
Abstract
Introduction
The COVID-19 pandemic confronted healthcare organizations worldwide with unprecedented operational and relational challenges. In such high-pressure contexts, middle managers occupy a pivotal yet often underexplored position (Mackay et al., 2022). They navigate between the strategic priorities of senior executives and the everyday realities of frontline staff, while sustaining trust, collaboration, and resilience under crisis conditions (Kempster and Gregory, 2015; Mintzberg, 1989). This ‘middle-levelness’ (Gjerde and Alvesson, 2019) demands a continuous balancing of formal authority, informal influence, and the relational work required to align divergent expectations.
Despite the acknowledged importance of this role, much leadership research continues to frame middle managers as discrete actors (Oldenhof et al., 2016b). In this literature individual skills and competencies are emphasized over the complex relational processes that underpin their effectiveness (Carroll et al., 2008; Garretsen et al., 2022; Harding et al., 2014; Hartviksen et al., 2019; Tengblad and Vie, 2012). Yet, as Sluss et al. (2011) argue, ‘a role is not lived or maintained ‘solo’ but relies on the relational incumbents to give it meaning and substance’ (p. 508). This observation resonates strongly in crisis situations, where role attribution - the ways in which others ascribe leadership to specific practices or actors - can be a decisive relational mechanism (Meschitti, 2018). However, such processes remain underdeveloped in relational leadership scholarship (Crevani, 2015; Uhl-Bien, 2006).
Relational leadership theory (Uhl-Bien, 2006) conceptualizes leadership as a social, processual phenomenon - emerging through interactions, mutual influence, and shared sensemaking - rather than as a property of individuals. In contrast, role attribution theory (Anglin et al., 2022) often treats attributions as cognitive evaluations of individuals’ behaviour. Therefore, in our study we examine role attribution not as a separate framework but as a relational process within relational leadership, particularly salient during crisis. This integration responds to calls for research that foregrounds leadership as enacted in and through relational practices (Ladkin, 2020; McCauley and Palus, 2021; Uhl-Bien and Ospina, 2012) and examines how such practices are shaped by - and shape - contextual pressures (Cunliffe and Eriksen, 2011; Ospina et al., 2020; Raelin, 2016), such as crises (Riggio and Newstead, 2023; Wu et al., 2021).
Our study addresses this gap by examining how middle managers in a Dutch academic hospital enacted leadership during the acute phase of the COVID-19 crisis, and how these practices were recognized - or rendered invisible - through the relational process of role attribution. Drawing on at-home ethnography, semi-structured interviews, and group discussions, we illuminate leadership as an emergent, situated process rooted in everyday relational work. Our central question in this paper is therefore: how is leadership enacted through relational practices such as role attribution during crisis situations?
Background
Relational leadership: A processual perspective
Relational leadership focuses on social interactions and the co-construction of meaning through collaboration (Uhl-Bien, 2006). Within the relational leadership literature, scholars distinguish between post-positivist and social constructionist approaches (Fairhurst and Connaughton, 2014; Fulop and Mark, 2013). The former emphasizes individual agency, treating actors as ‘independent, discrete entities’ (Uhl-Bien, 2006, p. 655). In contrast, the processual, social constructionist perspective, advocated by Uhl-Bien (2006), is grounded in the principle of ‘processes, not persons’ (p. 655). Herewith, viewing individuals, leadership, and other relational realities as dynamically interconnected through ongoing interaction.
Relational leadership, when conceptualized in this way, aligns with plural and collective forms of leadership such as distributed, shared, and leadership-as-practice (Denis et al., 2012; Fulop and Mark, 2013; Kempster and Gregory, 2015; Ospina et al., 2020; Raelin, 2016). This perspective shifts analytical attention toward how individuals collectively act, create order, and enact change, shaping and being shaped by their contexts (Cunliffe and Eriksen, 2011; Hosking, 1988; Spyridonidis et al., 2022). Leadership is thus understood as an ‘iterative and messy social process shaped by interactions with others’ (Sayles, 1964, cited in Uhl-Bien, 2006, p. 664). This view is particularly useful for examining how middle managers make sense of leadership during crises and how such leadership is recognized, or obscured, through the actions and attributions of others (Smircich and Morgan, 1982).
Exploring role attribution as a relational process
While relational leadership theory emphasizes interaction and shared meaning, role attribution theory examines how leadership is ascribed to individuals or practices based on expectations, perceptions, and contextual cues (Anglin et al., 2022; Biddle, 1986). Roles are shaped both by how others expect them to be enacted and by how individuals perceive and perform them. Sluss et al. (2011) extend this understanding by conceptualizing roles as co-constructed through ongoing social interaction, making them fluid and context dependent.
In crisis situations, role attribution becomes especially salient and dynamic (Wu et al., 2021). Middle managers may face shifting responsibilities and expectations as organizational priorities evolve rapidly (Tarakci et al., 2023). Gjerde and Alvesson (2019) highlight the necessity for middle managers to navigate across multiple organizational layers, balancing hierarchical directives with collaborative engagement. This fluidity requires quick adaptation to emerging conditions and the ability to manage complex relational dynamics (van Schothorst-van Roekel et al., 2020). We therefore study role attribution not as a separate theoretical frame, but as one relational process of many relational processes within relational leadership, central to understanding how certain actions come to be recognized as leadership in crisis settings.
Middle managers in hospitals in crisis
Hospital middle management is inherently complex (Oldenhof et al., 2016b), situated at the intersection of strategic decision-making and operational execution. Positioning theory offers a useful lens for understanding how middle managers position themselves and others in social interaction, thereby influencing the collective enactment of leadership (Meschitti, 2018). This positioning affects not only how they carry out their work but also how their leadership contributions are perceived and valued.
Traditional perspectives on managerial work emphasize planning, organizing, leading, and controlling, while more recent approaches highlight its dynamic, situated, and relational nature (Azambuja et al., 2022; Korica et al., 2017; Mintzberg, 1994; Tengblad, 2006; Tengblad and Vie, 2012). In hospitals, these dynamics are intensified by multi-professional collaboration, high-stakes decision-making, and the need to balance formal authority with professional autonomy (Noordegraaf, 2020). Crisis conditions magnify these tensions (Weick, 1988), accelerating change and creating heightened uncertainty (Mabey and Morrell, 2011; Western and McDonnell, 2022).
Crisis leadership research typically focuses on how leaders analyze, make sense of, and respond to crises, what Harrison (2025) terms ‘leadership through crisis’ (p. 1). This perspective emphasizes the distinct role leadership plays in navigating organizations through disruptive and high-stakes events (Riggio and Newstead, 2023). In contrast, ‘leadership by crisis’ (Harrison, 2025, p. 1) refers to the construction or manipulation of crisis narratives as a basis for exercising leadership. While the latter is associated with political and rhetorical power plays, our study is concerned with leadership through crisis, conceptualized as a relational, processual phenomenon. From a discursive perspective, crises are intersubjectively constructed through processes of crisis identification, definition, and constitution (Rycker and Don, 2013), which are themselves shaped by power relations and social interactions (Meschitti, 2018). This aligns with our view of relational leadership in crisis as emerging through the situated practices and mutual attributions of multiple organizational actors.
In sum, this theoretical framing positions our study to explore how leadership is enacted through relational practices during crisis situations, and how role attribution operates as one of these relational processes herein.
Methods
Design
This paper is based on a qualitative - interpretive study (Schwartz-Shea and Yanow, 2012) into the work of business managers in a Dutch academic medical center (AMC) during COVID pandemic. We used at-home ethnography (Alvesson, 2003, 2009), in-depth interviewing (Langley and Meziani, 2020), elicitation techniques (Barton, 2015) and member check focus groups (Birt et al., 2016), in 2020 and 2023, to understand how business managers in an AMC construct their work in times of crisis and what leadership means to them in that context of crisis.
Early ethnographic observations from the first and third author informed the design and focus of subsequent interviews, while emergent insights from interviews were used to refine ongoing field observations and prompts in the member-check focus groups. This iterative interplay ensured that each method built on, and deepened, the insights from the others.
COVID-pandemic in the Netherlands
In early 2020, the Netherlands faced the COVID-19 pandemic, an exogenous shock with significant impacts on society, organizations, and individuals (Garretsen et al., 2022). The first case was officially reported on February 27, 2020, by a Dutch hospital (2020). Shortly after, the World Health Organization (WHO) declared COVID-19 a global pandemic on March 11, 2020 (WHO, 2020). As March progressed, the crisis intensified, driven by shortages of essential resources like face masks, gloves, specialized nurses, ICU beds, and ventilators (Wallenburg et al., 2021).
This strain was not evenly distributed across the 72 Dutch hospitals; those in southern regions faced overwhelming numbers of critically ill patients. The escalating pressure raised concerns about life-and-death decisions for healthcare professionals, leading to what was termed ‘Code Black’.
The crisis prompted unprecedented efforts to coordinate patient referrals and manage hospital capacities (Wallenburg et al., 2021), fostering new relationships and leadership practices. This study examines how business managers in a Dutch academic medical centre perceived their roles and leadership during this crisis.
Research context and participants
The AMC in our study is one of seven AMCs in the Netherlands, with over 1100 clinical beds, nearly 12,000 employees, and a 1.2-billion-euro turnover in 2020.
AMCs play a vital role in Dutch healthcare, combining complex patient care, biomedical research, and professional training (Cardinaal et al., 2022). These AMCs also serve regional and national functions, particularly during COVID-19, when they coordinated care efforts due to their advanced infrastructure in imaging, care facilities, and laboratories.
The eight business managers in our study had five to twelve years of management experience. They had diverse backgrounds in finance, law, and business management, and ranged in age from mid-thirties to mid-fifties. Four of the managers are men. These managers oversaw non-medical affairs in medical departments, including budget management, process optimization, and clinic supervision. Annual department budgets ranged between 15 and 70 million euros.
Medical departments were organized by specialty (e.g., ENT, Cardiology) and were each headed by a professor who reported directly to the executive board. The business managers acted as the ‘right hand’ to these department heads.
The first author’s role as a business manager during the COVID pandemic provided firsthand access to data collection, despite the limitations of research methods during the pandemic (Kuijper et al., 2022). We addressed the challenges of at-home ethnography and potential bias (Alvesson, 2009; Cunliffe and Karunanayake, 2013) by integrating ethnography with interviews and focus groups.
Data collection
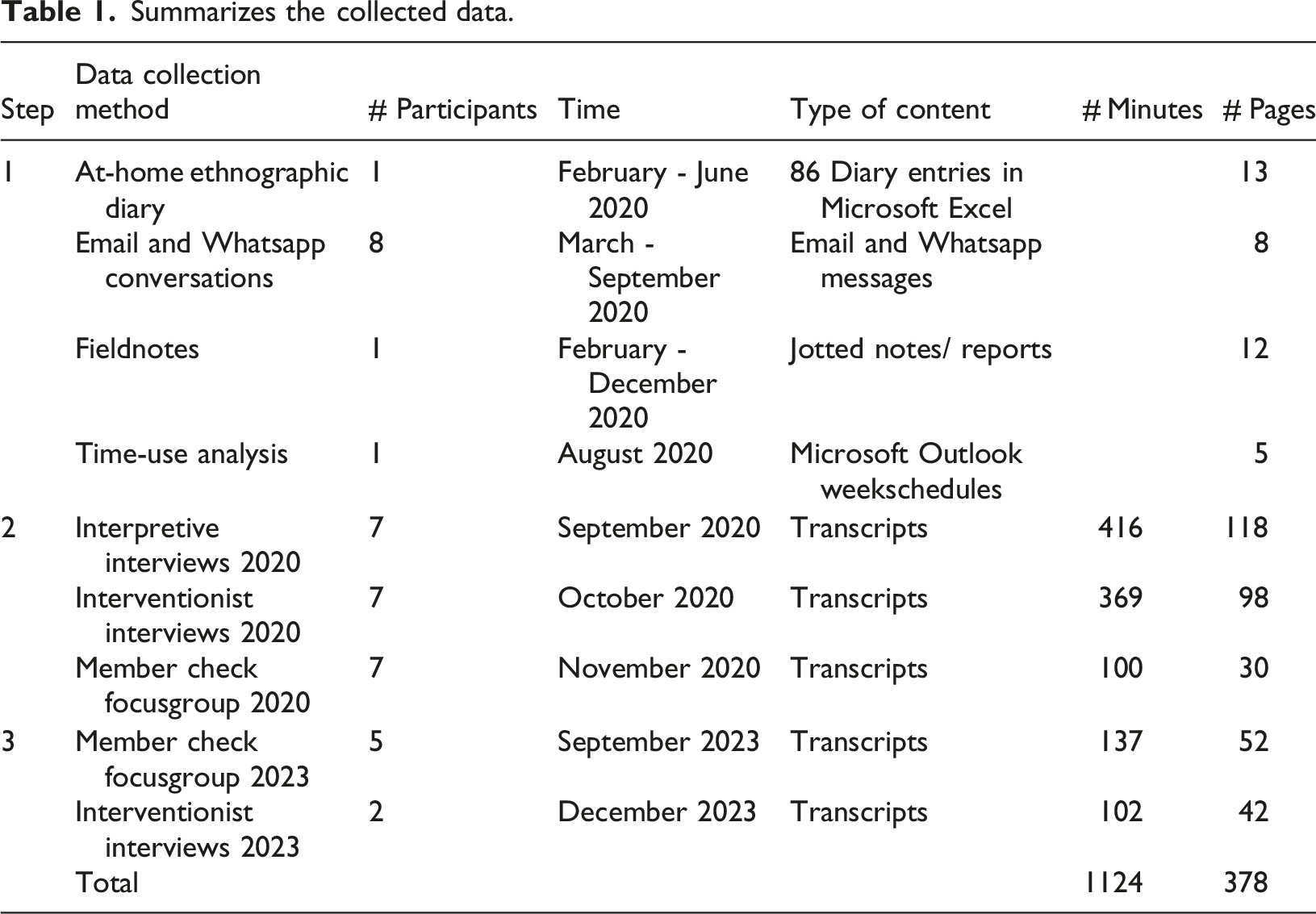
Summarizes the collected data.
At-home ethnography
Ethnography is defined as ‘a way of writing about and analysing social life’ (Watson, 2011, p. 202). For this study, we employed what Alvesson (2009) describes as ‘at-home ethnography’ to explore the practices of business managers in an AMC and the significance of relational leadership (Uhl-Bien, 2006) from a firsthand perspective. The first author, a business manager at the AMC during the COVID-19 pandemic, also pursued a PhD on relational leadership in this specific context. This unique combination allowed him to conduct an ethnographic study while actively working, positioning him as an ‘observing participant’ (Moeran, 2009). Throughout the study, the first author regularly debriefed with the research team, who provided critical distance by challenging assumptions and interpretations, thus reducing the potential bias associated with this kind of insider research.
This approach mitigated common challenges of ethnographic research, such as access and time constraints (Alvesson, 2003), but also increased the risk of ‘going native’ (Gioia and Chittipeddi, 1991, p. 435). Unlike autoethnography, which emphasizes deep personal experiences (Greenhalgh, 2017), at-home ethnography focuses on interpreting actions and communications from a reflective distance (Alvesson, 2009, p. 162). The first author kept a diary to document changes in work tasks and evolving relationships with colleagues, because in ethnography ‘one may be less able to liberate oneself from some taken-for-granted ideas or view things in an open-minded way’ (Alvesson, 2009, p. 166). This diary facilitated reflexive memoing (Deterding and Waters, 2018) and included observations from crisis management meetings, which were compiled into field notes (Bryman, 2012). Reflexive memos were also discussed within the research team to surface taken-for-granted assumptions, and to critically examine how the first author’s dual role as manager and researcher shaped the interpretation of events. For example, the two authors that did not work in the hospital sometimes observed that the first author interpreted certain events more from the perspective of a business manager than from that of a researcher, which opened space for further reflexive dialogue.
Diary keeping, field notes and time-use analysis
At the onset of COVID-19, the first author asked seven business manager colleagues to keep a diary as part of a study on relational leadership. Participants were selected based on gender, department size, and involvement in COVID care. All provided formal consent. An Excel file was created for diary entries, and a WhatsApp group was set up to encourage participation and facilitate discussions. The first author also checked in with participants twice weekly.
After two weeks, it became clear that maintaining diaries was too burdensome due to increased work pressures. Data collection methods were then adapted, focusing on reflective discussions in the WhatsApp group, observations of online meetings, and email reflections from March to May 2020.
We collected the first author’s 15-page ethnographic diary (Alvesson, 2009), 15 diary entries from participants, 8 pages of WhatsApp and email discussions with three participants regarding their day-to-day activities and thoughts, 12 pages of fieldnotes from work meetings, and a 5-page time-use analysis from the first author’s Outlook schedule. Time-use analysis, which reveals how time is allocated and its significance (Feldman et al., 2020), was used to compare business managers' activities pre-COVID and during the pandemic.
Interviewing
After May 2020 the initial wave of COVID had passed and the collected data were analyzed. This, firstly, led to an interpretive interview (Langley and Meziani, 2020) with each of the seven business managers. The aim of this interview was to uncover and identify leadership experiences and meaning given to these experiences by the business managers in their practice before and during COVID. Secondly, the first author interviewed all business managers a second time from an interventionist perspective (Langley and Meziani, 2020). This second interview round was focused on reflexively going through daily practices of the business managers. In these interviews quotes from relational leadership literature were used to elicit (Barton, 2015) reflexivity of the interviewee on her/his experience from a relational leadership perspective. See Appendix 1 for topic guides of both types of interviews. All fourteen interviews were audio recorded and transcribed verbatim.
Focus group interviews
Following the analysis of the fourteen interviews and the at-home ethnographic accounts, a focus group was held in November 2020 to validate the findings (Birt et al., 2016) and explore key topics further. These included the importance of relationships, decision-making during crises, organizational structure, and the social positioning of business managers in crises. An independent chair led the session, while the first author observed and took notes (Bryman, 2012), which were later discussed with the chair. The session was recorded, transcribed, and analysed.
In October 2023, we conducted a second focus group to examine whether perspectives on the managers' roles during crises had evolved since 2020. Due to scheduling conflicts, five participants joined the focus group, and the remaining two were interviewed separately. The same topics from the 2020 focus group were revisited, with the addition of ‘the influence of hierarchy’ and ‘the relevance of power distance’ on the business managers’ work. These topics had emerged from the initial analysis of the data gathered in 2020.
Both the 2020 and 2023 discussions helped clarify the evolving dynamics of relational leadership during crises. The topic guides for the focus group meetings are provided in Appendix 2 for reference.
Data analysis
The data collection and data analysis were intertwined throughout the study (Gjerde and Alvesson, 2019; Nicolini and Korica, 2021), consistent with our qualitative – interpretive methodological stance (Schwartz-Shea and Yanow, 2012). Rather than applying a linear coding framework, we adopted a recursive cycle of reading, memoing, and thematic clustering, moving between the entire dataset and specific incidents to identify patterns and relational dynamics relevant to our research focus.
Our choice of methods such as diary keeping, observational – participation (Moeran, 2009), interviewing (Langley and Meziani, 2020), and at-home ethnography (Alvesson, 2009) asked for continuous analysis of the meaning of the data in the ‘local and situated’ in relation to the aim of the study. Our analysis is therefore what Locke et al. (2015) call ‘an open-ended, forward-looking, trial-and-error’ (p. 372) process between systematic analysis and iterative discovery.
To deepen the empirical analysis, we analyzed the data abductively (Timmermans and Tavory, 2012) by making multiple rounds of iterations between the at-home ethnographic accounts and the interview and focus group data. Part of this process was discussing the findings with the research team. Through this circular process we were able to focus on what stood out in the whole of the data (Gjerde and Alvesson, 2019; Locke et al., 2008, 2015, 2022). By means of reflexive thematic analysis (Braun and Clarke, 2020, 2022) and live coding (Locke et al., 2015) we structured our analysis by drawing on the first author’s firsthand knowledge of the organizational context, complemented by the professional expertise of the other authors in nursing, medicine, and organizational behavior.
We used Atlas.ti to structure our coding and identify themes and patterns (Ospina and Foldy, 2010). We used memos and time stamps in Atlas.ti to code the diary, email, and WhatsApp conversations, as well as the interview and focus group transcripts. Furthermore, in the Summer of 2024 we member checked the findings with the participants prior to writing the final version of the manuscript. This approach adds to the rigor of the analysis process (Deterding and Waters, 2018; Lazard and McAvoy, 2017), is consistent with at-home ethnographic methodology (Alvesson, 2003, 2009) and this process fueled the discussion in the research team on positionality and reflexivity of the first author (Nicolini and Korica, 2024). Additional rigor was ensured through confrontation between data sources, prolonged engagement in the field, and iterative member checks at multiple stages of the research process.
In sum, our approach combined the strengths of prolonged insider engagement with systematic reflexive practices and team-based critical dialogue. In line with our qualitative–interpretive methodology (Schwartz-Shea and Yanow, 2012), we iteratively moved between data sources, revisited interpretations over time, and incorporated participant feedback at multiple stages to generate a contextually grounded and theoretically informed account of relational leadership in crisis. This reflexive, interpretive stance ensured that our findings are not only empirically rich, but also analytically robust and transparent.
Findings
In our study, business managers initially described leadership using terms drawn from general leadership literature, emphasizing skills, traits, and competencies. They referred to visionary leaders and symbolic figures such as Nelson Mandela, while also interpreting management tasks like budgeting and planning as elements of leadership. However, as our longitudinal study unfolded - moving from interviews during the acute crisis in 2020, to focus groups and interviews in 2023 - their language shifted. Leadership was no longer described primarily in terms of competencies or charismatic figures, but rather as a relational and processual phenomenon enacted in practice. They spoke of being physically and emotionally present, protecting their teams from cascading demands, and maintaining fragile connections across organizational layers under pressure. These reflections prompted us to examine how their roles were constructed and attributed within the specific context of crisis.
Our ethnographic and interview data reveal that the crisis did not radically alter the work of business managers, but it amplified and exposed underlying dynamics already present in their roles. Their position was inherently fluid, shaped by contextual demands and relational expectations. While COVID-19 heightened the stakes and speed of decisions, the central challenge was in how their roles were attributed meaning by others - colleagues, team members, and supervisors - who often positioned them as connectors, interpreters, and protectors. In this sense, the crisis illuminated the relational leadership practices that business managers perform, and how these practices became visible and consequential through role attribution.
Drawing on both at-home ethnographic accounts and interview data, we identify three interrelated themes: (1) crisis as a relational amplifier, (2) enacting relational support through listening, shielding, and being present, and (3) decision-making and connecting networks as relational practices. Each theme integrates multiple data sources to illustrate how leadership recognition emerged from ongoing interactions, and how the visibility or invisibility of leadership was co-constructed in practice. Together they demonstrate how relational leadership in crisis is enacted through role attribution in daily practice.
Crisis as a relational amplifier
During the crisis, business managers consistently described their experiences as one of amplification. The pressures, ambiguities, and gaps that had always been part of their role suddenly became more visible and acute. In a 2020 focus group, participants emphasized that “everything was magnified,” from communication failures to interpersonal tensions. Manager 5: “I think that the crisis has magnified everything. So, I believe that where we previously had minor disconnections, such a crisis makes it painfully obvious that connections are missing.” Manager 6: “Yes, I think you must be very conscious of it because the entire playing field has changed. All the normal lines of communication suddenly disappeared, and you must actively organize new ones.” (Patch from focus group meeting 2020)
These accounts reveal how role attribution became highly visible under pressure. Managers were suddenly looked to as the ones responsible for repairing broken lines of communication, even though these gaps predated the crisis. The sense of expectation placed upon them underscores the relational nature of leadership: their authority did not derive from formal mandate alone, but from colleagues attributing responsibility to them in moments of uncertainty.
The ethnographic diaries from the business managers confirm that the pace of work became more fluid and hyper-focused in March 2020. Manager 4 described in a diary entry that work and organizing “became fluid.” At the same time, access to information became central to how managers were positioned as leaders. Even when information was scarce, incomplete, or rapidly changing, managers were often treated as if they “knew what to do.” This perception, as some reflected, also enabled others to sidestep responsibility by deferring upwards to managers. Thus, the very ambiguity of managers’ roles was magnified and turned into a relational attribution of expertise.
As time progressed, the return of “business as usual” responsibilities clashed with ongoing crisis demands. Manager 2 reflected: “(…) in the onset of crisis, a lot of 'business as usual' things disappeared for months. Suddenly they were not important at all, no longer a priority. And when the new crisis team came, it came back in full force. And then you're just sitting there again. Well, I found that quite a difficult experience. Uh, period. Because you were still half in the crisis with all kinds of things. And then you must get to work on everything that was left behind.”
This quote illustrates the dual demands of role attribution. In the acute phase, managers were seen as crisis leaders, expected to filter information and provide stability. But as central command structures shifted back, they were re-attributed as routine managers responsible for catching up on everything that had been deferred. The tension between these two attributions points to the fluidity of their leadership roles in practice.
The first authors’ at-home ethnographic records support this account, though with some nuance. Analysis of his agenda showed that the number of meetings did not dramatically increase compared to pre-crisis months. What changed was the all-consuming focus of those meetings, their online format, and the intrusion of crisis discussions into evenings and weekends. We also noted how personal experiences coloured these perceptions. One diary entry in March stated: “Tomorrow is my first visit to the hospital in two weeks. I feel I should be more present but at the same time find this remote working effective and beneficial to my family.”
Such reflections highlight the complexity of the magnifying effect: while managers experienced extreme intensity, they also noted unexpected personal benefits, underscoring the multi-layered nature of their lived experience.
In sum, these accounts show how crises act as magnifiers of existing ambiguities and expectations. For business managers, this meant their role was not fundamentally new but refracted through heightened relational demands. Authority was attributed to them as communicators, stabilizers, and coordinators - roles that made visible the relational dimensions of leadership such as being present, listening, and supporting others.
Listening, shielding, and being present
When asked in September 2020 to reflect on their leadership during the first wave of COVID-19, many managers initially referred to charismatic notions of leadership. Yet as conversations deepened, their accounts shifted to the more mundane and practical practices that defined their daily contributions. The following excerpt illustrates this turn: “Because I was also just. Of course, I couldn't do anything at the bedside or in the helicopter. That was of no use to them. But I was always there, so also, I tried to be here, so that if one came back exhausted, at least I was there, and the door was open, and they could briefly tell me what it had been like. (…) that is a very important part, I think, of my position. By the way, my door is always open, but it was to an extreme extent. You know, just dropping all… business as usual, when attention was needed. Of course, you try to do that anyway, but in this case, it was just to an extreme extent, and I felt, yes, sometimes a little powerless. Hey, like: gee, what can I do to help? And if you are present in such a crisis meeting, it is of course very marginal what you can really add. And I found that very difficult, yes.” (Interview Manager4)
This quote demonstrates the tension managers felt: their traditional managerial tasks—budgeting, long-term planning, supervising projects—became less visible, while relational practices such as listening, being available, and showing presence became foregrounded. Importantly, these practices were not self-attributed as “leadership.” Instead, they became recognized as leadership by others, precisely because team members looked to managers for emotional anchoring in moments of crisis.
Several managers described the importance of being present in the hospital despite policies advising non-essential staff to work from home. One referred to this choice as “professional disobedience,” framing presence not as rule-breaking but as a form of relational responsibility. By showing up physically, they signalled solidarity and availability, even when they doubted their own usefulness.
These doubts were common. One manager reflected on the strangeness of his shifting role: “But of course, something really happens to us, right? We pretend that we have not had any problems at all as a person or manager, or that we just carry on. (…) both of my departments, were completely turned upside down. And I was really just an observer, because from the [new crisis management team,] new assignments came every minute, and left, right, doesn't matter. Okay, you know, it took a while before I found my place, like: What can I still contribute to this organization? It really took a while. And then I thought, OK, I'm a bystander, and what can I do? Yes, my people, who were all a bit frantic, like: Where should we go? And: who can we be with? Okay, I thought, that's my role now. But that was strange because it felt like scaling down. Because you are letting things go.” (Interview Manager2) Here, the manager articulated a strong sense of diminished authority, even “scaling down.” Yet precisely through this recognition of limits, his role attribution shifted: that colleagues saw him as a bystander, but his presence and availability gave him value as a stabilizer. In relational terms, leadership emerged through the expectations and needs of others, not through his own claims.
By 2023, managers were able to reflect on these experiences with greater distance. In focus group discussions, they emphasized that seemingly mundane practices – listening, being present, helping, shielding team members from confusing messages – were not secondary but essential. These practices also connected directly to their more rational tasks of budgeting and project management, because maintaining trust and cohesion enabled those tasks to be executed. In their words, relational and functional work were intertwined.
The significance of these relational practices also became visible in how managers experienced organizational hierarchy. One participant reflected: “And he just can't get through some things. But if I send an email: ‘kind regards, [name], manager’, then it will be arranged tomorrow. And I think that's crazy. I mean… So apparently if one person asks, who doesn't have that job, and then the other person asks again, you can get it done. So, hierarchy is indeed there. And well, what I just said, it is also about being taken seriously. So, someone who has that [managers’] position is more likely to be taken seriously than the other…” (Interview Manager3)
This example highlights how leadership was attributed not only through presence and support but also through positional recognition. Even when managers themselves doubted their contribution, the organizational system conferred authority on them by virtue of their title. What they did with this attributed authority – shielding, interpreting, supporting – made their leadership relational rather than purely positional.
One manager further articulated this protective role: “(…) we all try to keep unclear messages away from our people, as much as possible. Choices that are made now, whether it is the nurse from orthopaedics, or something else that must come to us, it certainly has a lot of consequences. And then I think, as a department manager, you monitor that communication. Because it may also come from a different source, but we decided that it can only come via me, and that is how it should be. And I then ask those people: ‘This is what we are going to do! What's it like there [on the ward]? Do you understand the meaning of what we need to do? How can I help?’” (Manager 8, focus group meeting 2020)
Here, relational leadership was enacted by taking ownership of communication flows, shielding teams from confusion, and ensuring clarity. The emphasis is on attribution: team members looked to managers to filter and interpret, even when managers themselves questioned whether that was “leadership.”
In the first authors’ ethnographic diary these accounts echo. In his department, a local crisis management team was formed to implement organizational decisions. Expertise from medical and nursing staff was prioritized, while his management role shifted into a more supportive role – organizing meetings, maintaining connections, and facilitating communication. One diary entry from March 12 illustrates this shift: “This morning, we have decided to close outpatient clinics and scale down surgical programs. The department works like a well-oiled machine, the team leaders take the lead. I don't really have to do much. What is my added value? I created a Whatsapp group for the crisis- [department name] team and scheduled daily online meetings. We will inform each other every day and set out actions. [name of head of department] is the chair. I am asked to make to-do lists and make a lot of phone calls to hear if everyone is okay and can proceed. In particular, [team leader A], takes a leading role with [doctor A] and [doctor B]; They organize the entire clinic and OR. Terrific!”
Like the managers above, he found that leadership was not self-claimed but attributed through relational practices. The most valuable contributions were not necessarily decisive commands but small connective actions that made others feel supported and informed.
The accounts above underscore that leadership in crisis emerged less from heroic acts and more from relational practices that were recognized by others as vital. Managers’ listening, shielding, and supporting work was often not consciously considered by themselves as leadership, yet deeply consequential to their teams. This highlights the relational process of role attribution, where leadership is co-constructed in practice. At the same time, these practices could not exist in isolation. They were interwoven with the need to make decisions and to connect across organizational networks, such as crossing departmental and professional boundaries. In the next theme, we examine how managers enacted leadership through decision-making and network-building, showing how relational practices underpinned their authority to act.
Decision-making and connecting networks
Decision-making is a regular aspect of business managers’ work. Yet during the COVID-19 crisis, both interviews, Whatsapp data, diary entries and focus groups revealed how the urgency of the situation introduced heightened stress and visibility into even routine decisions. Managers found themselves responsible for allocating resources such as desks, chairs, and laptops for remote working, as well as redistributing medical and nursing support for COVID wards. These demands redefined their positioning, requiring them to adapt their roles in ways that were both practical and relational. “(…) in a crisis management attitude, you feel even more decisive, you feel that a more decisive appeal is being made to you or something. And at the same time, you must remain connected, be extra transparent. And those are some of the words that come to mind, like: that is the appeal that I really feel that people are making and the call for clarity, transparency, choices. (…) That is the appeal that I feel very strongly.” (Interview Manager 7)
Here, decisiveness is framed not as an individual trait but as a response to the expectations of others. Role attribution was enacted relationally: colleagues and staff demanded clarity, transparency, and choices, positioning managers as those responsible for embodying decisiveness. The legitimacy of these decisions depended on relational credibility, not formal authority alone.
This relational grounding of decision-making was evident in how managers described the role of trust. “(…) from building trust in the relationship that you have with each other. That trust is created toward you as a leader so that you carefully consider the decisions you make and then you will experience that if a decision comes up that conflict with what is good for the employee, he or she will accept it much more easily. Because he knows that you have integrity, transparency, organizational interests, that you also weigh the employee side and say: ‘Okay, I have thought about everything carefully, but we will go straight ahead.’” (Interview Manager 5)
Managers emphasized that trust-building was not a preliminary step before decision-making but part of an ongoing relational process. Trust was enacted through continuous collaboration, making decisions both acceptable and sustainable.
This dynamic became particularly salient in discussions of networks. In focus groups, managers reflected that their work largely consisted of creating and sustaining connections across organizational units. Manager 6: “I think that our work mainly consists of making connections, making, creating, I think that is very much a part of our work. You work together based on connection, even in the position we are in, it is important to connect with parts of the organization that you do not yet know or that you do not know the employees.” Chair: “And which organizational units are you not yet familiar with? What do you mean?” Manager 6: “Well, I can imagine that we are the ones who should know a little about all the layers and all parts of the organization or at least know that if you don’t have the answer, you can go somewhere for an answer, to fetch the right information. And I notice that this is also very important for employees, for example, that you function as a kind of source of information to take people to other parts of the organization.” Manager 5: “And I also think that knowing the organization, we can always sense undercurrents, et cetera, and you only get that if you are connected to each other and if you are let in.” (Manager 6, focus group 2020)
These reflections reveal that managers conceptualized their influence less in terms of commanding decisions and more in terms of enabling connections. Being perceived as a “source of information” or as someone who can “sense undercurrents” positioned them as so-called relational brokers. Again, role attribution was central: managers’ legitimacy as connectors was granted by others who recognized and depended on these bridging functions.
The ethnographic diary of the first author corroborates this emphasis on networking. While he did not perceive decision-making itself as more intense, he struggled to remain attuned to the department’s needs and to connect with the right people. Crisis structures temporarily disrupted existing contacts, shifting information flows toward frontline professionals. This disrupted managers’ usual gatekeeping role, creating frustrations but also new opportunities to build informal connections. A WhatsApp message he received from a floor manager illustrates this: “Information is lacking. Other departments are also running into this. Can you please check with your colleagues if they have the same problem? If so, we will need to organize something to be better informed.”
In practice, relational leadership meant restoring and sustaining information flows through informal networks. Managers’ authority to decide was inseparable from their ability to connect people and share knowledge across professional and organizational boundaries.
Taken together, these accounts show that decision-making in crisis was not an isolated act of authority, but a relational process grounded in trust and connectivity. Managers were expected to be decisive, but this decisiveness was legitimized through the webs of relationships they cultivated. Our findings show that leadership in crisis was enacted through role attribution and relational practices.
Discussion
This study advances our understanding of relational leadership in crisis by conceptualizing role attribution as a constitutive relational mechanism within such contexts. In doing so, we show that leadership in crisis does not merely rely on competencies or authority but is actively produced through the interplay of enacted practices and others’ recognition of those practices.
In our case, everyday managerial practices such as listening, shielding, making decisions, and connecting gained meaning and visibility through attribution by colleagues and other organizational actors. This shows that leadership in crisis emerges through the constitutive interplay between role enactment and recognition.
Our findings extend the notion of ‘leadership through crisis' (Harrison, 2025, p. 1) by showing that it is not enacted through decisive command but through the relational practices of listening, shielding, and connecting – practices that became consequential precisely because others attributed leadership to them in moments of uncertainty.
In our data, managers frequently described their roles during the crisis using general management and leadership terminology, noting that the crisis intensified existing organizational processes. They identified their role in bridging gaps across organizational layers and addressing information asymmetries, and some were tasked with leading crisis management efforts for their departments or the entire AMC. Role attribution varied depending on opportunities and task divisions, with confidence and influence often stemming from past crisis experience or strong organizational relationships.
Although managers felt their hierarchical positions mattered less during the crisis, these positions still enabled them to influence outcomes effectively. Their access to the board and critical information supported decisive actions, and they observed that the crisis revealed both strengths and weaknesses within the organization, supporting Weick’s(1988) assertion that crises expose underlying dynamics. The ability to make quick decisions and leverage internal networks demonstrated how relational leadership practices are deeply intertwined with managerial roles in high-pressure settings.
Building on these insights, the next sections position our findings within existing leadership theory, showing how the attribution process connects language, practice, and social order.
Leadership as vernacular
The expanding field of leadership studies has made the concept of leadership a common part of workplace vocabulary, a phenomenon that Smircich and Morgan (1982) refer to as ‘vernacular.’ Alvesson and Sveningsson (2003a) note that leadership often arises from daily interactions and discussions among organizational members with specific roles. These actions are recognized as leadership based on the individual’s status rather than the intrinsic value of the activities themselves (Alvesson and Sveningsson, 2003b). Larsson and Lundholm (2010) suggest that we should view leadership as ‘embedded in management rather than distinct from it’ (p. 160). However, like ‘manager-centrism’, there is a risk of ‘leaderism’ (Bresnen et al., 2015), which interprets all activities as leadership and thus reinforces a narrow focus on individual leaders (Alvesson, 2017). This perspective, often criticized for ‘blackboxing’ leadership (Larsson and Alvehus, 2022), overlooks the co-constructed nature of leadership practices. Our findings sharpen this perspective by showing how attribution is central to the vernacular process: when managers frame their work as ‘just doing my job’, colleagues may still attribute leadership to these practices. Attribution, therefore, functions as the bridge between everyday managerial language and the recognition of leadership.
Furthermore, our analysis distinguishes between leadership as enacted in relational practices during the crisis, and leadership as talked about by participants. In this context, relational leadership practices align with Kars-Unluoglu et al. (2022) concept of ‘unleading’, referring to ‘leaderly actions’ that often go unnoticed. For leadership to become part of the vernacular, however, it is essential for all involved parties to recognize and understand these practices. Fairhurst et al. (2020) stress the importance of understanding how leadership becomes relevant in a collective setting to fully grasp how it is enacted in practice. Our study takes this further, showing that relational leadership practices (Uhl-Bien, 2006) derive meaning from daily interactions and the attributions made by others. Leadership emerges through its enactment and the discussions surrounding it, which aligns with Carroll et al. (2008) call to move leadership beyond the ‘competency paradigm’. Thus, attribution as relational process sharpens our understanding of how vernacular leadership talk becomes consequential.
Beyond manager-centrism
Traditional views of leadership and management often emphasize individual managerial actions, focusing on the behaviors, traits, or decisions of leaders. However, our study highlights that understanding the complexities of organizational life requires attention to context, processes, and relational interactions (Cunliffe and Eriksen, 2011; Ybema et al., 2009). Our findings show that managers' everyday activities – such as listening, supporting, and decision-making – are essential to relational leadership (Fulop and Mark, 2013; Larsson and Lundholm, 2010), particularly during crises (Wilson, 2020). Interestingly, managers initially did not recognize these actions as leadership; instead, others attributed leadership to these practices, rendering the managers’ contributions largely invisible. In this way, attribution shifts our attention from leaders’ intentions to the relational dynamics through which their actions are recognized as consequential. This provides a more processual account of relational leadership in crisis.
A related finding concerns what managers termed ‘professional disobedience' – the deliberate choice to be physically present despite institutional guidelines advising otherwise. Rather than individual rule-breaking, our data suggest this is better understood as a relational act: presence signalled commitment and care precisely when formal structures provided little guidance, aligning with what Wallenburg et al. (2019) and Kok et al. (2023) describe as professionals deviating from institutional norms out of relational responsibility rather than personal defiance.
Furthermore, our findings align with interactional perspectives on leadership, emphasizing that leadership emerges through social interactions and is co-constructed by multiple actors (Clifton et al., 2020). This emphasizes the importance of relational processes, where leadership is continuously shaped and negotiated within the social context. By foregrounding attribution, we show how leadership recognition is distributed and relational, hence, not manager centric. This shift from a manager-centric view to a relational and process-oriented understanding of leadership reflects the complexities of organizational life and the multifaceted nature of leadership as it is practiced and perceived in real time.
Social order through role and position
The roles and positions of business managers help establish a social order that maintains organizational structure and supports decision-making, even during crises (DiBenigno, 2019; Oldenhof et al., 2016a). In this study we found that during the crisis period, relational processes intensified, showing that managers must continuously adapt and negotiate their roles (Sluss et al., 2011). Traditional role theory, however, often overlooks these relational aspects (Anglin et al., 2022).
In our data, role attribution operated as a relational mechanism within crisis leadership: colleagues’ expectations and recognitions shaped what managers could do, how they positioned themselves, and how they were able to mobilize resources. Our findings reveal that role attribution is not just an individual or cognitive process but also relational, shaped by interactions and shared responsibilities between managers and their teams (Sluss et al., 2011). These interactions create a mutual understanding of roles, enabling managers to execute their duties, take on influential positions, and manage communication flows, particularly during crises. This underscores the importance of relational leadership practices, which are deeply embedded in the managerial work of our business managers (Korica et al., 2017; Larsson and Lundholm, 2010). And advances processual understandings of relational leadership by demonstrating that role attribution is a constitutive mechanism of leadership in crisis.
Therefore, our study shows that crisis amplifies the interdependence between formal role, relational positioning, and enacted practices. Our findings stress the relational nature of role attribution (Anglin et al., 2022; Sluss et al.). Theoretically, this underscores that attribution should be recognized as central to relational leadership rather than peripheral. Practically, it implies that organizations need to invest in trust-building and relational capacity long before crises occur. Future research should, therefore, further explore these relational dynamics and their effect on organizational resilience and effectiveness in healthcare settings. Future research would, benefit from the use of more practice-oriented methods, such as shadowing (Lalleman et al., 2017; Nicolini and Korica, 2024), to further explore the relational nature of role attribution in situ.
Strengths and limitations
This study provides an exploration of relational leadership practices among hospital business managers during a crisis, leveraging interviews, at-home ethnography (Alvesson, 2009), and document analysis. The combination of these methods allowed for a nuanced and humanized (Cunliffe, 2022) examination of role attribution and relational leadership, with abductive reasoning highlighting key relational dynamics. While Korica et al. (2017) point out the limited scope and potential biases of such methodologies, they also emphasize the depth of insight they provide.
Alongside these strengths, three limitations merit discussion. First, the first author’s position within the hospital introduced potential bias, as participants may have felt pressure to align with the researcher’s role or withheld certain information due to ongoing collaborations. Moreover, the iterative and reflexive design may have amplified a relational reading of practice, meaning the patterns described are partly co-constructed through the research process. To mitigate these risks, we triangulated the ethnographic data with interviews (Langley and Meziani, 2020) and WhatsApp and email correspondence, employed an external supervisor during focus groups, and incorporated reflexive memoing (Deterding and Waters, 2018). Research team discussions further enhanced rigor, involving the first author and a supervisor from within the hospital context alongside two supervisors from outside. Second, the data on role attribution derives predominantly from the managers themselves, leaving how they were perceived by others outside the direct empirical scope of this study. Third, findings are presented as collective patterns; individual variation in leadership style and crisis response may be considerable, and future research might productively examine how personal propensities interact with the relational dynamics we describe.
Conclusion
Our study demonstrates that while business managers initially described leadership in terms of skills and competencies, their reflections on their own work during the COVID-19 crisis emphasized relational and processual practices - being present, protecting teams, making decisions, and maintaining connections. These practices illustrate that leadership was enacted and recognized through relational processes of role attribution, rather than individual competencies alone. The crisis did not transform the essence of managerial work but magnified its fluidity and relational character, as managers bridged organizational layers, managed information asymmetries, and balanced crisis and routine tasks. Importantly, their hierarchical positions, although perceived as less relevant, proved a source of influence by granting access to critical information and decision-making arenas. By highlighting how leadership emerges from everyday managerial activities under pressure, this study contributes to a more situated understanding of relational leadership in crisis. For hospital leaders, these findings underscore the importance of supporting relational role processes as a foundation for resilient crisis management.
Supplemental material
Supplemental material - Leadership as relational practice: The interplay of role attribution in a hospital context during COVID-19
Supplemental material for Leadership as relational practice: The interplay of role attribution in a hospital context during COVID-19 by Arjan Verhoeven, Erik Van De Loo, Henri Marres, Pieterbas Lalleman, in Leadership
Supplemental material
Supplemental material - Leadership as relational practice: The interplay of role attribution in a hospital context during COVID-19
Supplemental material for Leadership as relational practice: The interplay of role attribution in a hospital context during COVID-19 by Arjan Verhoeven, Erik Van De Loo, Henri Marres, Pieterbas Lalleman, in Leadership
Footnotes
Acknowledgements
We are deeply grateful to the business managers who participated in our study. They provided invaluable insights, especially at a time of unprecedented crisis.
Ethical considerations
Our study is compliant with local ethical approval guidelines for healthcare governance research in The Netherlands. Furthermore, all participants gave their informed consent before data was collected. This study is compliant with COREQ.
Consent to participate
All participants gave written consent for conducting the study and publishing the findings.
Author contributions
Arjan Verhoeven designed the study. Arjan Verhoeven conducted the interviews and focus group interviews. Arjan Verhoeven, Henri Marres, Erik van de Loo and Pieterbas Lalleman analyzed and interpreted the data. Arjan Verhoeven prepared the manuscript. Pieterbas Lalleman, Henri Marres and Erik van de Loo commented on the manuscript. All authors approved the final version for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.