
Abstract
Objectives
To examine the impact of social and emotional support on serious psychological distress (SPD) in individuals with type 2 diabetes (T2DM) and functional disabilities after controlling for socio-demographic factors and health status. Findings provide information for healthcare providers to enhance patients’ psychological well-being.
Methods
Data from 529 adults were obtained from the 2021 National Health Interview Survey, including those who had T2DM and also reported significant difficulty or inability to perform an activity in any of the following domains: seeing, hearing, walking or climbing stairs, communicating, remembering or concentrating, or practicing self-care. Descriptive analysis and a hierarchical regression model of SPD were used.
Results
The mean age of participants was 67.88 years old, and the mean duration of diabetes diagnosis was 16.88 years. Notably, 12.5% of individuals reported SPD. A decreased likelihood of reporting SPD occurrence was associated with older age (odds ratio (OR) = 0.95), a longer duration of T2DM diagnosis (OR = 0.97), having at least a high school education (OR = 0.54), and receiving social and emotional support.
Discussion
Social and emotional support likely mitigates psychological distress, suggesting that social and emotional support resources should be enhanced, especially among individuals who are younger and those more recently diagnosed with T2DM.
Introduction
More than 61 million (26%) of adults aged 18 years old and over in the United States experience disabilities. 1 The Centers for Disease Control and Prevention (CDC) defines disability and functioning by evaluating the difficulty level in six domains of functioning, including seeing, hearing, mobility, communication, cognition, and self-care. 2 Another chronic health issue escalating in the US is diabetes. This prevalence has rapidly increased, with the estimates of individuals diagnosed with diabetes nearly doubling from 18.8 million to 37.3 million between 2010 and 2020.3,4 Most diagnoses are for type 2 diabetes (T2DM), making up 90–95% of those diagnosed. 4
Diabetes increases the risk of comorbidities, including cardiovascular disease, obesity, stroke, visual impairment, arthritis, and kidney disease. 5 Consequently, people with diabetes are at greater risk for mobility disabilities, difficulty with activities of daily living (ADL), and difficulty with instrumental activities of daily living (IADL).6,7 In the United States, 16.3% of people with disabilities have diabetes, compared with 7.2% of people without disabilities. 1 Gregg and Menke 8 reported that about 25% of adults with diabetes reported a work disability, and one-tenth reported an IADL disability. The association between diabetes and disability is bidirectional. Among people with disabilities, increased sedentary behavior, muscle disuse, and altered lean-to-fat ratios enhanced the risk of developing T2DM. 8
Serious psychological distress (SPD) scale is a global measure designed for use in population studies. Although SPD is a non-specific psychological distress without a DSM-IV diagnosis, it refers to high levels of emotional, mental, or behavioral distress that interfere with an individual's ability to function in daily life. 9 SPD scale strongly discriminates between community cases and non-cases of DSM-IV diagnoses. 9 People with diabetes have been reported to have SPD as much as two times higher than their counterparts. 10 Similar to earlier studies that included people with disabilities, Okoro et al. found that adults with disabilities are nearly seven times more likely to report SPD than those without disabilities. 11 Healthy People 2030 reported data from the 2018 NHIS showing that 22% of adults with disabilities aged 18 years and over experienced SPD. 12 SPD often shows significant associations with individuals’ lower quality of life 13 and can exacerbate disabilities in individuals with diabetes and further negatively affects the quality of self-management. For example, people with diabetes or disabilities have been reported to be at higher risk for adverse health behaviors, including physical inactivity, smoking, excessive alcohol consumption, and diabetes-specific self-care.11,14,15 People with both diabetes and functional disabilities are at higher risk for SPD 16 and may be more affected by psychological distress, which will further impair their ability and performance of activities needed to maintain health, including adherence to medications, regular health checks, and practicing healthy behaviors.14,15,17,18 Adults with both diabetes and disabilities might need additional support mechanisms incorporated into treatment protocols to assist them in preventing or reducing psychological distress. Understanding the factors associated with SPD is critical for this population, as detecting SPD early and tailoring interventions for individuals will help them maintain health and prevent or delay complications of co-occurring diabetes and disabilities.
Several demographic and physical health factors are reported as relevant to SPD. In one instance, Huang et al. analyzed data for 3474 people with diabetes, finding that being Hispanic, younger in age, or having more chronic diseases served as significant factors that increased the prevalence of SPD. 19 Okoro et al. studied 52,456 adults with disabilities, reporting that compared to non-Hispanic Whites, Hispanics, the unemployed, and the previously married or who had never married had a greater risk of experiencing SPD. People with chronic health conditions such as asthma, coronary heart disease, diabetes, high cholesterol, stroke, and obesity are likewise at increased risk of having SPD. 18
Importantly, social support has been reported as a key factor in the care and health outcomes of people with diabetes or disabilities. Social support may buffer the impact of diabetes distress on health-related quality of life in people with T2DM 20 and modify the association between disability acquisition and mental health. 21 Social isolation and lack of social networks contributed to lower levels of physical activity, lower fruit and vegetable consumption, being overweight or obese, more smoking, fair/poor general health, and dissatisfaction with life.22–24 People with both diabetes and disabilities are at greater risk for mental distress, which can adversely affect healthcare activities. The positive relationship between social and emotional support, health outcomes, and life satisfaction warrants further examination. However, there is a lack of research that takes into account the influences of social and emotional support, as they are critical to the psychiatric and medical care of people with both T2DM and functional disabilities. Moreover, one objective of Healthy People 2030 for people with disabilities is to reduce the proportion of adults with disabilities who experience SPD from 22% to 7.6%. 12 Thus, the purpose of this study is to examine the magnitude of the effects of social and emotional support on SPD among people with both T2DM and functional disabilities. The research question for this study was how social and emotional support affects SPD in individuals with both T2DM and functional disabilities after controlling for socio-demographic factors and health status.
Methods
The data were extracted from the 2021 National Health Interview Survey (NHIS), collected by the National Center for Health Statistics (NCHS) at the CDC. 25 The NHIS is an annual survey representative of non-institutionalized civilians 18 years or older in the U.S. Households are selected using a cross-sectional, geographically clustered sampling methodology. Participants were initially interviewed in person by trained Census Bureau interviewers, with follow-ups via phone. 26
Sample
We used data from the sample adult core component of the NHIS, which included 2650 individuals who answered “Type 2” to the question “According to your doctor or other health professional, what type of diabetes do you have? Is it type 1, type 2, or some other type?” The Washington Group Short Set on Functioning Scale 27 was used to determine if participants have disabilities. This scale includes six domains of functioning: seeing, hearing, mobility, communication, cognition, and self-care. Respondents were asked about difficulties they experienced for each, be it no difficulty, some difficulty, a lot of difficulty, or if they cannot perform the given activity. Any respondent indicating a lot of difficulty or being unable to do an activity in any domain was considered to have a disability 1 and was selected from the pool of 2650 people to be included in the study. Excluding missing responses, the sample size was 592. Each variable included here had missing data of less than 5%, sufficient for assuming a 5% alpha error with 80% power.
Measures
Demographic variables consisted of race/ethnicity (Non-Hispanic White, Hispanic, Black, and other), sex (0 = female, 1 = male), age in years, education (0 = below high school, 1 = high school degree or above), marital status (0 = single, 1 = married/living with a significant other), and employment status (0 = not working, 1 = worked last week). Physical health-related factors included: (a) the number of other chronic diseases, or a summed score if participants answered “Yes” for hypertension, heart disease, stroke, COPD, asthma, cancer, kidney disease, liver disease, or arthritis, which are common co-morbidities among patients with diabetes or geriatric populations 5 ; (b) years since diabetes diagnosis; and (c) if taking insulin (0 = no, 1 = yes). Social/emotional support was assessed by asking participants, “How often do you get the social and emotional support you need?”, with responses, “rare/never,” “sometimes,” “usually,” or “always.”
SPD was assessed with the Kessler-6 scale. It measures frequencies of experiencing six different manifestations of psychological distress over the past 30 days: (1) nervous; (2) hopeless; (3) restless; (4) depressed; (5) everything was an effort; and (6) worthless. SPD is used widely in general-purpose health surveys. Possible scores ranged from 0 (no mental distress) to 24 (SPD). Scoring 6 or greater indicates mental distress, and 13 or greater suggests SPD. 9 This scale has demonstrated good reliability with a Cronbach's alpha of 0.88 in a study among people with diabetes. 19 Our logistic regression analysis had a cutoff score of 13 and used the NHIS's dichotomous variable SPD (0 = no, 1 = yes). 9
Ethical considerations
This study has been exempted from Ethics Review Board approval since it is a secondary analysis of a dataset that has already been identified for public use.
Data analysis
Data were managed using SPSS 28.0. Descriptive statistics were used to describe the participants’ characteristics. Independent t-test and Chi-square analysis compared differences between participants with and without SPD. A hierarchical logical regression analysis predicted SPD (no = 0, yes = 1) from the following predictors: (1) demographic factors, including race, gender, education level, age, marital status, and employment status; (2) physical health factors, including the number of other chronic diseases, years of having diabetes, and insulin usage; and (3) social and emotional support. Beta coefficients (β) and odds ratio (OR) with a 95% confidence interval (95% CI) were computed with the statistically significant value set at p < 0.05.
Results
Participants’ demographic and clinical information appear in Table 1. This study included 592 participants. This included 65.4% non-Hispanic White, and 42.2% were males. About half (49.3%) had at least a high school degree. The average age was 67.88 ± 11.36 years old. The average number of other chronic diseases in addition to T2DM was 2.97 ± 1.44, and the average years since being diagnosed with T2DM was 16.88 ± 11.68. Around 40% received insulin treatments to manage T2DM. Two-thirds (66.6%) of participants reported usually or always receiving needed social and emotional support.
Descriptive characteristics of the sample (N = 592).
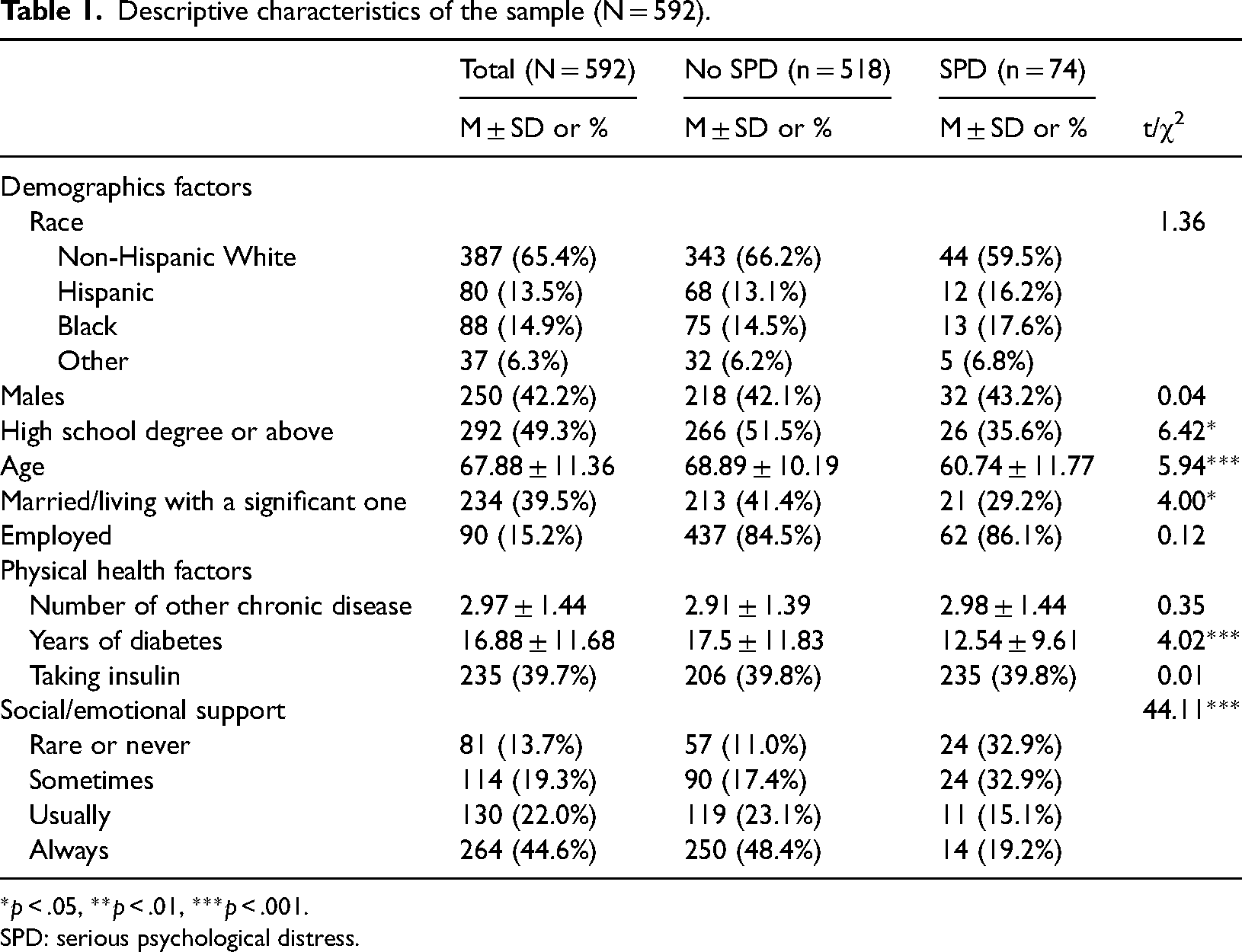
*p < .05, **p < .01, ***p < .001.
SPD: serious psychological distress.
Comparison between SPD groups
Seventy-four (12.5%) participants were in the SPD category. The prevalence of SPD significantly differed based on the participants’ education level (χ2 = 6.42, p < 0.05), age (t = 5.94, p < 0.001), marital status (χ2 = 4.00, p < 0.05), years of having diabetes (t = 4.02, p < 0.001), and perceived difference in levels of social support (χ2 = 44.11, p < 0.01). Detailed comparisons between the two SPD groups appear in Table 1.
Hierarchical logistic regression analysis
Table 2 presents the hierarchical logistic regression analysis findings, identifying significant predictors of non-SPD versus SPD. The entire model containing all predictor variables explained 25.5% (Nagelkerke R2) of the variance in SPD and was statistically significant (χ2 = 79.05 p < 0.001), indicating the model's ability to distinguish between people categorized in non-SPD versus SPD groups. Initially, we observed decreased odds of SPD among older individuals (β = −0.07, OR = 0.94, 95% CI = 0.91–0.96, p < 0.01) and being married (β = −0.64, OR = 0.94, 95% CI = 0.29–0.97, p < 0.05). In the second model, age remained significantly associated with SPD, but among physical health factors, only years of having diabetes were significantly associated with SPD; those with diabetes for a shorter duration were more likely to have SPD (β = −0.03, OR = 0.97, 95% CI = 0.94–1.00, p < 0.05) compared to those who lived longer with diabetes. In the final model, participants of younger age (β = −0.05, OR = 0.95, 95% CI = 0.93–0.97, p < 0.001) and shorter duration of having T2DM (β = −0.04, OR = 0.97, 95% CI = 0.94–1.00, p < 0.05) were more likely to report SPD compared to older persons with a longer diagnosis of T2DM. Having at least a high school degree (β = −0.63, OR = 0.54, 95% CI = 0.30–0.97, p < 0.05), and perceptions of having received social or emotional support at “usual” (β = −1.25, OR = 0.29, 95% CI = 0.11–0.70, p < 0.01) or “always” (β = −1.91, OR = 0.15, 95% CI = 0.07–0.34, p < 0.001), frequencies were less likely to report having SPD compared to those reporting rare or no social support.
Hierarchical logistical regression model of SPD (N = 592).
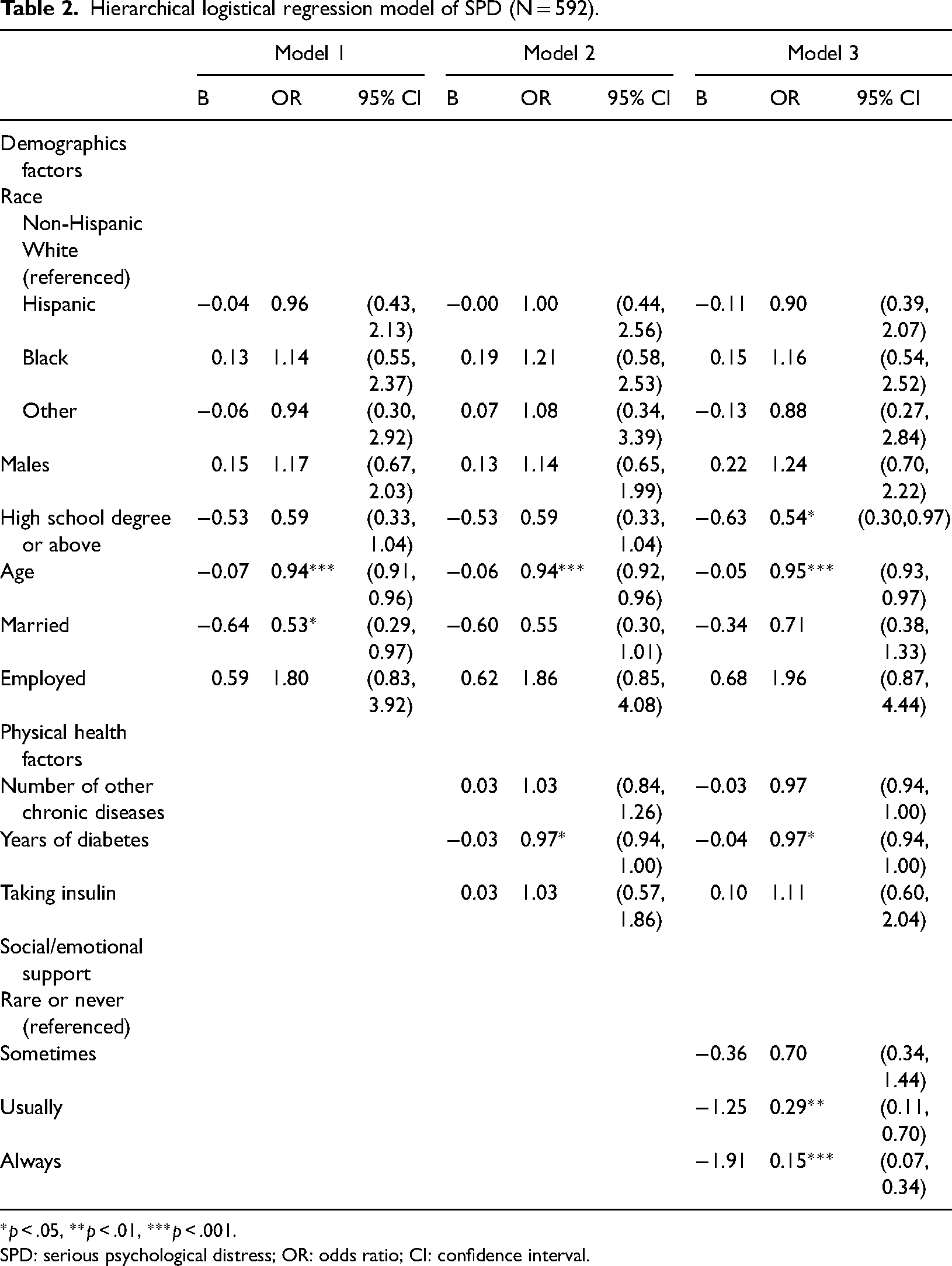
*p < .05, **p < .01, ***p < .001.
SPD: serious psychological distress; OR: odds ratio; CI: confidence interval.
Discussion
It is crucial to understand how multiple factors, including demographics, physical health, and social support contribute to mental health risks in people with both T2DM and functional disabilities to inform appropriate responses to increased mental distress risk. Factors include demographics, physical health, and social support. Here, we analyzed data from a nationally representative population, finding that adults with disabilities and as well as diabetes have a higher prevalence of SPD (12.5%), about three times higher than the general population prevalence rate of 3.2% to 4.0%. Even though SPD does not map directly to specific DSM-IV diagnoses and is not used to assess diabetes-related distress, it can capture more general psychological distress, which strongly correlates with poor health outcomes and undertreatment among people with either diabetes or functional disability.10,18,28
People who had less than a high school degree, were younger in age, and had a more recent diagnosis of diabetes were more likely to report SPD. These findings remain consistent with other studies examining SPD in people with either disabilities or diabetes.10,18,19,29 Younger adults or those with a more recent disability diagnosis may experience challenges and barriers in managing family, social, and work responsibilities, 30 dealing with financial concerns, 31 or accessing health care. 32 Further, younger adults with diabetes and an additional functional disability may experience challenges in entering the workforce, which may limit their ability to live independently and increase psychological distress. 33 Self-management education, along with appropriate transition support to new social roles and employment support services for young adults with diabetes and disabilities, may prove effective in helping them manage the changes and challenges associated with diabetes and related functional disability. For instance, the Chronic Disease Self-Management Program (CDSMP), which focuses on disease management skills, including decision-making, problem-solving, and action planning, has been shown to be an effective strategy for improving patients’ self-efficacy, health distress and depression, energy and fatigue symptoms, social limitation, and cognitive symptoms. 34
In addition to analyzing demographic and physical health factors, this study explored the role of social and emotional support in SPD. As hypothesized, social and emotional support made substantial contributions to the predictive model of SPD. Participants who reported “usually” and “always” receiving social and emotional support were found as less likely to report SPD than those reporting “rarely” or “never” receiving such support. Our findings highlight the importance of social and emotional support in preventing SPD among people with combined diabetes and functional disability. Here, SPD incidence was substantially greater among participants with an unmet need for support. Our study found that only 66.6% of people with both T2DM and a disability received the needed level of social and emotional support, lower than that of adults without a disability (78.6%). 35 This indicates that the assessment of social and emotional support is highly congruent with the practice of primary care for people with both diabetes and a disability. Healthcare providers should ensure access to social support and networks to minimize the development of SPD. Special considerations should be given to individuals more likely to develop SPD because of risk factors such as inadequate social and emotional support, unmarried or living alone status, lower educational attainment, and financial hardships. 35 Additionally, the findings suggest the necessity to incorporate social and emotional support and psychological distress prevention and management interventions into diabetes self-management education programs. Given that social support is a core component for self-management of chronic conditions, 36 it appears important to help expand a patient's social network and include family members or caregivers and peer support in rehabilitation plans for people with diabetes-related functional disability.
Some limitations of this study exist that are worth noting. First, despite being a national survey, this study used a cross-sectional design, so a causal relationship between SPD and other variables cannot readily be determined. Longitudinal studies are needed to better understand the influence of social support on SPD. This data was collected in 2021 from people living in the U.S. who might still have been adjusting to lifestyle changes during the COVID-19 pandemic. Practices like social distancing and gathering limitations could have contributed to social support needs. These factors ought to be taken into consideration when interpreting findings from this study. Similarly, participants’ social desirability concerns and recall response bias could have influenced survey responses, especially for sensitive/stigmatized questions such as psychological distress. This study used a single question to evaluate social and emotional support, a practice widely used in national surveys.26,37 Still, the single question might not be comprehensive enough to capture multiple dimensions of social and emotional support. For example, social and emotional support consist of multiple domains (e.g. amount of social and emotional support; source of social and emotional support, including family-focused and friend-focused support, transaction of various forms of support, including instrumental, emotional, and informational support; and perceived quality and satisfaction of social/emotional support). Such a multifaceted nature of social and emotional support should be considered in future studies with the use of other measurement tools, including the Perceived Support Scale that includes 17 questions to evaluate in greater detail the type of social support and satisfaction with support, 38 or the Multidimensional Scale of Perceived Social Support (MSPSS) that includes 12 items measuring perceived adequacy of social support from family, friends, and significant others. 39 More attention should be given to social and emotional support as a focus of intervention efforts to improve patients’ psychological well-being and further improve overall health outcomes. Healthcare providers should routinely assess the quality of social and emotional support for people with both diabetes and functional disabilities and provide appropriate care, such as helping to navigate resources or involving primary or secondary caregivers in patient care.
Conclusion
This study analyzed extracted data from the 2021 NHIS and found that social and emotional support is a key factor in protecting individuals against the negative mental health effects of having both diabetes and disability acquisition. These findings may apply to populations with both functional limitations or disabilities and T2DM. Populations in the analysis who experienced less social and emotional support are likely to be more vulnerable to poor mental health and may have an increased risk of poor disease management and unhealthy health behaviors. Most importantly, we found that the effects of younger age and more recent diabetes diagnosis on SPD were of much greater magnitude than being older and having longer diabetes diagnoses. The findings from this study highlight the need to develop policy and practice strategies to screen and support people at a higher risk of developing SPD.
Footnotes
Contributorship
Y.C.H. contributed to the conceptualization of the research question, data research, conducted data analysis, and wrote the manuscript. M.B. contributed to the conceptualization of the research question, contributed to idea discussions, and reviewed/edited the manuscript. E.C. and H.Y. contributed to idea discussions, and reviewed/edited the manuscript. Y.C.H. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of interest statement
The authors reported no potential conflicts of interest. This manuscript has not been published and will not be submitted elsewhere for publication while being considered by the Chronic Illness. However, the abstract was presented in the Southern Nursing Research Society (SNRS) conference poster presentation section on 3/2/2023.
Ethical approval
This study has been exempted from Ethics Review Board approval since it is a secondary analysis of a dataset that has already been identified for public use.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Dr Ya-Ching Huang.