
Abstract
Objectives
To identify perceptions and experiences related to caring science and collaborative care in intervention participants of the Collaborative Care to Alleviate Symptoms and Adjust to Illness (CASA) study, a randomized, multi-site clinical trial for patients with chronic heart failure and reduced health status.
Methods
Forty-five participants completed semi-structured, telephone interviews with a focus on intervention components, impact of the intervention on participants’ lives, and recommendations for intervention change. Data were analyzed using an inductive content analysis approach focusing on the presence and frequency of text to identify patterns, categories, and themes across participants without an a priori code book. The validity of the identified categories was enhanced through triangulation.
Results
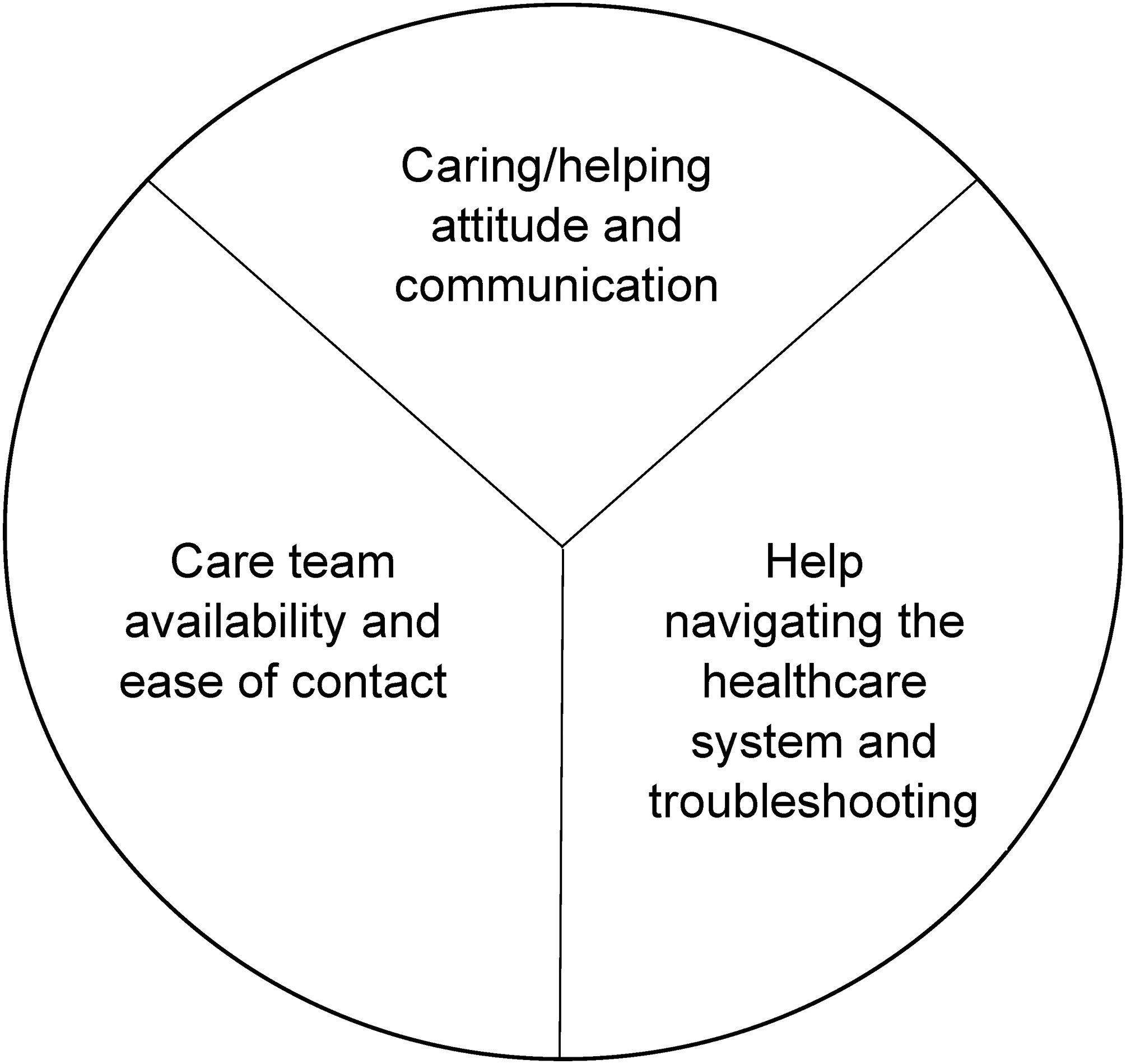
Three themes were identified: (1) intervention providers’ caring/helping attitude and caring/helping communication; (2) care team availability to respond to concerns or questions; and (3) help with understanding and navigating the healthcare system.
Discussion
Patients highly value caring attitudes and communication, availability, and empowerment to understand and navigate healthcare systems. These attitudes and behaviors may be important mediators of the success of collaborative care programs. These are consistent with the theory of caring science, a framework that is relevant more broadly to patient-centered and team-based care models.
Introduction
Collaborative care is an evidence-based intervention supported by nearly 80 randomized clinical trials in 24,308 patients. 1 While much of the evidence for collaborative care demonstrates improvement in depression and anxiety, trials have also found improvements in pain, fatigue, diabetes, cholesterol, and hypertension control.2–6 Collaborative care is a multi-professional, team-based approach to patient care, with a structured management plan, scheduled follow-up, inter-professional communication, and case management. Case management involves a health worker taking responsibility for follow-up care to assess patient adherence to treatment, monitoring progress, and taking action when treatments are unsuccessful. 1 Collaborative care is well designed to address the needs of patients with multimorbidity and complex health needs by integrating primary care and specialist care. Furthermore, collaborative care is patient-centered. 7
The Collaborative Care to Alleviate Symptoms and Adjust to Illness (CASA) intervention was developed to improve quality of life for patients with heart failure by integrating palliative care approaches for symptom management and psychosocial care for depression with disease-specific medical management. 8 Designed using a patient-centered care framework, the collaborative care team included a primary care physician, registered nurse, social worker, cardiology, and palliative care physician. While their heart failure-specific health status did not significantly improve, participants in the randomized clinical trial reported improvements in anxiety, depression, and fatigue. 5
Despite the successes of collaborative care, few studies have sought patients’ perspectives on why or how collaborative care is useful. Two systematic reviews of collaborative care concluded that further understanding is needed for how to best disseminate collaborative care, especially using qualitative methods with key stakeholders.9,10 Understanding patients’ perspectives on collaborative care could yield insights on important mechanisms for not only collaborative care, but also patient-centered care and team care.
To further understanding of patients’ perspectives of collaborative care, the CASA intervention trial pre-planned a qualitative assessment of participants’ experiences. Prior work from our group described the key palliative care intervention components and processes that participants described. 11 In this paper, we describe the “caring” themes that emerged and examine the concept and importance of caring science within collaborative care delivery models.
The concept of “caring” is considered a core component of medicine 12 and nursing. 13 Caring science is an approach to healthcare that prioritizes holistic, compassionate care and the importance of human connection, empathy, and understanding. Caring science demonstrates associations of caring with both clinician and patient outcomes. 12 Caring science includes contributions from all over the world which differ in definitions of caring, philosophical underpinning, conceptualization of clinician–patient relationship, and practical application.14–19 For example, Watson's theory prioritizes human relationships, while Leininger's theory emphasizes culture and diversity. In this manuscript, we used Watson's theory to interpret the results because of its applicability across settings,20,21 evidence base, 22 and focus on relationship processes23–25 that emerged during our analysis. Watson's theory is based in 10 Caritas Processes© that describe caring as a process between two individuals that helps in finding meaning in health or illness experiences. 24 These caring relationships can transcend the specific caring acts physically given or received, allowing for healing, dignity and humanity to be centered for both the caregiver and care-receiver.
Methods
This qualitative study was a pre-planned aim of a National Institutes of Health-funded multi-site randomized clinical trial of CASA (clinicaltrials.gov NCT01739686) 8 approved by the Colorado Multiple Institution Review Board (COMIRB #11-0969). In the randomized clinical trial, we studied whether CASA, a symptom and psychosocial collaborative care intervention, improved heart failure-specific health status, depression, and symptom burden in patients with heart failure. 5 CASA included (1) a registered nurse who addressed common symptoms using structured guidelines developed for the study; (2) a social worker who provided a structured psychosocial intervention to help patients adjust to living with illness and address depressive symptoms, if present; and (3) a team, including the nurse, social worker, a primary care clinician, palliative care specialist, and cardiologist that reviewed patients’ care and provided orders for tests and medications to patients’ clinicians for review and signature. The nurse and social worker training, described elsewhere, 8 included training in empathic communication and motivational interviewing.
The pre-specified objectives of the qualitative evaluation were to (1) identify valuable core intervention content and processes and (2) identify barriers and facilitators to the implementation and sustainability of the intervention. 8 The project was led by a palliative care researcher (D.B.B.) with 8 years of clinical experience providing collaborative care to patients with serious illness. The Consolidated Criteria for Reporting Qualitative Research (COREQ) 32-item checklist is included in Appendix 1.
Setting and participants
Participants were enrolled into the trial from the Veterans Affairs Eastern Colorado Health Care System (provides care to qualifying United States veterans), an urban safety-net hospital (provides care to underserved urban persons), and an academically affiliated hospital (provides care to whole state of Colorado). Patients with heart failure were identified through study sites’ electronic health records. The diagnosis was defined using administrative data supplemented with diuretic dosing (furosemide ≥20 mg/day or equivalent), left ventricular ejection fraction ≤40%, or brain natriuretic peptide (BNP) levels ≥250 pg/mL or NT-proBNP ≥ 1000 pg/mL. During the study screening process, patients who reported reduced heart failure-specific health status (Kansas City Cardiomyopathy Questionnaire Short Version (KCCQ-12) score of less than or equal to 70) and were bothered by at least one of the study's target symptoms (fatigue, shortness of breath, pain and/or depression) were targeted for enrollment. Patients with active substance abuse or serious mental illness were excluded. During informed consent, participants were aware they may be offered participation in an optional interview if they were randomized to the intervention arm.
In addition to interviews with intervention participants, interviews with participating primary care physicians (N = 4) and close-out summaries completed by the intervention team nurse and social worker were conducted.
Data collection
All participants who were randomized to the intervention arm and completed the 6-month self-report measures were offered participation in the interview. There was no limit placed on the sample size of interview participants. The interview guide (Appendix 2) was developed and piloted in the CASA pilot study 26 and subsequently revised for the CASA randomized clinical trial. A qualitative research assistant conducted the interviews and was trained by the study PI (D.B.B.) and qualitative methodologist for the project. Interviews were conducted by telephone, audio-recorded, and transcribed verbatim.
Primary care physicians were asked about their experience with the CASA intervention, what they heard from their patients about CASA, and what recommendations they had to improve the CASA intervention. Close-out summaries were completed by the team nurse and social worker when participants completed the intervention. The summaries documented participant characteristics, what did and did not work about the intervention for that participant, and barriers and facilitators of the health care system that impacted intervention success.
Data analysis
Data analysis was performed after completion of data collection. All transcripts were entered into ATLAS.ti software for data organization and management. We utilized a descriptive content analysis 27 for coding within a general inductive approach, meaning we developed initial codes by reviewing the data rather than an apriori codebook. Our analysis focused on the presence and frequency of text to identify patterns, categories, and themes across participants. One analyst coded five transcripts and then reviewed the codebook and transcripts with a second analyst. The two analysts revised the codebook and jointly recoded the five transcripts, then separately coded additional transcripts until there was 100% accuracy with joint coding (n = 10 additional transcripts). One analyst coded an additional 10 transcripts, which were reviewed by the second analyst with coding unchanged. The first analyst then coded the remaining transcripts. Content codes were grouped and compared to develop broader themes around participant experiences of the intervention. The sample size was not determined by achieving saturation as all participants completing the intervention were invited to participate in interviews. However, at the conclusion of the coding process, no new or additional codes were emerging from the interview text. As results emerged, the research team identified participants’ expression of caring as critical to collaborative care. Therefore to present participants’ perspectives regarding the importance of “feeling cared for as a care recipient,” we matched caring-related text categories to Jean Watson's Caring Science “Caritas Processes”23–25 to provide a broad framework of themes focused on understanding the importance and relevance of caring within broader team-based care models.
To promote analytic rigor, triangulation was used throughout the data analysis process. The analysts met regularly with the broader research team to review the emerging results. Data triangulation was performed by comparing emerging results from this analysis to (1) close-out summaries of intervention participants completed by the nurse and social worker and (2) interviews with participating primary care physicians. An audit trail describing the analytic process was maintained throughout.
Results
Of 158 participants randomized to the intervention arm, 124 completed 6-month follow-up measures and were offered participation in the interview. Of 124 eligible participants, 45 (36%) participated in the interview and were included in analysis. Interview participants (Table 1) were primarily white and male in their seventh decade of life (67.1 ± 9.7 years). Participants had chronic heart failure, with the majority within New York Heart Association Functional Class II and III; impaired health status as measured by the Kansas City Cardiomyopathy Questionnaire; and symptoms of depression. The population had multimorbidity common to this chronic illness (Table 1). The majority had hypertension, diabetes, and obstructive sleep apnea. There was no difference in interview participation across the three study sites. The only significant difference in characteristics between interview participants and non-participants was that non-participants were more likely to have severely reduced left ventricular ejection fraction (p = 0.03).
Patient participant demographics.
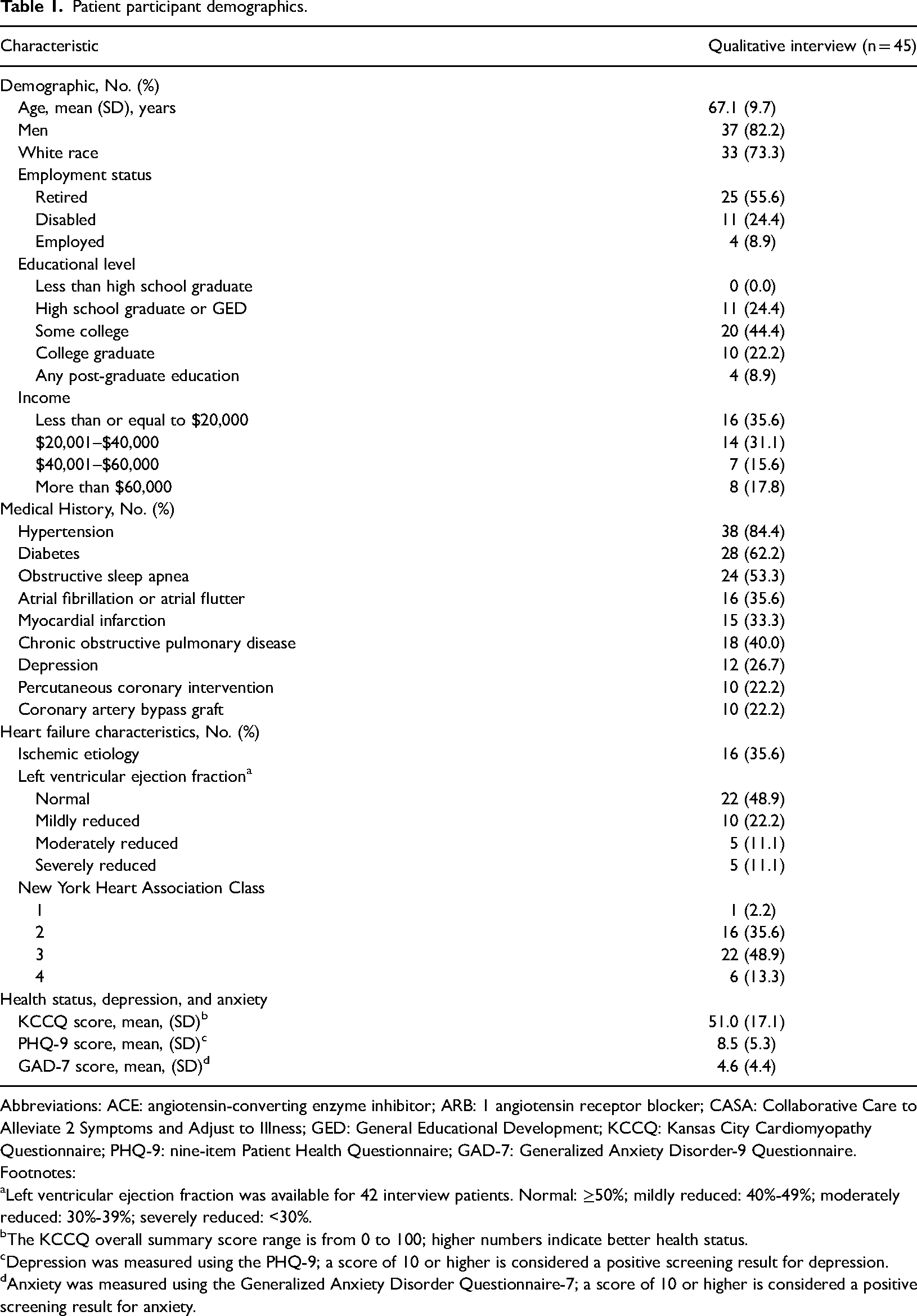
Abbreviations: ACE: angiotensin-converting enzyme inhibitor; ARB: 1 angiotensin receptor blocker; CASA: Collaborative Care to Alleviate 2 Symptoms and Adjust to Illness; GED: General Educational Development; KCCQ: Kansas City Cardiomyopathy Questionnaire; PHQ-9: nine-item Patient Health Questionnaire; GAD-7: Generalized Anxiety Disorder-9 Questionnaire.
Footnotes:
Left ventricular ejection fraction was available for 42 interview patients. Normal: ≥50%; mildly reduced: 40%-49%; moderately reduced: 30%-39%; severely reduced: <30%.
The KCCQ overall summary score range is from 0 to 100; higher numbers indicate better health status.
Depression was measured using the PHQ-9; a score of 10 or higher is considered a positive screening result for depression.
Anxiety was measured using the Generalized Anxiety Disorder Questionnaire-7; a score of 10 or higher is considered a positive screening result for anxiety.
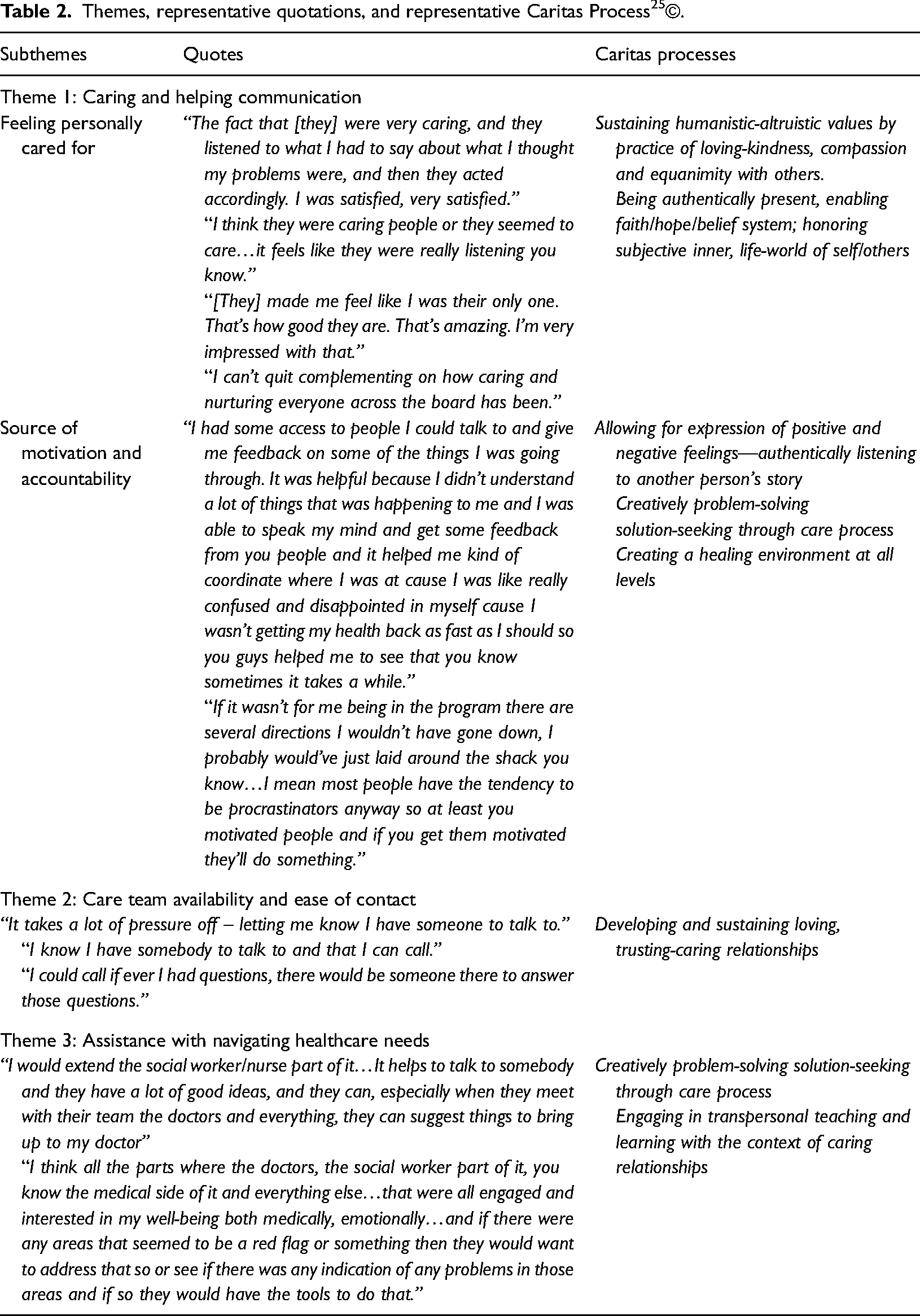
Three major themes captured participants’ perception of the value of the CASA collaborative care intervention (Figure 1). These three themes all related to caring and included: (1) intervention providers’ caring/helping attitude and caring/helping communication; (2) care team availability to respond to concerns or questions; and (3) help with understanding and navigating the healthcare system. Table 2 presents the three major themes with representative quotations and the corresponding Caritas Processes with which they align.
What is caring in collaborative care for chronic illness?.
Themes, representative quotations, and representative Caritas Process 25 ©.
Theme 1: intervention providers’ caring/helping attitude and caring/helping communication
Participants expressed that feeling personally cared for, receiving helpful advice from team members, and having a sense of motivation and accountability to the two members of the intervention team (nurse and social worker) was one of the most beneficial experiences of the intervention. These feelings of being cared for stemmed from the direct, regular communication as part of the intervention process with the participants and team members. One participant in response to how the program impacted their life, summarized the importance of caring communication in this way: …when you got somebody that's caring…you know somebody does care, and somebody is trying to better your overall health, so I don’t know how anybody could feel that the program wasn’t helpful.
Another beneficial aspect of caring communication with the intervention team was the helpful advice that participants received during the telephone interactions. Multiple participants expressed the positive experience of being able to speak candidly about both medical and personal concerns. One participant summarized the experience with team communication in this way: “I think it is really good for moral and emotional support.” Understanding that they would receive accurate medical responses was another component of helpful advice. One participant who wished the intervention would have lasted longer than 6 months stated: I like interacting with them, they always are positive even when you feel like things are bad, they give you feedback on what's going on with you…with your health they are very, very good at reaching to you on your level, and that to me has been wonderful.
Theme 2: care team availability to respond to concerns or questions
In addition to the scheduled intervention visits, participants had access to the intervention team throughout the study period. Participants highly valued the direct interactions as well as the availability to contact the team outside of structured sessions. On participant stated: “Just knowing someone has your back physically and mentally is very relaxing and takes the pressure off; knowing you can call them with any question or concern and know that they will get back to you.”
Many expressed benefit-finding in the intangible, psychological aspects of having a broader support network readily available through the intervention, even if they did not contact the intervention team outside of scheduled intervention visits. One participant summarized this experience in the following way: “Just that added security I guess of knowing that there were more people and processes to help…that's always beneficial.” Another participant stated: “Just knowing that at least twice a week I’m going to have outside contact with someone, that has been a very big part of it.”
Theme 3: help with understanding and navigating the healthcare system
Through participation in the intervention and direct access to the intervention team, several participants highlighted the improvements in their own understanding of their medical problems: “Several times I called [team members] because I had problems I didn’t understand. I talked to them, and they looked into it to find out if there was anything that could be done.” This highlights that, for this participant, having improved access allowed him to both ask for help in understanding a problem and to have a team in place that would assist him with finding the solution.
In response to the intervention team collaborative process, many participants had additional evaluation or new options for medical management. One participant described having an x-ray test expedited after mentioning a worsening pain during one of the study contacts. Other participants described having a more accurate medication list and understanding their medications better as a result of the intervention. These direct connections from the participant to their medical care through the intervention team were highly valued and were the basis for several to recommend that the intervention should continue over time. One participant succinctly described the experience in this way: “They say they’re going to talk to your doctor and they do. Or they say they are going to send an email to your doctor and they do. So those are all big plusses in my book.” Although these were not specific components of the intervention, these clinician behaviors clearly impacted participants’ downstream perceptions of feeling valued and cared.
Triangulation of themes
Triangulating the three themes from participant interviews with nurse and social worker close-out summaries and primary care physician feedback demonstrated significant alignment across the three groups. Close-out summaries demonstrated that the nurse and social worker also identified helping, caring communication as an important aspect of the intervention. They recommended that in future interventions, staff be specifically trained to recognize the importance of caring communication as part of the intervention. Summaries also overlapped with theme 3 that improving participants’ ability to or assisting participants with navigating the healthcare system was an important aspect of the intervention. These summaries suggested that nurses could be trained to teach patients healthcare navigation skills to improve experiences and outcomes.
Interviews with primary care providers paralleled theme 2, with availability and ease of contact with the nurse being highly valuable. One physician described this availability as “one stop shopping” to help address all of patients’ concerns. Additionally, physicians recognized that the dedicated extra attention from the nurse or social worker, even if medical interventions weren’t changing, was valuable to participants.
Discussion
Participants in the CASA collaborative care intervention valued the feeling of being cared for; the feeling of accountability and importance; their own improvements in understanding; helping communication from the intervention team; the availability and ease of access for communication; and the assistance with navigating the healthcare system. These valued experiences and perceptions by participants further our understanding of how collaborative care improves patient-reported outcomes and the “key ingredients” of collaborative care interventions. Furthermore, these results add to the literature by identifying specific aspects of caring that patient's value, from patient voices.
The Cochrane collaborative care systematic review 1 describes four key ingredients to collaborative care for chronic illness: “multi-professional approach to patient care (primary care provider and at least one other health professional or paraprofessional), structured management plan, scheduled patient follow-up, and enhanced inter-professional communication.” Collaborative care models in practice vary considerably on which components they include, 10 and recent studies note it can be difficult to ascertain what the key ingredients really are. 28 Our research indicates that, from a patient perspective, the most frequently identified positive aspect of the program was patients’ feelings of being genuinely cared for and valued by the intervention team. This demonstration of caring behavior and practice aligns with caring science and Watson's Human Caring Theory, which provides a framework for understanding participant perceptions of the CASA collaborative care intervention.
According to participants, several of the Caritas Processes were demonstrated by members of the intervention team. These Caritas Processes may help explain the themes identified in this study and, in particular, participants’ feelings of being genuinely cared for (Table 2). These include authentically listening and allowing for expression of positive and negative feelings; creatively problem-solving through caring process; engaging in teaching and learning within the context of caring relationship; creating a healing environment; and sustaining human dignity.
The “scheduled follow-up” component of collaborative care over time establishes what Watson describes as a “transpersonal relationship” and the process of caring within this relationship may be one way in which collaborative care interventions lessen symptoms of depression and improve other outcomes. For healthcare professionals at large, establishing a caring relationship has long thought to be a key ingredient to improving patient outcomes. 29 Caring relationships speak to the broader concept of treating individuals with dignity—to make them feel important and valued. 30 For example, individuals who report being treated with dignity have higher levels of care satisfaction and importantly are more likely to receive optimal preventive care. 31
We identified two previous studies that elicited perspectives on experiences with collaborative care from patients with chronic illness or multimorbidity. Patients in a study in England appreciated the holistic nature of collaborative care, yet preferred medical and mental health to be separated, a finding that did not emerge in our cohort. 32 A study from the Netherlands revealed similar patient appreciation of relationships with collaborative care clinicians. 33 A scoping review of the related concept of integrated care identified four themes, 34 three of which resonated with our findings: (1) developing collaborative relationships, (2) personalizing patient care to address individual needs, and (3) improving patient access to care (related to our theme of understanding and navigating the health care system). The development of collaborative relationships is at the heart of caring science and, although difficult to tangibly define, may be a key factor for participants’ experiences and improvements within a collaborative care model.
Were caring skills, attitudes, and behaviors taught as part of the study, or already present in the intervention nurse and social worker? While intervention training included helping communication and motivational interviewing, this study was not designed to answer this question. This question represents a persistent challenge in health service intervention research: how to distinguish the effects of the intervention from the interventionist. 35
This study has limitations. First, not all participants in the intervention completed the structured interviews. Participants with more severely reduced left ventricular ejection fraction were less likely to complete the interviews which may have influenced the results. Additionally, it is possible that participants who had a more positive view of the intervention experience were more willing to participate. Second, interview participants were similar with the majority being white, male retirees which limits the generalizability of these findings. It is possible that individuals who identify with different demographic categories find other components of collaborative care valuable. In future collaborative care studies, utilizing a measure of care experience by participants (for example the Watson Caritas Patient Score) 36 would further our understanding of the importance of caring and the possibility that it mediates improved outcomes.
In conclusion, participants in a collaborative care intervention highly valued feeling cared for by intervention providers through communication, availability and assistance with navigating the healthcare system. Caring science is one framework to explain participants’ positive experiences in collaborative care and one pathway through which interventions are effective. Future work could examine the hypothesis that caring attitudes and behaviors mediate outcomes in collaborative care and other forms of patient-centered and team-based care.
Supplemental Material
sj-docx-1-chi-10.1177_17423953241264862 - Supplemental material for “I Felt Like I Mattered”: Caring is a key ingredient of collaborative care for chronic illness
Supplemental material, sj-docx-1-chi-10.1177_17423953241264862 for “I Felt Like I Mattered”: Caring is a key ingredient of collaborative care for chronic illness by Bridget A Graney, Jennifer Dickman Portz and David B Bekelman in Chronic Illness
Supplemental Material
sj-docx-2-chi-10.1177_17423953241264862 - Supplemental material for “I Felt Like I Mattered”: Caring is a key ingredient of collaborative care for chronic illness
Supplemental material, sj-docx-2-chi-10.1177_17423953241264862 for “I Felt Like I Mattered”: Caring is a key ingredient of collaborative care for chronic illness by Bridget A Graney, Jennifer Dickman Portz and David B Bekelman in Chronic Illness
Footnotes
Acknowledgment
The authors would like to thank Lubin Deng, BA for assistance with Table 1.
Contributorship
DB contributed to the design and implementation of the research; DB, BG and JP contributed to the analysis of the results, the writing and final approval of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the NIH, (grant number NIH/NCATS Colorado CTSA [UL1 TR001082], R01-013422).
Ethical approval
The study protocol was approved by the Colorado Multiple Institutional Review Board (COMIRB #: 11-0969).
Guarantor
DB.
Informed Consent
All participants provided informed consent for participation in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.