
Abstract
Objectives
Childhood obesity has become a global threat due to its serious negative consequences. We aimed to determine the patterns of metabolic syndrome and cardio-metabolic risk factors in Turkish children with obesity.
Methods
We examined 169 schoolchildren with obesity in April and May 2019 in Samsun, Turkey. After clinical evaluation and anthropometric measurements, fasting blood samples were collected to measure total cholesterol, low and high-density lipoprotein, fasting blood glucose, triglycerides, and insulin levels.
Results
The proportion of those who met the metabolic syndrome criteria in boys was 14.3%, but it was twice as high in girls (28.2%). The most prevalent component of cardio-metabolic risk factor was increased waist circumference (96.4%) followed by a high homeostasis model assessment insulin resistance index (74.6%) and high blood pressure (29.0%). While the average high-density lipoprotein was higher in boys than in girls, on the contrary, insulin, HbA1c, and homeostasis model assessment insulin resistance concentrations were higher in girls. The prevalence of dyslipidemia was also higher in girls (67.1%) than in boys (47.6%), as were all impaired metabolic syndrome components.
Conclusions
One in five children with obesity was at risk of metabolic syndrome. For early intervention and prevention, children with obesity should be monitored in terms of cardio-metabolic risk factors, but obese girls are more prioritized.
Introduction
Childhood obesity, driven by environmental, social, genetic, and biological factors, threatens children's health globally. 1 In the past three decades, the frequency of childhood obesity, which includes many cardio-metabolic risk factors, has almost tripled worldwide. 2 It has been observed that excessive weight gain increases by up to 40%, especially in children in developing countries. 3 Obesity can negatively affect all body systems and functions such as neurological, psychosocial, musculoskeletal, dental, respiratory, endocrine, and cardiovascular.4,5 Most children with obesity have a high risk of becoming obese adults with metabolic syndrome (MetS), which has led to a dramatic increase in the rates of prediabetes and diabetes worldwide. 6
Dyslipidemia is defined as a decrease in high-density lipoprotein (HDL) with an increase in triglyceride, low-density lipoprotein (LDL), and total cholesterol (TC). In cardiovascular diseases (CVD), the pathophysiological process caused by dyslipidemia occurs much earlier in children with obesity. 7 CVD risk factors caused by childhood obesity include high blood pressure (BP), impaired blood glucose level, central obesity, as well as dyslipidemia. All these risk factors are defined under the title of MetS. 8
MetS is a fatal endocrinopathy based on insulin resistance and causes systemic disorders such as obesity, type II diabetes mellitus, and hypertension. 9 Although numerous studies show relations between obesity and high BP, hyperinsulinemia, and dyslipidemia, there is little data on the prevalence of these cardio-metabolic risk factors in children's population-based samples, except in children who presented to the hospitals. Therefore, this study aimed to determine the pattern of MetS and cardio-metabolic risk factors in obese schoolchildren.
Methods
Study design
Participants of this cross-sectional study were selected from primary school children who participated in a previous obesity prevalence study in the province of Samsun which is situated in the northern region of Turkey. With a population of 1,269,989, Samsun ranks as the country's 15th largest city and is located on the Black Sea coast. The students who were found to be obese and studying in first and second grade (n = 403) in the year 2016 were invited to the current study in 2019 (Figure 1).
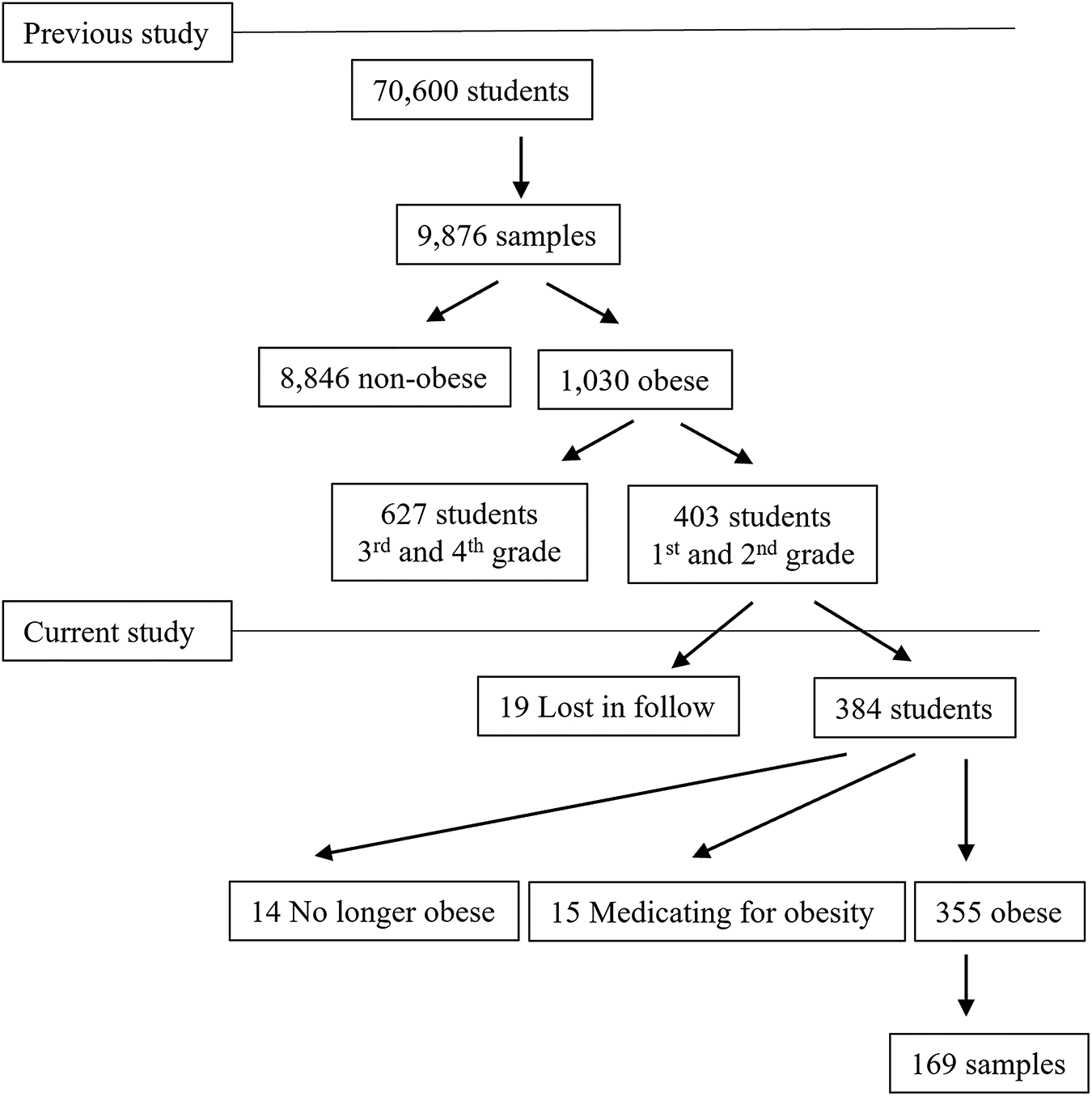
Flowchart of sample selection for the study group.
Study Population
We tried to reach the parents of 403 children by phone or e-mail based on information extracted from the records of the initial study between April and May 2019. Nineteen of these children were lost during the follow-up period. The anthropometric and clinical features of the children were re-evaluated and those who were non-obese anymore (n = 14), and who use medication due to obesity, or another metabolic disease (n = 15), were excluded from the study. Children whose body mass index (BMI) value is higher than two standard deviations by the WHO's BMI tables adjusted age and gender were considered obese and included in the study.
Sampling
The formula
The minimum sample size was calculated as 169, considering the number of the target children's population is 355, the p (MetS prevalence) value is 30%, the q value is 70%, the t-value is 1.96, and the sampling error margin is 5%. The participants were selected using a systematic sampling method.
Physical examination and biochemical analysis
Anthropometric measurements were conducted on the children dressed in lightweight clothing and wearing socks to accurately calculate BMI based on precise height and weight measurement. The student's height and weight were measured twice using a stadiometer with a sensitivity of ±0.1 cm (SECA Ltd, Medical Scales, and Measurement Systems, Birmingham, UK) and a calibrated scale with a sensitivity of ± 0.1 kg (Seca Mess und Wiegetechnik, Germany), and their averages were recorded. BMI was calculated using the formula of weight (kg)/height squared (m2). To compare BMI scores with age- and sex-specific references, a normalization conversion was performed, and BMI Z-scores were calculated. Waist circumference (WC) was measured at the end of a normal emporium by determining the length of a horizontal line parallel to the floor that passed through the midpoint between the uppermost lateral border of the ilium and the lower edge of the last palpable rib, using a plastic tape measure. WC measurements higher than the 90th percentile were considered indicative of central obesity. 10
BP measurements decrease with repetition, primarily due to familiarization. Systolic BP (SBP) tends to be 2–4 mmHg lower than the initial measurement, while diastolic BP (DBP) remains relatively stable. 11 Therefore, the BP was measured twice at five-minute intervals in a seated position, and the average value was recorded as mmHg. Total cholesterol (TC), low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglyceride (TG), fasting blood glucose (FBG), and fasting insulin levels were measured. The fasting blood samples were collected within a one-hour timeframe between 08:00 and 09:00 a.m. and analyzed using the COBAS 8000 c-702 (Roche) auto analyzer and colorimetric kits. The high-performance liquid chromatography method was employed to detect HbA1c, with values exceeding 6% considered high. The homeostasis model assessment insulin resistance (HOMA-IR) index was calculated using the formula: fasting glucose (mmol/L) × fasting insulin (IU/mL)/405. 6
Written informed consent was obtained from legally authorized representatives before the study. Ethical approval to report these cases was obtained from the Clinical Research Ethics Committee of Ondokuz Mayıs University (KAEK: 2018/1936).
Definitions
Dyslipidemia was defined as having any of the following values: TG ≥ 150 mg/dL, LDL thinsp;≥ 130 mg/dL, HDL < 40 mg/dL, and TC ≥ 200 mg/dL. Impaired fasting glucose (IFG) was considered for FBG > 100 mg/dL. Insulin resistance was calculated using the HOMA-IR index, with values higher than 3.54 defined as insulin resistance. 12 Hypertension was indicated by blood pressure > 130/85 mmHg. 13 According to the International Diabetes Federation (IDF) criteria for children aged 10 years or older. MetS was defined as the presence of central obesity (WC ≥ 90th percentile) and at least two or more of the following criteria: high SBP ≥ 130 or high DBP ≥ 85 mmHg, hypertriglyceridemia (TG ≥ 150 mg/dL), low HDL < 40 mg/dL, and elevated FBG ≥ 100 mg/dL. 14
Statistical analysis
Data analysis was performed using SPSS Version 22.0 (IBM Corporation, Armonk, NY, USA). The normality of data distribution was assessed using the Kolmogorov-Smirnov test. Quantitative data were presented as arithmetic mean ± standard deviation (SD), while qualitative data were expressed as numbers and percentages. Categorical variables were compared using the chi-square test. For the comparison of normally distributed continuous data, and the comparison of non-normally distributed continuous data, the Student's t-test and the Mann-Whitney U-test were used, respectively. A significance level of p < 0.05 (two-tailed) was applied to all tests.
Results
The study group comprised 169 children, of whom 84 (49.7%) were male, and 85 (50.3%) were female (Table 1). The mean age of the children with obesity was 10.2 ± 0.5 years.
Characteristics of the study group.
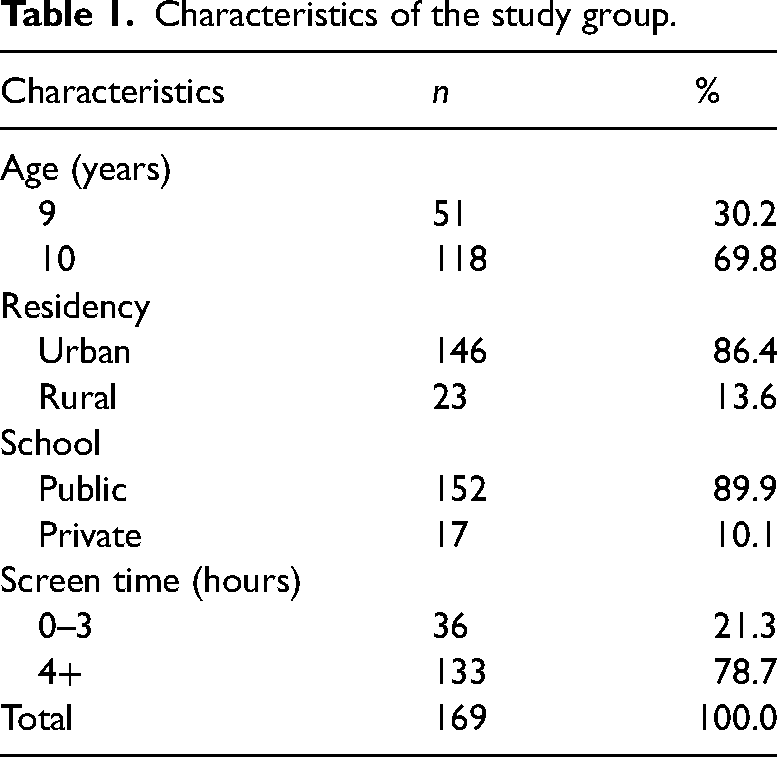
The parents of the study group consisted of 134 (79.3%) mothers and 35 (20.7%) fathers, with a mean age of 36.4 ± 5.6 years. The majority of the parents were homemakers, while 60 (35.5%) parents were employed. Six (3.6%) parents were illiterate, 69 (40.8%) had completed primary school, 27 (15.9%) had finished secondary school, 41 (24.3%) had graduated from high school, and 26 (15.4%) had completed university. The clinical and biochemical profiles of children with obesity are presented in Table 2. Insulin, HbA1c, and HOMA-IR levels were significantly higher in girls than in boys, while HDL levels were higher in boys than in girls.
The clinical and biochemical profiles of the obese children.
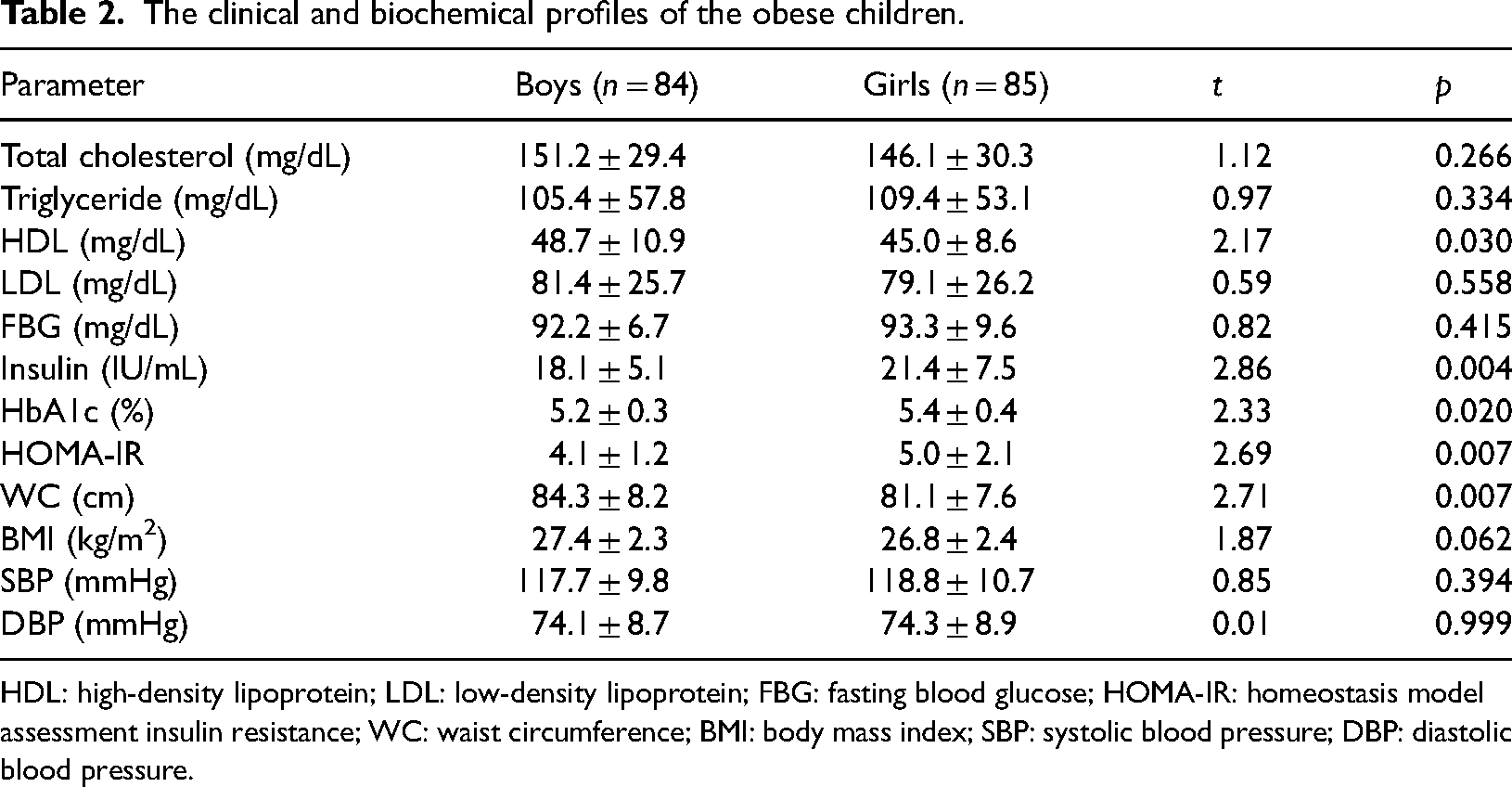
HDL: high-density lipoprotein; LDL: low-density lipoprotein; FBG: fasting blood glucose; HOMA-IR: homeostasis model assessment insulin resistance; WC: waist circumference; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure.
The prevalence of MetS was found to be 21.3%. While the prevalence did not significantly differ between children with obesity living in urban (21.9%) and rural areas (17.4%), a statistically significant difference was observed by gender (X2 = 4.90; p = 0.038). The prevalence of MetS was two times higher in girls (28.2%) than in boys (14.3%). The most prevalent component of MetS was increased WC (96.4%) followed by a high HOMA-IR index (74.6%) and high BP (29.0%). The prevalence of dysmetabolic factors in children with obesity is presented in Figure 2.
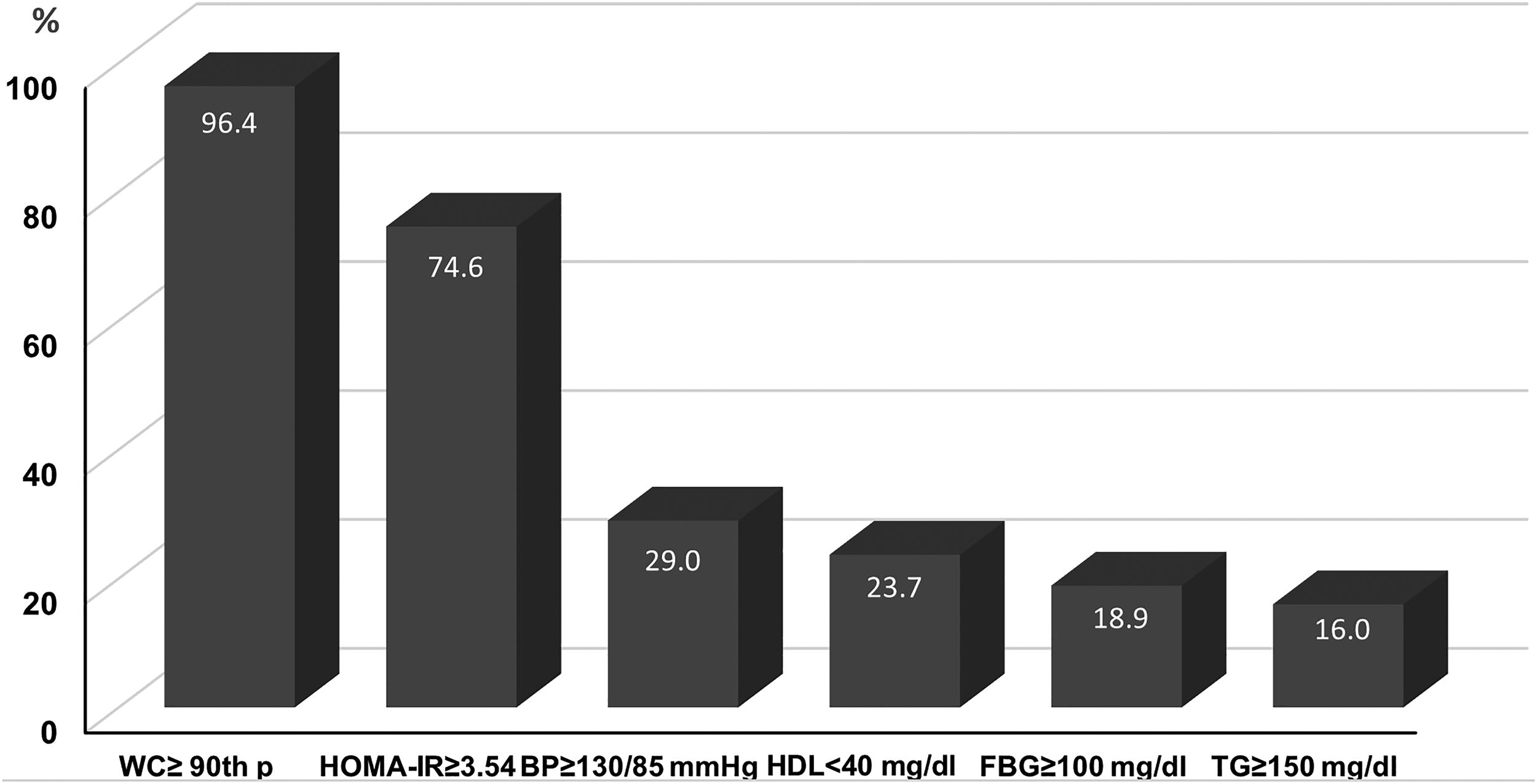
The prevalence of metabolic syndrome components in the study group.
The prevalence of all impaired MetS components was higher in girls than in males, especially low HDL and high FBG (Table 3). Similarly, the prevalence of dyslipidemia was found higher in girls (67.1%), than in boys (47.6%), significantly (p < 0.05).
The prevalence of MetS and impaired components by gender.
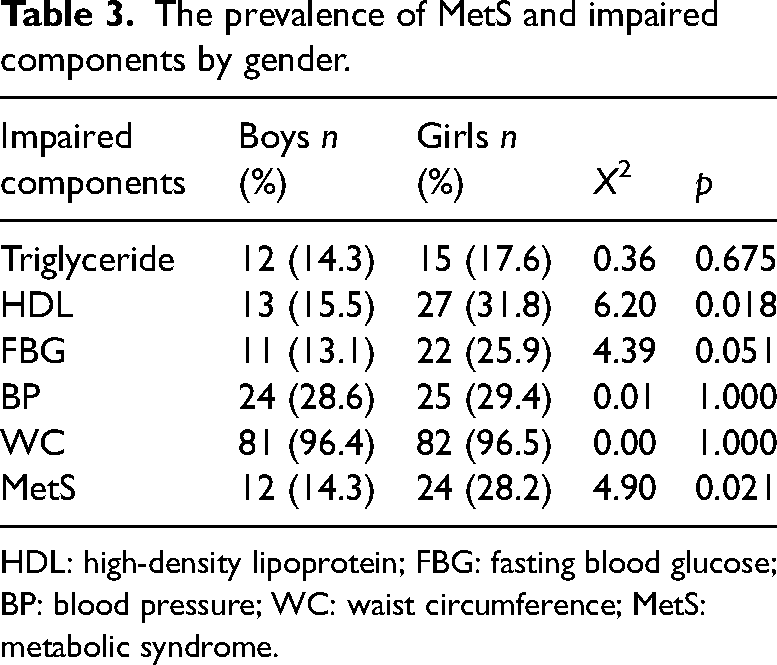
HDL: high-density lipoprotein; FBG: fasting blood glucose; BP: blood pressure; WC: waist circumference; MetS: metabolic syndrome.
When children with obesity were compared based on IDF criteria, it was found that BP and biochemical values were higher in children with MetS (Table 4). The mean values of the anthropometric measurements and BP were also elevated.
Distribution of clinical and biochemical parameters of the obese children by IDF criteria.
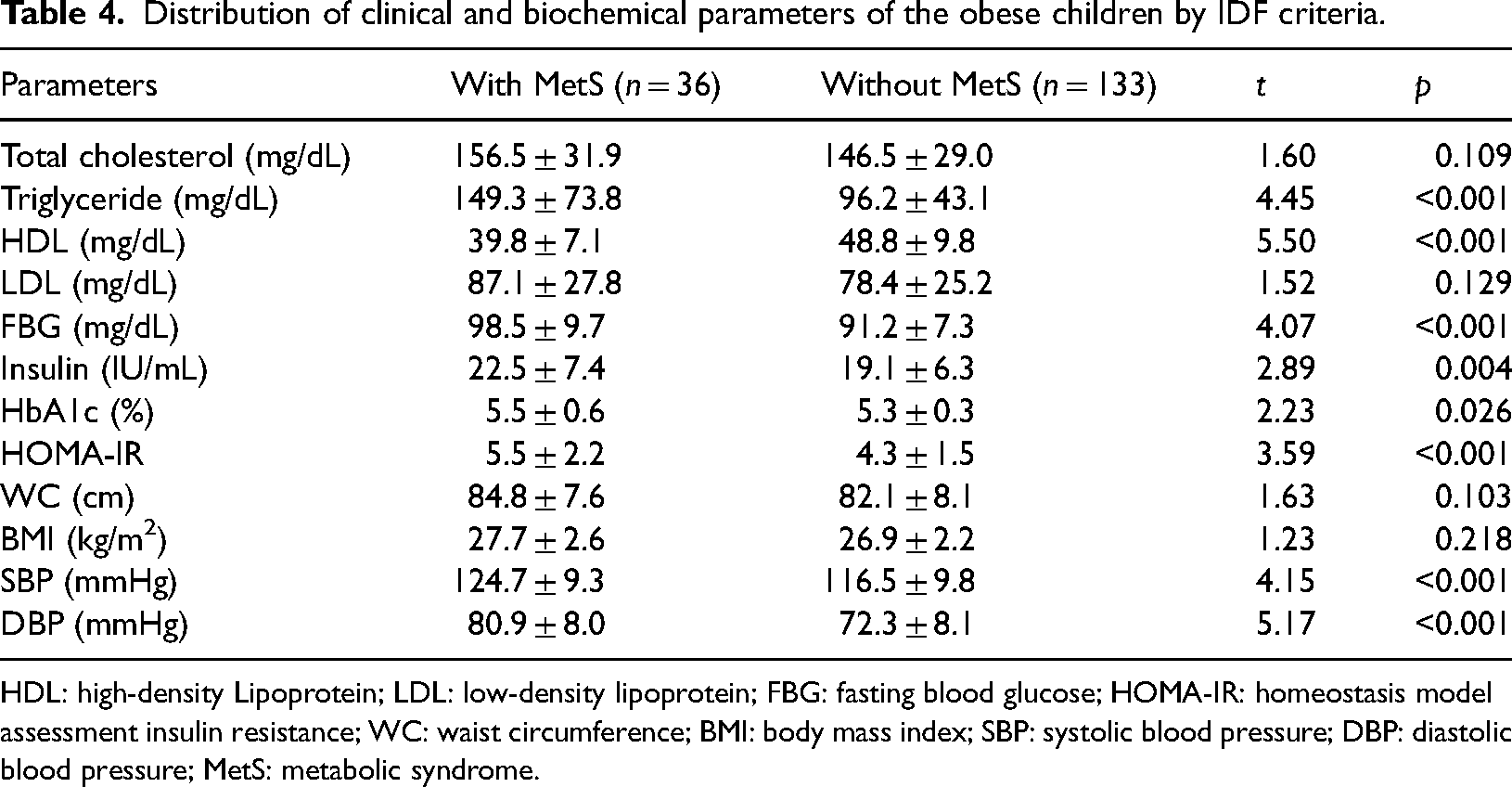
HDL: high-density Lipoprotein; LDL: low-density lipoprotein; FBG: fasting blood glucose; HOMA-IR: homeostasis model assessment insulin resistance; WC: waist circumference; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; MetS: metabolic syndrome.
Discussion
Obesity is a public health concern with severe implications for disease burden, including conditions like hypertension, diabetes, and cardiovascular disease, even in pediatric age groups. 15 Our results demonstrate that one in five children with obesity met at least three criteria for MetS. While waist circumference, BP, and triglyceride levels did not differ significantly by gender, the prevalence of low HDL and impaired blood glucose was higher in girls than in boys. Calcaterra et al. 16 found similar results in prepubertal children and suggested that the varying effects of gender on MetS components in the pediatric age group could be due to polygenic factors, diet, lifestyle, environmental factors, and sex hormones.
The prevalence of dyslipidemia in our study was 57.4%, which falls within the range of 31% to 76% reported in studies conducted on children with obesity in Turkey.17–19 This discrepancy may be attributed to variations in the upper limit criteria used to diagnose dyslipidemia. In children with obesity, adipose tissue inflammation elevates the levels of free fatty acids in circulation, leading to insulin resistance in other insulin-sensitive organs. This further underscores the link between adipose tissue and insulin resistance. 20 In our study group, the prevalence of insulin resistance among children with obesity was found 74.6%.
A recent systematic review of the pediatric literature highlights the diversity in methods and cut-off values used to determine insulin resistance in children and adolescents, resulting in a wide range of prevalence rates, spanning from 5% to 72%. 21 Studies conducted in Turkey indicate that insulin resistance in children with obesity varies between 35% and 45%.21,22 The identification of insulin resistance in three-quarters of children with obesity serves as a significant risk indicator. Insulin resistance plays a pivotal role in the development of dyslipidemia and hypertension, either directly or indirectly. Insulin plays a crucial role in clearing triglycerides from the blood and releasing free fatty acids from adipose tissue through the activation of lipoprotein lipase. 23 Hyperinsulinemia induces alterations in BP levels and vascular endothelial dysfunction through the nitric oxide pathway, impacting the sympathetic nervous system and its effect on renal sodium regulation. 24
The prevalence of hypertension, another CVD risk factor, was found 29.0%. Although the prevalence of hypertension in children with obesity varies widely, ranging from 4.3% to 57.0%, higher frequencies of hypertension are typically reported in studies involving hospitalized children.22,25,26 Both obesity and these conditions often persist into adulthood, further elevating the incidence and mortality rates related to heart disease. 27 Compared to their normal-weight counterparts, counterparts, children with obesity face a two to sevenfold increased likelihood of developing hypertension.28,29 Consequently, it is advisable to conduct additional screening for obesity-related risk factors, including plasma lipids and glucose, in children diagnosed with hypertension.
Despite varying definitions of MetS since 2003, numerous studies have reported an increase in its prevalence among children and adolescents, closely mirroring the rise in obesity within these age groups. 30 In the United States, the prevalence of MetS has either remained stable or slightly decreased in recent years, possibly due to heightened awareness of its health implications. 31 Prevalence rates of MetS in a representative sample of US adolescents have ranged from 2.0% to 9.8% across all teenagers and from 12.4% to 44.2% among obese teenagers. 32 In studies conducted on Turkish children with obesity, the prevalence of MetS has been reported in the range of 14 to 50%.33–35 Our province's prevalence of 21.3% aligns with these findings. Our relatively lower MetS prevalence can be attributed to the inclusion of children obtained through community-based research who have not yet exhibited clinical symptoms. Notably, the prevalence of metabolic disorders in girls was twice as high as in boys, despite a higher overall obesity prevalence among boys throughout our study. This raises questions about why concurrent disorders were less common in boys, despite their higher obesity rates. In addition to insulin resistance, it has been suggested that hormones synthesized by leptin and adiponectin may contribute to the development of MetS. 36 While high adiponectin plasma concentrations can reduce insulin resistance, leptin appears to play a promoting role in its development. 37
Ather et al. 38 reported elevated leptin levels in children with MetS, a positive correlation between leptin and overweight in adolescent girls, and positive correlations between high triglyceride levels and insulin resistance with leptin, along with negative correlations with adiponectin. The Brisighella Heart Study indicated that sex hormones are linked to alterations in the synthesis and secretion of adipokines, contributing to the development of MetS and similar chronic diseases. 39 This relationship is regulated by the presence of functional leptin receptors in reproductive tissues and steroid hormone receptors in adipocytes. In men, estrogen primarily originates from androgen metabolism within adipose tissue, leading to increased fasting plasma glucose, relative growth in fat accumulation, and insulin resistance. Additionally, adiponectin levels are lower in men compared to women, partly due to the negative correlation between testosterone and leptin. In men, a higher leptin/adiponectin ratio is associated with elevated blood pressure and triglyceride levels, as well as lower levels of HDL-C. Conversely, in women, it is linked to increased blood pressure and waist circumference. 39
A major strength of the present study is that it encompasses a representative population-based sample of Turkish children with obesity. Our study sample includes both urban and rural children, thereby enhancing the generalizability of the findings. However, there are some limitations to our study. Firstly, the study group was restricted to children aged 9 and 10 due to follow-up challenges. Secondly, despite reaching the minimum required sample size through an invasive method, our sample size remains relatively small. Consequently, caution should be exercised when interpreting results obtained from subgroup analyses. Lastly, it's important to note that, due to the nature of cross-sectional studies, causality cannot be definitively established.
Conclusion
Monitoring children with obesity, even when they are metabolically healthy, is essential for early detection of cardio-metabolic risk factors and prevention of their persistence into adulthood. It is crucial to initiate appropriate metabolic screening and assess associated comorbidities in children with obesity as early as possible. Therefore, documenting and understanding the relationship between childhood obesity and MetS in various populations hold tremendous significance in reducing CVD mortality. Community-based data serves as a valuable reference point for clinicians, including family physicians, pediatricians, and endocrinologists, who need to assess obesity-related risks. Additionally, this information is indispensable for public health professionals and policymakers as they calculate the burden of disease associated with childhood obesity and require baseline data to monitor the effects of new health policies.
Footnotes
Acknowledgements
Not applicable.
Contributorship
All authors contributed to the study's conception, design, data analysis, and interpretation of data. The first draft of the manuscript was written by CD. HNA and OT contributed to the development of the article, and all authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report these cases was obtained from the Clinical Research Ethics Committee of Ondokuz Mayıs University (KAEK: 2018/1936).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
CD
Informed consent
Written informed consent was obtained from legally authorized representatives before the study.
Trial registration
Not applicable.