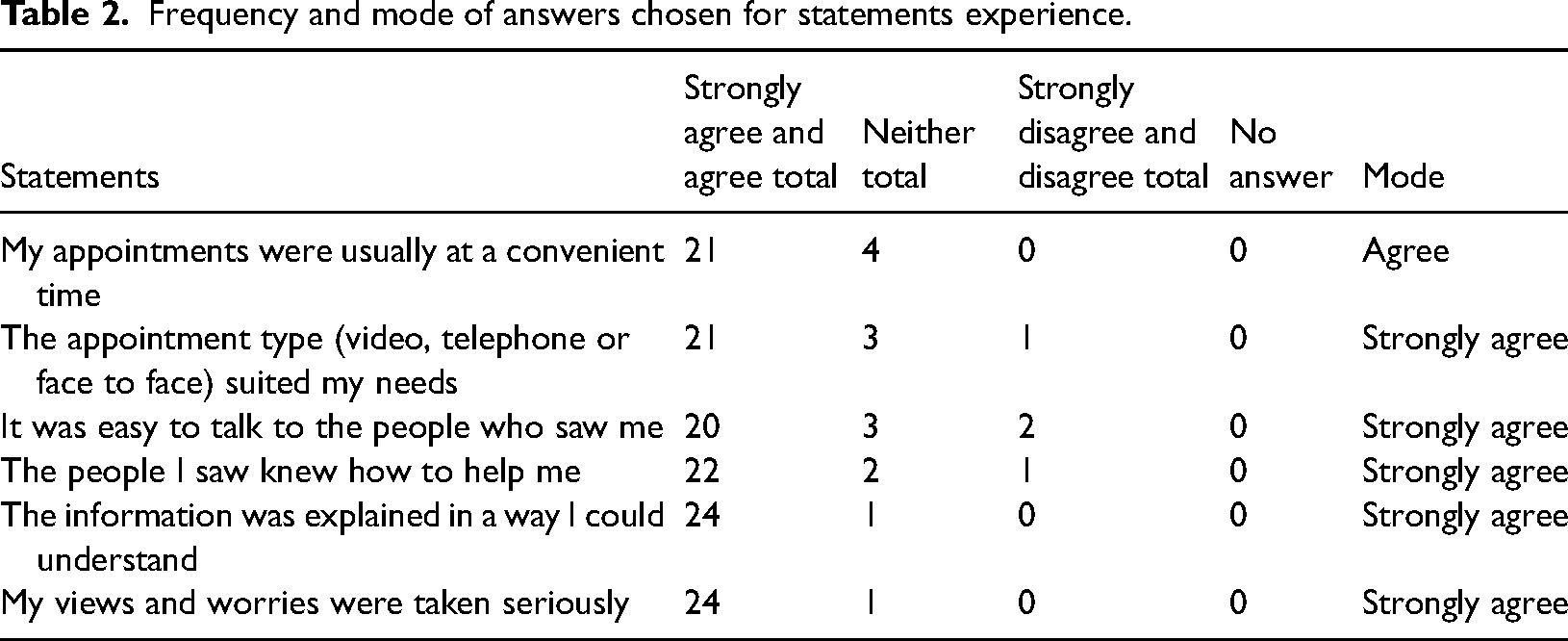
Similar to the results of the parents/carers, the results show that a large proportion of the answers for each statement was in the strongly agree and agree categories. Visual representations of the categories chosen can be found in supplementary material three. All statements were answered by all respondents.
Appointment methods
The responses regarding appointment methods show that most appointments were delivered solely over video. Overall, 7 out of 25 were delivered solely face-to-face. Some service users received a mixture of appointment methods and a small proportion received only telephone appointments. See Figures 1 and 2 for a visual presentation of the data.
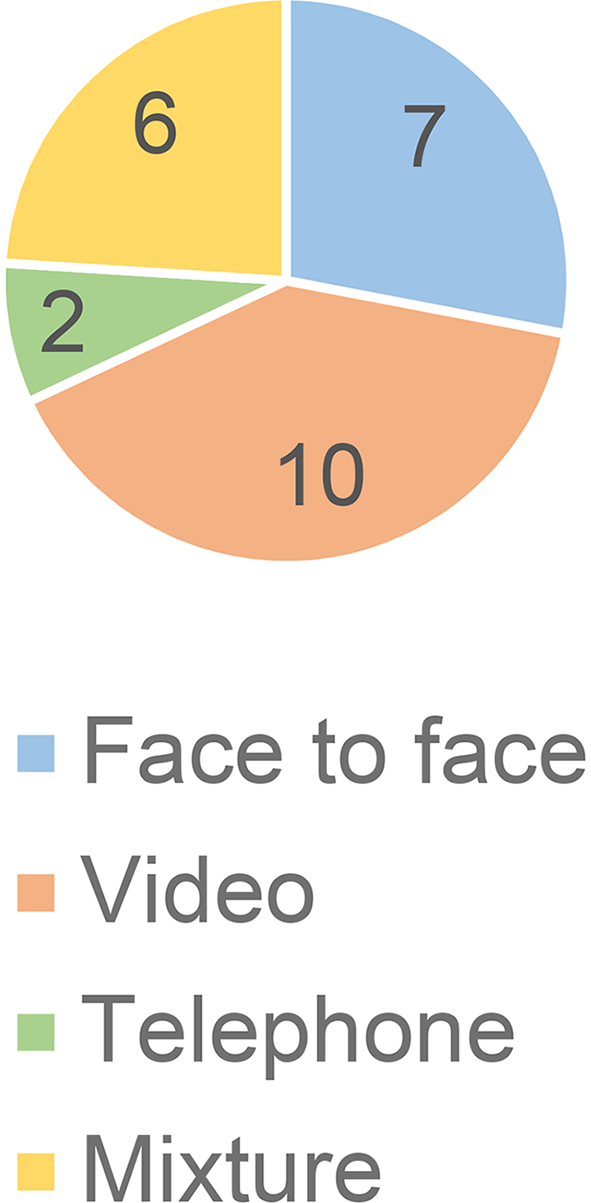
Most of my child's appointments were.
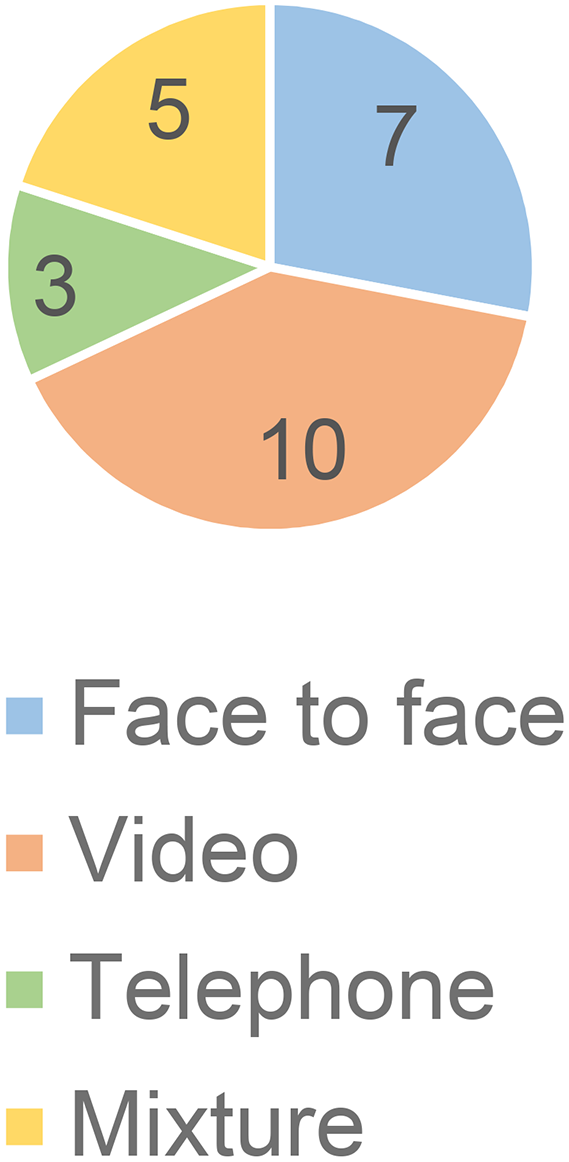
Children's/young person's appointment methods.
Outcomes of intervention
Results showed that a large proportion of both service users and their parents/carers felt support from the team enabled them to increase what they do each day. Five out of six statements received more votes from parents/carers than the service users. The greatest gap was between having more contact with friends and enabling teachers to support them. See Figure 3 for a visual presentation of the data.
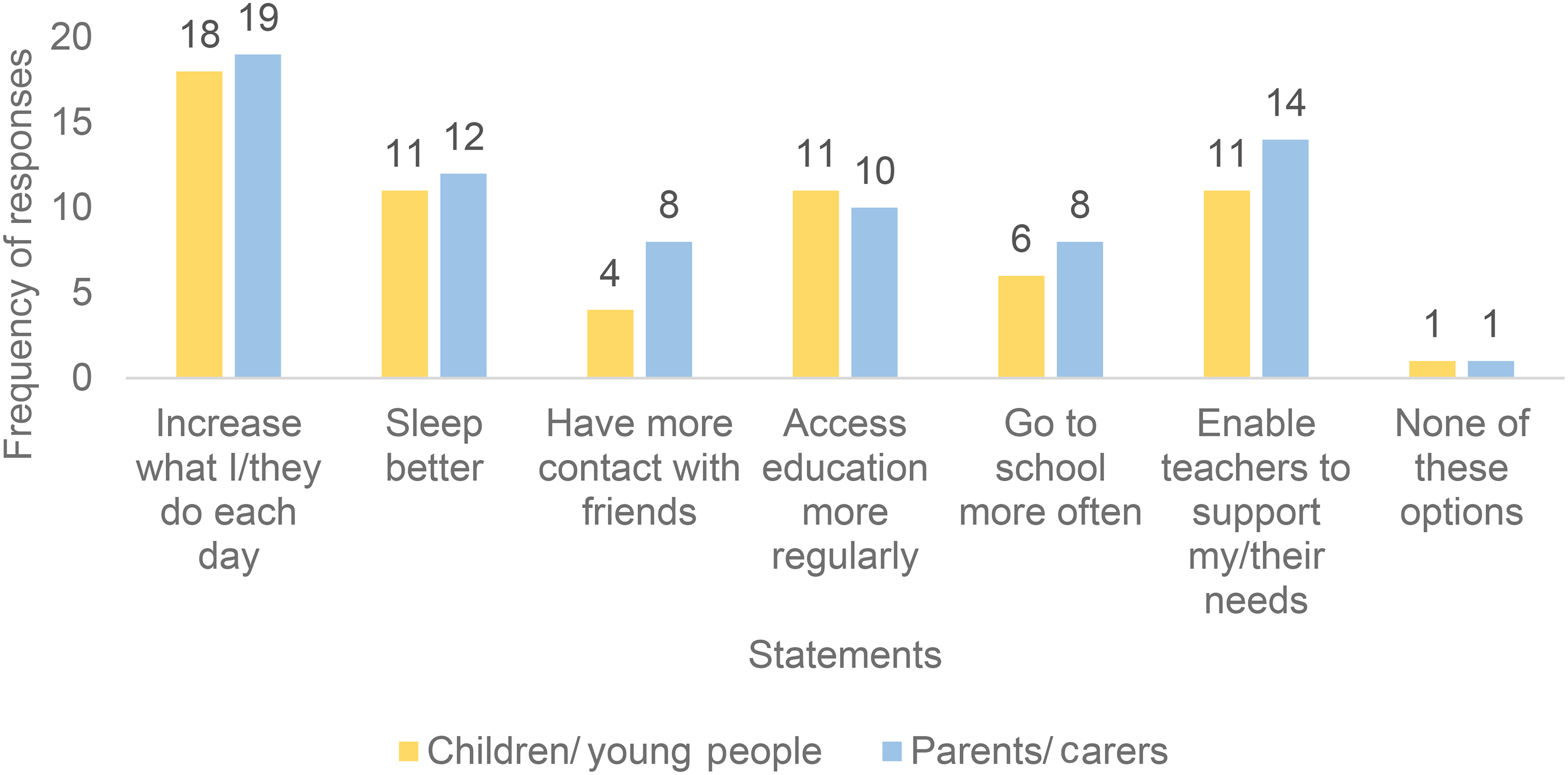
With the help we received my child was able to.
Likelihood of recommending service
Most service users and parents/carers would recommend the service to their friends and family. Parents/carers felt more strongly about this than the service users. Service users were less sure about this, with four selecting don’t know. One parent/carer and one service user of the same family would not recommend the service to others. See Figure 4 for a visual presentation of the data.
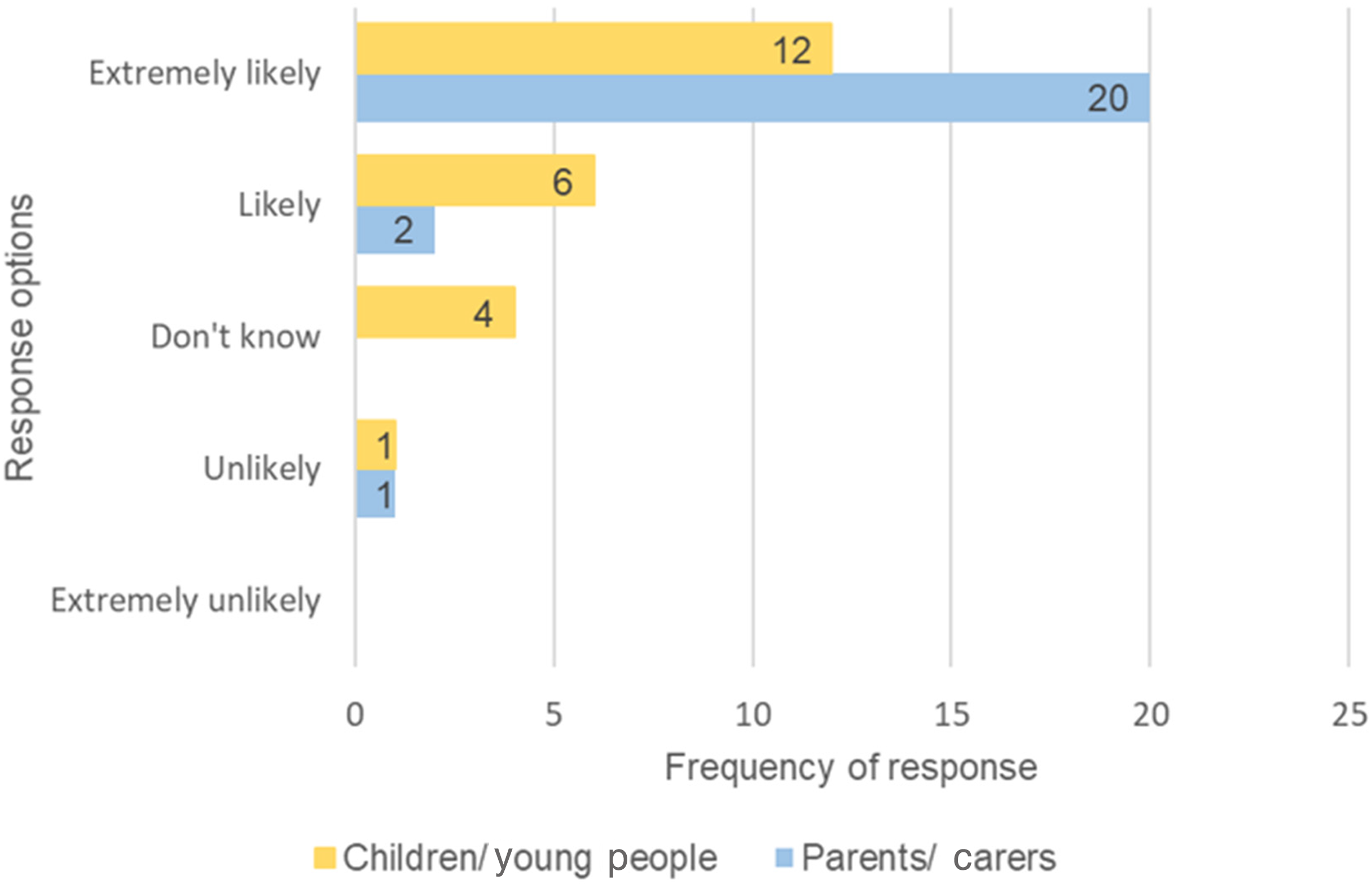
Likelihood of recommending the service to friends of family.
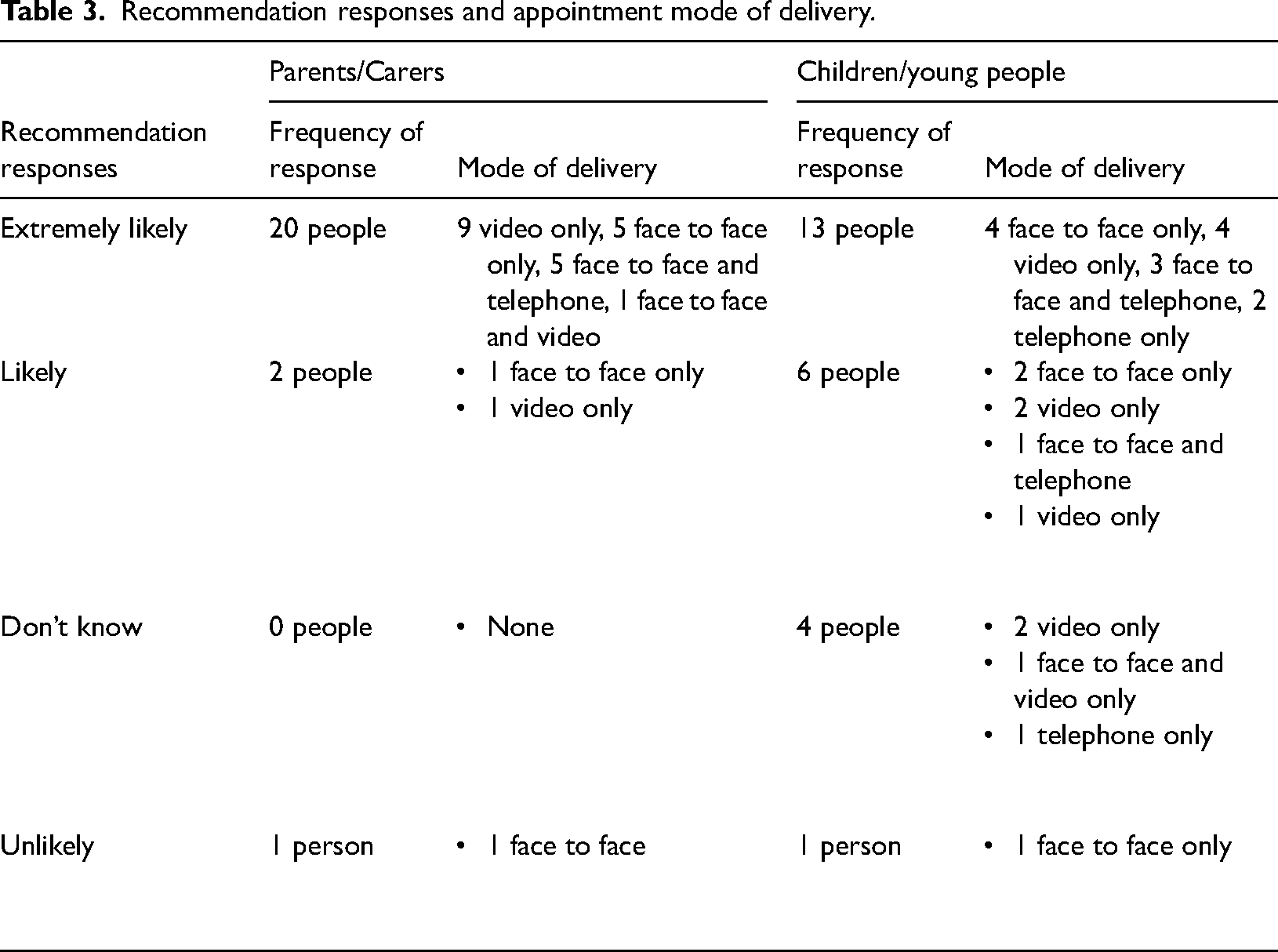
When breaking down the responses stating the likelihood of recommending the service into the appointment mode of delivery, there is a mixture of appointment types across the range of responses (see Table 3).
Recommendation responses and appointment mode of delivery.
Qualitative section
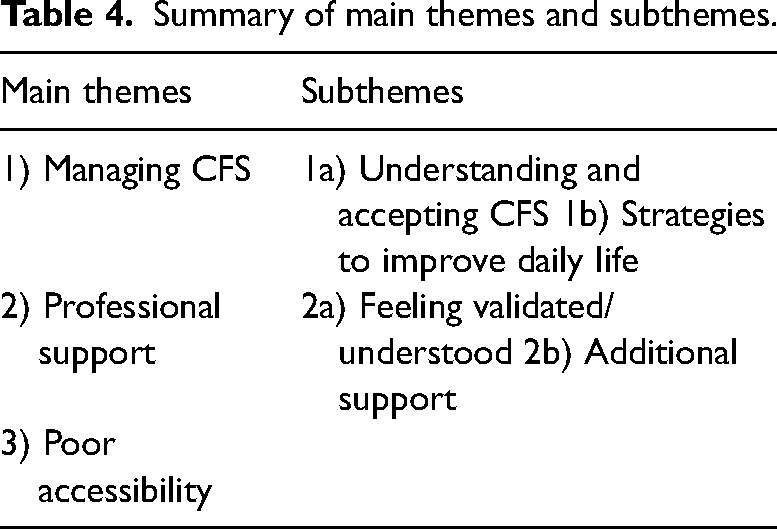
In total, 22 parents/carers and 19 children/young people responded to the free text questions about how the paediatric CFS team helped in other ways and 24 parents/carers answered the question about how the paediatric CFS team helped them as parents/carers. Overall, 20 adults answered the question asking about anything else they would like to say. Six children answered the question about what they disliked about their experience and three children answered the question asking about improvements that could be made. All answers were analysed together. A summary of themes and subthemes is displayed in Table 4.
Summary of main themes and subthemes.
Managing CFS
Understanding and accepting CFS
Many parents commented on how the service increased their understanding of CFS, for example, by providing education on CFS. It was noted the service appeared to help their children to have a better understanding of CFS and to help them accept their condition.
‘She definitely understands better what's happening to her.’ - Parent D
‘[The service] helped me to understand it's ok to have rest days.’ – Service User E
Parents/carers commented on how the service increased their understanding, enabling parents/carers to feel better informed, able to explain things better to school and better support their child. It was also commented on how the team increased others’ understanding, such as family members and school.
‘We understand the ‘ups and downs’ and can support her better.’ – Parent N
Strategies to improve daily life
A common theme identified was how the service helped to establish a routine, for example, by using a timetable. In addition, learning about pacing and the pacing workshop were recognised as helpful.
‘It made her think about listening to her body and reaction to energy use.’ – Parent V
Developing service users' abilities to identify symptoms prior to difficulties was noted as helpful. Improved quality of life, including helping to engage in conversations, improved health and balanced life, was attributed to being introduced to alternative methods.
‘[The service] has allowed me to become a more productive person.’ – Service User P
‘The tools to support improvements was life changing.’ – Parent R
Professional support
Feeling validated/understood
A theme was identified around the service users and parents/carers feeling more validated and believed from their contact with the team. It was reported that the team were friendly and supportive, and service users and parents/carers appreciated speaking to professionals who listened and put them at ease. However, one service user described finding it difficult to talk to the team.
‘Being believed by professionals helped both my son and I to feel validated and helped me feel less fearful of other services.’ – Parent W
Service users and parents/carers reported prior experiences of not being believed and it taking a long time to have symptoms acknowledged as a condition. One parent/carer reported their experience of professionals creating a sense of mistrust and feeling their observations were not accepted. It was noted that it would have been useful to have access to information about CFS earlier, rather than experiencing disbelief by professionals.
‘We are very grateful to be given the opportunity to have support from professional who understand CFS as things were beginning to affect our child's mental health as she was feeling she wasn't being taken seriously.’ – Parent C
Parent/carers talked about feeling relieved that their child was understood by the paediatric CFS team and relieved to know that other young people experience similar difficulties. One parent/carer and service user felt that the impact of CFS and their needs were not understood due to a disagreement about how many activities were recommended and not feeling able to meet these expectations.
‘I felt like the staff was not understanding what I was saying and that they were not understanding how exhausted I was feeling most days. The way they were talking to me was as if I wanted to feel better, I needed to try harder to do things which I found impossible to do.’ – Service User M
Additional support
Some parents/carers recognised how the team helped by linking in with other services, for example, helping to claim Disability Living Allowance and enabling longer exam times in education. One parent/carer and service user requested the team have more contact with school.
‘Talk more about how schools can help people suffering with CFS.’ – Service User Q
It was frequently noted that the team offered mental health support, including for low mood, anxiety, overthinking and feeling overwhelmed, related to CFS and Covid-19. The support provided was noted to lead to increased understanding of and improvements in psychological symptoms.
‘It has helped me stabilise my anxiety and break down my worries, to make them into a positive anxiety.’ – Service User N
Poor accessibility
Some grievances about the timing, frequency and length of appointments were reported. Service users reported appointments were too early in the morning or were tiring.
‘The phone calls were too long for me to concentrate.’ – Service User L
Service users requested more appointments to check progress and shorter sessions. Parents/carers suggested additional funding to increase the team size and resources and reduce waiting times. One parent/carer requested the team were more receptive to answering the phone. Another parent/carer commented that the service seemed aged for teenagers, and it would be useful to consider younger service users.
Some service users and parents/carers reported that the location of the team was too far from where they lived and out of the way. On one occasion, the journey was reported to have a negative effect on the service user.
‘As we don't live locally the journey had a very tiring effect on my daughter which cause her to have a relapse after each appointment lasting a minimum of a full week afterwards.’ – Parent M
Parent/carers suggested satellite or local clinics to make the team more accessible and convenient.
Discussion
This service evaluation aimed to explore the views of children, young people and their parents/carers regarding their experience of a paediatric CFS service. A total of 50 participants (25 parents/carers and 25 children) participated in the research. Responses to the survey highlighted that following engagement with the CFS service 37 respondents reported an increase in the child's daily activities, 25 reported that teachers were better able the meet the child's needs, 23 reported better sleep and 21 reported the child managed to access education more regularly. Additionally, 40 respondents reported being likely or extremely likely to recommend the CFS service to friends or family.
Additionally, service users were asked to respond to a series of statements that provide a context for the survey findings. The mode average response for parents/carers was ‘strongly agree’ in relation to the following statements: the professionals who saw my child listened to our concerns, I/we felt supported by the service during my child's treatment, our views and worries were taken seriously, the information and handouts given to us were clear and helpful, the staff who saw my child linked with other services to help and the appointment type suited our needs. Similarly, the mode average response for children attending the service was also ‘strongly agree’ to the following statements: the appointment type suited my needs, it was easy to talk to the people who saw me, the people I saw knew how to help me, the information was explained in a way I could understand, and my views and worries were taken seriously.
Additionally, 24 parents/carers and 19 children/young people responded to further open-ended questions with a thematic analysis revealing the following themes and subthemes: managing CFS (understanding and accepting CFS and strategies to improve daily life), professional support (feeling validated/understood and additional support) and poor accessibility.
Service users and parents/carers shared their experiences of not feeling listened to and mistrusting health care professionals in contrast to feeling believed, validated and understood by the paediatric CFS team. This was a clear strength of the team and shows the importance of taking time to build supportive, trusting and empathetic relationships. 2 However, two service users reported they did not find it easy to talk to staff. NICE 2 recognises that children and young people may need their parents/carers to help them communicate and it may take time to build trust.
Interestingly, parents/carers perceived the team made more changes to their child's life and communicated stronger feelings about recommending the service than the service users themselves. There is an absence of research evaluating the experience of parents/carers with children experiencing CFS; however, it is understood that parents/carers of children with additional health needs who require involvement in professional services often experience high levels of interpersonal stress, such as foster carers,27,28 carers of children who experience hospitalisation, 29 and parents of children with eczema, 30 epilepsy and asthma. 31 It is, therefore, meaningful for parents/carers to report high levels of retrospective perceived efficacy following their child's engagement with the CFS service, as this is likely to have a positive impact on the lives of the parent/carer and subsequently, the functioning within the child/parent dyad.
The importance of adaptive functioning within the child/parent dyad has been emphasised by recent developments in the fields of affective neuroscience and neurobiology. Concepts of ‘interpersonal neurobiology’ (see Refs.32–34), ‘intersubjectivity’ (see Refs.35–37), ‘social (co)regulation’ (see Refs.38–40) and ‘attunement’ (see Refs.41–43) outline the advantages of healthy patterns of relating within the child/parent dyad in developing a child's self and social identity. It is, therefore, not only important that parents/carers reported high levels of retrospective perceived efficacy of the paediatric CFS service but also that parents/carers reported feeling listened to, supported and taken seriously throughout engagement with the service. From these responses, it can be formulated that the paediatric CFS service contained, attuned and helped to co-regulate parents/carers which conceptually helps parents/carers to then contain, attune to and co-regulate their children, increasing the likelihood that therapeutic gains can be maintained.
Some service users requested more frequent and shorter sessions and found the distance to travel to the base problematic. This highlights the importance of adapting the timing, length and frequency of appointments to the person's needs, considering travel demands and providing care flexibly for each family, such as by online or phone consultations, as described in the NICE guidelines. 2
The statement regarding linking with other services had the most number of respondents disagreeing. NICE 2 recommend offering to liaise with education providers and support services. Linking with schools was reported as a benefit of the service in participant responses. It is important that paediatric CFS teams offer liaison to other services for all service users. In addition, psychological support to helpservice users manage their symptoms and reduce distress is recommended. 2 Support to manage anxiety was mentioned by eight service users as a helpful intervention and was an important aspect of the service offered.
Implications for practice
The service evaluation highlights a number of implications for paediatric CFS services:
Include children and young people in decisions about appointments, including appointment delivery format, timing, frequency, length and breaks. This will ensure the appointment meets their preferences and takes into consideration how fatigue may impact their ability to engage in sessions. Recognise that travelling to appointments can be very difficult, particularly for families who live far away. Continue to offer a range of appointment types, such as telephone and video appointments. Provide opportunities for liaison with schools for all service users as part of their care, for example, sending correspondence, attending meetings and offering training. Continue to listen to families and take their concerns seriously. Some young people may find it difficult to be open and build trust; therefore, extra attention should be paid to hearing the service user's voice and helping them feel comfortable to share their views. Monitor how well they are engaging, for example, through open discussions about their implementation of techniques and completion of between-session tasks. Regularly check with service users if the support is appropriate to their needs. Ensure clinicians have suitable administrative support to enhance the accessibility and effectiveness of the service. Continue to conduct service user feedback surveys to review the service. Future service evaluations may wish to consider a qualitative exploration of young peoples’ views to understand their thoughts about the service in more depth and make patient-driven improvements.
Strengths and limitations
Using a mixed-method format enabled a balance of depth and breadth of data. The response rate was reasonable considering the impact CFS has on this population. It is possible that for the younger generation online survey would have been more accessible, but the paper survey meant the sample was not limited to those with access to technology. Using a sample from one service in the North of England and capturing only the views of people who volunteered to complete the survey suggests the sample may not be representative of the population. The service users were at different stages of care and might have had different amounts of contact with the team, which may have affected the results of the evaluation. The demographics of respondents were not collected, such as age, gender and ethnicity, each of these would have helped provide context to the evaluation. As the surveys were anonymous, there is confidence that responses are truthful, although, response bias may still be present due to the results being returned to the CFS team.
A final discussion point is that the data was collected between April 2021 and May 2021. Contextually, this data collection period followed the second wave of Covid-19 in the UK in which Covid-19 cases had only just settled by April 2021. It is, therefore, highly likely that experiences of the Covid-19 pandemic impacted the experiences of the CFS service and subsequently the findings collated within the study, for example, considering the additional impact of Covid-19 on contact with friends, going to school and mood levels. It is possible that this may reduce the validity of the results and the level of transferability of findings for services currently operating in the post-pandemic era.
Conclusion
Children and young people with CFS present differently to adults and experience different impacts on their daily lives. NICE 2 recommend that children and young people with CFS should access support from a paediatric CFS specialist team. It is crucial for these services to capture the experiences of both service users and their families in order to review and improve their service provision, particularly with the changes brought in since Covid-19. This service evaluation project explored the experience of receiving care from the perspective of service users and their parents/carers in a paediatric Chronic Fatigue service. Overall, the service received extremely positive feedback and enabled lots of changes for the service users and their families. Families communicated benefiting from an increased understanding of the condition, learning new strategies, the team linking with schools, feeling validated and mental health support. The findings also highlighted several implications for paediatric CFS services, including considering the service users’ preferences for appointments, liaising with schools, enabling service users to share their views and conducting future service evaluations.
Supplemental Material
sj-docx-1-chi-10.1177_17423953231178185 - Supplemental material for Service users’ and parents/carers’ experiences of a paediatric chronic fatigue service: A service evaluation
Supplemental material, sj-docx-1-chi-10.1177_17423953231178185 for Service users’ and parents/carers’ experiences of a paediatric chronic fatigue service: A service evaluation by Gemma Hartley and Jack Purrington in Chronic Illness
Supplemental Material
sj-docx-2-chi-10.1177_17423953231178185 - Supplemental material for Service users’ and parents/carers’ experiences of a paediatric chronic fatigue service: A service evaluation
Supplemental material, sj-docx-2-chi-10.1177_17423953231178185 for Service users’ and parents/carers’ experiences of a paediatric chronic fatigue service: A service evaluation by Gemma Hartley and Jack Purrington in Chronic Illness
Supplemental Material
sj-docx-3-chi-10.1177_17423953231178185 - Supplemental material for Service users’ and parents/carers’ experiences of a paediatric chronic fatigue service: A service evaluation
Supplemental material, sj-docx-3-chi-10.1177_17423953231178185 for Service users’ and parents/carers’ experiences of a paediatric chronic fatigue service: A service evaluation by Gemma Hartley and Jack Purrington in Chronic Illness
Footnotes
Acknowledgments
This study was conducted as part of the first author's clinical psychology training programme at The University of Sheffield. The authors would like to thank tutors at The University of Sheffield for their mentorship and advice throughout this piece of research. The authors would also like to thank the service users and parents/carers who took their time to participate within this evaluation and the paediatric Chronic Fatigue team for supporting this project.
Contributorship
GH researched literature and conceived the study. GH completed data collection, analysis, and wrote the first draft of the manuscript. JP reviewed and edited the manuscript. All authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The service evaluation was commissioned by the Clinical Psychologist within the Paediatric Chronic Fatigue Team. The project was granted ethical approval from Audit and Effectiveness Officer in the Trust and registered with the Quality and Standards Database and Trust's Clinical Audit and Effectiveness Programme. All procedures contributing to this work complied with the BPS code of ethics and conduct and the HCPC standards of conduct performance and ethics.
Informed Consent
Consent was obtained to complete the therapeutic work with each service user. Consent was seen as an ongoing process which was reviewed regularly. Additionally, participants had provided consent to be contacted by the team regarding patient feedback. When invited to take part via a letter, participants were informed that participation was voluntary and not taking part would not affect their care in anyway. Participants were informed their responses would be anonymous. No identifiable details were saved on the computer or are included in the report. A total of 102 patients were sent a postal survey and their parents/ carers were sent a survey. Participants were given four weeks to respond to the survey.
Guarantor
GH
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.