
Abstract
Objectives
The study delves into the intricacies of cancer-related fatigue (CRF), the quality of life (QoL), and other demographic variables of female adolescent and young adult cancer survivors (AYACS) in the landscape of Kerala, India.
Methods
The cross-sectional study included 288 female AYACS who were selected through purposive sampling and completed self-reported questionnaires on CRF, QoL, and demographic and clinical data. Statistical analyses were applied, including correlation, one-way ANOVA, and regression.
Results
and discussion: The temporal dimension is particularly interesting, as individuals three to five years post-treatment report heightened CRF and QoL scores. Furthermore, the research unveils the pivotal role played by predictors such as marital status, educational attainment, and employment status in shaping QoL. Marital status and education emerge as positive predictors of well-being. The study unveils compelling insights into AYA cancer survivorship, revealing a profound impact of CRF on the quality of life dimensions. The role of spirituality, sometimes affecting social connectedness, adds intrigue.
Conclusion
The findings provide insights into the complex world of female AYACS, compelling researchers to ponder the significance of addressing CRF and tailoring rehabilitation systems during the critical post-treatment phase, with recognition of gender-specific challenges.
Introduction
Cancer is a global challenge, with an increasing number of diagnoses each year. Early detection, scientific advancements, and technology have improved survival rates, but cancer medications still have negative effects.
1
Adolescent and young adult cancer survivors (AYACS) face unique challenges that impact their social integration and overall well-being. Over 1.2 million AYAs aged 15–39 struggle with cancer diagnoses globally, with 80% expected to survive beyond five years.2,3 This burgeoning population faces the possibility of second cancers and treatment-induced long-term effects. As they transition from active medical intervention to the post-treatment cancer-free phase, they often find themselves ‘lost in transition,’ grappling with managing the repercussions of their illness and treatment rigours.
4
Cancer treatment for AYAs significantly impacts their physical, psychological, and social wellbeing. Despite advancements in treatment, they still wrestle with long-term side effects like fatigue, neuropathy, lymphedema, depression, anxiety, and cancer recurrence.
5
Unlike their older counterparts, AYACS face unique challenges like academic and vocational setbacks, fertility concerns, and social isolation.2,5 Research shows they experience higher levels of distress and unmet needs than their older and younger counterparts, emphasising the need for specialised survivorship care and strategies tailored to their unique needs.
6
Female AYACS are a significant subgroup facing unique challenges such as sexuality and fertility issues, particularly as young women harbouring dreams of future motherhood. They also face issues in identity formation, societal integration, and independence.5,7 Additionally, they experience higher levels of anxiety, depression, PTSD, and worry compared to their male counterparts, which can have long-term effects on their mental well-being if unaddressed.
8
Cancer-related fatigue (CRF) is a common yet under-diagnosed and long-lasting side effect of cancer treatment, lingering in the wake of treatment completion, thwarting attempts to reclaim even the semblance of a ‘normal life’, causing symptoms like anaemia, pain, and discomfort, and affecting an individual's quality of life, employment-ability, and physical manifestations. Female AYACS report higher CRF levels than their male counterparts. Despite progress in research on cancer survivorship, there is still a gap in understanding female survivors’ QoL, along with mounting evidence of gender differences.9,10 Kerala, a state with high literacy rates and a robust healthcare system, is an interesting case study due to its high cancer incidence and survival rates.
10
However, despite high incidence, there is a lack of studies exploring the concerns of this population, let alone AYACS. Thus, this study investigates the impact of CRF on the QoL of female AYACS in Kerala, exploring the following research questions to pave the way for developing targeted support and intervention strategies for this often under-reported cohort.
Is there a significant difference in the level of CRF between groups based on the time elapsed since primary cancer treatment? To what extent does the level of CRF predict QoL and its sub-dimensions in Female AYACS?
Methodology
Study design and participants: Using a cross-sectional design and purposive sampling, 288 female AYACS, diagnosed between 15–39 years (M = 31.7.4, SD = 5) and post-primary treatment, at least three months prior and not more than five years at the time of the study, were recruited from Kerala with the help of online and offline cancer survivors support groups. Inclusion criteria for the participants were (i) 18 + years of age, (ii) Proficiency in Malayalam (regional language) or English, (iii) awareness of their diagnosis, and (iv) absence of comorbidities or psychiatric conditions (as reported by them).
The respondents were divided into three groups: Group 1 (three months to 1 year (n = 88 (30.6%)), Group 2 (1–3 years (n = 107 (37.2%)), and Group 3 (3–5 years (n = 93 (32.3%)).
Procedure
After a brief briefing to the potential participants, interested participants were given a thorough explanation of the study and questions or concerns were diligently addressed.
Following this, participants received questionnaires and an informed consent form. The questionnaire includes questions on participants’ demographic information and medical records, in addition to self-administered assessments of CRF and QoL. The study was in accordance with the standards of the institutional ethics committee of the Indian Institute of Technology, Hyderabad (IITH/IEC/2021/12/13) and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Measure
Functional assessment of cancer therapy- Fatigue (FACT-F): Cancer-related Fatigue (CRF) was assessed using FACIT-F. This self-administered tool measured an individual's level of fatigue during their routine activities over the past week on a Likert scale. The internal consistency measured using Cronbach's alpha was 0.74 among the Indian population. 11 The Cronbach's alpha in this study sample was 0.94.
Quality of life-Cancer Survivor (QoL-CS): QoL was assessed using the QOL-CS, a 41-item visual analogue scale with four subscales (physical well-being (PWB), psychological wellbeing (PSYWB), social well-being(SWB), spiritual well-being(SPIWB). The questionnaire showed good test-retest reliability (.89) and a Cronbach alpha of 0.80–0.89 among cancer survivors. 12 The Cronbach's alpha for this study sample was 0.8.
Analysis
The data was analysed using mean, percentage and standard deviation. Further Pearson correlation, One-way ANOVA and regression analysis were run to analyse the data.
Results
Sample Characteristics
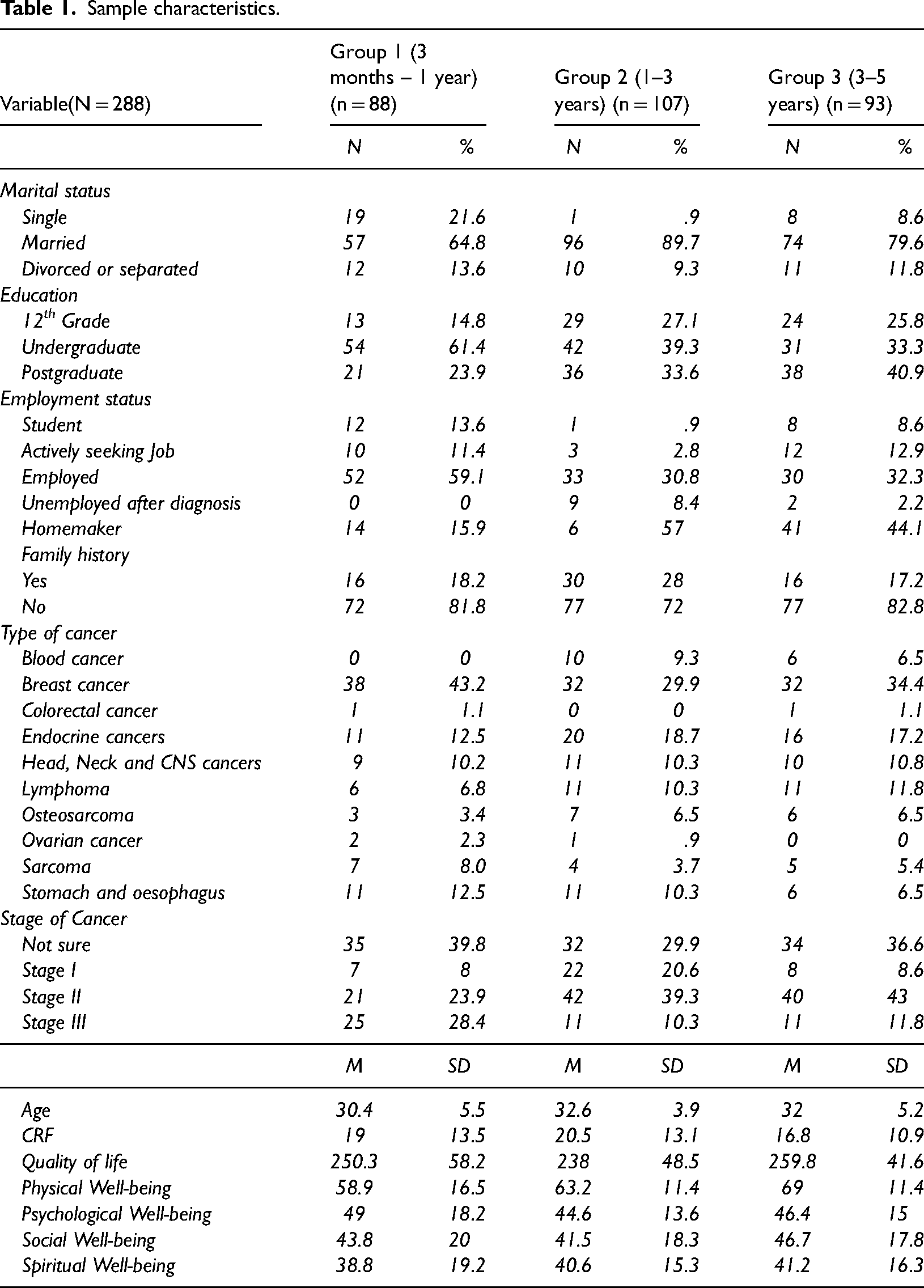
The participants(n = 288) were divided into three groups based on time since primary cancer treatment. The participants in Group 1 (age = 30.4+/- 5.5), Group 2 (age = 32.6+/-3.9) and Group 3 (age = 32+/-5.2) were post-treatment, three months to 1 year, 1 to 3 years and three to five years prior to participation in the study. The Participants were primarily married (78%), had an undergraduate degree(44%), employed(39.9%) and were mostly survivors of breast cancer(37.5%)(see Table 1). Pearson correlation analysis revealed significant positive correlations between QoL and its sub-dimensions with PWB (r = .455, p < .01), PSYWB (r = .618, p < .01), SWB (r = .796, p < .01), and SPIWB (r = .152, p < .01). Noteworthy positive correlations were found between SWB and PWB (r = .465, p < .01) and PSYWB (r = .366, p < .01). While SPIWB exhibited a negative correlation with SWB (r = -.241, p < .01). CRF demonstrated significant negative correlations with QoL (r = -.552, p < .01), PWB (r = -.613, p < .01), PSYWB (r = -.262, p < .01), and SWB (r = -.496, p < .01) implying that higher levels of fatigue are associated with lower levels of QoL (see Table 2).
Sample characteristics.
Correlation matrix.
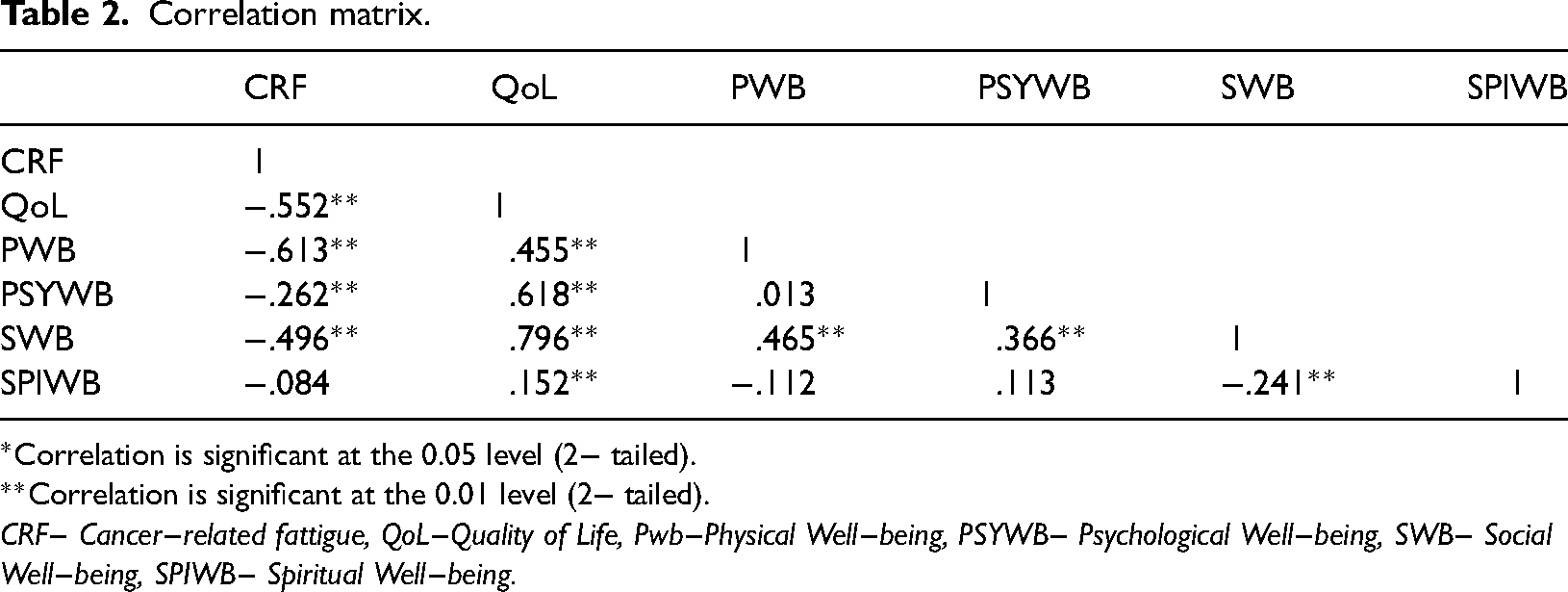
Correlation is significant at the 0.05 level (2− tailed).
Correlation is significant at the 0.01 level (2− tailed).
CRF− Cancer−related fattigue, QoL−Quality of Life, Pwb−Physical Well−being, PSYWB− Psychological Well−being, SWB− Social Well−being, SPIWB− Spiritual Well−being.
One-way ANOVA and Tukey post hoc tests were run to understand the differences between groups based on various independent variables(see Table 3). The groups based on time since treatment revealed significant differences for CRF (F(2285) = 3.4, p < 0.05), PWB (F(2285) = 13.3, p < 0.01), and QoL (F(2285) = 4.8, p < 0.05). Post hoc analyses indicated that Group 3 (3- 5 years post-treatment) exhibited elevated levels of CRF (M = 36.8, SD = 10.9), PWB (M = 69, SD = 11.4), and QoL (M = 259.8, SD = 41.6), indicating the long term effects of cancer treatment on well-being dimensions. Similarly, groups based on marital status revealed statistically significant differences in QoL(F(2, 285) = 3.82, p < 0.05) and PWB (F(2, 285) = 9.01, p < 0.01). Married participants demonstrated higher levels of QoL (M = 263.2, SD = 54.9) and PWB (M = 67.3, SD = 7.6) compared to single, separated, or divorced counterparts, highlighting the impact of companionship on the well-being of study participants. Further groups based on level of education yielded significant differences in CRF (F(2, 285) = 4.3, p < 0.05), QoL(F(2, 285) = 11.2, p < 0.01), PSYWB (F(2, 285) = 11.5, p < 0.01) and SWB (F(2, 285) = 9.4, p < 0.01). Participants with a Master's-level education displayed higher levels of CRF (M = 36.2, SD = 10.4), QoL (M = 257.5, SD = 41.8), and SWB (M = 46.5, SD = 17.1). Furthermore, participants with undergraduate-level education achieved higher scores in PSYWB (M = 49, SD = 16.2), suggesting the effect of education on CRF and QoL dimensions of cancer survivors. Additionally, participants grouped by their occupational statuses show significant differences in CRF(F(3284) = .317, p < 0.01), PSYWB (F(3, 284) = 5.7, p < 0.05), and SWB (F(3, 284) = 4.88, p < 0.05). Employed participants exhibited superior scores in CRF(M = 34.6, SD = 12.2), QoL (M = 260.5, SD = 49.7), PSYWB (M = 49.6, SD = 16.4), and SWB (M = 48.6, SD = 19.2) in comparison to individuals who identified as students, unemployed, or homemakers. However, the type and stage of cancer did not show any differences in well-being. Regression analysis identified predictors of QoL among female AYA cancer survivors(see Table 4). The model for QoL was significant (F(6, 281) = 22.6, p < .001), explaining 34.8% of the variance. CRF (β = -.537, t = -11.10, p < .001), Education (β = .178, t = 3.59, p < .01), and Employment status (β = .125, t = 2.37, p < .05) were significant predictors. Similar patterns were observed for other well-being dimensions, with various predictors explaining significant proportions of the variance. Further, the model was significant for PWB (F(6, 281) = 31.2, p < .001), explaining 42.5% of the variance. CRF (β = -.585, t = -12.8 p < .001), Type of cancer (β = -.094,t = -.2.06, p < .001) Marital status (β = .181, t = 3.68 p < .05) were significant predictors. Additionally, the model was significant for PSYWB(F(6, 281) = 6.128, p < .01), with the predictors accounting for 11% of the variance. CRF (β = -.260,t = 4.59 p < .01), and Level of Education (β = .199,t = 3.19 p < .05) were significant predictors. For SWB, the overall model was significant (F(6, 281) = 19.4, p < .01), explaining 31% of the variance. CRF(β = -.487,t = -9.81 p < .01), Stage of cancer(β = -.124,t = -2.46p < .05), Marital status (β = .098, t = 1.93 p < .05), Level of Education(β = .126, t = 2.47 p < .05) and Employment status(β = .214, t = 3.97, p < .01) as significant predictors. However, the overall model or the individual variables did not predict SPIWB.
Analysis of variance.
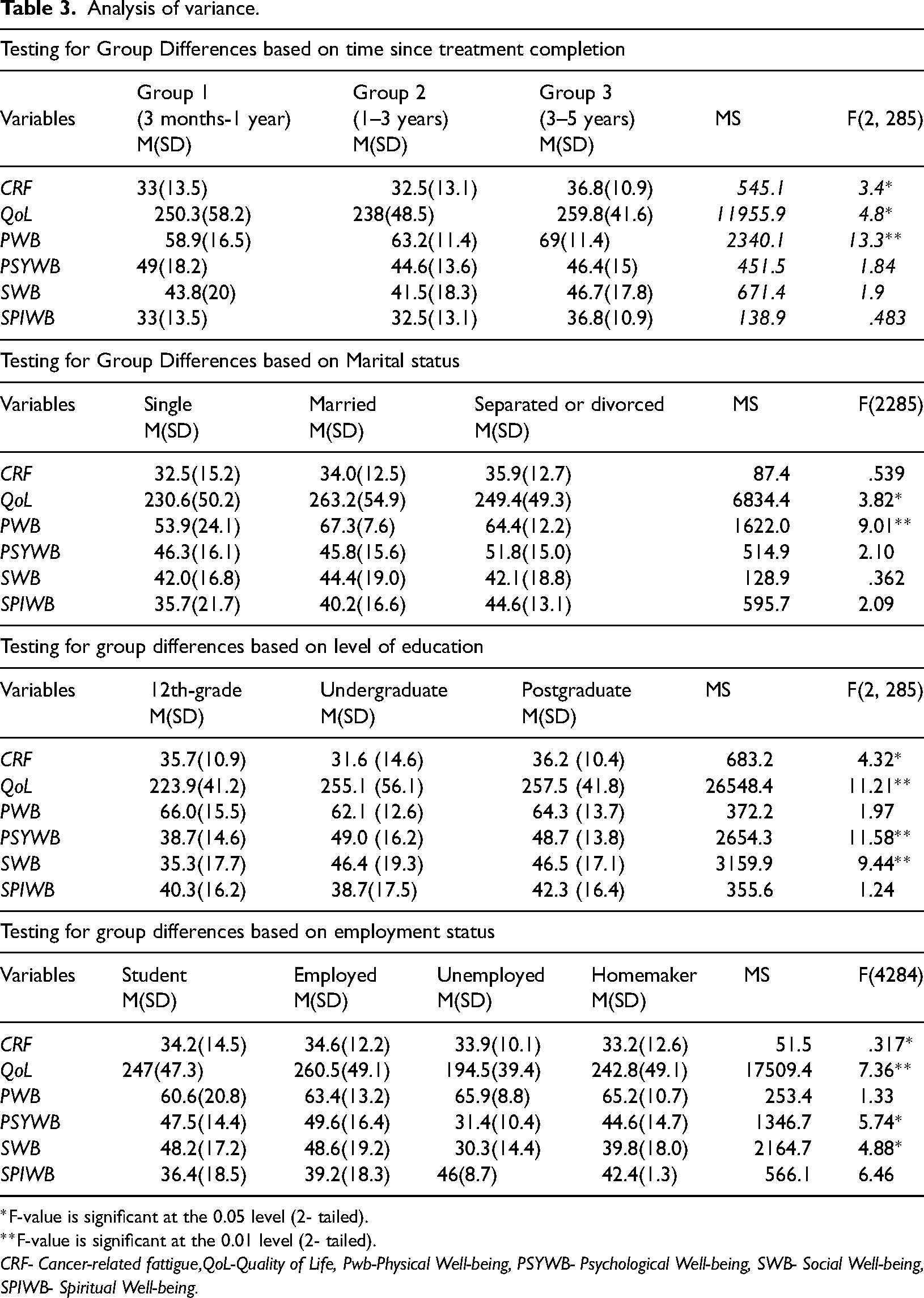
F-value is significant at the 0.05 level (2- tailed).
F-value is significant at the 0.01 level (2- tailed).
CRF- Cancer-related fattigue,QoL-Quality of Life, Pwb-Physical Well-being, PSYWB- Psychological Well-being, SWB- Social Well-being, SPIWB- Spiritual Well-being.
Regression analysis of quality of life predictors.
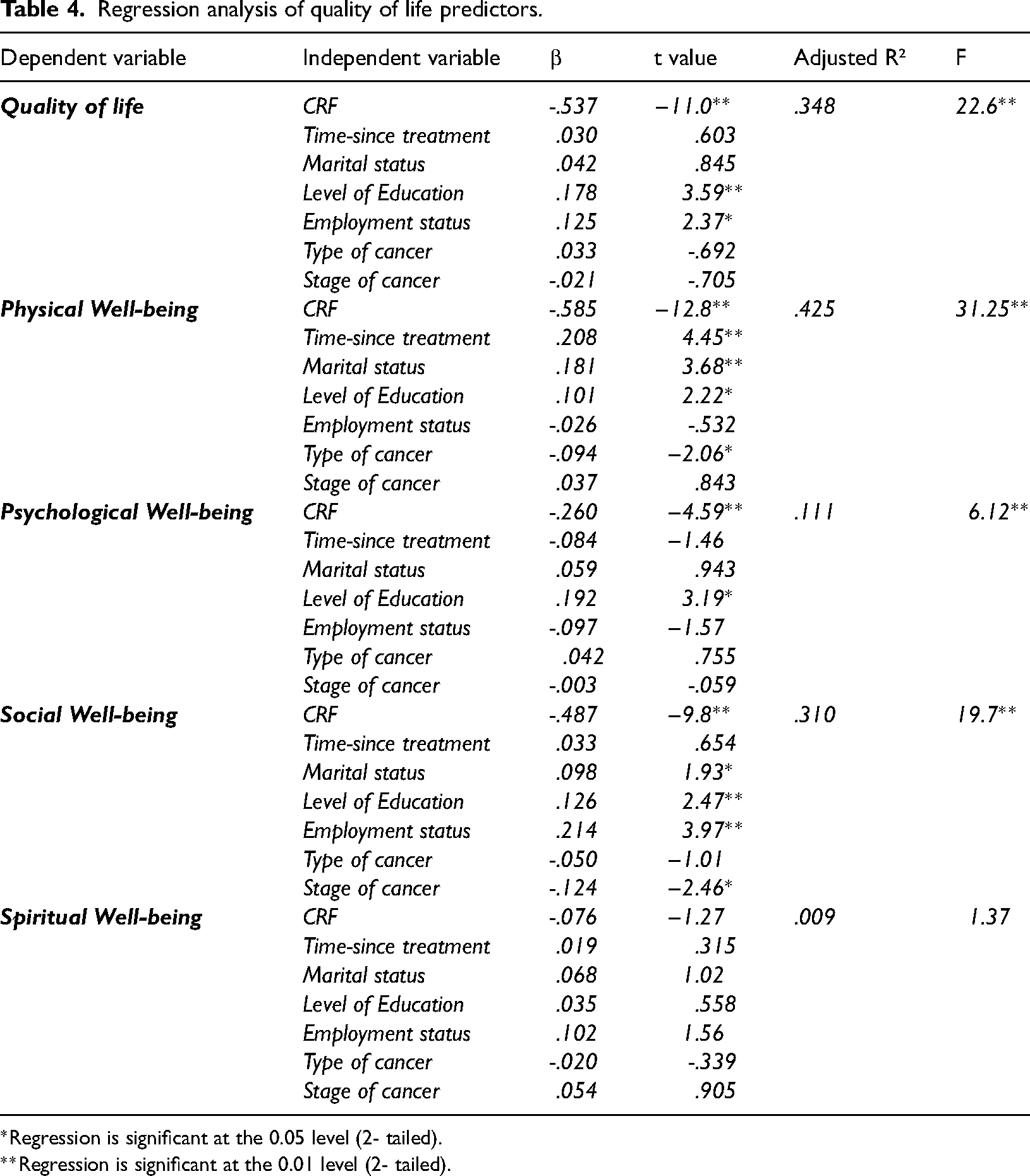
Regression is significant at the 0.05 level (2- tailed).
Regression is significant at the 0.01 level (2- tailed).
Discussion
The post-treatment phase of cancer survivorship is stressful and requires support to recover and re-engage in social and work-life roles. CRF has been linked to poor QoL, 9 studies investigating cancer patients in India also provide evidence for the effect of CRF on wellbeing. 13 Owing to the limited research in the cohort, the study examines the association between CRF, QoL, and demographic variables in post-treatment female AYA cancer survivors in Kerala, using validated CRF and QoL scales.
Predictors of Quality of Life: The study employed a combination of correlation, one-way analysis of variance (ANOVA) and regression analyses to comprehensively examine the predictors of QoL and its sub-dimensions among cancer survivors.
Physical, psychological, social and spiritual well-being
Positive correlations indicate that high scores on PWB, PSYWB, SWB, and SPIWB influence overall QoL. Similarly negative correlation between SWB and SPIWB suggests that more spiritual female AYACS tend to avoid social interaction, which lowers their overall QoL. Hence, here SPIWB acts as a double-edged sword, contradicting previous research which suggests spirituality as a source of comfort, instilling a sense of belonging, existential interconnectedness, and perceived social support. 14 Studies have also identified isolation and social support as strong predictors of SWB. 15 While emotional well-being (EWB) is a crucial component of overall quality of life, its exclusion from this study was due to several factors. The focus on specific domains like physical well-being (PWB), psychological well-being (PSYWB), social well-being (SWB), and spiritual well-being (SPIWB) allowed for a more in-depth analysis of these dimensions, which collectively cover significant aspects of EWB. For instance, PSYWB directly intersects with emotional health, while SWB and SPIWB consider the emotional impacts of social interactions and spiritual peace, respectively. By examining these domains, the study inherently addresses key elements of emotional well-being, even if it wasn't explicitly measured as a standalone factor. Future research could delve into EWB more comprehensively, exploring its intricate relationship with these and other QoL domains.
Cancer-related fatigue
Consistent with earlier studies, 16 the findings indicate a substantial negative relationship between CRF and QoL, as well as with physical, psychological, and social well-being, causing a crippling effect on a person's daily activities, social interactions, work performance, leisure activities, and life satisfaction, ultimately lowering overall well-being. The findings demonstrate CRF's impact on female AYACS and their QoL dimensions, emphasising the importance of addressing CRF to improve the overall health and QoL of female AYACS. This might mean helping cancer survivors with therapies like exercise, CBT, and mindfulness based stress reduction. 17 Regression analysis identifies CRF as a significant negative predictor of QoL in female AYACS in all domains except spiritual well-being. CRF-induced physical exhaustion may have hindered engaging in regular physical activity to maintain health. Similarly, CRF-induced psychological distress, including depression and anxiety, may have contributed to the negative impact on psychological well-being. Previous studies show that CRF also leads to social isolation, reducing survivors’ ability to participate in social activities and maintain relationships. 18 These findings underline the multifaceted nature of CRF and its varying effects on different aspects of a survivor's well-being, emphasising the importance of raising awareness of CRF among survivors, healthcare professionals, and stakeholders and for routine assessment and addressing of fatigue.
Time passed since treatment
The study found significant differences in CRF, PWB, and overall QoL among the three groups based on the amount of time post-treatment. When compared to participants in Groups 1 and 2, Group 3(3–5 years post-treatment) reported the highest levels of CRF, PWB and QoL scores, indicating the long-term impact of cancer treatment. The improvement in PWB and QoL despite higher level of CRF suggests the presence of other significant factors that help cancer survivors through their survivorship journey in improving their well-being. Nevertheless, these findings differ from earlier research in the field, which suggested a significant drop in the prevalence of fatigue after treatment's end. 9 Several interventions, including physical therapy, exercise, and leading an active lifestyle, have been shown to reduce CRF. 16 However, in the current sample, higher levels of CRF could be attributed to a majority of participants being employed and making every effort to return to their normal lives. It was also found that PWB improves over time post-treatment for cancer. Further, the positive relationship in cancer survivors may be attributed to physical recovery, adaptive coping, reduced treatment side effects, psychological adjustment, and ongoing medical monitoring. Hence the results underscore the importance of patience, self-care practices, and long-term medical follow-up in their journey towards recovery and sustained well-being.
Education, employment and marital Status
Aligning with previous research, marital status predicted PWB and SWB, indicating that being in a committed relationship, which provides social support and companionship, may benefit these aspects of well-being, contribute positively to the physical and social well-being of cancer survivors. 19 Level of Education predicted QoL, PWB PSYWB and SWB. In the present sample, having higher levels of fatigue and with most participants being graduates or post-graduates, a higher level of education was linked to a higher quality of life, psychological and social well-being. Better access to resources, improved health literacy, and stronger cognitive abilities may have enabled better health management for educated participants. Previous research suggests that higher education helps survivors perceive control over life stress than patients with basic education and that access to better employment opportunities also leads to better PWB and PSYWB. 20 Employment status significantly predicted QoL and SWB, showing groups-based differences in CRF and PSYWB, indicating better well-being for employed survivors than unemployed participants. Findings indicate that employment helped participants cope better with survivorship challenges and provided them with emotional and social support. However, the higher fatigue scores indicate that their work-related expectations could also have contributed to their stress and physical problems, making it harder to achieve self-actualisation and life satisfaction. 21 Furthermore, in the Indian context, females are expected to solely take care of the family chores along with their occupational responsibilities, 22 contributing to higher CRF. The study suggests that being engaged in work or meaningful activities may contribute positively to the overall well-being of cancer survivors, but the added difficulties while engaging in work-related activities need to be carefully understood to help create tailor-made employment opportunities for female AYACS, emphasising the necessity for vocational rehabilitation and support. Overall, the study emphasises the need for a multidisciplinary approach to address female AYA cancer survivors’ complex and gender-specific needs. Pointing out the importance of understanding the impact of CRF and other demographics, patient awareness, fostering support and knowledge among families, conducting comprehensive assessments, and creating individualised interventions to improve QoL of AYACS. The study also encourages governments and policymakers to support research and create funding initiatives.
Conclusion
The study highlights the negative impact of cancer-related fatigue (CRF) on the quality of life (QoL) of female Adolescent and Young Adult Cancer Survivors (AYACS) during their transition period. It underscores how CRF adversely affects daily activities, social interactions, professional performance, and overall well-being. The study emphasizes the importance of considering physical, psychological, social, and spiritual sub-dimensions when developing interventions and support systems to enhance QoL. Additionally, the necessity of vocational rehabilitation is highlighted to address the increased CRF experienced by survivors, particularly in relation to the challenges of resuming ‘normal life’ post-treatment, including the expectations surrounding their return to work and the pressure to resume regular activities even after three to five years post-treatment. While the study focuses on female AYACS, it is important to recognise that hormonal regulation, which is likely to be impacted differently by cancer treatment in males, could influence CRF and QoL in distinct ways. Therefore, while the predictors of QoL identified in this study provide a basis for developing comprehensive and customised interventions, future research should explore these aspects in male survivors to understand the gender-specific nuances of CRF and QoL. This would ensure that support systems are tailored appropriately for both male and female survivors.
Limitations and future implications of the study: The study on female AYA cancer survivors in Kerala has limitations such as a cross-sectional design, lack of generalizability, and potential response and social desirability biases due to the use of self-report questionnaires. Future research should explore experiences from different locations and use mixed methods for comprehensive interventions.
Footnotes
Acknowledgements
The authors thank Indian Institute of Technology Hyderabad and Indian Council of Medical Research for their support.
Contributorship
All authors contributed to the study's conception and design. First author performed material preparation, data collection, and analysis and wrote the first draft of the manuscript. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee (Institutional Ethics Committee (IEC), IIT Hyderabad (IITH/IEC/2021/12/13))and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author is supported by the Senior Research Fellowship (SRF) from the Indian Council of Medical Research (ICMR) (grant number ICMR JRF 2018 HRD 19).
Guarantor
PNG
Informed consent
Informed consent was obtained from all study participants.
Trial registration
Not applicable