
Abstract
Objectives
To contribute to a better understanding of the complexities of social support exchanged within couples coping with Parkinson's disease (PD), the present study aimed to identify costs and complications of support between persons with PD (PWPs) and their partners, as well as how to effectively manage such challenges.
Methods
In-depth interviews were conducted with 63 participants, including 31 PWPs and 32 partners. Interviews were transcribed and analyzed using constant comparative techniques.
Results
Participants reported the following complications and costs of social support: partners’ differing approaches to coping can make support difficult, support can be perceived as identity-threatening and controlling, support can lead to dependency, and support can be draining. In addition, participants discussed effectively managing challenges of support by seeking/providing support subtly, taking the other's perspective, and relinquishing control.
Discussion
In health care and interventions, it is important for PWPs and partners to be educated about social support so that couples can anticipate these costs and complications of support and consider which management strategies are likely to be effective for them in various circumstances.
Parkinson's disease (PD) is a neurodegenerative disorder that predominantly occurs in older adults. 1 The prevalence of the disease is rapidly increasing, and researchers estimate that there are nearly one million people in the United States living with PD. 2 This chronic, progressive disease is characterized by trouble with movement (e.g., tremor, rigidity) and often accompanied by other changes for the person with PD (PWP) such as difficulties with speech, depression, 1 and fatigue. 3 Moreover, uncertainty is common in the experience of chronic illness in generaleg,4,5 and PD in particular.eg,6,7 The physical manifestations and psychosocial issues related to PD can dramatically impact a PWP's daily life. 1 Furthermore, PD is a “disease of families” 8 (p202) and when a PWP is in a committed relationship such as marriage, PD can also considerably affect the PWP's partnereg,9,10 and their relationship.eg,11–13 For example, Roland et al. 14 found that spousal caregivers of PWPs often experience mental distress related to social isolation and worrying about their partner's safety and well-being. Additionally, caregivers of PWPs have reported physical health issues, 15 depression,15,16 sleep disturbances, 17 and decreased life satisfaction 16 due to the stress of caregiving.
How a couple copes with stressors related to PD may have significant implications for the quality of their relationship as well as each individual's mental and physical health. A form of coping that is particularly relevant to studying illness in a relational context is the exchange of social support, which Goldsmith defined as “what individuals say and do to help one another.” 18 (p13) Although scholars are increasingly exploring psychosocial issues in the landscape of PD (e.g., regarding chronic unpredictability 19 or stigma 20 related to the disease), social support within couples facing PD is not fully understood, as further explicated in the following section. The purpose of the current study is to examine the complexities of social support exchanged between PWPs and partners and, in effect, contribute to this understudied area and offer practical clinical recommendations to help this population.
Review of literature
Social support and Parkinson's disease
The role of social support in coping with PD is in need of further study.21–23 Most research on social support and PD has not focused exclusively on support exchanged within couples and instead has investigated perceptions of, or satisfaction with, support more broadly. The extant research on social support and PD has often demonstrated a positive association between either social support and better functioning (e.g., satisfaction with life or less depression), or dissatisfaction with support and negative outcomes such as distress.eg,24–27 Conversely, some research on PD and social support has produced mixed findings 21 or a lack of evidence regarding the relationship between social support and outcomes like quality of life 23 or depression. 28 For instance, McComb and Tickle-Degnen 21 found that the less support that PWPs reported having, the more stigmatized they indicated feeling. Paradoxically though, in this same study, a PWP perceiving more problems with social support was associated with less bodily discomfort. In discussing the mixed findings from their quantitative study about social support and PD, McComb and Tickle-Degnen noted that “social support is a complex idea” 21 (p58) and there is also a need for qualitative approaches to explore the intricacies of support. Indeed, standardized measures of social support and PD—while they have contributed substantially to this essential area of research and are often valuable for studying large populations—may include items that sometimes yield more complicated answers than can be fully captured quantitatively.
Qualitative studies regarding PD and social support within couples are scarce, a yet have the potential to add to the existing research by exploring complexities of support. Prior
qualitative research related to social support and couples coping with PD includes a study by Birgersson and Edberg, 29 in which they interviewed 6 couples facing PD about their experiences of support. They found that PD entailed a transition for couples’ relationships, and that support from outside sources was more commonly offered to PWPs than partners. 29 Additional qualitative studies regarding couples coping with PD have examined topics that are relevant to, though not focused explicitly on, social support. For instance, in a study about changing relationship dynamics in which they interviewed 15 individuals with advanced-stage PD and their partners, Constant et al. noted that dyads engaged in varying patterns of interaction (e.g., “closeness/withdrawal-resignation”) 12 (p4) as the PWP became more dependent on the partner. Other qualitative studies have also highlighted some of the ways that PD can affect a couple, including, for example, changes such as inducing relationship uncertainty 11 and feelings of being overwhelmed with managing the disease. 13 Although existing research has yielded valuable insight about PWPs’ and partners’ experiences, there is a lack of research regarding social support within couples with PD, including challenges of support.
Normative rhetorical theory of social support
Across various contexts, many benefits of social support (e.g., positive health outcomes) 30 have been reported, yet a growing body of research regarding social support in chronic illness has also acknowledged the existence of complications or problematic (e.g., low-quality or hurtful) support.eg, 31 A useful theoretical lens for understanding why some supportive attempts are more or less effective than others is Goldsmith's normative rhetorical theory.18,32 According to this theory, which has been applied to a variety of illness contexts (e.g., cancer, 33 HIV/AIDS, 34 and heart disease),35,36 social support can entail costs and complications, as well as have multiple meanings such that support that is helpful in some ways may be troubling in others. For example, in their normative rhetorical study of communication occurring between members of a couple in which one partner has undergone cardiac surgery, Goldsmith et al. 36 noted that expressions of caring may be perceived positively, but also can carry obligations for the patient (e.g., to follow advice). Furthermore, communicating about lifestyle modifications may be useful, but could also be viewed as an unwanted reminder of the illness or as a partner's efforts to control the patient. These multiple meanings of support can lead to dilemmas (e.g., whether to offer support).
In explicating this theoretical framework, Goldsmith 18 drew on an assumption established by prior communication scholarship: During any communicative interaction, participants aim to accomplish multiple purposes. That is, any time communication occurs, people are not only engaging in a task, but are also attending to goals related to protecting their own and others’ desired identities and maintaining or creating a relationship with others in the interaction.37–39 Balancing these objectives can be challenging.18,36,40,41 For example, a man with PD whose motor capabilities are diminishing may view his partner's constant assistance with daily tasks like getting dressed, eating, and bathing as largely helpful gestures denoting relational stability. At the same time, he may also feel helpless and distressed by the identity implications of receiving this aid—perhaps worrying that his partner has begun to view him as frail and dependent. Dilemmas like these, which arise as a result of the difficulty of balancing multiple goals (e.g., the task goal of receiving assistance and the identity goal of maintaining independence), can impact the outcomes of social support, making it important to study challenges of support and how to manage them in specific contexts. 18
To that end, the current study examines the complexities of social support within couples coping with PD, about whom further social support research is needed.21–23 Because social support has sometimes, but not always, been associated with positive effects, identifying challenges of support and how to manage them in the PD context can inform family-centered interventions for PWPs and partners and help health care professionals assist couples coping with this disease. The following research question was posed:
What costs and complications of social support are experienced between PWPs and partners, and how can such challenges be effectively managed?
Methods
Participant recruitment and data collection
This study relied on in-depth qualitative interviews, which can provide rich insight into people's perspectives, 42 to investigate social support within couples coping with PD. Data for this manuscript are drawn from two related datasets based on a total of 63 participants, including 31 PWPs and 32 partners. (For a summary of participant characteristics, please see Table 1.) Most recently, 19 participants were recruited and interviewed (via Zoom) in late 2021 and early 2022. This dataset builds upon and adds to a prior dataset regarding PD and social support within couples, collected via face-to-face interviews with 44 participants (who were recruited and interviewed in late 2010) as part of a larger project for the author's dissertation (which also included other data, published elsewhere, about different topics related to the experience of PD). b The data regarding social support has not been previously published, and combining data from these two different sets permitted a more detailed and focused study of social support within couples coping with PD. In both datasets, participants were asked the same questions about social support exchanged with their partner, yet the second set of interviews explored this topic more deeply by also including additional “focused questions to learn about [existing] categories” (as recommended by Charmaz regarding theoretical sampling). 43 (p200)
Demographic characteristics of participants.
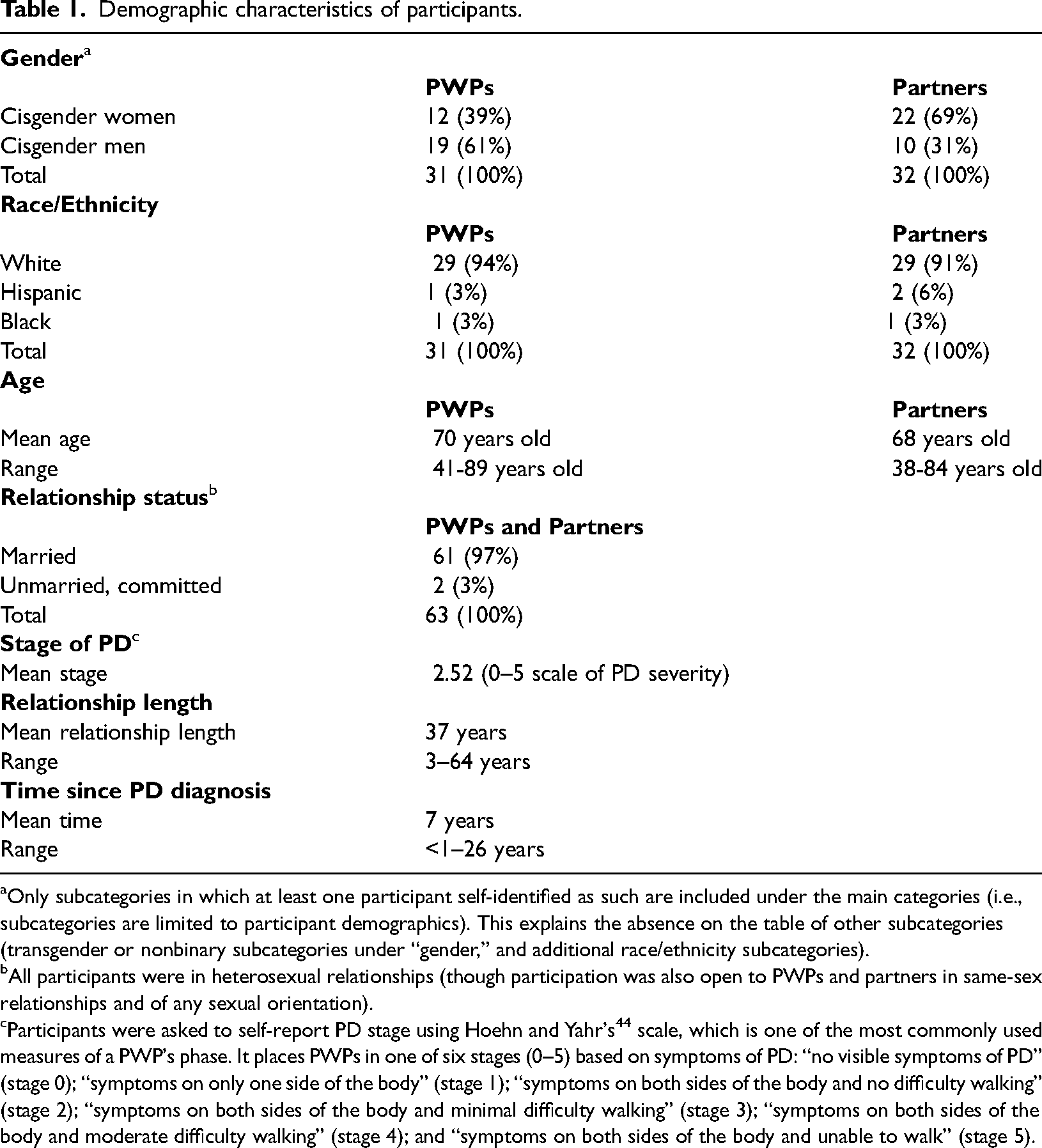
Only subcategories in which at least one participant self-identified as such are included under the main categories (i.e., subcategories are limited to participant demographics). This explains the absence on the table of other subcategories (transgender or nonbinary subcategories under “gender,” and additional race/ethnicity subcategories).
All participants were in heterosexual relationships (though participation was also open to PWPs and partners in same-sex relationships and of any sexual orientation).
Participants were asked to self-report PD stage using Hoehn and Yahr's 44 scale, which is one of the most commonly used measures of a PWP's phase. It places PWPs in one of six stages (0–5) based on symptoms of PD: “no visible symptoms of PD” (stage 0); “symptoms on only one side of the body” (stage 1); “symptoms on both sides of the body and no difficulty walking” (stage 2); “symptoms on both sides of the body and minimal difficulty walking” (stage 3); “symptoms on both sides of the body and moderate difficulty walking” (stage 4); and “symptoms on both sides of the body and unable to walk” (stage 5).
Approval was received from the Human Subjects Institutional Review Board (IRB) at California State University, Fullerton, and the University of Illinois before each of the two different sets of recruiting/interviewing. Participants were recruited via online and in-person support groups for PWPs and partners. To do so, the author emailed or called coordinators of PD support groups, asking for permission to distribute recruitment flyers. In addition, participants were recruited via online and newspaper advertisements along with snowball sampling. Inclusion criteria required having PD or being the partner of a PWP, and being in a committed, cohabitating relationship with the same partner since at least the time of the PD diagnosis. All participants were provided with either a physical or electronic copy of the consent letter in advance. Prior to each interview, informed consent was obtained. c
Using a semi-structured interview guide that included questions about social support and coping (and, for the dissertation dataset, other questions related to PD that are outside of the scope of this manuscript and reported on elsewhere), in-depth interviews were conducted. Although both members of a couple were not required to participate, they opted to in all cases except five (for a total of 29 couples plus 2 individual PWPs and 3 individual partners). Interviews were conducted individually, d with the exception of seven interviews in which participants preferred to be interviewed with their partner, and lasted approximately 45 to 150 min each. The majority of the interviews were conducted by the author, though in some cases, another researcher (the author's partner, who also has experience and doctoral training in qualitative methodology) conducted interviews as well so that both members of a couple could be interviewed at the same timeslot for the participants’ convenience. Participants who were interviewed face-to-face were located in the Midwestern region of the United States, and most chose to be interviewed at their home. Other participants were located in various regions throughout the United States. Each individual was offered $25 for participating. Interviews were recorded and transcribed.
Data analysis
Data analysis occurred both during and after data collection using an iterative approach, “in which the researcher alternates between considering existing theories, research interests, or predefined questions/goals . . . with emergent qualitative data.” 42 (p11), see also 45 The data analysis process was primarily conducted by the author, with the other interviewer also coding a subset of the earlier dataset to compare and help ensure trustworthiness of the categories. In cases in which both members of a couple participated, data were first analyzed at the individual participant level and then compared at the dyadic level by assessing each participant's data in light of the corresponding partner's. Although transcripts were initially analyzed in two subgroups based on whether the participant was a PWP or partner, these were later combined because all of the final categories were based on data from both subgroups.
Transcripts were carefully read through many times using constant comparative techniques 46 with the goal of detecting patterns within and across transcripts. Constant comparative methods entail “compar[ing] data with data to find similarities and differences” including “within the same interview and . . . in different interviews.” 43 (p132) During rounds of initial coding, terms were added to the transcripts to identify constructs, which were then compared and grouped together as appropriate to create analytic categories. These categories were constantly reevaluated and revised as a better understanding of the data emerged. Then, in rounds of focused coding, all transcripts were assessed again with these categories, which were evaluated for ways they might be related. This analysis process was conducted with both datasets. To merge the data, codes and categories were compared and combined with each other, further revising them as needed into a final analytic framework, against which all data were again recoded. 43 Lastly, example quotations from participants were chosen to include in the results of this manuscript (using pseudonyms).
Results
Complications and costs of social support
Results of this study demonstrate that supportive attempts can entail challenges.
Participants reported several complications and costs of social support, including partners’ differing approaches to coping can make support difficult, support can be perceived as identity-threatening and controlling, support can lead to dependency, and support can be draining.
Partners’ differing approaches to coping can make support difficult
Many PWPs and partners noted that, at times, support is complicated by the fact that they have a different approach to coping with PD than their spouse. For example, members of a couple might have conflicting preferences related to how often to talk about PD as well as the extent to which they seek or avoid information about the disease. Ed, a 57 year-old partner, explained that he would rather avoid most information about PD because reading the “horror stories” online would interfere with his desire to “not worry about something that might not happen.” This preference, however, clashes with his wife Tina's inclination to learn as much as she can about the disease and share this information with him. The couple's conflicting preferences regarding information present a challenge as described by Tina, age 59: He really didn’t want to read about it, and I’m a “if something's broken, let's fix it or find out about it” person, and he is not that kind of person. . . . He was angry because I was forcing him to learn some information he wasn’t prepared for.
Support can be perceived as identity-threatening and controlling
Another difficulty for both PWPs and partners is that support sometimes has negative implications related to identity and control. Partners may face the challenge of wanting to offer their PWP help, yet struggling to find a way to do so without implying that the PWP cannot complete the task independently. For example, Lydia, a 62 year-old partner, said, “If . . . I'm trying to put him in a more comfortable position or something, he will say, ‘I can do it. I'm not a baby.’” In addition, Warren, a 67 year-old PWP, said that he has become frustrated at times with his wife's behavior at his doctor's appointments: “One time we went to Dr [name omitted], and she was kind of putting words in my mouth, and I was saying, ‘Now wait a minute. Let me talk here.’” Going to medical appointments with the PWP can be a valuable form of social support; however, PWPs may feel undermined if they have the perception that their partner is trying to take control of the appointment. As also noted by Constant et al., 12 partners often face the challenge of attempting to provide support without disrupting the PWP's autonomy.
In the current study, some partners explained that what they intended as supportive reminders to their PWP (e.g., about eating well or exercising) were sometimes negatively interpreted as “nagging,” echoing findings from past research about couples coping with other chronic conditions (e.g., coronary heart disease). 36 Encouragement by social network members to participate in health-promoting activities (and cease health-diminishing ones) may be viewed as health-related social control.48,49 Social control has sometimes been associated with poorer adherence to health-enhancing behaviors, 50 though other research has indicated that some individuals (i.e., older adults) do not seem to view receiving social control negatively. 51 Adding further complexity to this issue is the fact that although social support and social control have typically been examined as separate constructs, they are “closely . . . intertwined” in that “[a] conversation about some life stressor may be interpreted as support, control, or both and more.” 35 (p81)
This interwoven nature of social support and social control is evident, for example, in some PWPs’ and partners’ reports of the partner encouraging the PWP to discontinue certain activities (e.g., driving, woodworking) due to safety concerns resulting from PD symptoms. People tend to be more risk-averse for others than themselves regarding physical safety 52 and, in that vein, several PWPs in the present study felt that their partners inflated the danger stemming from PD related to some activities. For example, 72 year-old PWP Van hurt himself with a power saw more than a decade after being diagnosed with PD, but did not feel it was necessary to discontinue his hobby of woodworking, declaring, “Two accidents in 50 years [of woodworking] isn’t bad.” His wife believed his PD symptoms contributed to the accident and wanted to help him find an alternative hobby, whereas he attributed the cause to his own carelessness and was reluctant at first to give up woodworking (though he did at her prompting). Some research suggests that women tend to be more involved in their spouses’ health than men are, and that men may have a more positive reaction to wives’ social control if they view it as normative. 49 This seems consistent with Van and his wife's case; she is highly involved in his care and, even when reflecting on this challenge of support, he noted that he is aware that “she is just trying to help.”
Support can lead to dependency
Another potential complication of support is that it can lead to dependency for the PWP.
This challenge applies to, and was reported by, both members of the dyad; PWPs may not always want to receive help out of fear of becoming dependent, and partners might not know at times whether assisting their PWP is necessary versus being “enabling.” Joe, a 47 year-old partner, spoke of his belief that his wife has become unnecessarily reliant on his support at times because she is accustomed to his help: “There are a lot of times that I think I’m getting played, like I’m doing [a task] and she's sitting there on the couch. I’m enabling her.” Other participants expressed the concern that, if a partner constantly provides tangible assistance to a PWP, the PWP may become physically incapable of completing certain tasks (which they sometimes referred to as the “use it or lose it” phenomenon). Helen, an 80 year-old partner, said that her husband has become more dependent on her in recent years, both as a result of the disease advancing and him becoming accustomed to her assistance: I’d say in the last two years, probably, [taking care of him] has been harder, because now he's become dependent. . . . He can do [tasks] but it's very slowly. . . . I feel bad because it's hard for him to get up so then . . . I feel guilty if I don’t help him. That's the hard part for me.
Support can be draining
A final cost frequently mentioned by participants is that providing support can be draining. Although this challenge relates primarily to partners (who, according to past research, 29 are less likely than PWPs to be offered support from outside sources), the fact that support can be draining for partners can induce significant concerns for PWPs as well. For example, Rick, a 78 year-old PWP, worried about the stress caregiving has brought his wife: “I really, truly don’t know how much more she can take.” Several participants noted that the COVID-19 pandemic had intensified this challenge. For instance, Meryl, a 66 year-old PWP, discussed being uncomfortable leaving the house due to her concern of being exposed to COVID-19 (particularly because it is difficult for her to wear a mask because of the PD symptom of drooling). As a result, she worries about the strain on her husband, with him being her “only support.” Similarly, several participants explained that COVID-related concerns led to a disruption of in-home professional caregiving, placing more stress on the partner. For example, 74 year-old partner Jackie reported that, although her husband was previously receiving in-home nursing care a couple of times per week, they had to stop those services for over a year during the start of the pandemic: “There were a lot of people . . . getting sick because of caregivers coming [into the home] in the Parkinson's community, so we had to give up help.”
Strategies for effectively managing complications and costs of support
To manage costs and complications of support, both PWPs and partners discussed using strategies of seeking/providing support subtly, taking the other's perspective, and relinquishing control. First, some participants highlighted the value of seeking/providing support subtly. Lisa, a 47 year-old PWP, noted that many of her PD symptoms (e.g., shaking, losing her train of thought mid-sentence) cause her embarrassment when they occur in public, and that her husband can “save the day” by subtly providing assistance: “If I get stuck in a conversation [in front of others], he’ll jump right in and finish it where you don’t even notice what he did.” Second, taking the other's perspective can be helpful in reframing challenges of support for PWPs as well as partners. Tony, a 73 year-old PWP, said that when he begins to feel frustrated by his wife “telling me the same thing over and over again” related to PD in her attempts to support him, he reminds himself that she is trying to help him: “I know she's well-intentioned.” For partners, this strategy sometimes takes the form of remembering that the PWP is having a hard time, which is similar to a finding from prior research in the PD context in which PWPs’ spouses reported coping by viewing their own challenges as secondary. 9
Finally, relinquishing control was a third strategy used by both PWPs and partners to effectively manage costs and complications of support. Ron, a 68 year-old PWP, said he learned to “take it in stride” when his wife offers to perform activities he formerly did. He said, “It's just easier to let her drive. Taking it in stride is [my way of] coping with it.” Furthermore, partners sometimes employ this strategy in order to reduce the possibility of communicating support that is identity-threatening and to avoid imposing social control on their PWPs. Pam, a 51 year-old partner, recalled, “I decided that I wasn’t going to become this nagging wife that says, ‘Did you do your exercises?’ I wanted him to own it.” Similarly, Todd, a 76 year-old partner, explained of his wife with PD, “She's a strong person, and she wants to remain that way—not dependent on anybody. So I let her have her independence. I guess what I’m saying is I don’t help unless she asks me to.” While relinquishing control often entails avoiding providing support that the PWP has not asked for, some partners reported that listening to and following what the PWP does say is also crucial. For instance, Tessa, a 70 year-old partner, said of her husband, “He has always been very clear that [his PD medication] is something he wanted to manage. So I really had to just let him manage it.”
Discussion
The current study makes the important contribution of extending our understanding of the complexities of social support within couples coping with PD. Specifically, PWPs and partners described several costs and complications related to the exchange of social support with one another: partners’ differing approaches to coping can make support difficult, support can be perceived as identity-threatening and controlling, support can lead to dependency, and support can be draining. The reality that caregiving within couples facing PD can be draining has also been documented by past research,eg,13,14,17 yet it is worth noting that the COVID-19 pandemic exacerbated this challenge for some PWPs and partners. Consistent with Goldsmith's normative rhetorical theory,18,32 these costs and complications of support sometimes result from the difficulty of balancing multiple goals (i.e., related to task, identity, and relationship) and can lead to dilemmas. For example, as evident in the current study's data, partners might wish to accomplish a task goal of communicating support, but not know how to do so without threatening the PWP's desired identity (e.g., as independent and capable) or being perceived as enacting an undesirable identity themselves (e.g., as controlling), both of which can have negative relational consequences as well. Furthermore, one member of the dyad may wish to share updates about PD with the other but, if their informational preferences are discordant, this might interfere with a relational goal of avoiding conflict. As described in past research, these dilemmas sometimes exist because supportive attempts can have multiple possible meanings (e.g., advice can be viewed as caring or as an unwanted intrusion that threatens the recipient's identity).36,41
An essential part of this study's aim to extend the understanding of complexities of social support within couples coping with PD was to not only delineate costs and complications, but also to illuminate what strategies PWPs and partners consider to be effective in managing these challenges of support. In past research about PWPs, dissatisfaction or problems with social support have been associated with negative outcomes such as distress, depression, and anxiety;eg,24–27 therefore, it seems probable that effectively managing costs and complications of support could have positive implications for mental health. In the current study, participants reported seeking/providing support subtly, taking the other's perspective, and relinquishing control as effective ways of managing costs and complications of support. Considering why and when (i.e., under what circumstances) certain strategies are viewed as effective or helpful is valuable.18,40,41 For example, from a normative rhetorical perspective (i.e., in terms of balancing goals related to task, identity, and relationship),18,32 seeking/providing support subtly is especially important when in a public arena because it can help maintain the PWP's desired identity. In addition, relinquishing control is often effective because it eliminates the relational strain that can stem from a power struggle. In some cases, partners noted that they would relinquish control with most tasks, yet continue to insist on helping with certain activities (e.g., driving) that might otherwise pose a safety threat to the PWP or others.
Clinical implications
Results of the current research can inform interventions and a family-centered model of PD care that attends to mental health as well as physical. It is important for health care providers to be mindful of the ways illness impacts and is affected by the family, 53 and counseling for PWPs or family members may be useful. 1 Health care that focuses on both mental and physical health seems to be especially crucial in light of the COVID-19 pandemic, which worsened the strain of many couples coping with PD (as well as exacerbating uncertainty experienced by PWPs). 7 A pilot study testing the benefits of a self-management program for couples facing PD indicated a promising relational result (i.e., “less concealment of [PWPs’ and partners’] worries/concerns from each other”), pointing to the potential for dyadic interventions for this population. 54 (p887) In additional interventions and care geared toward PWPs and partners, it would be valuable for couples to be educated about social support so that complications and costs of support could be anticipated and normalized, as well as prevented or managed. For instance, PWPs and partners could be encouraged to share with their partner their individual preferences related to support, and discuss or roleplay which management strategies are likely to be effective for them in certain circumstances.
Limitations and directions for future research
Regarding limitations, one factor to consider is that data represent participants’ perceptions. Although gathering in-depth data related to PWPs’ and partners’ perspectives on social support within the couple was the purpose of the study (and, in general, a strength rather than a limitation), members of a couple did not always report the same management strategies in their interviews; thus, it is difficult to know if a partner's perception of a strategy as effective is congruent with the PWP's perception. In addition, the sample was relatively homogeneous (e.g., most participants were White and all were in heterosexual relationships) and, therefore, the results cannot be generalized to all PWPs and partners coping with PD. Another limitation is that the majority of data analysis was done by a single researcher (i.e., the author). Finally, this study did not extensively assess the role of possibly mitigating factors—such as age, gender, relational history, or illness stage—on the communication of social support in couples coping with PD. Future research might further investigate such variables.
Footnotes
Acknowledgements
The author would like to thank Dr Scott D. Martin for assistance with some of the earlier data collection and analysis related to this study. The author presented a poster representing an earlier version of this project at the May 2019 International Congress of Qualitative Inquiry in Urbana, IL. A portion of the manuscript stems from the author's dissertation, though the author has also since collected and included a substantial amount of additional data.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Institutional Review Boards at California State University, Fullerton (protocol #HSR-21-22-99), and the University of Illinois.
Informed consent
Informed consent was obtained from each participant, as described in the “Participant Recruitment and Data Collection” section of the manuscript.
Guarantor
SM