
Abstract
This article describes a risk audit carried out on the support provided for 36 people with profound learning disabilities who had been resettled from hospital care to supported housing. The risks were those factors identified in the literature as associated with deleterious effects on quality of life. The audit was carried out with a specially designed tool that covered 24 possible risks and involved a support worker familiar with the service user choosing the most appropriate statement regarding each risk. Their judgements were verified by care managers and social needs assessors. Whilst one or more risks were identified for 32 of the 36 service users, the overall result showed relatively low risks for the group as a whole with 62 incidences (7%) from a possible 864, which nevertheless highlighted several areas that needed attention. The results of the audit have led to action plans for the provision and for the individual service users for whom risks were identified.
Background
The deinstitutionalisation of people with intellectual disability has dominated public policy in most developed countries since the 1970s (Braddock et al., 2001). Deinstitutionalisation involves the service user being accommodated in some form of supported housing or residential care in the community rather than being cared for in an institution such as a hospital. Resettlement has now taken place for the majority of service users in the United Kingdom, and this raises questions and stimulates studies regarding whether the anticipated improvement in their quality of life has materialised.
One such study was the evaluation of the resettlement of 36 service users from Orchard Hill Hospital to supported housing and residential care in the community and its impact on their quality of life is described in Sines et al. (2012). They found an overall improvement in quality life over an 18-month-period comparing life in the hospital with life in supported housing or residential care. Quality of life was measured on four occasions with a specially developed audit tool that covered seven domains: Quality and Location of Housing; Care Planning and Governance; Physical Well-Being; Social Interaction and Leisure Activities; Autonomy and Choice; Relationships; and Psychological Well-Being. Improvements were found overall and in each of the domains with some improving more than others. They also sampled the views of support staff and parents whose views reflected, in the main, the improvements detected by the audit. The findings of this study were consistent with those of Bhaumik et al. (2011), who also found an improvement in quality of life indicators following resettlement using the Questionnaire on Quality of Life (QQoL) tool as a measure.
However, the quality of life tool that had been applied in the Orchard Hill study (Sines et al., 2012) had focused on indicators in seven domains representing quality of life, but not specifically on the possible negative effects and hence risks of resettlement and their management. It was possible therefore that the service users might have demonstrated an improved quality of life but nevertheless be at risk in certain respects. The Bhaumik et al. (2011) tool similarly concentrated on positive indicators of quality rather than risk factors.
A review of the literature (Watts et al., 2006) identified both positive and negative results of resettlement from hospital to supported housing in the community. Following this review and the possible risks highlighted, it was decided by the London Borough of Sutton to commission the Social and Health Evaluation Unit to undertake an audit of the resettled service users from Orchard Hill Hospital to supported housing in the community focusing on the possible deleterious effects or risks of the resettlement.
Risk and risk management
Risk and risk management are complex concepts with environmental, physical, social and psychological features. They also involve economic, political and indeed philosophical considerations. There is a literature concerned with the definition, operationalisation and management of risk and risk management and a number of government policy statements. Two distinct but related themes characterise the literature. On the one hand, it is stressed that responsible social and health care involves risk identification and management for the service users. On the other hand, there is an increasing emphasis on the desirability of individual risk taking as a feature of personalisation. There is thus a tension between risk management as a feature of care and fostering individual freedom to take risks as an element in personalisation.
An article from the Social Care Institute for Excellence (2010) on Enabling Risk, Ensuring Safety: Self-Directed Support and Personal Budgets emphasises the importance of individual adults who use social care and support services being able to make their own decisions and to take risks that they deem to be acceptable to lead lives in their ‘own way’. In a similar vein, Close (2009) in an article entitled ‘Safeguarding and personalisation: two sides of the same coin’ noted that ‘individual adults who use social care and support services and/or their carers should be able to make their own decisions and take risks that they deem to be acceptable to lead their lives their way’.
In a comprehensive document – Promoting Quality Care: Good Practice Guidance on the Assessment and Management of Risk in Mental Health and Learning Disability Services – the Department of Health (2010) summarises a range of key policy imperatives underlining the importance of risk and its management. It emphasises that risk assessment and management is a fundamental part of care within a learning disabilities service, the responsibility for which is part of the practice of all service providers.
The issues are clearly encapsulated by Appleby et al. (2006) in a report on an Enquiry into Suicide and Homicide by People With Mental Illness, which was published online in 2006. They stress the importance of regular assessment of risk and that within Learning Disability Services, an integral component of sound, robust and safe care delivery is a consideration of risk, and how that risk is effectively assessed and managed, in whatever context it arises. They call for a human rights approach to be adopted with the involvement of people with disabilities and their carers in the risk process; the inclusion of protective factors to minimise risk and to respect individual wishes; excellent service coordination between agencies, shared and multi-agency collaboration and accountability, and importantly ‘ensuring that risk assessment and management processes utilise positive risk taking strategies, where appropriate’. They caution that over-stating risks and being overly risk-adverse carry human rights implications with the service user and resource implications for services and can also lead to unnecessary exclusion from services and stigmatisation.
In reviewing research evidence, Mitchell and Glendenning (2007) found that studies tended to concentrate on risk in relation to mental capacity, incompetence and positive risk-taking approaches for people with learning disabilities.
We could not find any published studies involving a risk audit tool comparable with the one in this study.
Background to the risk audit
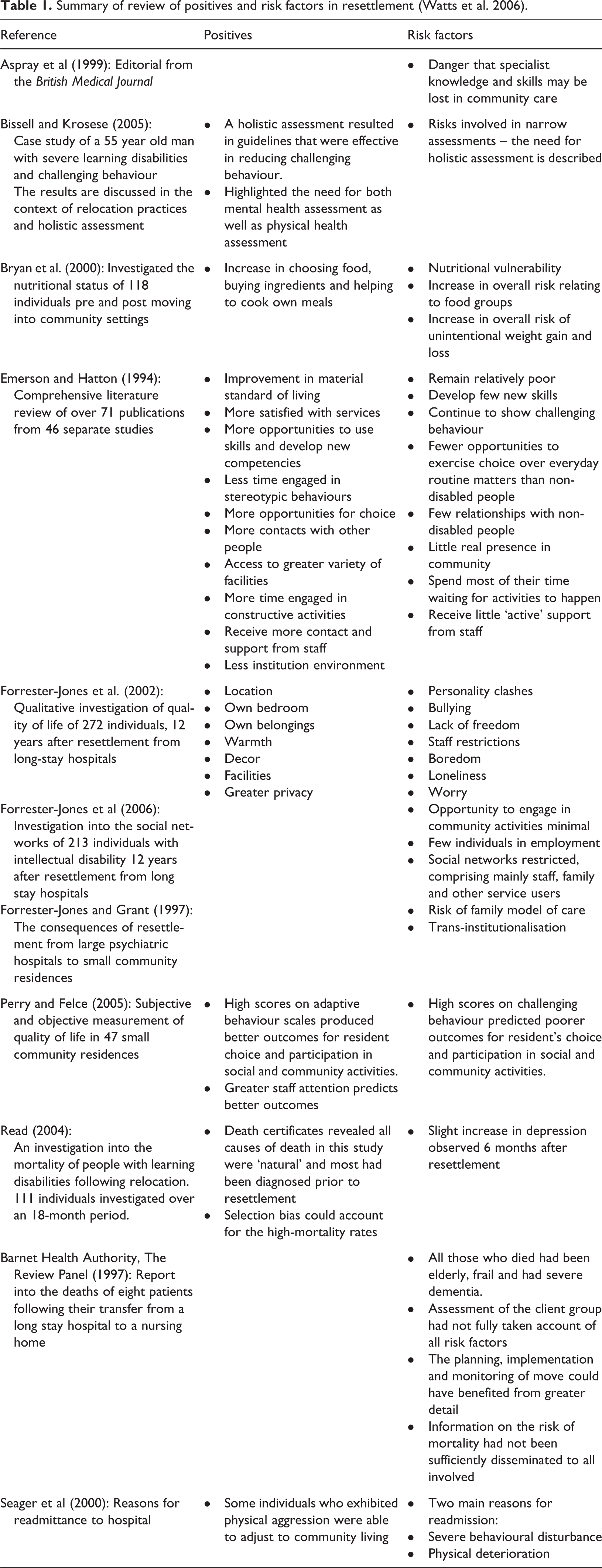
In a review of the advantages and disadvantages of resettlement from hospital to community for those with learning difficulties, Watts et al. (2006) found both benefits and risks. The review addressed two main research questions: what are the benefits of relocating people with learning disabilities from long stay hospitals into community settings and what are the potential risk factors of doing so? While the benefits appeared to outweigh the risks there were, nevertheless, a significant number of risks reported. This conclusion was reflected in a later review by Bhaumik et al. (2011), who concluded that while the literature on the effects of deinstitutionalisation has largely shown favourable outcomes, there is evidence that life in the community is not always a positive experience. The results of the Watts et al. review are summarised in Table 1. It is the risks identified in this review that were the main determinants of the items in the audit tool used in this study.
Summary of review of positives and risk factors in resettlement (Watts et al. 2006).
The risk audit
Following this review and the possible risks highlighted, it was decided by the London Borough of Sutton to commission the Social and Health Evaluation Unit to undertake an audit of the resettled service users from Orchard Hill Hospital to supported housing in the community focusing on possible deleterious effects of the resettlement. The quality of life of 36 service users resettled from Orchard Hill had been assessed previously on four occasions over an 18-month-period and measured as having improved (Sines et al., 2012). The findings of this study were consistent with those of Bhaumik et al. (2011), who also found an improvement in quality of life indicators following resettlement.
However, the quality of life tool that had been applied in the Orchard Hill study had focused on seven domains representing quality of life, but not specifically on the possible negative effects and hence risks of resettlement and their management. Therefore, it was possible that service users might have demonstrated an improved quality of life but nevertheless be at risk in certain respects.
The risk audit tool
From the literature review and analysis of the risk factors attendant on the resettlement of adults with profound learning disabilities from hospital accommodation to supported living in the community (Watts et al. 2006), 24 areas of potential risks were identified. These were as shown in Table 2.
Risk factors and risks.
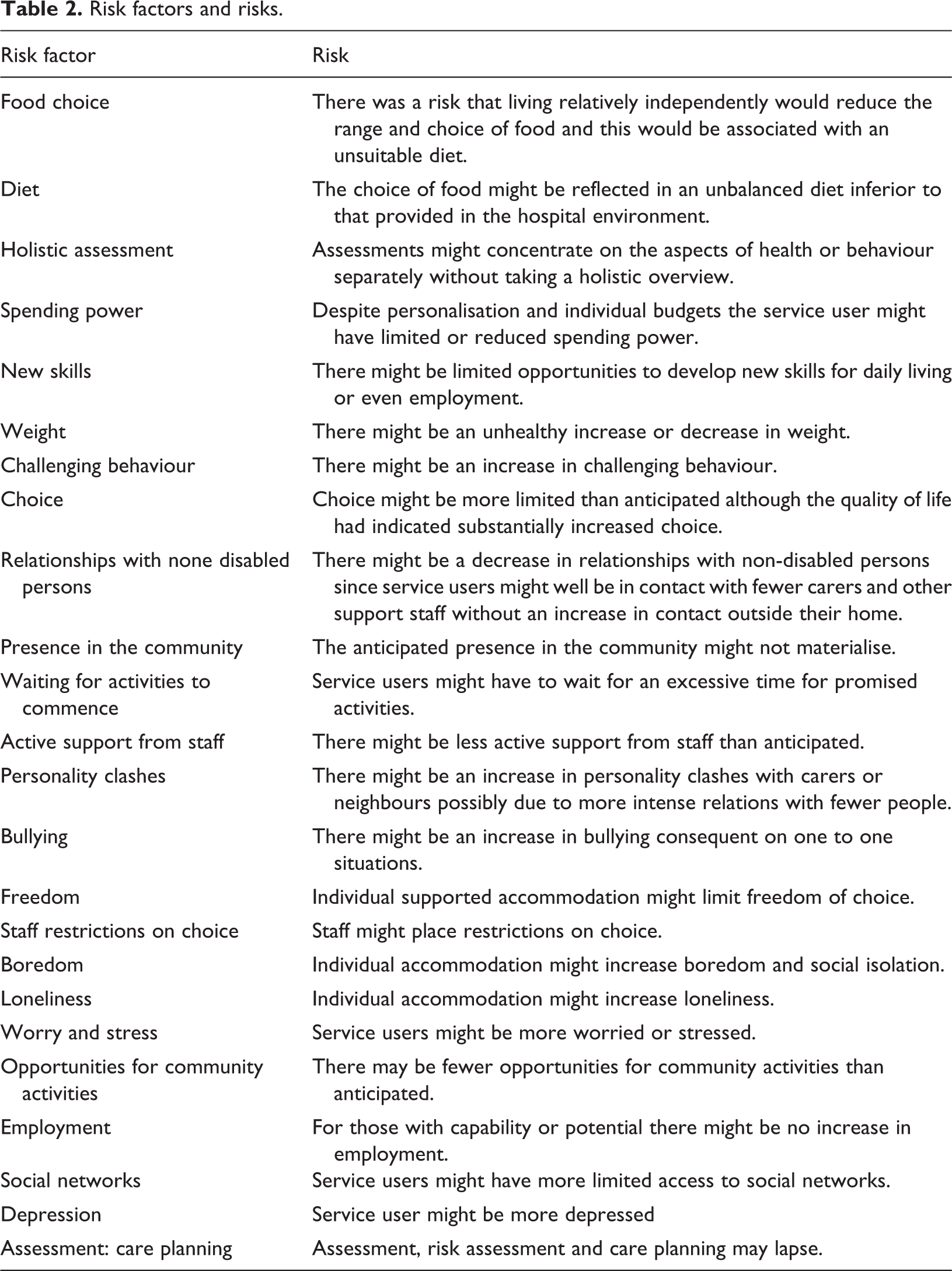
The topics chosen not only reflected the literature but were also selected as being amenable to assessment by a support worker. Each of the 24 topics had four statements attached to it, with one of these statements devised to be most indicative that the risk might be present. Respondents were invited to identify for each service user the most appropriate statement for each of the 24 topics. Whilst the choice of an indicator statement for a particular service user might signal some cause for concern, the audit method is not infallible and results had to be interpreted with caution and common sense.
Clearly, some of these risks could be a consequence of the expected advantages of supported individual accommodation not occurring. Others might be a function of more time being spent alone and unsuitable choices being made. Others might follow from a more limited social contact and an intensification of individual social problems. The comparison inherent in the risk assessment is with the previous accommodation in hospital-based facilities.
While we conceived these risks as indicating an undesirable outcome, it might be argued that some risks should be accepted as a consequence of increased freedom of choice for individuals. This tension reflects the debate between risk sensitive care and the encouragement of freedom to take risks referred to above.
Sample
The sample for the audit consisted of 36 service users who had profound learning disabilities and many had additional disabilities including autism, Down’s syndrome, epilepsy and various physical disabilities, including sensory impairment. The genders were almost equal with 19 females and 17 males. The average age was 51 years with a range from 41 to 68 years and a SD of 5.68. The majority of the service users were described as having no spoken language with a small number having severely limited language and one very limited language. Most had lived in Orchard Hill Hospital since early childhood until middle age.
Procedure
The draft tool was reviewed by managers from each of the four providers and also by the senior needs assessor from the purchaser to ensure relevance and intelligibility. It was also piloted with four support staff to ensure intelligibility and feasibility.
The four providers of supported housing or residential care undertook to ensure that audits were completed for each service user. ‘Guidance notes’ were prepared for each support worker together with an individual letter explaining the purpose and background of the tool. No difficulties were reported in the completion of the audits.
A support worker who knew the service user well completed the audit tool. Their judgements were verified by the social service needs assessor and the support worker’s manager. The audit was an attempt to see whether any of the risks identified in the literature might be present for any of the service users resettled from Orchard Hill. Since this was a service audit, formal research ethical approval was not required.
Results and discussion
In all, audits were completed for 36 service users. For these service users, the vast majority of potential risks were not found to be present. Of the 864 possible risks (36 × 24) only 62 (7%) were identified as possibly present. However, for 32 service users, at least one risk factor out of the potential 24 was identified. Individual reports were prepared for each service user highlighting the risks identified and the provider agreed to investigate and monitor the situation. This single incidence is not, however, included in the following analysis, which is of factors where risks were identified for at least two service users.
Whilst overall the occurrence or management of the risks appeared to be satisfactory, and allowing for the individual service users with some risks identified, four areas had two or more risks and are discussed below. In each case, we have indicated the number of responses and the indicative statement, and also discussed the implications of the result and action recommended.
Assessment and care planning resulted in a variety of responses, which in itself suggested that the area was variably understood and managed and hence possibly indicative of risk.
The indicative statement chosen in the majority of the audits (32 of 36) was:
Service user is assessed and care plan reviewed as needs arise.
In constructing the tool, this statement was chosen to represent a relatively unstructured approach to assessment and care planning and hence a possible risk.
The alternative statements available indicated that a review took place monthly, quarterly, or half-yearly intervals. A limitation of the set of statements emerged in that a number of respondents added a statement that the care plan was reviewed annually and advised that this statement was not available as an option in the assessment tool. There were also variations between providers and within providers, with only one provider being unequivocal and inserting annually for their four service users.
This amount of variation would suggest that there is not a generally understood standard. However, it might be that a clear understanding has been obscured by the way in which the item merges processes that are functionally separate. It is now clear that this item encapsulates three processes, namely, assessment, support planning and care planning. The first two are the direct responsibility of the purchaser, whereas the third is the responsibility of the providers.
Further consideration of this topic clarified definitions and responsibilities for the assessment and care planning and highlighted different interpretations of assessment, care planning, responsibilities and time scales.
The results from this item should, therefore, be interpreted with caution, since respondents might not have been clear regarding which of the processes was being audited.
There is sufficient ambiguity, misunderstanding and variety here for us to recommend that service contracts should clearly set out responsibilities for assessment, personal support planning and care planning and the time scales associated with each. Regular monitoring should seek to ensure compliance with these standards.
Staff restrictions on choice was highlighted as a possible area of risk where 11 service users were linked with the indicative statement:
Service user’s choice is of necessity restricted by staff.
Several auditors qualified the use of this statement by referring to diet where there are of course risks if the diet is not monitored. Given the physical health status of a number of service users (e.g. for those who present with diabetes, obesity or other health-related challenge) it may well be that restrictions are necessary. However, we recommended that this area should be kept under review to make sure that the potential for personalisation and informed choice is not being limited unnecessarily.
The next most common risk areas were new skills and relationships with non-disabled people. where the risk was identified, in both cases, for nine service users.
For new skills, the indicative statement was:
Service user is unable to develop new skills.
Clearly, it could be the case that a minority of service users might appear incapable of developing new skills but there should be attempts to identify very modest goals for all service users with additional efforts made to achieve them in the most challenging cases. We recommended that this should be reflected in care plans and service contracts.
For relationships with non-disabled people, the indicative statement was stated as:
Service user has fewer relationships with non-disabled persons than they had in the hospital.
The fact that some service users (nine) may have fewer relationships with non-disabled persons than in the hospital is worrying and reflects similar concerns about social relationships as emerged from the quality of life audit (Sines et al., 2012). We recommended that special steps should be taken to commission additional activities in the community for service users to maximise the opportunities for social interaction. This should also address the next two risks identified, which included opportunities for community activities (seven), and presence in the community (six). We recommended that service contracts should require providers to evidence both social engagement/activity plans and regular reports on community activities and user participation. In order to optimize community activities, scoping exercises should be carried out in the local communities to identify possible activities.
(Lack of) Opportunities for community activities was identified as a risk for seven service users. The indicative statement was:
The service user has limited opportunities for community.
Given that the group are now living in supported housing in the community where possible community involvement is seen as a positive advantage, it is disappointing that a fifth of the sample have limited opportunities for community activities. We recommended that the opportunities that are available in the local communities should be explored and identified and positive steps are taken to encourage involvement taking account, of course, of individual preferences.
Similarly, six service users were identified as having limited presence in the community, where the indicative statement was:
Service user has limited presence in the community
This is again a disappointing result that suggests that the potential for enhanced community living may not being fully exploited. Of course this may reflect the capability and disposition of the service users concerned, but we recommended that consideration should be given to the community activities specified in the contract and their effectiveness and to individual care plans.
Waiting for activities to commence was identified as an issue for five people. The indicative statement was:
Service user spends considerable time waiting for activities to start.
While it is no doubt that service users will spend some time inevitably waiting for activities to begin, this was identified in the literature as a particular cause of frustration where there was a delay from the promised or anticipated start time. No major delays were reported in the current audit, but we recommended that support staff should monitor delays and try to keep them to a reasonable minimum if and when they do occur.
Reduction in freedom was identified for three people, where three indicative statements gave some cause for concern. The optimal and expected response was:
Freedom is a distinctive feature of this service user’s life compared with his/her life in the hospital.
Clearly, freedom is a relative term, but nevertheless, compared with the institutionalised life in hospital-based accommodation, greater freedom should result from individual housing. Those whose freedom was not considered to be a distinctive feature of their life were described as ‘enjoying as much freedom as circumstances allow’ or ‘necessarily restricted’ or for whom ‘freedom was unrealistic’.
We recommended that providers should reflect on the kind of freedom each service user should expect and include appropriate objectives in their care plan.
Evidence of ‘depression’ characterised three people for whom the indicative statement was:
Service user appears very depressed.
Whilst it might be predicted that some people from a population of 36 might be depressed, this characteristic should be carefully monitored and addressed in care plans.
Similarly worry and stress was reported for two service users with the indicative statement:
The service user usually appears worried.’ And again this should be addressed in care plans.
Two service users were reported as enjoying fewer social networks than in the hospital with the indicative statement being:
Social networks are limited for this service user.
While results for this item relate to small numbers, this does reflect a concern that followed the application of the quality of life audit undertaken previously for these service users (Sines et al., 2012). This is particularly relevant when service users are relocated into their new homes that are managed by a diverse group of service providers. Consequently, service commissioners and managers are advised to measure the potential impact that the new accommodation might present as risk factor to limit social interaction.
Finally, two service users were reported as having limited choice, the indicative statement being:
Service user has little real choice.
This result, albeit for only two service users, and the result for eleven users, where staff were described as necessarily restricting choice (reported above), highlights an area for consideration generally and should be identified and monitored in individual care plans and individually designed risk assessments.
Results where a risk was identified for one service user only are not discussed here. However, individual reports were produced for each service user so that they might be taken into account in care planning and support planning.
It should be noted that a number of risks were not identified for any service users and these included those associated with challenging behaviour, personality clashes and bullying. While we do not have data for these risks when the service users were in hospital care, it seems likely that their absence in this study is a feature of individual supported housing.
Conclusion
A risk audit carried out by support workers proved to be a feasible method of checking whether risks reported in the literature were occurring in this relatively recently resettled population. Allowing for the limitations of the method, risks were identified with organisational and individual implications. As is described above, risks were reported to the purchaser and individual providers and recommendations made regarding contracting and organisation generally and, specifically, in individual care plans. The specially developed tool proved feasible and reliable. It has face and construct validity but further studies will be required to demonstrate correlational and predictive validity. It is available for those who wish to use it from the first author.
A risk audit of this kind should not only identify risks and suggest remedial action but should also serve to stimulate discussion on the appropriate balances between risk management and individual personal choice.
Tools of this kind require a regular review of the literature to ensure that the risks audited are as current as possible. The utility of such audits depends on the use, which is made of the results in the review of both individual care plans and organisational procedures.
Risks identified for an individual should certainly be included in his/her care plan and appropriate action followed and monitored. When larger numbers are involved, and it is a matter of judgement whether numbers in single figures represent a significant trend, policy, circumstances and operations should be reviewed.
When numbers more than 10 occur for a particular risk careful consideration should be given to amending the commissioning contract to require service providers to provide evidence of how they are planning to maximum personal choice, whilst militating against the occurrence of harm or risk.
Since the resettlement programme reported in the current study is still at a relatively early stage, any risk that occurs subsequently should be carefully monitored in case it is the first sign of a trend.
In conclusion, we recommended that the risk audit tool should be reviewed annually to reflect the up to date literature and should be used annually to monitor provision and the status of service users.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.