
Abstract
Objective
This qualitative exploratory study aimed to deepen the understanding of selective disclosure among adolescents and young adults (AYAs) living with chronic conditions, particularly in the context of intimate relationships. The project created a space for AYAs to reflect on and share their lived experiences of managing chronic illness and disclosing it to potential partners.
Methods
The study used a participatory design that combined elements of Youth Participatory Action Research (YPAR) with citizen science. Four YPAR partners, young people with lived experience of chronic illness, were actively involved in all stages of the research process, including topic selection, recruitment, development of questions, data collection, analysis, and dissemination. Additionally, 44 AYAs participated as respondents to a longitudinal qualitative survey consisting of 35 open-ended questions that focused on intimacy, challenges, coping mechanisms, and support systems. NVivo 14 was used to code and analyze responses thematically.
Results
Of the 44 AYAs contacted, 27 answered all survey questions. The sample had a high representation of young women with diabetes and LGBTQ + individuals with ADHD and other chronic conditions. Levels of self-acceptance, feelings of empowerment, and previous experiences of disclosure shaped participants’ willingness to disclose their health conditions in intimate situations. Supportive social and relational environments, including open-minded partners and trusted peer networks, encouraged disclosure. In contrast, experiences of stigma, fear of rejection, and concerns about being misunderstood or reduced to their diagnosis acted as barriers. Additionally, the presence of visible medication use or physical symptoms contributed to a sense of vulnerability, further complicating the decision to disclose.
Conclusion
The study sheds light on the nuanced relationship between chronic conditions, self-identity, and intimacy among AYAs. It highlights the importance of creating supportive environments and promoting open communication in both clinical and social settings. By integrating YPAR partners throughout the research process, the study highlights the value of participatory methods in capturing diverse youth perspectives and promoting more empathetic approaches to addressing intimacy related challenges in healthcare contexts.
MESH terms
Chronic Disease / psychology*; Qualitative Research; Truth Disclosure*; Young Adult.
Keywords
Introduction
Adolescence and young adulthood are critical developmental periods characterized by identity formation, growing independence, and the pursuit of intimate relationships. 1 For adolescents and young adults (AYAs) living with chronic illnesses, these transitions are further complicated by the ongoing demands of managing a long-term health condition. Chronic illness during these life stages often disrupts normative trajectories, influencing self-concept, social participation, and future aspirations.2,3 AYAs frequently describe experiences of biographical disruption and, in some cases, biographical retrogression, as illness reshapes their sense of autonomy and belonging.3,4
A growing body of qualitative research highlights the psychosocial challenges AYAs face, including stigma, altered body image, and the negotiation of visibility and concealment in social contexts.5,6 Disclosure of chronic illness, particularly in the context of romantic and intimate relationships, emerges as a central concern. Decisions about whether, when, and how to disclose are deeply personal and shaped by fears of rejection, misunderstanding, and loss of normalcy, as well as practical considerations related to treatment and symptom management.7,8 While some AYAs strive for openness to foster trust and authenticity, others engage in chronic concealment to maintain a sense of control and avoid stigma. 6 These strategies reflect broader tensions between vulnerability and mastery, as young people seek to “rule their condition” rather than be ruled by it. 2
Despite these insights, existing literature often treats disclosure as a static decision rather than a dynamic, relational process embedded in the affective and social worlds of young people. Reviews of qualitative studies underscore the complexity of these experiences but also reveal gaps in understanding how AYAs themselves conceptualize and navigate disclosure in intimate contexts.6,7 Furthermore, most research has been led by researchers, which may limit the depth and relevance of findings for youth populations.
Belongingness Theory (BT) provides a valuable lens for interpreting these dynamics. According to BT, the human need to belong is a fundamental psychological drive that requires frequent positive interactions and enduring relationships characterized by care and concern. 9 Meeting this need is associated with improved psychological outcomes, including enhanced self-esteem, greater life satisfaction, and reduced anxiety and depression.10,11 For AYAs with chronic illnesses, the pursuit of belonging is complicated by illness-related disruptions, physical absence, and stigma. Self-disclosure, particularly of sensitive health information, often demands high levels of trust and emotional safety, which are not always readily available in adolescent social environments. 12 BT emphasizes the role of supportive relationships, whether with peers, family, educators, or healthcare professionals, in buffering the psychological burden of chronic illness and fostering conditions for open communication and mutual understanding. 13 Applying BT thus helps explain how AYAs negotiate intimacy and disclosure while striving to maintain social bonds and a sense of belonging.
To address these gaps, this study employs a participatory research design, engaging AYAs with chronic conditions as co-researchers to explore how they navigate selective disclosure within the context of intimacy, belonging, and health vulnerability. By centering youth perspectives, this approach aims to generate nuanced, actionable insights into the emotional and social factors shaping disclosure decisions and their implications for well-being.
Materials & methods
Study design: Citizen science and youth-led research journey
This study, was grounded in a Citizen Science (CS) methodology, defined as a collaborative research approach in which individuals outside the traditional scientific community, in this case AYAs with chronic conditions and no formal qualitative research training, actively contribute to the research process from its earliest stages.14,15 This inclusive, participatory framework values lived experience and seeks to democratize knowledge production.
The research was inspired by the narrative collection “The Chronic Sick: 25 Stories about Being Young with a Chronic Condition”, 16 which provided insights into the diverse experiences of AYAs living with chronic illness. Building on this inspiration, two senior researchers invited seven of the young authors featured in the book to participate as Youth Participatory Action Research (YPAR) partners, with four agreed of these authors agreeing to join the project. Early meetings were held in a flexible, hybrid format to build trust and ensure meaningful engagement.
In the initial phase, the research team, consisting of the researchers and the four YPAR partners co-developed the central research question: “What is it like to be an adolescent or young adult living with a chronic condition in Denmark today?”. To explore this question, the team collaboratively mapped a broad range of relevant discussion points, resulting in an umbrella of potential themes (see Figure 1). After deliberation, the team decided to focus this project specifically on the pillar of “intimacy and self-disclosure”, recognizing its significance and the need for deeper exploration within the broader context of living with a chronic condition.
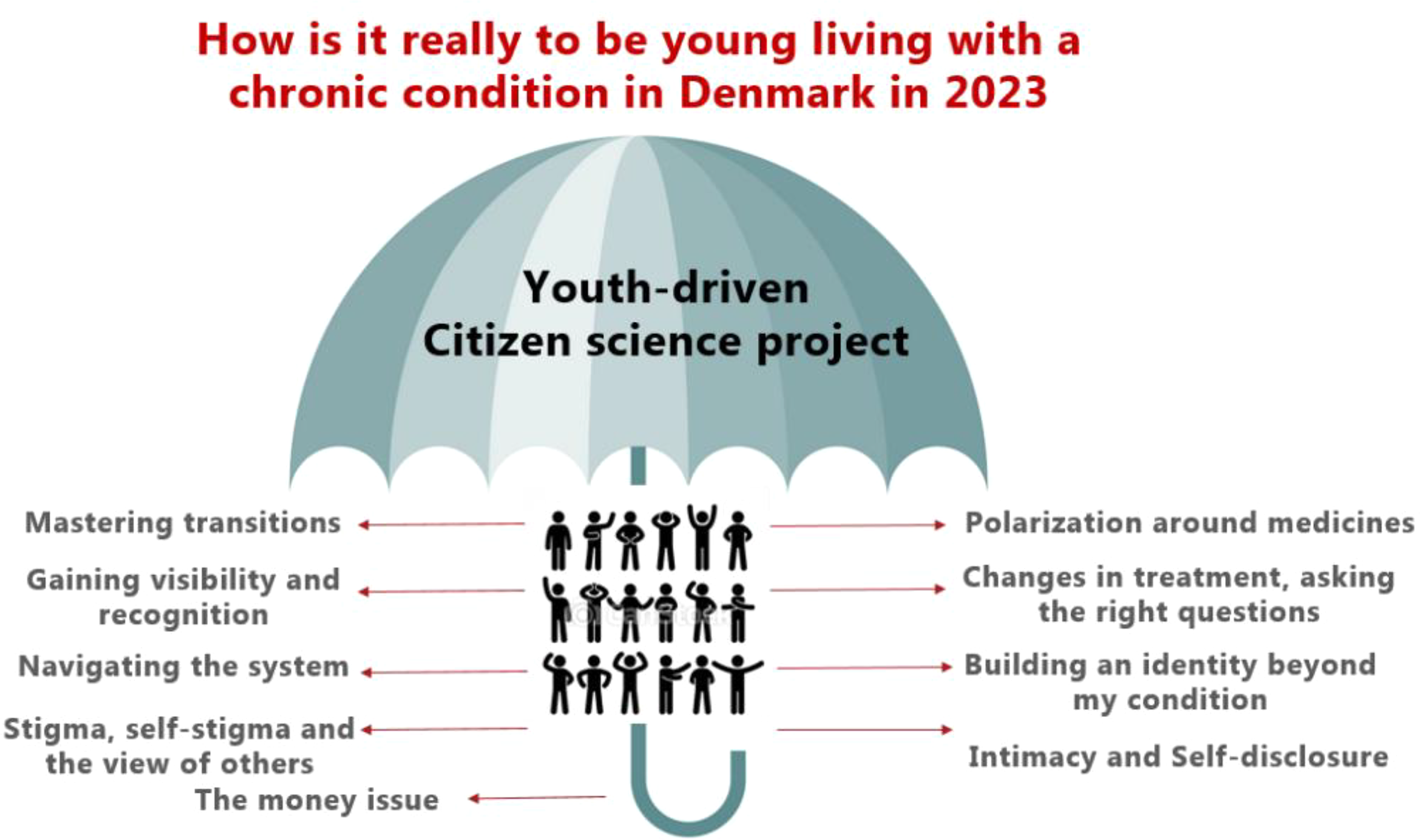
Collaborative theme mapping: youth perspectives on chronic conditions in Denmark.
This collaborative process included a focused literature review and consultations with domain experts, including the principal investigator of the MyVoice project, 17 which informed the creation of a question bank structured around the selected theme. The four YPAR partners played a central role in refining sub-themes and selecting open-ended questions for broader data collection.
Throughout the study, the four YPAR partners – who are themselves AYAs, but distinct from the broader group of AYAs who completed the questionnaire – contributed to all stages of the research process, including recruitment strategies, defining inclusion criteria, survey development, data collection, analysis, and interpretation. Their lived experiences informed the design of survey prompts, the collaborative thematic analysis, and the validation of findings. The YPAR partners were compensated for their involvement. This participatory approach, grounded in citizen science principles, enriched the data and empowered young people to shape both the research agenda and outcomes.14,15
Recruitment
44 AYAs aged 15 to 25 years in Denmark were recruited to capture key developmental transitions from mid-adolescence through young adulthood. This age span was chosen to capture the evolving experiences of intimacy, identity, and health management that characterize these stages. Chronic illness was defined as a self-identified physical or mental health condition lasting longer than six months and requiring ongoing management or having a sustained impact on daily life. 18 Both somatic (e.g., autoimmune or neurological) and non-somatic conditions (e.g., ADHD, depression, anxiety) were included. This breadth was a deliberate methodological choice aimed at identifying shared relational and intimacy-related experiences across diagnoses, rather than condition-specific differences. While the distinction between “somatic” and “non-somatic” conditions reflects a contested mind-body binary, these categories were used pragmatically to reflect participants’ self-reported conditions rather than to imply a strict separation between physical and mental health. Where more specific labels were retained in quotation attributions to support contextual interpretation, while maintaining the study's focus on shared relational and intimacy-related experiences rather than diagnosis-specific comparisons.
Inclusion criteria were age 15–25 years, residence in Denmark, self-identification as living with a chronic illness, and ability to complete weekly written surveys in Danish. Recruitment took place through the personal and social networks of the YPAR partners.
This study was conducted with inspiration from the MyVoice project, a longitudinal digital platform using recurring open-ended surveys to capture adolescents’ and young adults’ lived experiences. 17
Data collection
Data was collected over a 12-week period in autumn 2022 using the online survey tool SurveyXact. Each Monday, the AYA participants received a link to a new set of open-ended questions, accessible on mobile and desktop devices. The weekly, staggered design was used to reduce participant burden and to allow reflections on intimacy and relationships to develop over time. Participants were encouraged but not required to respond each week; partial participation was included in the analysis. Communication was co-signed by researchers and YPAR partners to emphasize shared ownership. Participants were assigned unique identification numbers for secure tracking and compensation.
After four weeks, the study paused briefly for an interim analysis, and highlights were shared in a short video. Final data collection concluded in December 2022. Survey responses were submitted in Danish; selected quotations were translated and reverse translated. Responses typically ranged from a few sentences to several short paragraphs.
Although the broader project focuses on living with chronic illness more generally, this survey module specifically examined sexual, romantic, and intimate relationships. Broader illness-related questions were included in the final week to support holistic reflection. While informed by YPAR principles, participants who answered the survey are not described as citizen scientists; participatory elements were primarily enacted through the sustained involvement of YPAR partners in study design and interpretation.
Data analysis
Thematic analysis was conducted collaboratively by senior researchers and YPAR partners, who brought valuable experiential insight into the interpretation process. YPAR partners received training and ongoing support in qualitative analysis, specifically in applying Braun and Clarke's six-phase thematic analysis framework. 19 Coding was performed in pairs, consisting of one senior researcher and one YPAR partner, working intensively over one week to code and identify key themes using NVivo Software (version 14). Data interpretation employed retroductive reasoning, integrating both inductive and deductive approaches, and was informed by belongingness theory 9 as a conceptual lens. The final phase involved validating the narrative on intimacy and selective disclosure, with continued input from two YPAR partners who remained engaged throughout the data interpretation phase.
Legal and ethical considerations
Since no biological material was involved, ethical approval from Danish health research authorities was not required. All procedures complied with University of Copenhagen policies and the General Data Protection Regulation (GDPR). Responses were securely stored, and YPAR partners signed guest-researcher agreements to access data. Informed consent was obtained from all participants, with clear communication of the study's aims, potential benefits and risks, and the voluntary nature of participation. Participants had the right to withdrawal at any point, and data from those who opted out were deleted. Anonymity and confidentiality were safeguarded through secure storage and the use of pseudonyms. Participants received a modest honorarium (300 DKK) for their involvement.
To minimize psychological discomfort, the team consulted an expert from the MyVoice project 17 to ensure that survey questions were respectful, inclusive, and supportive. Cultural sensitivity was also prioritized, with deliberate inclusion of AYAs representing a spectrum of sexual and gender identities. The project aimed to collect data while empowering participants by aligning activities with their needs and feedback. Preliminary results were shared regularly through email and short videos, promoting transparency and co-ownership.
Results
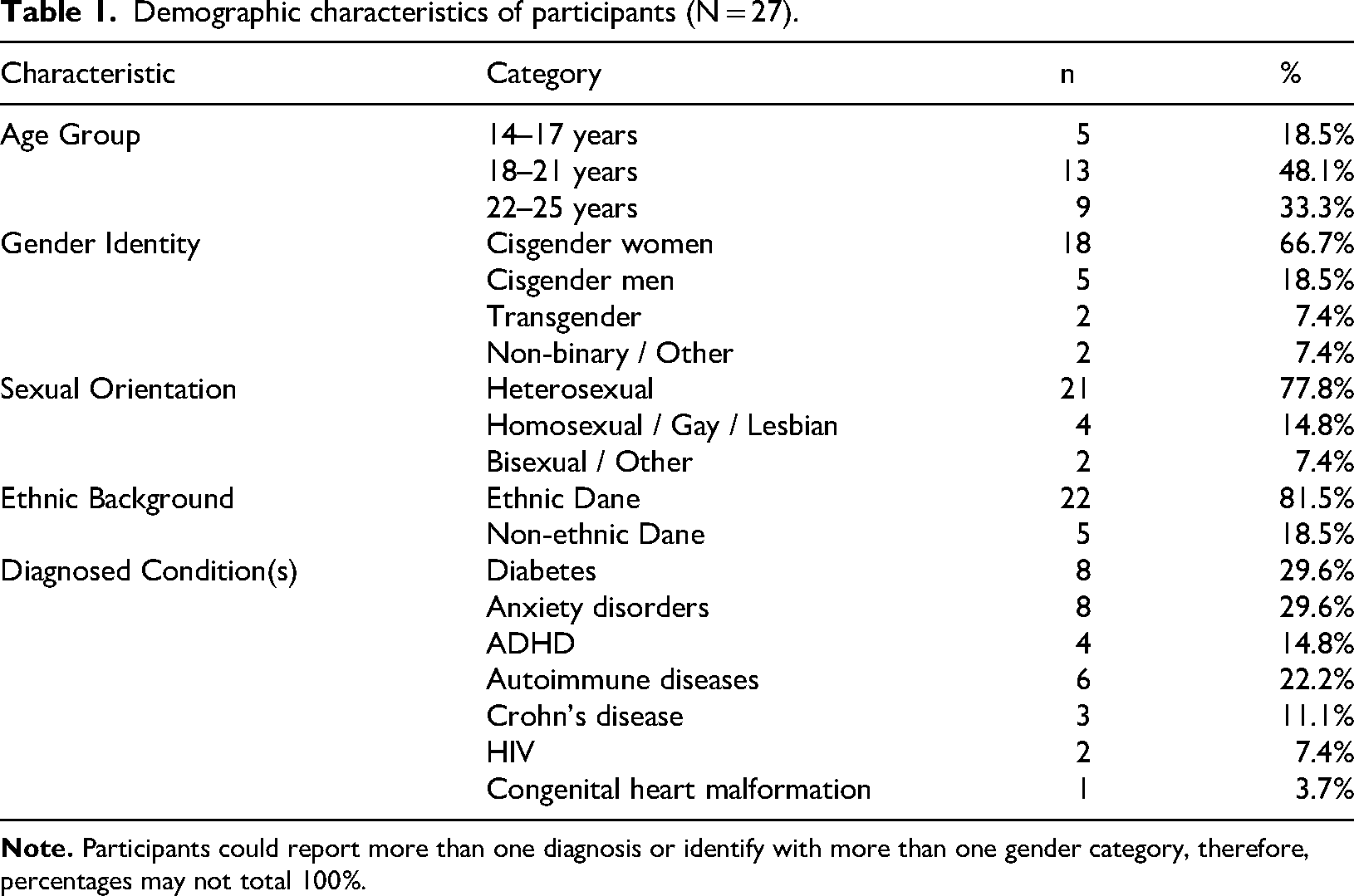
Despite some attrition over time, particularly among younger participants, and a higher representation of young women, the final sample included substantial diversity in age, chronic conditions (both somatic and non-somatic, with labels justified in the methods section), and sexual and gender identities, including a high proportion of LGBTQ + participants (see Table 1).
Demographic characteristics of participants (N = 27).
Thematic analysis (from codes to global themes).
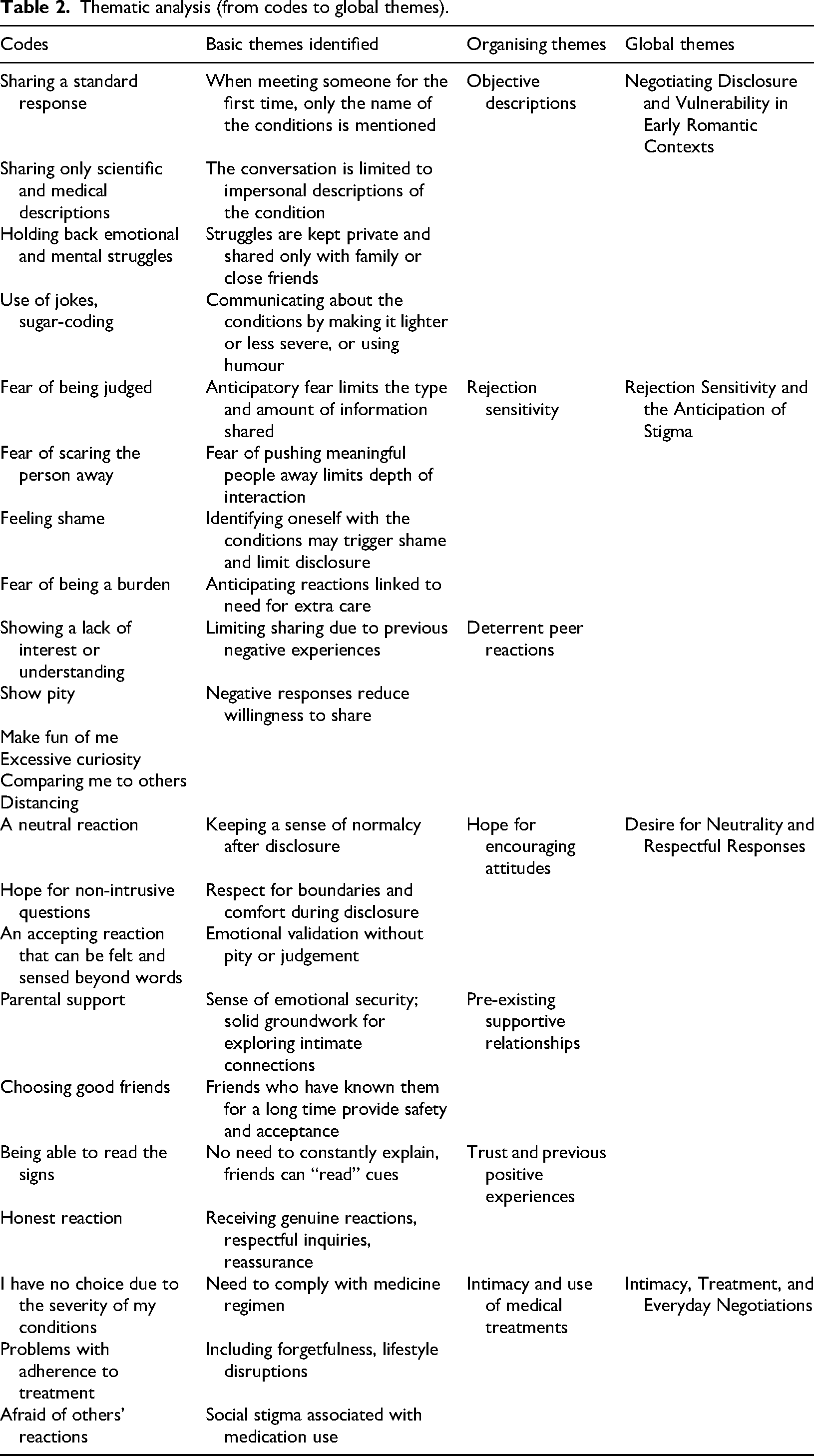
Rather than presenting broad organizing themes (see table 2), the analysis below focuses on four interrelated themes that capture novel insights into how chronic illness shapes romantic and sexual experiences. Unless otherwise specified, participants’ accounts primarily refer to dating new partners or early-stage romantic relationships, with explicit notes where experiences involve long-term partners. To protect anonymity while supporting contextual interpretation, participant characteristics included with quotations are limited to age group and chronic condition.
Theme 1: Negotiating disclosure and vulnerability in early romantic contexts
A central finding was how participants navigated when, how, and to whom to disclose their chronic condition. Disclosure was described as a strategic and gradual process, particularly in early-stage dating, and often involved careful consideration of timing, context, and the perceived receptiveness of the potential partner. Participants frequently began with neutral or factual descriptions of their diagnosis and delayed sharing the emotional or sexual implications of their condition until trust had been established. “I often start by mentioning that my heart is on the opposite side, and all my organs are mirrored. It's a good icebreaker because it opens the door to humor. If it's well-received, I might consider sharing more specific details jokingly.” – P14, early 20 s, somatic condition
This pattern suggests that early, factual disclosure could function as a protective strategy, while greater understanding and acceptance of one's condition enabled more open and confident engagement in intimate relationships.
Participants emphasized that disclosure was easier when they had a grounded understanding of their condition, linking self-awareness with empowerment in relationships. Many participants emphasized not allowing their illness to define them, framing disclosure as just one aspect of identity rather than the entirety of their self-concept: “I’ve learned that my illness does not define me; it's just one aspect of who I am. Even though managing it requires daily medication and frequent doctor visits, it does not overshadow my life. I’m not my illness.” – P5, late teens, autoimmune condition
For some, receiving a diagnosis facilitated acceptance and improved communication in relationships: “Receiving my ADHD diagnosis has given me a language to articulate who I am, making it easier for others to understand me. It's as if it's helped me navigate social interactions more confidently.” – P23, early 20 s, mental health condition
Participants also highlighted the role of role models and peer learning in normalising illness, further demonstrating mechanisms that supported vulnerability and empowerment. “I vividly recall a lecture by a chronically ill adult during my school days; seeing someone like me sharing their experiences was incredibly empowering.” – P12, late teens, somatic condition
Theme 2: Rejection sensitivity and the anticipation of stigma
Fear of rejection strongly shaped participants’ willingness to pursue intimacy. Participants described anticipatory concerns about being judged, pitied, or seen as burdensome, which influenced both early-stage dating and interactions in longer-term relationships. Prior negative experiences heightened these fears, illustrating how past encounters informed present disclosure strategies. “I often hesitate to share because I doubt whether the person will truly accept my explanation. I worry they might view me as lazy or making excuses.” – P3, early 20 s, mental health condition
Distressing past encounters, even with friends or family, reinforced these feelings: “In the past, I attempted to confide in a close friend about my challenges, only to be met with the response that I ‘shouldn’t let my illness dictate my life.’ It was deeply hurtful, particularly because I trusted that person. It underscored that even profound affection does not guarantee comprehension of chronic illness.” – P21, late teens, somatic condition. “Despite efforts by my parents and close friends to empathize, others frequently offer remarks like ‘It could be worse,’ ‘Time heals all,’ or ‘You’ll get better at managing.’ While these sentiments may stem from good intentions, they undermine my experiences and the daily hurdles I face due to my illness.” – P23, early 20 s, somatic condition
Queer participants highlighted the intersection of sexual or gender identity with chronic illness, noting that being part of a minoritized community added layers of concern about disclosure, desirability, and social acceptance: “As a queer person, I already feel different when dating. Adding illness on top of that makes me think even more about when to say something.” – P19, early 20 s, mental health condition
Differences across age and condition type were apparent. Younger participants (15–18 years) described more uncertainty and hesitation in dating, while older participants leveraged past positive experiences to guide disclosure. Participants with non-somatic conditions reported more concerns about disbelief or minimisation of their experiences, though overall strategies for disclosure were similar across somatic and non-somatic conditions. Finally, a small subset of participants described actively decentering romantic or sexual relationships by choice or necessity, framing this as a pragmatic or protective approach rather than a source of distress.
Theme 3: Desire for neutrality and respectful responses
Across accounts, participants expressed a strong preference for neutral and non-pitying reactions when disclosing their condition to potential partners. Acceptance, rather than dramatic reassurance or caretaking, was highly valued, as it allowed them to maintain dignity and a sense of equality in romantic and sexual interactions: “I’m aiming for a neutral reaction. So, there is no pity, outright rejection, excessive interest, or attempts to solve everything. It's scarce when the reaction is just acceptance, treating the situation as a straightforward, neutral aspect of myself.” – P6, early 20 s, neurological condition
Participants emphasised the importance of respecting boundaries while showing curiosity: “I hope that the person listens and possibly asks questions if there is something s/he is thinking about, but respects my boundaries if I say there's something I don’t want to talk about. I hope they listen and understand me, but don’t change their view of me because of it or treat me differently.” – P17, late teens, mental health condition
The subtleties of tone, body language, and empathy were also highlighted: “I don’t open up if I don’t expect a space and openness towards the subject. It doesn’t have to be an immediate understanding, but curiosity about my condition and interest in my experience are important. Additionally, I struggle with people showing me pity. There is a delicate balance between when the pity of others makes me feel incredibly strong and when it makes me feel weak. It cannot be explained in words. The appearance of the person's body language, tone of voice, and eye contact determines this for me.” – P19, early 20 s, mental health condition
Theme 4: Intimacy, treatment, and everyday negotiations
Participants described how chronic illness shaped practical and emotional aspects of intimacy, including medication adherence, fatigue management, and sexual or social planning. These negotiations were particularly relevant in longer-term relationships, where routines and support needs became visible. Here, participants described the interplay among self-care, relationship negotiation, and disclosure patterns, directly supporting claims that move beyond the discussion of empowerment through awareness. “Since I have an illness that requires treatment 24/7, I have no option but to follow the same routine, no matter where I am. Everything else has consequences for my health.” – P24, early 20 s, somatic condition
Challenges included social embarrassment or lifestyle disruptions related to medication: “I should be taking pills every day, in addition to my bimonthly medication at the hospital. However, I don’t take the pills, partly because I generally have a strained relationship with medicine and pills in general, but also because I’m on the go a lot - sleeping out, coming home late, and generally just forgetting about it. It seems like an annoying thing to have to think about. And pack up for trips and go out in front of others as if you are sick or addicted to something, which is a thought I do not like.” – P9, early 20 s, somatic condition
Supportive pre-existing relationships, particularly with family and close friends, enabled participants to navigate intimacy more confidently: “While I deeply value my connections with others, it is primarily with my family that I feel comfortable communicating my need for care, be it related to my condition or not. Having witnessed my journey with my condition since childhood, my parents have become a steadfast source of support. Knowing I can always turn to them for assistance brings me immense comfort and reassurance.” – P6, early 20 s, neurological condition
Positive prior disclosure experiences with partners also facilitated openness: “My current boyfriend demonstrated immense understanding when we discussed the possibility of being together. He took the time to assess whether he could support me adequately, and that level of honesty and care means a lot to me.” – P2, late teens, mental health condition
Together, these themes illustrate how disclosure, intimacy, and illness management were negotiated relationally rather than as fixed individual decisions.
Discussion
This study addresses Venema et al.'s call for increased attention to disclosure practices within romantic relationships, 20 while also responding to the keen interest of our four YPAR partners in exploring the theme of intimacy among peers. Importantly, this study broadened the scope of participants by including a diverse range of health conditions (including non-somatic chronic conditions), sexual orientation, and gender identity and expressions, including gay, trans, and pansexual youth participants. Through this broader lens, we seek to deepen understanding of intimacy dynamics across varied demographic groups.
Our findings highlight several interconnected aspects of disclosure in intimate relationships. Foremost, sharing vulnerability appears more manageable when individuals maintain a grounded and informed relationship with their health condition rather than distancing themselves from it. Participants drew on awareness, acceptance, and self-care as internal resources supporting disclosure, while family and peer support provided external conditions that reduced fear of rejection. At the same time, disclosure functioned as a form of relational risk that participants actively managed in anticipation of other's responses. Past negative encounters and heightened fear of rejection shaped how, when, and to whom participants disclosed, aligning with conceptualisations of rejection sensitivity within the Belonginess Theory. 10 From this perspective, uncertainty or fear of dismissal posed significant hurdles to disclosure, whereas greater understanding and acceptance enabled more open engagement in intimate relationships.
These dynamics were particularly evident in accounts of medication disclosure. While many young individuals described openness about their needs, particularly in intimate contexts, others reported instances of non-disclosure, especially when away from home. Together, these narratives underscore the intricate interplay between internal fortitude, external support systems, past relational experiences, and the perceived importance of medication management in shaping individuals’ readiness to share vulnerabilities within ongoing relationships.
Our findings also illuminate aspects of disclosure that appear specific to intimate relationships, rather than general social or academic settings. While concerns about stigma, pity, or judgment are consistent with broader disclosure research, participants’ accounts highlight that intimate contexts uniquely involve negotiations of trust, attraction, equality, and relational reciprocity. Disclosure in romantic relationships was closely tied to emotional closeness and the desire for mutual understanding and consent, raising the relational stakes compared to disclosures to peers, teachers, or clinicians.
By investigating the experiences of young participants in disclosing, this research sheds light on several key aspects that align with earlier research, as Carter et al. found. 21 At the same time, some AYAs may choose to disclose their illnesses early in a relationship to establish trust and authenticity; there is a stronger tendency to disclose after several months in the relationship, thus delaying disclosure due to fear of rejection or stigmatisation. Kaushansky et al. found similar insights, with young participants expressing a fear of not being physically desired by their partners, being viewed as different, pitied, or seen as a hassle. 22 We also observed this anticipated fear and heightened rejection sensitivity among our participants. We found agreement with Kaushansky et al. in the common reasons for disclosure, perceived trust, and the reasons for withholding, such as fear of rejection and pity. 22
Although this study remains exploratory and does not seek to establish correlations, we observed a distinct connection between self-acceptance and self-care in learning to embrace vulnerability with a grounded, even mature, approach to sharing vulnerability. As was the case in studies by Carter et al., 21 our research supports the significance of being aware of one's condition and using that awareness to inform disclosure strategies, rather than attempting to minimize or detach from the condition. This approach empowers individuals to engage authentically in relationships while managing emotional and practical challenges.
The Belongingness Theory 10 provides a useful framework for interpreting these findings by conceptualising rejection sensitivity, as heightened awareness of potential relational threats. This sensitivity strongly influenced decision-making regarding disclosure, as AYAs carefully weighed relational risk against the desire for intimacy. At the same time, participants’ narratives highlighted resilience and bravery, with disclosure operating not only as a form of vulnerability but also as a pathway to deeper relational connection through trust and mutual understanding.
Finally, limited research has explored the strongly expressed desire for intimacy and its impact on the imperative task of self-managing illness, including medication adherence. This is a pivotal aspect with significant implications for their health. 23 Audulv et al. 24 and Boxer et al. 25 have highlighted the nonverbal communication inherent in AYAs’ engagement in illness self-management. Nevertheless, Zhang et al. 26 concur that this disclosure mode poses challenges, potentially hindering open dialogue and possibly leading AYAs to perceive it as coercive, as the authors termed ‘forced disclosure.’
Clinical practice recommendations proposed by AYAs
By creating a safe and supportive environment for AYAs to discuss their concerns and fears about disclosing, clinicians can foster open communication and actively listen to their experiences without judgment. By validating their emotions and concerns, clinicians can help alleviate some anxiety surrounding disclosure. Clinicians could also provide education and resources to help AYAs make informed decisions about when and how to disclose their illness to a romantic partner. This may include discussing the potential risks and benefits of disclosure, as well as strategies for effectively communicating their needs and boundaries. Our findings additionally suggest that clinicians should consider developmentally tailored approaches, as younger adolescents (14–17 years) may require more structured guidance and skill-building to navigate disclosure, while older youth (18–25 years) may benefit from discussions emphasizing relational negotiation, sexual consent, and autonomy.
Strengths and limitations
There is a widespread consensus today that researching the quality of life and well-being of AYAs should involve them as partners in research. 27 They are viewed as experts in their own lives. When interpreting our findings, it is essential to consider that although all study participants live with chronic conditions, factors such as the type and severity of their condition and their age influence their willingness to disclose. The age range of 14–25 encompasses multiple developmental stages, from mid-adolescence to young adulthood. Younger participants may have less dating experience and may engage with disclosure differently than older participants, which could influence the generalizability of our findings. We observed a higher attrition rate among younger participants, suggesting that some in this age group may find the topic less relevant.
Despite encountering methodological challenges inherent to participatory qualitative research, involving youth in a deeper level of research engagement produced pertinent outcomes that could translate into viable real-life strategies. As our co-researchers expressed in the final evaluation, it bolstered their health literacy and sense of empowerment.
Overall, this study demonstrates that AYAs’ disclosure practices in romantic contexts are shaped by an intricate interplay of self-knowledge, prior experiences, anticipated responses, and relational expectations. The findings highlight the importance of developmentally appropriate support and the distinct dynamics of intimate relationships, extending existing research on chronic illness disclosure beyond general social or academic contexts.
Conclusion
This study examines the intricate landscape of disclosure practices in romantic relationships among AYAs managing chronic health conditions, building on the YPAR partners’ interest in exploring vulnerability among peers. Our research extends existing knowledge by identifying key internal and external factors that influence the sharing of vulnerability, with particular emphasis on the roles of self-acceptance, external support systems, and past experiences. Furthermore, we align with Baumeister and Leary's Belongingness Theory, demonstrating how disclosure acts as a catalyst for intimacy and deepens relationship bonds.
Looking forward, our study highlights the need to incorporate discussions on disclosure into clinical practice. By supporting youth in managing their health conditions with confidence and resilience, clinicians can help enhance relationship satisfaction and overall quality of life. Promoting open communication, validating emotions, and encouraging self-care practices are crucial components of empowering AYAs to navigate their disclosure journey effectively.
Supplemental Material
sj-docx-1-chi-10.1177_17423953261457951 - Supplemental material for Exploring the boundaries: Selective disclosure, intimacy and belongingness among young adults with chronic conditions
Supplemental material, sj-docx-1-chi-10.1177_17423953261457951 for Exploring the boundaries: Selective disclosure, intimacy and belongingness among young adults with chronic conditions by Lourdes Cantarero-Arevalo, Caroline Buhl, Anders Skov Nielsen, Lysander Slyngborg, Nanna Smistrup, Liv M. Kastrup and Lotte Stig Nørgaard in Chronic Illness
Footnotes
Author contributions
Lourdes Cantarero-Arevalo (LCA), Caroline Buhl (CB), Anders Skov Nielsen (ASN), Lysander Slyngborg (LS), Nanna Smistrup (NS), Liv M. Kastrup (LMK), and Lotte Stig Nørgaard (LSN) contributed to the study design, research, and data analysis. LCA authored the manuscript, while CB, ASN, LS, NS, LMK, and LSN provided critical revisions of the manuscript. Acknowledgements: We would like to express our sincere gratitude to Dr. Melissa DeJonckheere and Dr. Tammy Chang from the University of Michigan for their invaluable advice and support in this work. Dr. Chang, the founder and principal investigator of the MyVoice project, and Dr. DeJonckheere, a leading researcher in the initiative, have both provided critical insights that strengthened our study. We are also deeply thankful to all the citizen scientists who participated in the project and generously shared their opinions, perspectives, and lived experiences. Their contributions were essential to the development and depth of this research.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the University of Copenhagen's Ethics Committee.
Informed Consent
Informed consent was obtained from all participants. The young citizen scientists and adult citizen scientists provided signed consent forms. For the 14-year-old participant, informed consent was signed by the participant's mother.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Guarantor
LCA
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.