
Abstract
Objective
This study aims to explore beliefs and perceptions about hypertension among patients living with hypertension in a local district in the Eastern region of Ghana.
Methods
A descriptive qualitative approach was adopted, and the Health Belief Model was used to guide the data collection, analysis, and organization of the study findings. Overall, seventeen participants were interviewed. In-depth interviews were conducted using a semistructured interview guide. Participants were conveniently selected from a district local Government Hospital. Data gathered were transcribed verbatim and analyzed using thematic analysis.
Results
Almost all the participants acknowledged hypertension as a severe but chronic illness that can cause sudden death. They also identified that lifestyle practices and individual attitudes were associated with the hypertension condition's causes, management, and control. The findings revealed several unscientific misconceptions and beliefs about hypertension, which could influence their disease management and control decisions.
Discussion
Patients’ decisions on alternative treatment for hypertension are primarily based on beliefs and misconceptions based on the information they receive from unregulated media and peers. The prevention and control of hypertension should focus on behavior and lifestyle modification which needs reinforcement through health education and promotion.
Background
Hypertension is the most common and preventable noncommunicable disease (NCD) affecting a large population worldwide. Hypertension has affected over 1.13 billion adults worldwide.1–3 The incidence of hypertension is known to occur in 13–41% globally, with middle- and low-income countries mainly affected. 2 A study conducted in selected countries in East and West Africa demonstrated hypertension affecting a quarter of the respondents aged 18 years and above. 4 Similar results emerged from a systematic review and meta-analysis by Bosu and Bosu, 5 indicating a hypertension prevalence of 27%. The study of Bosu and Bosu concluded that more than one in four adults have hypertension in most global populations, which is a serious public health concern.
Several studies have established that hypertension causes many diseases and deaths among the affected populace. For example, hypertension is known to be the leading cause of cardiovascular conditions such as heart failure, aortic valvular disease, left ventricular hypertrophy, atrial fibrillation, and abdominal aortic aneurysms.5–7 The increased risk of cardiovascular diseases has been linked to systolic blood pressure values between as low as 110
Compliance with prescribed treatment averts rapid mortality rates throughout medical practice and controls hypertension. Noncompliance with treatment has significantly affected suboptimal hypertension control in low- and middle-income countries. 11 A cross-sectional survey involving 12 countries in sub-Saharan Africa showed poor hypertensive medication compliance among patients diagnosed with hypertension. 12 Similarly, a study in Nigeria and Ghana demonstrated that noncompliance with treatments for hypertension stands at 66.7%. 13 Furthermore, some patients diagnosed with hypertension often hold strong cultural beliefs and engage in traditional practices that may influence their healthcare-seeking behaviors. 14 These cultural beliefs can impact patients’ decisions regarding treatment options, adherence to prescribed medications, and the use of traditional healers. 15 Patients in peri-urban communities may face limited access to healthcare facilities due to geographical factors and infrastructural challenges. 15 The absence of primary healthcare facilities near these communities often leads to reliance on informal healthcare providers or traditional healers. 16 Financial constraints and geographical distance to healthcare facilities also hinder patients from seeking preventive and curative services. 17
Based on the existing evidence, millions of individuals worldwide, especially in underdeveloped nations like Ghana, suffer from hypertension. Effective management and prevention of hypertension requires an awareness of patient perceptions and misconceptions about the condition in peri-urban populations. However, insufficient study in Ghana has made it challenging to design effective treatments and instructional materials. This study explores beliefs and perceptions about hypertension among patients living with hypertension in a local district in the Eastern region of Ghana.
Materials and method
Study design
This study adopted a descriptive qualitative approach which allows for a deep exploration and understanding of the phenomenon under investigation. Qualitative research is well-suited for revealing beliefs and misconceptions that may be challenging to measure through quantitative methods. 18 This approach enables researchers to understand the sociocultural and environmental factors influencing individuals’ beliefs and misconceptions about hypertension. 19 Researchers can gain a holistic understanding of the issue by capturing the context in which these beliefs and misconceptions emerge. Participants may hold views not documented or aligned with general medical knowledge, and through open-ended questioning, researchers can uncover these hidden or nuanced beliefs. This qualitative study, underpinned by the Health Belief Model, 20 provides in-depth insights into the beliefs, misconceptions, and factors impacting patients’ attitudes and actions toward hypertension management in a peri-urban community in Ghana.
Setting
The study was conducted in a local district government hospital in the Eastern Region, a peri-urban community in Ghana. Typically, patients in peri-urban communities in Ghana often have a wide range of socioeconomic backgrounds. Some may be engaged in agricultural or informal sector work, while others may have formal employment. Many patients in these communities face financial challenges and poverty, making it difficult to access adequate healthcare services.21,22 Also, patients’ education levels in peri-urban communities in Ghana vary significantly. While some individuals may have completed higher levels of education, others may have limited literacy and formal education. This variation in education can also affect patients’ comprehension of health information and their ability to navigate the healthcare system. 23
Patients in peri-urban communities in Ghana face a particular burden of communicable diseases such as malaria, cholera, and tuberculosis (Ghana Statistical Service, 2018). However, they also face increased NCDs, such as diabetes and hypertension, often associated with lifestyle changes and urbanization. 15 This setting was purposefully chosen because evidence revealed that hypertension emerged as the primary cause of death at the Eastern Regional Hospital in 2018, with an increase of nearly 70% from the previous year, 2017. 24
Population
The study population includes all patients aged 19 years and above who were medically diagnosed with hypertension and reported at the outpatient follow-up appointment clinic. Follow-up appointments for hypertensive cases are special clinics organized once a week for known cases which require regular assessments, review of medications, and counseling. These patients may have controlled or uncontrolled hypertension and reside within the neighboring environment of the district hospital. Seventeen participants who met the age inclusion criteria and were diagnosed a year or more ago were purposively selected at the follow-up clinic. With assistance from the clinic nurse in charge, all the recruited participants had been diagnosed with hypertension at the facility and received treatment for at least one year. Hypertensive patients with comorbidities or were only one-time visitors to the district and hospital were excluded from the study.
Data collection
The study used a convenient sampling approach to select participants from the hospital. Data collection occurred in 2020 and lasted two months in the last quarter of the year. The first author, responsible for the data collection, discussed with the participants time and place conducive for the interviews. Data collection was conducted mostly at the participants’ residences and the hospital premises using a semistructured interview guide developed based on the constructs of the Health Belief Model. 25 All participants signed a written consent form before the interview. Seventeen participants were interviewed for at least 50 min to one hour each. The interviews were digitally audio-recorded and transcribed. Data saturation was reached with the 15th participant, and additional two interviews were conducted to confirm and validate data saturation.
Data analysis
Data obtained from the interviews were managed and analyzed. A language expert transcribed and translated interviews in the local (“Twi”) language. The researchers read the transcripts severally to familiarize themselves with the data. The researcher used field notes to augment the data obtained in the interviews. We gave pseudonyms to all the transcripts to ensure anonymity. The transcribed data were coded manually through continuous line-by-line reading and assigning labels to words or phrases of transcribed data to identify codes. Codes with similar meanings and characteristics were grouped to form concepts. Five themes were identified based on the constructs of the health belief model. The first and last authors did the coding, which was reviewed and validated by the second and third authors. The researcher compared independent coders’ results to evaluate the initial codebook's reliability.
Trustworthiness
All the participants consented, and interviews were conducted in a favorable environment of the participants’ choice, which promoted relaxation and free expression. Each interview was immediately transcribed verbatim and coded. The interviews carried out in the local language were translated by a local language expert and reviewed by the researcher to ensure a true reflection of participants’ perceptions. There was a vivid explanation of the research design, data collection procedure, and analysis based on a qualitative approach. All research team members evaluated the interview guide to ensure it contained good questions that would solicit enough responses to answer research objectives. The audit trail of audios, field notes, transcripts, interview questions, consent forms, and all relevant information and documents were kept in a passworded folder to ensure confidentiality.
Ethical considerations
Ethical approval was sought from Ghana Health Service Ethical Review Committee with the approval number (GHS-ERC032/10/19) and management of the district hospital. Also, pseudonyms were used to ensure anonymity. Participants voluntarily consented to the study, and interviews were conducted privately. The data obtained is accessible only to members of the research team.
Results
Demographic profile of participants
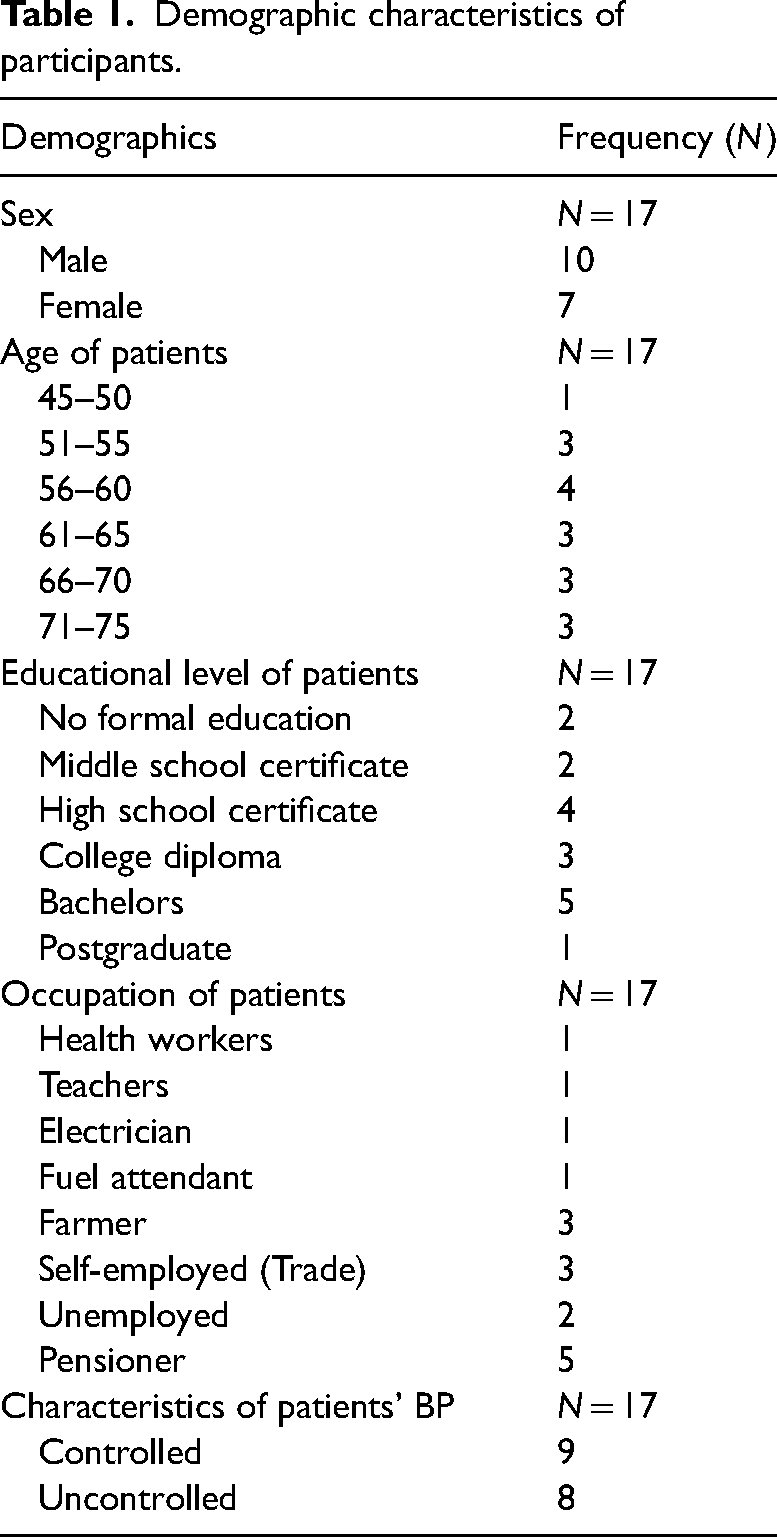
Table 1 presents the demographic characteristics participants in this study. All the participants were diagnosed with hypertension and received treatment at the facility. None of the participants had comorbidities. Averagely, the participants were diagnosed with hypertension seven years ago. Fifteen of participants were Christians, and only two were Muslims. Twelve of them were married, while five were divorced. The monthly income of the participants ranged between 100 and 2000 Ghana cedis (17.35–346.43 USD).
Demographic characteristics of participants.
Thematic findings
Perceived causes of hypertension
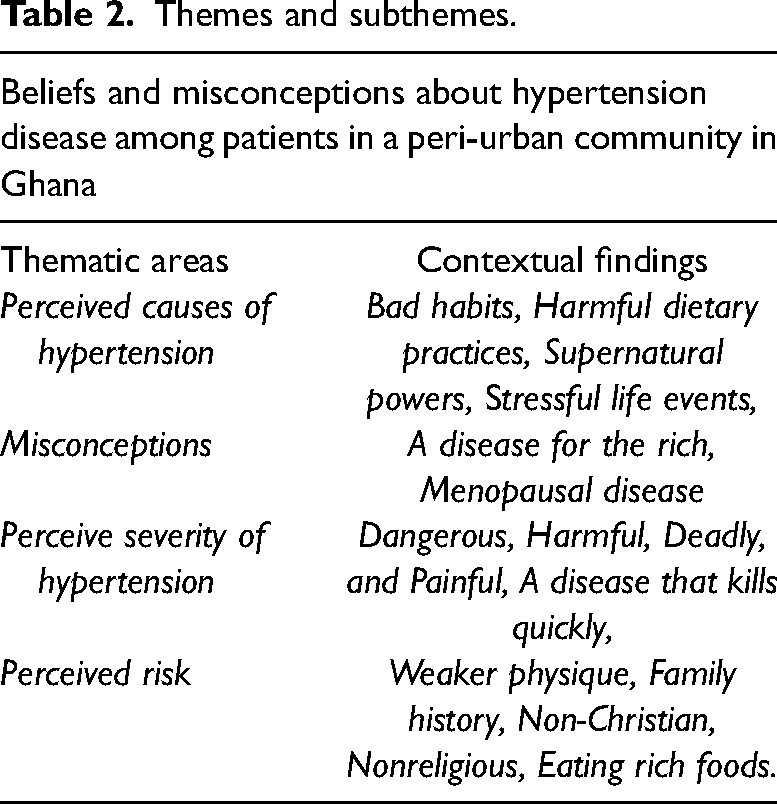
A summary of the thematic findings, grouped according to the constructs of the Health Belief Model, is presented in Table 2. Almost all the participants in this study believed that several factors, including bad habits, harmful dietary practices, and some supernatural powers, triggered their hypertension. They indicated that bad eating habits and poor diets caused hypertension. They speculated that one of the causes of their ailment was the result of their late eating.
I ate late most of the night, usually after 7 pm. I have been used to this for a long time; it has become part of me. I ate whatever I liked and ate whenever I felt like eating. Like when I went to bed early and woke up around 11 pm. I could soak gari [cassava flakes] and eat before I sleep again. I think this was the reason I had hypertension [P2]
Themes and subthemes.
Some of the participants were also of the view that eating certain foods can contribute to hypertension. Examples of such foods mentioned by the participants included fresh meat and foods containing excess oil, salt, and sugar. Others believed that excessive alcohol could also cause hypertension.
The intake of rich foods such as too much oil, fresh meat, cow meat, goat meat, fish, and others can cause this condition. I like koobi [salted fish] too. Anytime I ate ampesi [boiled yam], I ate it with koobi. I wish I had known this earlier because I have access to all these based on the job description as a kitchen staff. These foods lead to hypertension, and I have heard that those who take too much of these foods will usually get hypertension [P1].
In addition to the harmful dietary practices, participants mentioned stressful events such as losing a close relative to be associated with hypertension. Others believe that thinking, worrying, and frustrations can cause hypertension. A participant had this to say:
Too much stress, worrying, and thinking about things can cause hypertension. The pressure came when a Fulani man shot and killed my son, leaving his children with me. So if I am there and think small, the pressure will increase [P13].
On the other hand, participants mentioned factors they believe caused hypertension are not physical but spiritual. These factors included intuition, casting a spell, supernatural forces such as witches, and sexual activity with a woman while standing. A participant had this to say:
I think the cause of hypertension is beyond the physical. Witches can buy hypertension for people. For instance, I had issues with some of my co-workers who went to see a spiritualist and cast a spell on me. They wanted to kill me, so my blood pressure kept rising despite medical intervention. When they went to the spiritualist, they tied me up and sprinkled medicine (juju) at the workplace, and I stepped on it and became a victim. That is what I discovered when I did some consultations [P1].
Misconceptions
The researchers identified several misconceptions from the data regarding participants’ understanding of hypertension. Some participants expressed that hypertension affects wealthy people who can meet all their needs. According to some participants, the high cost of hypertension medications also suggests why it is a disease for the rich.
The last time I bought one drug from the hospital pharmacy, they said it would cost 45 cedis [8.0 USD]. I could not buy it because I had no money then [P6]. It is a disease of rich people, but I do not have that kind of money.
Few participants believed that hypertension meant having too much blood in the body. Their description of too much blood was high hemoglobin and adequate circulating blood volume. A typical participant's statement is captured below:
Hypertension is a disease of the blood. At first, I thought it had to be too much blood in the body, and because of that, I was careful not to take blood tonics to make my blood plenty [P4].
Other participants believed that certain diseases and physiological changes were the causes of their hypertension. These thoughts and misconceptions were feedback from friends and families as they shared their symptoms with them. At the beginning of my symptoms, I thought it was menopause. Some of my friends say menopause also can cause blood pressure. They say hypertension can lead to madness [P3].
Perceive threats of hypertension
Perceive threat of hypertension looks at participants’ perceived predisposition to hypertension. This section uncovered participants’ thoughts on the likelihood of developing hypertension and their views on its severity. Perceived threats also included participants’ perceptions of hypertension's medical and social effects. The medical and social impact was based on participants’ experience and what health professionals and nonhealth workers have informed them.
Perceived severity
Most participants reported that hypertension was a severe disease and used terms such as dangerous, harmful, deadly, and painful to describe the condition. These revealed participants’ views on the seriousness of hypertension. Some participants viewed the severity of hypertension from the complicated nature of its management.
Hypertension is very dangerous; the moment you stop taking your medicine, you are in trouble and feel strong heartbeats, and when you take it continuously, you feel weak. So, there is nothing good about this disease [P10].
Most of the participants described hypertension as a disease that quickly kills. Participants mentioned that hypertension could kill someone suddenly without exhibiting signs or symptoms. Some participants recounted situations where their friends or relatives had died unexpectedly, and it was later discovered that they died of hypertension. Meanwhile, none of them showed any severe signs or symptoms before their death.
I see hypertension as a severe disease because sometimes it is deadly and can quickly kill you if I check how it comes. I remember I spoke to a friend one evening, and I was told he had died the next day. This person was strong, and he even visited me at my house. That was why I asked the doctor whether to start sharing my properties when I was diagnosed with hypertension because I knew I would not live long [P13].
On the contrary, a few of the participants expressed the view that hypertension was a disease of a less severe nature. These participants likened hypertension to minor ailments, which they perceived would demand a short treatment period.
I did not know that hypertension was deadly. I thought it was similar to stomach aches and would not require a daily intake of drugs [P2]. I thought hypertension was a minor sickness, and within a short time, it would go away [P16].
Perceived risk
Perceived risk focuses on the participant's perception of the possibility of developing hypertension. From the study, all the participants stated not being susceptible to hypertension, and some expressed disbelief about the diagnosis. Participants cited reasons for their nonvulnerability, which included having average body size, being middle age, hardworking, looking strong, having low/middle socioeconomic status, absence of family history, being a health worker, being a Christian, eating less “rich” foods, and praying against diseases. No, no, not at all. I never thought I could develop hypertension, but I doubted it when I was told. I am a health personnel, an environmental health officer for that matter. But I was informed by the doctor; hence there is little you can do. I have to accept the diagnosis [P4].
I thought hypertension was for obese people and those who have money, and they spend it eating rich foods and fresh meat, but me a slim woman, and I do not know why I have developed hypertension [P11].
Some of the participants believed hypertension affects people who physically look weak. They, therefore, said that their physique and ability to perform activities of daily living do not predispose them to develop hypertension.
The way I look, my stature, how I was working, I was strong, and I went to the farm, and from childhood, I have been well, and I never visited the hospital for any illness. I could do anything, so I never thought I would have hypertension [P3].
However, almost all the participants identified some members of their family who had hypertension. Some participants believed a person could only get hypertension through his father's lineage. They stated that hypertension could not be transmitted through maternal blood only. My blood is different from my mother's blood, who had hypertension. We Ewes inherit our father's blood, and since my mother and I do not have the same father, our blood is different. So, I do not see why I should get hypertension [P6].
Discussion
This study identified beliefs regarding hypertension's causes, misperceptions, and severity in a local Ghanaian community. The scientific literature supports the view that poor dietary habits, such as poor diets and late-night meals, contribute to the etiology of hypertension. 26 In addition, eating certain foods and substances, such as excessive fats, a salty diet, and meat consumption, was listed as contributing to hypertension, supporting the findings of two other studies.27,28 In other studies, in the scientific literature, stress, excessive alcohol consumption, and anxiety were cited as causes of hypertension.29,30 This is consistent with the findings of Kongarasan and Shah 31 who found that over 90% of patients were aware of the causes of hypertension. However, participants expressed disbelief in their diagnosis, believing they could have avoided being diagnosed with hypertension. Beyond preventive measures, this study uncovered supernatural attributes regarding disease causes in the African context, similar to the findings from other studies.32,33 These explain inadequate and inaccurate knowledge concerning the causes of hypertension in Ghana.
The participants’ beliefs that hypertension is a disease of the affluent support the findings of Jones et al. 34 In addition, there were misconceptions and beliefs that hypertension meant having a high hemoglobin or blood volume, so taking blood tonics when prescribed was unnecessary. These findings are inconsistent with similar findings from other studies conducted in the Ghanaian context.22,35,36 The study also describes the participants’ perceptions of the health risks associated with hypertension. As reported by participants from countries such as Nigeria, rural Bangladesh, and the southeastern United States, hypertension is a “silent killer” that is harmful and hazardous.37,38 Hypertension, associated with a high mortality rate, confirms the World Health Organization's conclusion that hypertension is responsible for one out of every eight deaths worldwide. 3 Unfortunately, the contradictory findings equating hypertension with self-limiting minor ailments may contribute to noncompliance with the prescribed treatment.39,40 This suggests that participants who viewed their conditions as minor may be more likely to forego treatment or default on the treatment and control regimen.
The threat of hypertension was based on the fear of the likelihood of contracting the disease. Positive behaviors are influenced by an individual's perception of disease risk. However, the study results indicate that some participants believe they are immune to hypertension. Thus, the expressions of disbelief upon hypertension diagnosis. This finding contradicts the claims made 40 in a study that revealed participants’ high perceived susceptibility to hypertension.
Furthermore, the perception of invulnerability to hypertension makes it challenging to control and prevent hypertension-related complications. Other studies have determined that the higher an individual's susceptibility to hypertension, the more likely they are to engage in healthy behaviors that reduce the risk of disease development.41,42 Therefore, health professionals must carefully plan treatment regimens to include health education regarding hypertension's risk factors, management, and control.
Hypertension diminishes work output and productivity. There were references to the adverse effects of hypertension on social life and work in the study's findings. The finding that hypertension has negatively affected the social lives of affected individuals is consistent with the findings of other studies. 43 These impaired social lives directly impact their economic activity, resulting in low income. This invariably results in low life quality or poverty. Other studies have uncovered several other medical complications of hypertension, including transient ischemic attacks, impaired vision, stroke, palpitation aneurysm, and metabolic syndrome.3,44 In the Ghanaian context, several factors account for hypertension and its complications, including lack of blood pressure monitoring leading to undiagnosed patients, uncontrol blood pressure, self-medication, and treatment defaults.21,45 This reiterates the emphasis on health promotion and education on NCDs and management among populations in Ghana.
Study implications
The study has provided insight into the beliefs and misconceptions of patients diagnosed with hypertension in a local district in Ghana. Unfortunately, most of these beliefs were unscientific information that patients held for several years. Unsurprisingly, some of these participants and many others are living with undiagnosed, uncontrolled, and other complications of hypertension. These should influence health promotion, disease prevention strategies, and hypertension management. The participant's level of ignorance and misconceptions requires public education on hypertension and probably NCDs holistically. Patients must receive regular and comprehensive hypertension education from the hospital. This education will provide patients with accurate information about hypertension, dispel any erroneous beliefs they may hold, and reduce the rate of treatment noncompliance and complications.
Limitations
This study's small sample nature will not permit a concrete conclusion to be drawn from the findings; hence, the challenge to generalize the results. Nevertheless, the revelations of the misconceptions that patients have provided give the impetus for further investigations into hypertension. The authors believe there is a need for a quantitative probe of a causal relationship between beliefs and hypertension. Furthermore, as healthcare providers, most of the unscientific beliefs and misconceptions gathered about hypertension during data collection were worrying. There was a compelling urge to teach and disabuse the participants’ views about the negative beliefs; however, the research was not designed for health education. Future studies should use intervention and participatory approaches to teaching and educate participants who will have misconceptions and limited knowledge of the condition.
Conclusion
Hypertension is perceived as a dangerous disease that leads to sudden death and other severe conditions such as stroke. Results of the study have demonstrated that patients living with hypertension in the local communities may attempt to seek treatment from the hospital. However, these patients are also highly at risk of defaulting treatment and probably trying other treatment options such as herbal, over-the-counter drugs, and prayers based on their beliefs and misconceptions. Patients’ decisions on treatment and control of their conditions are influenced mainly by the information they believe, which is mostly unregulated and unscientific. The prevention and control of hypertension should focus on behavior and lifestyle modification which needs reinforcement through health promotion and education.
Supplemental Material
sj-docx-1-chi-10.1177_17423953231199525 - Supplemental material for Beliefs and misconceptions about hypertension disease: A qualitative study among patients in a peri-urban community in Ghana
Supplemental material, sj-docx-1-chi-10.1177_17423953231199525 for Beliefs and misconceptions about hypertension disease: A qualitative study among patients in a peri-urban community in Ghana by Jemima Otemah, Lillian Akorfa Ohene, Josephine Kyei and Irene Owusu-Darkwa in Chronic Illness
Footnotes
Acknowledgments
The authors acknowledged the contribution of study participants.
Availability of data and materials
The datasets generated and analyzed during the study are available from the corresponding author upon reasonable request.
Contributorship
The study was conceived by JO, LAO, and JMK. Data collection and analysis were done by JO under supervision and assistance of LAO and JMK. JO and IOD drafted the initial manuscript. LAO and JMK reviewed and edited the manuscript. All authors, JO, LAO, JMK, and IOD, took turns to read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethics approval was gained from the Ghana Health Service Ethical Review Committee with the approval number (GHS-ERC032/10/19) and management of the district hospital. Informed consent to participate in the study was obtained from all participants. All methods were carried out by relevant guidelines and regulations.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.