
Abstract
Objectives
To assess the quality assurance of a specialist palliative care clinic focused on chronic diseases and explore the satisfaction and acceptability of the telemedicine model amongst patients and caregivers.
Methods
A cross-sectional 23-item survey was developed by the clinical team, approved by ethics and distributed to patients and caregivers. Data collection ran between September 2021 and February 2022, and SPSS was used for data analysis. Demographics were collected from hospital records.
Results
Thirty-five surveys were returned. The cohort had a median age of 82 years, and the most common primary diagnosis was renal failure. Participants rated telemedicine as easier to access than face-to-face appointments due to convenience. Telemedicine was rated highly for future utility, with video consultations being perceived as more useful than telephone consultations. Participants responded overwhelmingly well towards the clinic.
Discussion
Findings demonstrated high levels of satisfaction with the Supportive Care Clinic model and for telemedicine. However, logistical challenges and the desire for face-to-face appointments were also identified. The study highlights the importance of offering a range of modalities for patient engagement in healthcare services and suggests that telemedicine should complement, rather than replace, face-to-face consultations. Future investigations should explore patient and caregiver sentiment towards telemedicine platforms alongside patient deterioration.
Introduction
Palliative care (PC) needs amongst patients with end-stage chronic disease have become increasingly recognised. 1 Ischaemic heart disease has become the most prevalent cause of death worldwide with chronic lung disease being the third most common. 1 Outpatient PC services are critical to quality home-based care. 2
In response, the Supportive Care Clinic (SCC) was established at an Australian metropolitan health service to provide non-malignant chronic disease PC. The clinic targeted patients who scored positive on the Supportive and Palliative Care Indicators (SPICT) tool, 3 often after acute exacerbations. These patients were functionally well requiring occasional assistance, with a median Australia-modified Karnofsky Performance Status score of 60. 4 Patients were typically engaged six months before their death and more than three-quarters of patients remained engaged with the clinic at the time of death.
Due to extended COVID-19 pandemic restrictions affecting Melbourne throughout 2020 and 2021, the model of patient care was radically impacted. The pandemic expedited the utilisation of telemedicine by SCC. We define ‘telemedicine’ as the remote practice of medicine via telecommunications technology and further categorise this into telephone (audio-only) consultations and video consultations (video and audio).
Methods
A cross-sectional 23-item survey, developed by the clinical team and piloted with clinicians and patient representatives, explored satisfaction and acceptability of the telemedicine clinic model. The survey used a mix of open-ended responses and Likert scales where participants indicated their level of agreement to statements to elucidate satisfaction. Ethical approval was granted (details omitted for double anonymized peer review). SCC patients and caregivers were eligible to participate if they had attended at least two SCC appointments and were able to complete the survey in English. Data collection ran between September 2021 and February 2022. Demographics were collected from hospital records (Figure 1).
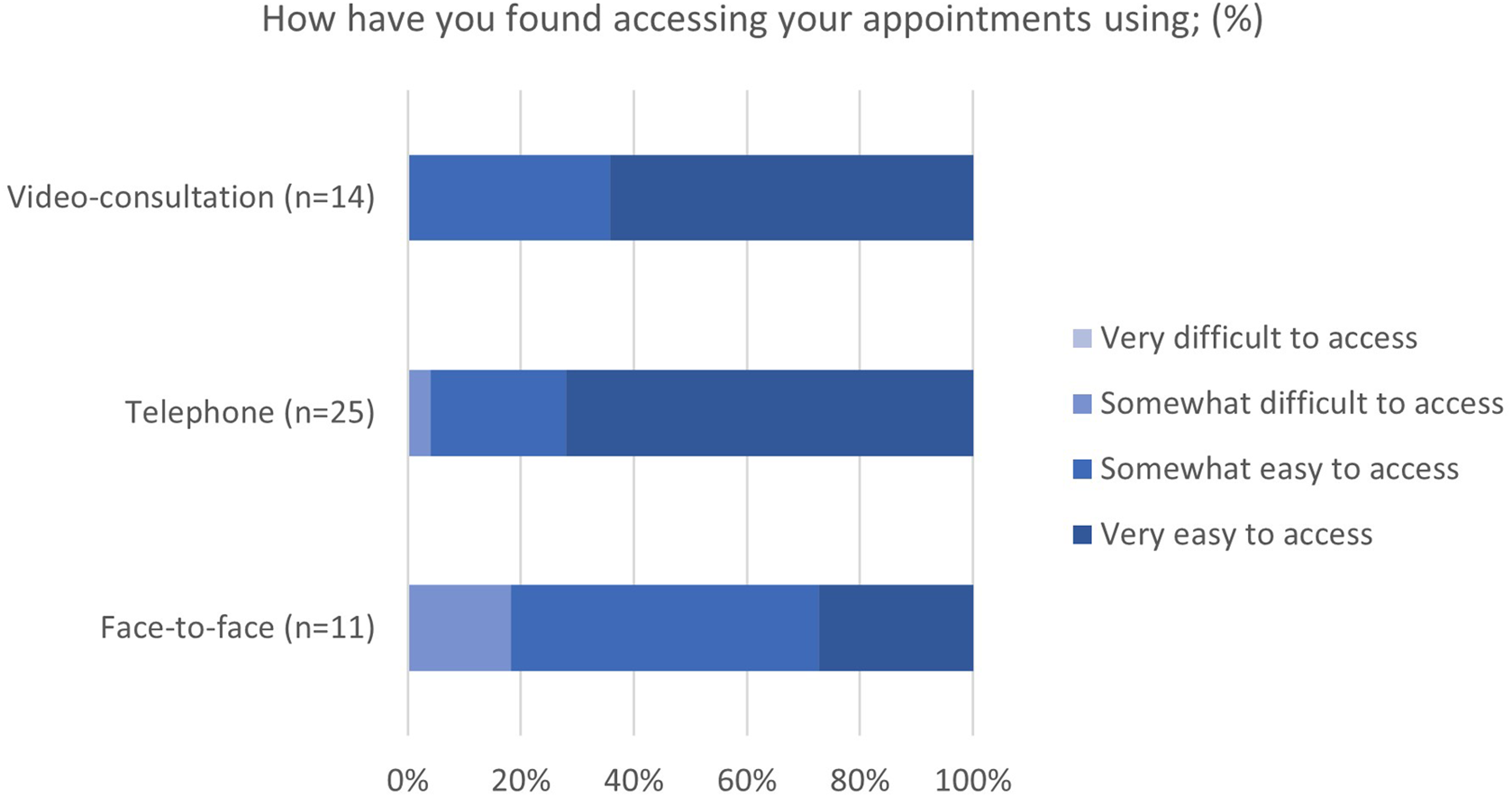
Respondent opinion on the ease of access.
Results
Of 95 patients, 49 were identified as eligible to participate. Reasons for ineligibility included being non-English speaking (n = 13; 30.95%) or attendance of less than two appointments (n = 10; 23.81%). Patients and their caregivers were invited to participate with consent. From 82 distributed surveys (49 patients and 33 caregivers), 35 surveys were returned (21 patients and 14 caregivers).
The eligible cohort had a median age of 82 years (range 39 to 94 years), 49.05% were male and 90.47% were living in a private residence. All patients had non-malignant disease, most commonly renal failure (41.51%). The SPICT 3 was used to gauge care needs. We defined a patient as having ‘care needs’ if they met at least one general indicator and at least one clinical indicator of poor health. The mean SPICT score of this cohort approximated 6, indicating, considerable care needs.
Of attended appointments, 20.34% were in-person, 22.74% by video consultations and 55.12% were via telephone.
Participants were asked to rate their attended appointment modalities according to ease of access on a 5-point Likert Scale. Participants rated both video consultation and telephone as easier to access than face-to-face appointments. Video consultation was rated ‘just as good as face-to-face’ or ‘better than face-to-face’ by 87.50% (n = 8) of participants that had utilised both appointment modalities. Additionally, there was greater satisfaction for telephone appointments when compared with face-to-face appointments (n = 15; 66.67%). Participants also responded overwhelmingly well (almost 100% positive) towards the clinic, both in addressing their needs and to the utility of the clinic in complementing other healthcare services.
Telemedicine was rated highly on a continuous variable scale when it came to future utility. On this scale, very useful was defined as ‘70 and above’ on a scale of 0 to 100. No participant felt that telemedicine was not useful. When comparing the two telemedicine modalities, participants indicated that video consultation had greater utility than telephone consultations, with a greater proportion indicating video consultation as very useful (65%) compared to telephone (40%).
Open-text comments revealed suggestions for improvement, including expanded clinic locations for those patients desiring face-to-face care and implementing reminders for telemedicine appointments.
Discussion
Our findings demonstrate high levels of satisfaction for the SCC model and for telemedicine. This is likely because telemedicine offers the convenience of being at home while still receiving care, particularly during the restricted movement of people during the COVID-19 pandemic. 5
The greater proportion of attended appointments via telephone can possibly be attributed to patients’ limited technological knowledge or access to connect successfully to video-conference platforms. These logistical challenges cannot be disregarded; in future service planning, it will remain important to offer patients a suite of available modalities through which they can engage with healthcare. In the open-text comments, the desire for face-to-face appointments by some patients exemplifies the importance of offering this care modality, rather than a remote model of care only. Our findings suggest that a hybrid model that offers telemedicine in addition to physical appointments, would meet most patients’ preferences.
This study has some limitations. Firstly, it is a cross-sectional assessment of patients known to the SCC clinic, potentially leading to positive feedback bias. Secondly, it is a small study that was not able to include patients of non-English backgrounds or cognitively challenged patients and hence lacks the power to be representative more generally. Lastly, despite the response rate being consistent with survey response rates in the literature, 6 there was an unavoidable non-response bias present, as 58% of patients and caregivers did not respond.
Outside of this project's scope, future studies are needed to explore patient and caregiver sentiment towards telemedicine platforms alongside patient deterioration. We postulate that telemedicine will become increasingly important and favourable as patients deteriorate and become less mobile – a phase that, pre-telemedicine, may have seen a patient disengage with outpatient clinic services. Telemedicine allows for the reach of outpatient specialist care through to the terminal phase without a patient needing to be physically present at a clinic. More research will be required to develop guidelines for triaging patients for telemedicine versus a face-to-face consultation.
Conclusion
This study has demonstrated patient satisfaction with a chronic disease-only PC clinic and a video consultation model of care for PC consultation in the outpatient setting. The findings will assist future health service planning for chronic diseases.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.