
Abstract
Little research has been carried out on the physical health of people with autism spectrum disorder (ASD). From the studies conducted with both children and adults, few studies have moved beyond retrospective record analysis and survey and conducted health assessment. The majority of the studies are from the United States of America with a small number conducted in Europe. A scoping review was conducted to determine what is known of the physical health of adults with ASD and to identify research gaps. In addition to studies of adults, this review includes studies of children to determine possible health trajectories. From the findings, it can be stated with confidence that people with ASD have a high rate of comorbidity and increased risk for chronic disease.
Introduction
As the current approach of episodic incident-based funding to treat health disorders in many Western countries such as the United States and Australia is now widely acknowledged to be unsustainable, health promotion is receiving increased attention (Armstrong et al., 2007; Russell et al., 2008). Population health-related factors such as the prevalence of overweight and obese citizens are generally known and the links of being overweight or obese to metabolic syndrome, cardiovascular disease, type 2 diabetes, and associated social problems are widely documented. Despite the shift in focus to the health of the citizenry, little is known of the physical health of people with autism spectrum disorder (ASD). There is a small but growing body of international research related to the physical health of children with ASD but a marked paucity of studies related to the health of adults with ASD. This lack of knowledge of the physical health of adults with ASD is significant, as although average life span for someone with ASD is not known, generally life spans for people with developmental and intellectual disabilities are normalizing. A scoping review to determine what is known generally of the physical health of people with ASD is warranted. A systematic review of mortality in ASD, from the limited pool of studies available internationally, identified that people with ASD have a higher risk of mortality in the population than those without ASD (Woolfenden et al., 2012). The higher risk of mortality from the limited literature appears to be all case mortality (Mandell, 2013). With aging of this population, a disproportionate rate of chronic illness can be expected (Howlin and Moss, 2012). This chronic disease will reduce the quality of life and place a burden on health resources (Guh et al., 2009). Although not consistent in study findings, it has been established that people with intellectual disability have an inequitable burden of health risks as compared to the general population (Havercamp et al., 2004). It is emerging from the limited studies available that people with ASD share at least a similar burden, and arguably from the majority of studies a higher burden of risk, for less than optimal health than people with intellectual disability and the population without disability (Broder-Fingert et al., 2014; Rimmer et al., 2010).
In 2000, Berney wrote of autism research through the metaphor of 19th-century exploration in which, “well mapped areas are outweighed by the unknown, from which emerge traveller’s tales of strange practices and exotic cures” (Berney, 2000: 24). Much has changed in the ensuing 16 years in relation to the territory of ASD. However, a recent mapping of the needs of adults with comorbid ASD and intellectual disability identified that a marked absence of a program of research to determine the health and wellness of this group of people with intellectual disability exists (Van Dooren et al., 2016). The research gap related to the physical health of adults with ASD is understandable as it has occurred in the context of less than 2% of ASD research funds being spent on research with adults with ASD (Office of Autism Research Coordination. National Institute of Mental Health on behalf of the Interagency Autism Coordinating Committee, 2012). To put this in perspective in the US$400 million is invested annually in ASD research; however, few studies have been supported that have focused on priorities of adults with ASD including physical health and health-care needs (Nicolaidis et al., 2013). It would appear that the ASD cartographers have been busy focusing on the pervasive elements of the triad of impairments, particularly in children, but the overall health and well-being of those with ASD is a new frontier. This may be symptomatic of the often-held general perception that ASD is a disorder of childhood (Mandell, 2013). From the literature, it is not clear whether the absence of research related to the needs of adults is restricted to the group of people with ASD with comorbidity as identified by van Dooren et al. (2016), or ASD in general. To determine what is known of the health and wellness generally of people with ASD, the importance of considering both studies of childhood and those of adults in the one comprehensive review of the literature is underpinned by the contemporary understanding of health trajectories. It is understood, for example, that children who are overweight or obese are more likely to experience obesity as adults (Curtin et al., 2010). “Compared to the general pediatric population children with autism have higher rates of co-occurring medical and psychiatric illnesses, yet very little is known about the general health states of adults with autism” (Croen et al., 2015: 814). The proposed trajectory from childhood health risks to adult health, in the context of a paucity of adult research on health status of those with ASD, underpins the importance of inclusion in the same review. This inclusion adds an extra dimension when considering the impact of the limited adult studies.
In the current obesogenic/poor health predisposing environment, it has been suggested that people with autism are exposed to the same risk factors as the general population with additional autism specific factors (Curtin et al., 2014). These risk factors include restricted dietary preferences and habits, challenges participating in socially mediated physical activity such as sport and many weight management initiatives, restricted behavior manifested in increased screen time, a high prevalence of sleep disorder, and a high comorbidity of mental disorders with associated use of psychotropic medications (Broder-Fingert et al., 2014; Curtin et al., 2010, 2014; Hinckson et al., 2013). These factors raise the index of suspicion that people with ASD may face increased health risks.
The aim of the scoping review was to determine what is known of the physical health and well-being of people with ASD through consideration of studies across the life span. Mental health is discussed only when reported in studies including physical health.
Method
A scoping literature review was undertaken to determine what is known of the physical health of adults with ASD and to identify research gaps (Arksey and O’Malley, 2005). The search terms: “autism,” “autistic disorder,” “Asperger’s disorder,” “autism spectrum disorder” were combined in an iterative manner with obesity, obese, diab*, cardiovascular, physical health, and well-being and searched in the databases Medline, PsycINFO info, and PubMmed for the years 2000–2015. Abstracts were reviewed to identify studies of the physical health of people with ASD. All studies identified were included in the review.
Studies that did not explicitly identify participants with autism, ASD, autistic disorder, or Asperger’s disorder were excluded from the review. A large number of small studies exploring gastrointestinal health and autism were identified. The causative elements to becoming overweight and obese are not linear and can include neuroendocrine and genetic factors (Pitetti et al., 2007). Neurometabolic factors related to autism while often presented as potentially causative factors in discussion articles and case reviews probably account for less than 5% of ASD presentation (Manzi et al., 2008). Although the basis of many of the next can’t miss cures (Nash, 2002), this is a small heterogeneous group and beyond the scope of this article to detail. After a review of the literature, it was determined that: the benefit of laboratory testing for a high-functioning child with a normal appearance and moderate language impairment is minimal. Selective metabolic testing should be initiated only in the presence of suggestive clinical findings, including lethargy, cyclic vomiting, early onset seizures, dysmorphic features and mental retardation. (Manzi et al., 2008: 311)
Based on the presence of a comprehensive review already existing, and the conclusion of the impact on a small heterogeneous subgroup of people with ASD, these single-focused studies were excluded from this review.
Only studies published in English were included in the review.
Reference lists of identified articles were examined to identify any other studies not identified in the original search. See Table 1 for search results.
Search results.
Findings
Child studies
Research on the health of children with autism as a separate group or a part of a broader sample included primary and secondary analysis of questionnaires/surveys (Curtin et al., 2010; Rimmer et al., 2010), medical records review (Broder-Fingert et al., 2014; Kohane et al., 2012), and one study that conducted a health assessment of participants (Stewart et al., 2009). Two small-scale intervention studies were identified (Hinckson et al., 2013; Pitetti et al., 2007). See Table 2 for a summary of studies in which specific findings for the sample with ASD are reported and discussed.
Summary of studies evaluating health in children and adults with ASD in which specific ASD findings are reported.
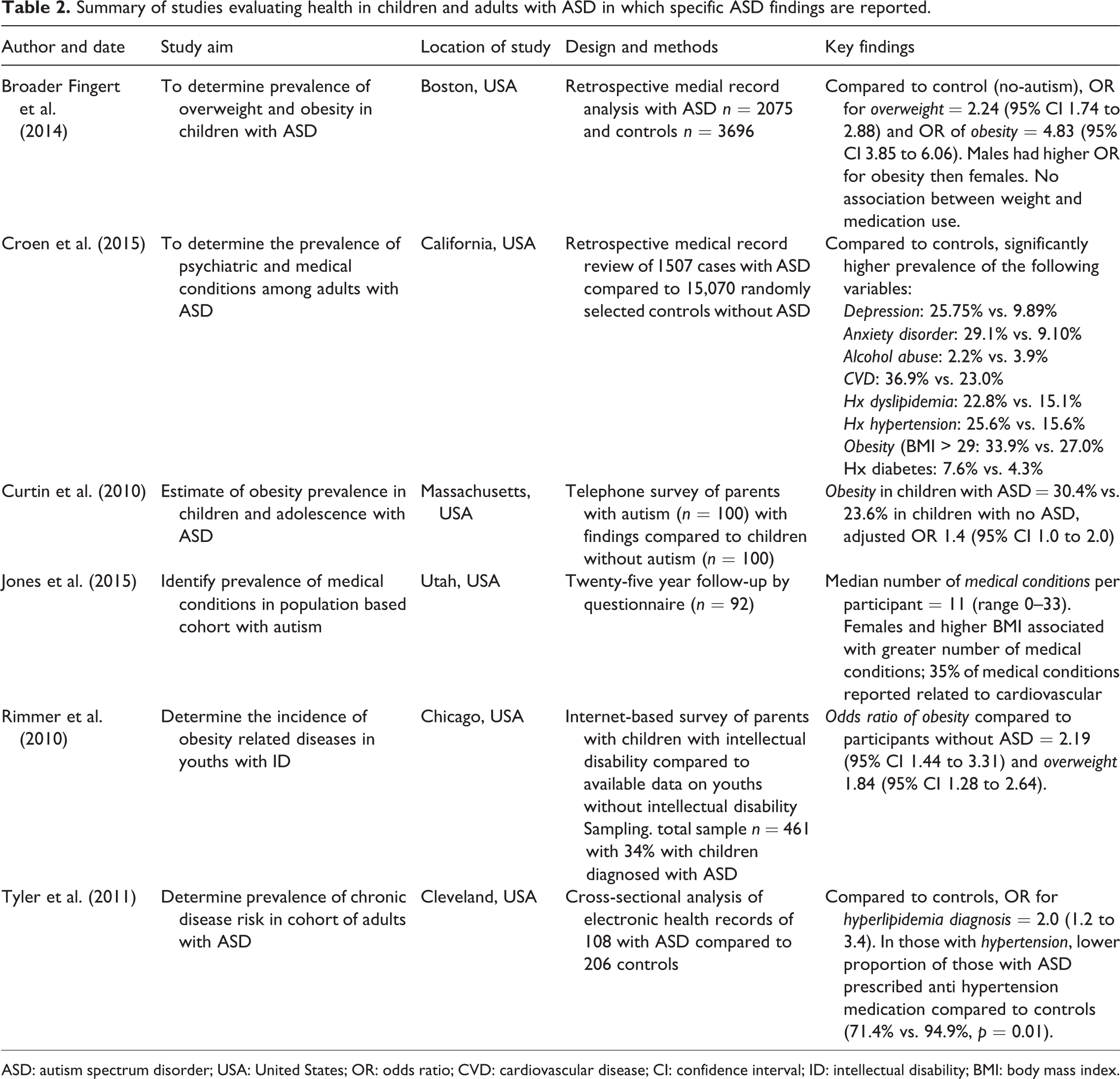
ASD: autism spectrum disorder; USA: United States; OR: odds ratio; CVD: cardiovascular disease; CI: confidence interval; ID: intellectual disability; BMI: body mass index.
Curtin et al. (2010) examined the prevalence of obesity in children with ASD. A secondary analysis was conducted for children aged 3–17 years from the US National Survey of Children’s Health 2003–2004. This survey was originally conducted by computer-assisted random number dialing of households with children in the United States. The study was limited by the acknowledged reliance on self-report by parents or guardians and the criteria for ASD being the question of whether a health professional or doctor has ever told the parent the child has autism. In the sample, 483 children with autism were identified based on this criterion. They were found to be 40% more likely to be obese than children without autism. In addition, 94% were identified to have a comorbid health condition as compared to 17% of those without autism.
Rimmer et al. (2010) conducted a survey of 461 parents of children aged 12–18 years of age with intellectual and developmental disabilities (including ASD) in the United States. The sampling method precluded calculation of a response rate, and the survey was based on self-report of parents or guardians. A link to a survey website was advertised through disability and health advocacy organizations, a disability website, and a parenting magazine. On the website were the inclusion criteria and the survey. Children with ASD made up 34.5% of the sample. For those with ASD, 24.6% were identified as obese and 42.5% as overweight. This finding was compared to those with intellectual disability without comorbid ASD from which 12.4% were identified as obese and 27.2% as overweight. Those in the combined sample who were obese or overweight reportedly experienced a significantly higher proportion of comorbidities. The rate of being obese or overweight in the sample was reported to be two to three times higher than non-disabled youths matched for age and gender at the time of the survey.
Broader-Fingert et al. (2014) examined the prevalence of being overweight and obesity in children with ASD aged 2–20 years through a retrospective analysis of medical records for those with a diagnosis of autistic disorder or Asperger syndrome sampled from an integrated health system in Massachusetts in the years 2008–2011. It was determined that 2017 people with autistic disorder and 901 people with Asperger syndrome had a height and weight measurement that allowed calculation of the body mass index (BMI). A control group of 3696 people was selected from the same system. Both the autistic disorder and Asperger’s groups were reported to have significantly higher odds for being obese or overweight than the control group. The Asperger’s group had higher odds than the autistic disorder group. An interesting finding was that no association between use of psychotropic medication and being overweight or obese was identified in the sample.
Kohane et al. (2012) focused on comorbidity in a sample of people with ASD. The study used a retrospective analysis of electronic health records from three general hospitals and a children’s hospital in Boston, USA. Diagnosis was based on the ICD-9 (International Classification of Diseases 9). The records were interrogated based on hypothesis-driven questions to compare comorbidities for those with ASD younger than 35 years as compared to those without. The sample was reported to be almost 15,000 without further clarification. The ASD group was found to have a significantly higher prevalence than those without autism of central nervous system (CNS) anomalies, epilepsy, diabetes, bowel disease, sleep disorders, and schizophrenia. The prevalence of schizophrenia and sleep disorders in the ASD sample was reported to be 10 times higher than the sample without autism. The findings were further analyzed based on being aged 0–17 years or 18–34 years. The older cohort was significantly more likely to have a diagnosis of diabetes, bowel disease, and schizophrenia than those in the younger cohort. The limitation of the same individual being included more than once if they attended different hospitals in the sample was acknowledged.
Studies in which health assessments are undertaken to collect the data overcome the limits of retrospective analysis of records and self-report in surveys. Only one study using such measures of health, excepting the two intervention studies, was identified. Stewart et al. (2009) conducted a study of 206 children and adolescents who attended nine special schools in Scotland in the United Kingdom in 2007. The sample was children and adolescents with intellectual disability and included 43% who had a comorbid diagnosis of ASD. No breakdown of findings was provided based on diagnosis. Height and weight were measured and it was determined that 43% of girls and 32% of boys in the combined sample were obese. This was reported to be higher than the general population.
In summary, through survey, Curtin et al. (2010) identified that children with ASD in their sample were 40% more likely to be obese than those without ASD and 94% versus 17% have comorbidities. Rimmer et al. (2010) determined in their sample that people with ASD are at a higher risk of being overweight and obese than those with intellectual disability without comorbid ASD. An association between being overweight or obese and the experience of increased comorbidity was noted in the combined sample. Through retrospective analysis of medical records, Broder-Fingert et al. (2014) identified that children with ASD have higher odds of being overweight or obese than a matched control group. In the ASD group, those with no comorbid intellectual disability had higher prevalence of being overweight or obese than those with comorbid intellectual disability. No association was identified between psychotropic medication use and weight. Kohane et al. (2012) identified that their sample of people with ASD experienced CNS anomalies, diabetes, epilepsy, bowel disease, and schizophrenia significantly more frequently than those in the control group. The only study that involved conducting health assessment of participants sampled a group of children with intellectual disability in which a portion also had ASD and identified an increased risk of being overweight or obese for the study cohort than the general population.
From the studies of health of children with ASD, it is clear that there is a disproportionately high rate of comorbidity as compared to those without ASD. General physical health status viewed through being overweight or obese was worse for those with ASD than those without, including those with intellectual disability. This has clear implications for intervention with children with ASD and their families and carers. The findings also signal a disproportionate risk of ill health in adulthood.
Two small-scale intervention studies aimed at promoting physical exercise and healthy habits were identified. Pitetti et al. (2007) in a sample of 10 children with ASD and comorbid intellectual disability aged 14–18 years who resided in a Midwestern US residential treatment facility evaluated a treadmill walking program. The study was limited by the small convenience sample, in which only five participants had the intervention and five served as controls. Outcome variables were exercise capacity measured by walking speed and elevation tolerated on the treadmill, BMI, and exercise frequency. Improvements were observed on all measures for the intervention group.
Hinckson et al. (2013) evaluated a combined intervention of physical activity and diet changes for children with intellectual disability and/or ASD identified to be overweight or obese in New Zealand. The small convenience sample was made up of seven people with ASD and three with intellectual disability only who attended a special school. A 10-week program that involved healthy eating education sessions with parents and twice weekly exercise sessions with the children was conducted. There was an identified pre and post difference in the 6-min walk test, with improvement after the intervention. This study was labeled as the first combining an exercise and diet intervention with people with ASD.
Adult studies
The adult studies of health in people with ASD as a separate group or a subsample of a larger group consisted of analysis of health record data (Croen et al., 2015; Kohane et al., 2012; Tyler et al., 2011), secondary analysis of survey data (Hsieh et al., 2014), survey (Jones et al., 2015), and one study in which health assessment of participants was conducted (de Winter et al., 2012). See Table 2 for a summary of studies in which specific findings for the sample with ASD are reported and discussed.
Tyler et al. (2011) conducted a case-controlled analysis of electronic records for people with ASD receiving care through the Cleveland Clinic, USA, in the years 2005–2008. A sample of 108 adults with ASD was identified with an average age of 29 years. A control group was matched on age, gender, ethnicity, and health insurance cover. One quarter of the sample with ASD had comorbid intellectual disability. It was identified that compared to the control group people with ASD were more likely to be diagnosed with hyperlipidemia, constipation, and epilepsy. Asthma was a less regular diagnosis. It was also identified that for those diagnosed with hypertension or hyperlipidemia, they were less likely to have prescribed intervention for those conditions than the control group. People with ASD were prescribed psychotropic medication significantly more regularly. No significant differences were detected in prevalence of hypertension, diabetes, osteoarthritis, gastro esophageal reflux disease, osteoporosis, chronic obstructive pulmonary disease, or cardiovascular disease between the study and control groups. The limitation of retrospective analysis of records was acknowledged, and the need for further investigation that collects measurements of health parameters was discussed.
As discussed earlier in relation to studies of children Kohane et al. (2012) used a retrospective analysis of electronic health records from three general hospitals and a children’s hospital in Boston, USA. The data was analyzed for individuals with ASD up to 35 years of age and identified higher prevalence of CNS anomalies, epilepsy, diabetes, bowel disease, sleep disorders, and schizophrenia than in those without ASD. The identification of higher prevalence of schizophrenia and diabetes in the young adult cohort as compared to the children with ASD is noteworthy, as insight is generated into trajectories of health and ill health.
Croen et al. (2015) conducted a retrospective case analysis of 1507 individuals with ASD aged 18 years and over, in northern California, who received care through Kaiser Permanente in the years 2008–2012. The sample was compared to a control group from the same service matched on age and gender (n = 15,070). In the sample with ASD, 19.2% had a diagnosis of comorbid intellectual disability. Adults with ASD had a higher prevalence of chronic conditions including dyslipidemia, hypertension, obesity and thyroid disease, and sleep disorder. In the sample with ASD, 54% had a recorded comorbid psychiatric condition which could be expected to compound physical comorbidity. Of those with comorbid psychiatric disorders 29% experienced anxiety, 11% bipolar affective disorder, 26% depression, 8% obsessive compulsive disorder, 8% schizophrenia, and a further 6.3% other psychoses. Psychiatric disorders were reported significantly more frequently than in the control group. Females had a higher burden of chronic conditions than males. The sample is potentially skewed by the insurance requirements to obtain service in the Kaiser Permanente system. It is not clear if anxiety and depression are describing symptoms, or formerly recorded disorder, with shifting terminology used in the descriptors.
Hsieh et al. (2014) used data from an ongoing Longitudinal Health and Intellectual Disabilities Study to examine prevalence of obesity in the US sample of adults with intellectual disability that included a subsample of people with ASD. The data consisted of n = 1619 (response rate 56.9%). Health staff completed the surveys in cases where the person was unable to do it. It was identified that adults with intellectual disability have a higher rate of obesity than the general population. The subgroup with the highest rate of being overweight and obese in the sample was people with Down syndrome followed by people with ASD for both categories. Factors contributing to obesity were taking medications with known effect of weight gain, sedentary lifestyle, and soft drink consumption.
Jones et al. (2015) recontacted participants of a 1980s epidemiologic survey conducted in Utah in the United Sates, who were identified as having ASD to participate in a health survey. Ninety-two of the past participants (response rate 30%) agreed to participate in a new health survey. Of these BMI could be calculated on 58 participants. The median age of the participating sample was reported to be 36.1 years with a range of 32.5–50.5 years. An average of 11 chronic conditions per participant was identified, with females experiencing higher comorbidity in the study sample. For those of whom a BMI could be calculated, obesity had an association with a higher number of comorbid conditions. In the sample, 27% were identified as obese, 18% over weight, and 18% underweight. Insomnia was experienced by 28.3% of the study sample. For those of whom a BMI could be calculated, the rate of obesity and being overweight is reported to be lower than the general population in the United States at the time. No association was identified between psychotropic use and BMI, hypertension, hyperlipidemia, or diabetes. In the study sample, 54.3% were taking four or more medications. It was stated that the sample with ASD experienced a disproportional amount of medical conditions, hospitalizations, and surgeries as compared to the general population.
There was only one study identified with adults with ASD in which health assessment was conducted (de Winter et al., 2012). In this Dutch study, cardiovascular risk factors were explored in a sample of 980 adults, 50 years over, with intellectual disability. The sample included people with ASD but these were not reported separately. It is included in this review as it was the only identified study in which health assessments were conducted. The method included physical examination including vena puncture, use of pedometers, and a review of records. It was identified that hypertension, diabetes, and metabolic syndrome prevalence did not differ between the study sample and the general Dutch population. Hypercholesterolemia was lower than the general population. There was no identified association between atypical antipsychotic use and cardiovascular risk factors. Higher risk factors were associated in the sample with participants who lived independently and could make their own food choices.
In summary from retrospective analysis of health record data, Tyler et al. (2011), in their study, identified that people with ASD were more likely than the controls to be diagnosed with hyperlipidemia, constipation, and epilepsy. They were less likely to be diagnosed with asthma. In terms of care, those diagnosed with hyperlipidemia or hypertension were less likely to have medications prescribed for this than those diagnosed in the control group. The question with asthma arises as to whether it is a case of equitable identification and treatment, as opposed to prevalence. People with ASD in this sample were more likely to have psychotropic medication prescribed than the control group. Croen et al. (2015) identified a significantly more likely experience of most chronic conditions for people with ASD in the study sample. Comorbidity of psychiatric conditions was very high for people with ASD. From survey, Hsieh et al. (2014) determined that people with intellectual disability in their sample had higher rates of obesity than the general population. It was further identified, that coming behind Down syndrome, the ASD subgroup were more likely to be overweight or obese. Conversely, Jones et al. (2015) identified in their sample a lower rate of being overweight or obese for people with ASD than experienced in the general population. No association between psychotropic medication use and cardiovascular risk factors was identified. Insomnia in the ASD group was high at 28.3%. The only study in which health assessments of participants were conducted, which while including people with ASD and comorbid intellectual disability, did not specifically report on people with ASD as a subgroup was of people 50 years and over in the Netherlands (de Winter et al., 2012). It was found that the prevalence of hypertension, metabolic syndrome, and diabetes did not differ from the Dutch population, although the results may have been impacted by a healthy survivor effect. No association was identified between cardiovascular risk factors and use of psychotropic medication use. It was identified that higher risk factors were associated with milder intellectual disability as people could make their own food choices.
A clear case emerges from the findings of the need for ongoing and thorough health assessments for adults with ASD and interventions promoted at optimizing health and well-being. Interventions to support equitable treatment of those with ASD in primary health care are indicated. The link between taking psychotropic medications in which a symptom is weight gain and actual weight gain has not been conclusively established in either the child or adult samples.
Discussion
From this review, it is clear that there is a paucity of research related to the health of people with ASD including a remarkable lack of studies that have included direct health assessment of participants. The majority of studies have been completed in the United States. Presently, a clear understanding of the general health status for people with ASD is lacking; however, cardiovascular risk factors and the presence of comorbidities are mostly reported to be higher than for people without ASD. Life expectancy statistics are uncertain for this group, although mortality risk appears higher than for those without ASD (Woolfenden et al., 2012). From the findings it is clear that risk begins early in life and therefore bodes poorly for later life outcomes. Generally, it can be stated that people with ASD in the United States have more risk of being overweight or obese than the general population and potentially increased prevalence of other cardiovascular risk factors across the age span. Risk may be higher for females and those with no or mild comorbid intellectual disability. Where risk exists, it appears that primary care intervention to mitigate the risk is less likely to occur for people with ASD than those without. This finding is further supported by a study that looked at quality of follow up care for people with diabetes using medical record data (Shireman et al., 2010). High rates of comorbid psychiatric disorders, including schizophrenia, are experienced as compared to the general population. This may deliver a double burden as people with mental illness also experience poor physical health and multiple barriers to effective physical health interventions. Of note is that no correlation between psychotropic use and being overweight or obese was found in one study of children (Broder-Fingert et al., 2014) and in adults (de Winter et al., 2012; Jones et al., 2015). Only one of the studies reported a correlation between taking obesogenic medications and risk of being overweight or obese (Hsieh et al., 2014). In a study of people with developmental disability (not specifically ASD), it was identified that people with developmental disability were more likely to have a lack of emotional support than those in the other groups (Havercamp et al., 2004). Although none of the health studies of people specifically with ASD reported emotional support, it can be assumed this may be a significant factor worthy of future exploration in light of the high comorbidity of mental illness and ASD.
Conclusion
The initial cohort first diagnosed with ASD in the 1950s and 1960s have reached the period of life where age-related health needs would be expected, yet there is a paucity of research into the health and health needs of older people with ASD (Happe and Charlton, 2012; Howlin and Moss, 2012). It is now 21 years since Asperger’s disorder was introduced into the Diagnostic and Statistics Manual and the time when the diagnostic vision of clinicians again expanded to once more allow the recognition of ASD in those without a comorbid intellectual disability, and consequently there is now a wave of young adults with a diagnosis of ASD (Mulder and Cashin, 2014). This wave reflecting the proportional shift from approximately 20% of people with ASD diagnosed who did not have a comorbid intellectual disability to the now reversed proportions. Research expenditure has not followed the shifting demographic profile of those with ASD as reflected in the small amount invested into research with adults with ASD (Van Dooren et al., 2016). This review clearly highlights that further research is indicated. There is a critical need to increase our understanding of the health profile of people with ASD, including trajectories of illness from childhood across the life span and the predictors of health and ill health. This will allow an understanding of the ramifications of chronic disease for this group, the risk profiling for chronic illnesses, and will guide development of informed primary health-care services and interventions. This identified need challenges the current bias of research investment in ASD toward childhood and early adolescence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.