
Abstract
People with an intellectual disability are less physically active, live more sedentary lives, have lower fitness levels and are more likely to be overweight or obese than the general population. No evidence exists on the impact of participation in Special Olympics Ireland (SOI) on physical activity and physical fitness levels. Adults with intellectual disabilities (16–64 years) were recruited from services and SOI clubs. Physical measures included waist circumference, height, weight, blood pressure, heart rate and 6-min walking test. Self-report questionnaires gathered data on physical activity levels. Actigraph (GT3X) accelerometers were used to gain an objective measure of physical activity. SOI participants accumulated more moderate to vigorous physical activity per day, had higher fitness levels and more positive health profile scores than those not taking part in SOI. SOI has the potential to make a positive difference to people’s physical health and subsequently their overall health and well-being.
Introduction
Special Olympics Ireland (SOI) is a popular organization or club that people with intellectual disability attend offering opportunities for involvement in sport and enhanced social networks. SOI was founded in 1978. Over the past 37 years, it has grown significantly and today has approximately 9000 athletes participating in 15 sports across 385 clubs throughout the island of Ireland. There were over 27,691 people registered on the National Intellectual Disability Database at the end of December 2013, indicating that approximately 33% of people with an intellectual disability are currently members of SOI. It is the most popular source of physical activity for people with intellectual disabilities (McCarron et al., 2014).
Regular participation in physical activity is widely acknowledged as being important for primary and secondary prevention of an array of conditions such as several chronic diseases, including obesity, coronary heart disease, hypertension, type 2 diabetes, osteoporosis, depression and colon cancer (Blumenthal et al., 1999; Bonaiuti et al., 2002; Evans, 1999; Marshall et al., 2003; Thompson et al., 2003). It can also reduce the risk of premature death (Warburton et al., 2006). This is particularly beneficial to those with an intellectual disability who are at a greater risk of co-morbidities such as respiratory disease, cardiovascular disease and cancer (Prasher and Janicki, 2002). Macera et al. (2003) found that inactive people are twice as likely to develop/die from chronic heart disease as active people. Rippe et al. (1988) highlight even if a person was to perform activities of low to moderate intensity, such as walking for pleasure, dancing or yard work on a daily basis, they would reap long-term health benefits and reduce the risk of cardiovascular disease.
People with intellectual disabilities
People with intellectual and physical disabilities who are more physically active tend to visit doctors less and have fewer medical complications according to the National Disability Authority (Hannon et al., 2006). The link between the benefits of physical activity to mental health has been a hot topic for many years. Andrews (2005) reported that physical activity increases well-being by increasing pride in physical accomplishments, improving body image and promoting more self-confidence. Often, people with an intellectual disability can experience difficulties in developing positive self-concepts of both physical and social competencies. These negative thoughts may have derived from situations of social isolation, discrimination, discrimination and stigmatization. Participation in physical activity allows for the prevention of isolation (Mutrie et al., 2007). Group activity has been proven to increase levels of participation in physical activity due to the enjoyment and social support it provides (Allender et al., 2006). Physical activity provides an outlet for people to share their experiences, difficulties and achievements (Allender et al., 2006). Physical activity has also been shown to have a mitigating effect on challenging behaviours in people with intellectual disabilities (Moone and Renzaglia, 1982; Nishiyama et al., 1986; Washburn et al., 2002).
Bartlo and Klein (2011) conducted a systemic review of the literature on the physical activity benefits and needs for adults with an intellectual disability. Within this review, they found compelling evidence to suggest that physical activity is important in creating improvements in a number of aspects of a person’s physical state. Findings suggest that physical activity was responsible in positively affecting balance, muscle strength and also quality of life in individuals with intellectual disabilities. They also suggested that exercise programmes need to be adapted so that they can facilitate the individual needs of people with intellectual disabilities.
Wu et al. (2010) evaluated a 6-month physical fitness programme on people with an intellectual disability living in a disability institution in North Taiwan. Post-intervention scores found statistically significant decreases in individual’s weight, body mass index (BMI) score, BMI category and significant positive improvement in V-shape sit-and-reach test, sit-up in 30 s and 60 s tests. Similarly, Carmeli et al. (2005) investigated the effects of physical training on balance, strength and well-being of older adults with mild intellectual disabilities. Positive relationships existed between all categories tested as a result of exercise participation for adults with intellectual disabilities.
Guidelines for physical activity drawn up by the American College of Sports Medicine and the American Heart Association specify recommendations for all members of the population including people with intellectual and physical disabilities (American Heart Association, 2007). Adults (aged 18–65) should accumulate at least 30–60 min of moderate-intensity aerobic activity 5 days per week or engage in 20–60 min of vigorous activity 3 days per week. It is further recommended that activity must be at least 10 min in duration to count towards daily goals and that a combination of moderate- and vigorous-intensity physical activity is acceptable. The National Physical Activity Guidelines for Ireland are consistent with recommendations worldwide and include recommendations specific to people with a disability concurrent with the guidelines set out for America in 2007. It recommends a minimum of 30 min of moderate to vigorous physical activity per day for adults to garner health benefits and where possible, people with intellectual disabilities should aim to meet the same guidelines. When adults with intellectual or physical disabilities cannot meet these guidelines, they should aim to be as active as their ability allows, taking into account specific health risks and limitations and should avoid inactivity where possible (Department of Health and Children and the Health Executive, 2009).
While SLÁN 2007 study (Ward et al., 2009) found that a high proportion of the Irish population do not meet the minimum physical activity guideline, a report by Hannon et al. (2006), who did a secondary data analysis of the 1998 and 2002 SLÁN data, revealed that people with an intellectual or physical disability were even less likely to comply with the known minimal physical activity recommendations. The Hannon et al. (2006) report showed that 35% of people with an intellectual or physical disability reported no physical activity of at least moderate intensity per week, compared to just 10% of the general population. People with an intellectual or physical disability were also found to be less likely to undergo physical activity of any type including leisure, housework or work when compared to those reporting no disability (Hannon et al., 2006). The TILDA (The Irish Longitudinal Study on Ageing) report on people with disability in Ireland further highlighted that 77.3% of Irish adults with intellectual disabilities over the age of 40 years were considered overweight or obese (McCarron et al., 2014).
Issues with low levels of physical activity are not exclusive to the Irish intellectual disability population with research showing that people with an intellectual disability are less physically active than the general population worldwide (Robertson et al., 2000; Stanish et al., 2006; Temple, 2007). The proportion of people with an intellectual disability who are overweight or obese also appears to be higher compared with the general population (Marshall et al., 2003; Martin et al., 1997; Prasher, 1995). In a UK study, Messent et al. (1999) examined a 7-day physical activity profile revealing that 22 of the 24 participants were significantly below the Department of Health minimum physical activity guidelines, demonstrated high levels of obesity and also scored lower levels of cardiorespiratory fitness levels compared to the general population. Using accelerometry to measure physical activity, adults with an intellectual disability in the United States (n = 44) only accumulated 7.73 ± 24.21 min of moderate to vigorous physical activity per day and 48% of the participants averaged zero minutes of moderate to vigorous physical activity per day (Bodde et al., 2013). Similarly, Frey et al. (2005) found that in a sample of 22 adults with intellectual disabilities, moderate to vigorous physical activity averaged 19.7 ± 17.6 min per day.
The NDA, in 2005, published a report on promoting participation in physical activity and sport for people with an intellectual or physical disability across Ireland. There has been considerable recognition in Ireland in recent years that people with an intellectual disability should be granted the same opportunities to access physical activity and sporting opportunities as the general population (NDA, 2005). The report highlights a number of barriers that can prevent such inclusion in Ireland. These include (i) negative school experiences and poor physical education provision in schools, (ii) lack of information and expertise provided by service providers such as coaches and staff at leisure centres, (iii) low expectations from family and friends, (iv) poor community facilities and lack of access to facilities and programmes, (vi) a lack of knowledge of the benefits of physical activity, (vii) lack of companions who can facilitate/assist people with intellectual and physical disabilities to access facilities and programmes when required and (viii) a lack of a culture of general participation in physical exercise and sport in Ireland.
To date, no evidence exists on the impact of SOI participation on physical activity, fitness or BMI levels in Ireland. The current study was carried out as part of a larger mixed-method study entitled ‘The SOPHIE study’ (Special Olympics Programmes Health Impact Evaluation) that explored the impact of SOI programmes on the health and well-being of individuals who take part in SOI programmes on the island of Ireland compared with persons with intellectual disability who do not take part in SOI. It compared physical activity, physical fitness levels, BMI and blood pressure (BP).
Methodology
Consent, assent and ethical issue
Ethical approval for this study was obtained from the Ethics Committee of Dublin City University and the ethics committees of the four care services for persons with intellectual disabilities from which the participants were recruited. Assent/consent forms were developed in an easy read format. Each step of data collection was explained to participants face to face on the day of data collection by a member of the research team. Participants and their family members marked which aspects of the study they agreed to and signed the consent/assent forms before participating in the study. Participants who were unable to provide a signature marked an ‘X’, this was witnessed by two researchers. All family members were asked to sign a consent form on their own behalf and on behalf of their family member with an intellectual disability.
Study participants were informed of their right to withdraw at any stage of the process or say no to any part of the study and that all information provided would be confidential. At the stage of applying for ethical approval, the question of non-verbal participant’s capacity to decline participation was raised as an issue by the Research Ethics Committee at Dublin City University and the research team were asked to be aware that this issue could arise. It was critical that the whole team were vigilant and mindful of non-verbal cues from participants which may have indicated their unwillingness to partake – in this instance, participants would not have been recruited. The situation did not arise however and in fact all those who took park were willing to do so and in fact seem to have enjoyed the experience.
Participants
Participants were recruited through the four intellectual disability service provider organizations from a large urban and rural geographical spread. Members of the research team met with a designated staff liaison person at each service and explained to them the purpose and processes of the study. All eligible individuals with an intellectual disability who were registered with the service providers were invited to participate in the study via intellectual disability friendly literature developed by the study team. This was followed up with a phone call where verbal information was provided to prospective participants. In total, 1908 individuals were invited by letter to participate in the study through the four service providers. On average, 2–3 calls were made to each individual invited to take part. If members of the research team were not successful in making contact after the fourth call, potential participants were removed from the list. In addition to raise local awareness of the study, advertisements were placed in local newspapers and a radio interview was conducted by the principal investigator of the team.
The overall SOPHIE study aimed to recruit up to 400 individuals with an intellectual disability from intellectual disability service provider organizations: 200 who do take part in SOI programmes and 200 who do not take part in SOI programmes. Inclusion criteria for participation were persons (i) with an intellectual disability, ambulant or non-ambulant, over 16 years of age, (ii) registered with a service for people with an intellectual disability, or registered with SOI, (iii) with verbal communication skills sufficient to provide information about themselves, or a family member willing to provide this information and (iv) with the ability to provide assent or a family member willing to provide informed consent. All participants were accompanied by a family member during data collection.
Measures
Having consented to taking part in the study, participants and family members were met in a location convenient to them, that is, local service provider location or local venues (e.g. sports hall) that were appropriate for data collection. A nurse qualified was present for the collection of all physical data. Data collection included self-report questionnaires, 6-min walk test, anthropometry and accelerometry.
Self-report questionnaire
As there is no validated instrument available for collection of self-reported physical activity data for this population, the questionnaire used to ascertain the self-reported level of physical activity was an adapted version of the Survey on Lifestyle and Attitude to Nutrition (SLÁN, 2009). This is a survey on the lifestyle, attitudes and nutrition that has been used across the general population in Ireland. The questionnaire used in this study contained questions on (i) demographics of the study participant, (ii) general health and (iii) physical activity levels. The physical questionnaire included questions on physical activity frequency and intensity from the short form International Physical Activity Questionnaire, used previously with the SLÁN 2007 study (Ward et al., 2009).
The questionnaire defined physical activity was defined as mild, moderate and vigorous. To help create a more user friendly questionnaire and to aid understanding for the study participants, pictorial representations of various activities representing mild activities such as golf, fishing and easy walking, moderate activities such as table tennis, heavy gardening and easy swimming, vigorous activities such as basketball, soccer and running were added to the physical activity section. All questionnaires were administered face to face with 1:1 researcher to participant/family member. Individuals with an intellectual disability were given the opportunity to answer the questions posed themselves, and assistance from family members was sought when required. The level of support required varied from individual to individual in this heterogeneous population. Research interviews typically took 60–90 min to complete.
Six-minute walking test
To ensure that participants were physically able to participate in the physical fitness walking test, all participants were required to complete a physical activity readiness questionnaire, which included recording resting heart rate, resting BP and recent cardiac history. All participants met the criteria and were deemed ready to complete the sub-maximal walking test. Participants completed the 6-min walk test, which is a widely accepted reliable and valid tool for measuring functional exercise capacity in people with disabilities (Casey et al., 2012; Nasuti et al., 2013; Vis et al., 2009; Waninge et al., 2011). It involves walking back and forth as quickly as possible on a flat, hard surface, along a straight path for 6 min. A 20-m flat surface was used throughout the study mainly for logistic purposes. It has been investigated for use as a predictor of morbidity and mortality (Alahdab et al., 2009) and has been used with clinical and healthy populations to assess functional capacity and cardiovascular fitness (Nasuti et al., 2013). It is inexpensive and is easy to set up and to follow. Following guidelines outlined by the American Thoracic Society (2002) on conducting the 6-min walk test, resting BP was taken prior to commencing the sub-maximal test. Participants were asked to remain seated for at least 15 min before the test began. After this time, we checked for contraindications, measured pulse and BP and made sure that clothing and shoes were appropriate. Our protocol stated that any individuals who had a resting heart rate of >120 bpm, or a systolic BP of >180 mm/Hg, or a diastolic BP of >100 mmHg were deemed unsuitable for the test and would be advised by the nursing team to seek further advice from their medical GP. All other standardized testing procedures published by the American Thoracic Society were adhered to during data collection in this study, with some modifications including 1:1 pacer and 15 s encouragement which were validated in a study with adults with an intellectual disability (Nasuti et al., 2013). The lead researcher called out instructions, while members of the research team accompanied participants on the walk, with the pace being set by the participant, not the researcher.
Anthropometry
The World Health Organisation STEPwise approach to Surveillance (STEPS) is ‘a simple, standardized method for collecting, analysing and disseminating data in WHO member countries’ (World Health Organisation, 2014). All measurements were taken twice and the mean was used for analysis. BMI was calculated using the Quetelet formula (weight (kg)/height2 (m2)). Waist measurements were taken at the narrowest point from the anterior view (or halfway between the rib cage and the superior iliac crest) at the end of a gentle expiration, with participants in a standing position.
Accelerometry
An objective measurement of physical activity was collected by inviting participants to wear an Actigraph (GT3X) accelerometer. It was worn over the right hip on an elasticized belt for 7 days. Participants were asked to wear the device while they were awake and to take it off while swimming/bathing or doing contact sports. Monitors were collected by study investigators either at the home of participants or in their service provider. Raw accelerometer counts were downloaded using ActiLife software (version 6.11.3) and used to calculate the time spent in light-, moderate- and vigorous-intensity physical activity and sedentary behaviour.
Data analysis
Self-report questionnaire
Within the self-report questionnaire, participants reported how many days they completed tasks at mild, moderate or vigorous intensities over the previous 7 days. They also reported how much time was spent doing each activity. From this, the average minutes spent doing light, moderate and vigorous activity reported per day was calculated by multiplying the number of days by the number of minutes and then by dividing by 7 days. Moderate to vigorous physical activity was calculated by adding the moderate and vigorous activity scores together.
The 6-min walk test
Scores were calculated by adding up the total distance (in metres) covered by the participant within 6 min, with the greater the distance covered indicating the greater fitness levels.
Anthropometry
BMI was categorized according to WHO (2006): normal weight 18.5–24.99 kg/m2, underweight 15–18.49 kg/m2, overweight 25–29.99 kg/m2 and obese BMI >30 kg/m2. Participants were divided into three groups according to their age: group 1: 16–24.99 years; group 2: 25–44.99 years; group 3: 45–64.99 years. BP was classified into six groups following the Irish Heart Foundation classification: normal, pre-hypertension, high stage 1, high stage 2 and hypertensive crisis.
Accelerometry
Accelerometer data were collected from 107 participants; however, a minimum of four valid days was required for inclusion in this study. A valid day was defined as having 10 or more hours of wear time. Non-wear time was defined by an interval of at least 60 consecutive minutes of zero activity counts (Troiano et al., 2008). Counts of minutes in sedentary, light-, moderate- and vigorous-intensity physical activity were calculated using Freedson adult cut-points (Freedson et al., 1998). Minutes of physical activity accumulated per level of activity were summed. In order to get average minutes per day, this figure was then divided by the number of calendar days the participant wore the monitor for a minimum of 10 h.
Health profile score
This was calculated for each participant by creating a new variable consisting of summed scores from BMI, BP, meeting ≥30 min moderate to vigorous physical activity daily by self-report, and distance walked in the sub-maximal fitness test. BMI categories were each given a value; normal weight (1), underweight (0.5), overweight (0.5) and obese (0). BP categories were scored as normal (1), pre-hypertension (0.66), high stage 1 (0.33), high stage 2/hypertensive crisis (0), meeting moderate to vigorous physical activity guidelines was scored as healthy (1) and unhealthy (0). Distance covered in the 6-minute walk test was divided into four quartiles (Q); starting with the furthest distance and scored as Q4 (1), Q3 (0.66), Q2 (0.33) and Q1 as 0. The optimal score for each of the four categories was 1 so when summed together, the health profile score ranged from a minimum of 0 (the most unhealthy) to a maximum score of 4 (the most healthy).
All data were analysed using SPSS version 21 with alpha set at p < 0.05. Where participants had incomplete data for a given variable, participants were excluded from analysis of this variable only. Descriptive statistics were calculated via means, standard deviations, minimums, maximums and percentages where appropriate. One-way between-groups analyses of variance (ANOVAs) were used to investigate differences in moderate to vigorous physical activity accelerometer scores across the three age categories. A series of two-way between-groups ANOVAs were conducted to explore the impact of SOI participation and gender on moderate to vigorous physical activity questionnaire and accelerometry data, fitness levels measured by the distance walked in a modified 6-minute walking test, and differences in health profiles of SOI/non-SOI participants.
Results
Of 146 participants, Eight per cent of the total invited participated in the research (n = 146). Table 1 shows the number of people who took part in the various measures within the study and a breakdown of SOI vs. non-SOI involvement. Some reasons for non-participation included other family commitments, venues unsuitable to travel to, no family members present to attend sessions, elderly parents unable to attend.
Number of participants completing various study measures.

BMI: body mass index; SOI: Special Olympics Ireland.
Table 2 shows the mean ± SD of age and BMI of the total sample, and also of the breakdown by SOI and non-SOI participants. Of the 146 participants involved in the study, 101 (69%) were SOI athletes and 45 (31%) were non-SOI participants. Of these 146 participants, 58.2% were male and 42.8% were female, with a mean age of 33.01 ± 11.09 years. Just under half (47.5%) of the population were considered to have a mild intellectual disability, while 46.1% were considered moderate, and 6.4% were deemed severe (see Table 3). Information on gender, age, BMI and BP of participants overall, and by SOI participation status are given in Tables 2 and 3. Table 4 gives an overview of minutes of sedentary, light and moderate to vigorous physical activity (by accelerometry and self-report), percentage meeting the 30-min moderate to vigorous physical activity guideline, and physical fitness score overall, and by SOI participation status. Results of the one-way between-groups ANOVA demonstrated that there was no significant difference in moderate to vigorous physical activity accelerometer scores across the three age categories; F(2, 77) = 0.87, p = 0.422.
Descriptive statistics of mean (SD) age, BMI and health profile score of both SOI and non-SOI groups.
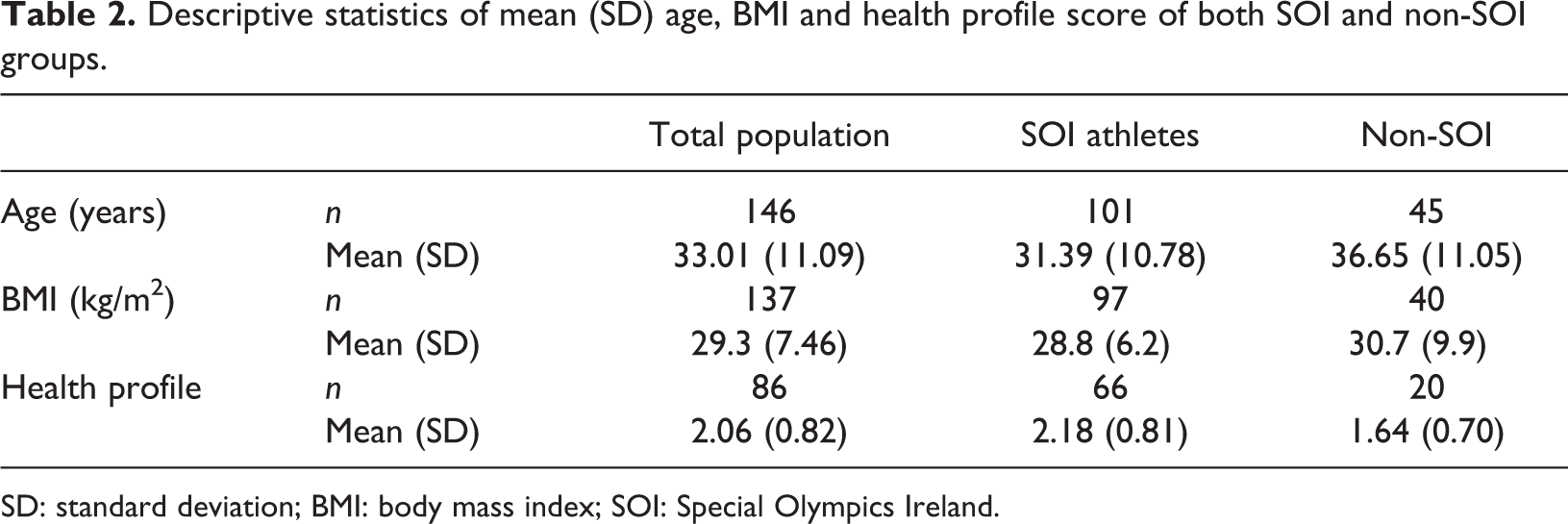
SD: standard deviation; BMI: body mass index; SOI: Special Olympics Ireland.
Frequency table of study participants.
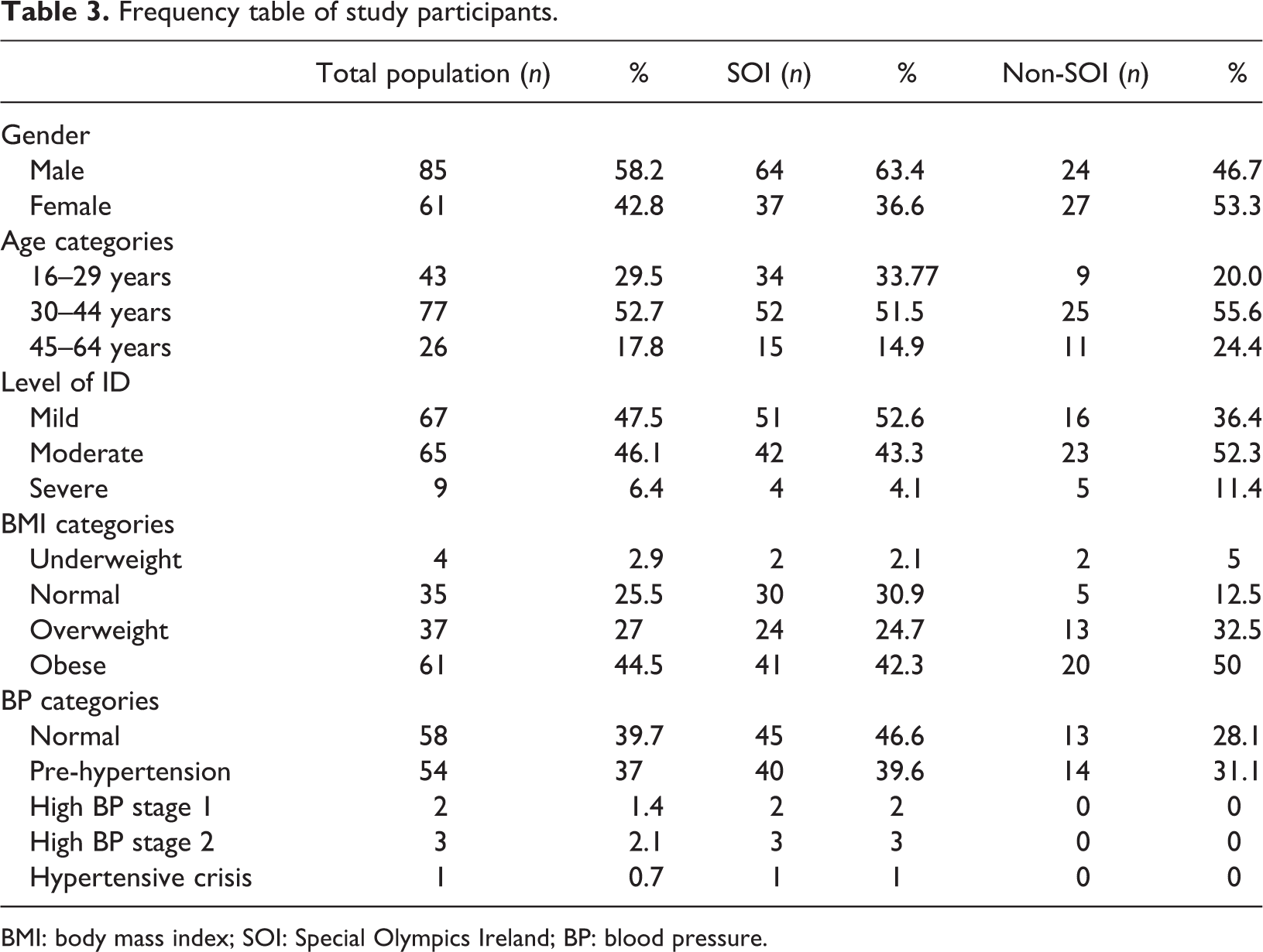
BMI: body mass index; SOI: Special Olympics Ireland; BP: blood pressure.
Mean (SD) physical activity and fitness data.
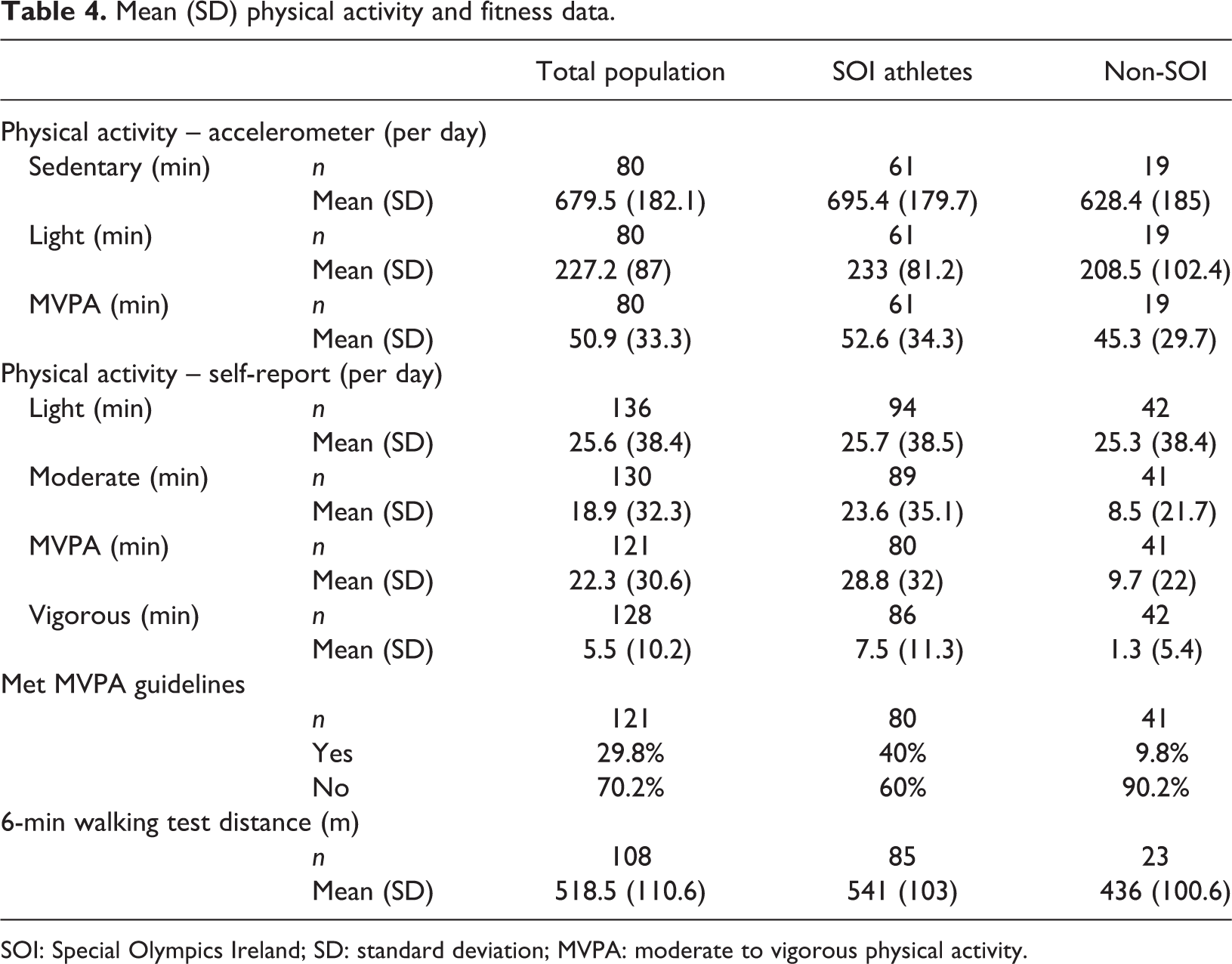
SOI: Special Olympics Ireland; SD: standard deviation; MVPA: moderate to vigorous physical activity.
When self-report minutes of moderate to vigorous physical activity were considered as can be seen in Table 4, again SOI participants recorded higher mean minutes of moderate to vigorous physical activity daily (28.8 ± 32) than non-SOI participants (9.7 ± 22). Results of a two-way between-groups ANOVA indicated that there was no significant interaction between gender and SOI status (F(2, 117) = 1.90, p = 0.171. There was a statistically significant main effect for SOI status however (F(2, 117) = 10.19, p = 0.002 with a medium effect size (partial η2 = 0.080), indicating that SOI participants accumulated significantly more minutes of moderate to vigorous physical activity daily than non-SOI participants. With regard to accelerometry data, SOI participants again recorded more mean minutes of moderate to vigorous physical activity daily (52.6 ± 34.3 min) than non-SOI participants (45.3 ± 29.7 min). Results of a two-way between-groups ANOVA show that this difference was not significant; however, the interaction between gender and SOI status was non-significant, F(2, 76) = 0.159, p = 0.691, and there was no main effect for either gender, F (2, 76) = 0.936, p = 0.336 or SOI status F(2, 76 = 0.384, p = 0.537).
Similarly, with reference to the physical fitness data, results indicate that the interaction effect between gender and SOI status was not significant, F(2, 104) = 0.787, p = 0.377, but there was a significant main effect for SOI status, F(2, 104) = 16.34, p = 0.000, partial η2 = 0.136. As can be seen from Table 4, this significant effect points to a significantly greater distance score of SOI participants (541 ± 103 m) compared to non-SOI participants (436 ± 100.6 m). Results of the two-way ANOVA investigating difference in the health profile show that there was no significant interaction between gender and SOI status, F(2, 82) = 1.33, p = 0.253 but that again there was a significant main effect for SOI status, F(2, 82) = 6.4, p = 0.013, with SOI participants scoring a significantly higher overall health profile (2.18 ± 0.81) than non-SOI participants (1.64 ± 0.70).
Discussion
Seventy two percent of the study population were classified as being overweight or obese which is consistent with findings from the IDS-TILDA study which found that 77% of adults over 40 years of age with an intellectual disability in Ireland, who had weight and height measurements taken, were overweight or obese (McCarron et al., 2014). These high figures are not specific to Ireland but are evident worldwide (Fisher, 2004; Moran et al., 2005; Yamaki, 2005). There was also a higher prevalence of overweight and obesity in the study population compared to the general population (SLÁN, 2007 report), of whom 61% are overweight or obese (Ward et al., 2009).
Participants in the current study spent most of their waking hours sedentary (71%), accumulating a mean 679.5 ± 182.1 sedentary minutes per day (11.3 h/day). These findings are consistent with previous research in relation to sedentary behaviour and people with intellectual disabilities (Messent et al., 1999; Phillips and Holland 2011; Temple and Walkley, 2003) although sedentary behaviour is a common problem across all populations. Those with intellectual disabilities tend to accumulate more time in sedentary behaviour compared to the general population.
The current study indicates that only 29% of the population self-reported sufficient moderate to vigorous physical activity minutes to meet the >30-min moderate to vigorous physical activity guidelines (American College of Sports Medicine, 2011). While no other Irish studies have been identified using similar methodologies for people with intellectual disabilities, the SLÁN 2007 study (Ward et al., 2009) used a similar self-report method as a means of gathering data on moderate to vigorous physical activity in a representative sample of the general population. Fifty five percent of the general population reported being ‘physically active’, meaning that they completed exercise or sport 2–3 times per week for a minimum of 20 min or engaged in more general activities, such as walking, cycling or dancing, 4–5 times per week accumulating to at least 30 min per day. In a study in Canada with 103 adults with mild to moderate intellectual disabilities aged 19–65 years, 64% reported that they participated in five or more bouts of moderate to vigorous physical activity per week; however, only 18% of participants accrued the recommended duration of 30 min moderate to vigorous physical activity per day according to pedometer data (Stanish and Draheim, 2005).
With regard to accelerometry data, those in SOI accumulated 52.6 ± 34.3 min moderate to vigorous physical activity per day in the current study compared to 45.3 ± 29.7 for non-SOI participants. Although the current study suggests that those with intellectual disabilities accumulate more minutes moderate to vigorous physical activity than previous research in the general and intellectual disability population perhaps with a larger sample size and a greater representation of people with severe and profound intellectual disabilities, results may have been different.
Unfortunately, fewer participants consented to wear the accelerometer and so less data is available on this element of the study, thereby reducing the representativeness of this element. Although the pattern is similar in both measures with SOI participants accumulating more mean minutes of moderate to vigorous physical activity per day than non-SOI participants, the large differences between accelerometer (50.9 ± 33.3 min) and self-report (22.3 ± 30.6 min) measured moderate to vigorous physical activity must be noted. It is unusual for accelerometer activity to be higher than self-report activity with self-reporting more commonly seen to overestimate physical activity (Klesges et al., 1990; van de Mortel, 2008). It must be considered, however, whether the cut-point thresholds used, which were developed for the general population (Freedson et al., 1998), are relevant and appropriate for this population. The high levels of accelerometer measured activity found within this population sample may have also been influenced by the fact that people with severe and profound intellectual disabilities were under-represented in this study population, thereby potentially favouring a more active sample. Robertson et al. (2000) suggest that levels of inactivity have been associated with more severe levels of intellectual disability. Those with more severe intellectual disabilities have greater limitations in completing activities of everyday living (Jones et al., 1999). Caution should be exercised in generalizing the current findings due to the limitations of a small sample size as well as the lack of severe and profound participants with intellectual disabilities.
Issues with conducting interviews and use of self-reporting for the intellectual disability population have been reported in the literature (Finlay and Lyons, 2001; Stalker, 1998). In order to gain comprehensive information, it is sometimes not merited to gain this directly from the individual themselves. For example, a common problem with self-reporting in the intellectual disability population is questions with content about time and providing a judgement of frequency (Booth and Booth, 1994). In the current study, participants were asked about how often they took part in different forms of activity. Self-reporting of activities was low; this may be because they were inactive but may also be a product of not being able to relay this type of information correctly. A balance needs to be found, and people with intellectual disabilities need to be able to have a voice. However, more consideration needs to be placed on creating validated questionnaires and highlighting specifically the population for which the instrument is designed.
Given the low sample size in the non-SOI group whose accelerometer data fit the inclusion criteria (n = 19), it is perhaps unsurprising that no significant difference in the moderate to vigorous physical activity level by an accelerometer was found in the current study, despite the descriptive statistics suggesting higher accumulation in the SOI group overall. When we consider self-report minutes of moderate to vigorous physical activity, those in SOI (28.8 ± 32) were found to be significantly more active (p = 0.002) than non-SOI participants (9.7 ± 22). In the current study, self-report data suggest that a large number of participants (70%) overall do not accumulate sufficient minutes of moderate to vigorous physical activity to meet the >30 min per day moderate to vigorous physical activity guideline for promoting better health. Of the two groups, 40% of SOI participants reported meeting the guidelines, compared to only 10% non-SOI participants. Findings are consistent with the TILDA report in 2014, which also showed that 70% of adults with intellectual disabilities reported engagement in low levels of activity, levels not likely to result in health benefits (McCarron et al., 2014). This compares with 59% of the general population who reported not meeting the moderate to vigorous physical activity guidelines in Ireland in the SLÁN 2007 report (Ward et al., 2009).
The mean distance covered in the 6-minute walking test in the current study was 518.5 m ± 110.6, with SOI participants walking a greater distance significantly (541 ± 110.6, p = 0.000) than non-SOI participants (436 ± 100.06). These compare to a study with a healthy older adult population who reported the mean distance score as 631 ± 93 m (Troosters et al., 1999). A study with people with heart failure reported the mean distance as 419 ±120 m (Faggiano et al., 1997), and in a study with people with chronic obstruction pulmonary disease, the mean distance was reported as 369 ± 18 m (Onorati et al., 2003). A study with participants who had severe multiple disabilities reported the mean distance as 389 ± 107 m (Waninge et al., 2011). With the population in the current study being people with mostly mild and moderate intellectual disabilities, it is not surprising that they scored higher distances than those with severe intellectual disabilities, chronic obstruction pulmonary disease and heart failure participants. It would be expected for those in the current study to score lower levels than the general population as people with intellectual disabilities are less physically active than the general population which should in turn impact on physical fitness scores.
Differences in test protocols must be considered when comparing between studies using the 6-minute walk test, which may all have the potential to affect walking distance of study participants, for example, familiarization sessions, pacers, level of encouragement and varying distances used. Familiarization sessions have been recommended for people with an intellectual disability (Rintala et al., 1995, Waninge et al., 2011) with Casey et al. (2012) finding an increase in walking distance after two practice walks. This emphasizes the need to account for a learning effect among people with disabilities. It is important to note that this was not feasible in the current study which may be seen as a limitation and as such the figures presented may underestimate to a small extent the true distance capability of individuals.
Consistent with previous research for people with intellectual disabilities, pacers and additional encouragement were used in the current study (Beets et al., 2005; Nasuti et al., 2013; Rintala et al., 1992; Waninge et al., 2011). The use of 1:1 pacers adds to the staffing demand so future researchers may wish to examine the impact of removing pacers or increasing the participant-to-staff pacer ratio. In order to prevent affecting the distance walked, the protocol of Waninge et al. (2011) was followed, where individuals with an intellectual disability self-paced with pacers walking beside them. Encouragement was also given every 15 s in accordance with the modified 6-minute walk test protocol set out by Nasuti et al. (2013).
Depending on the study, there are different protocols used in terms of the length of the walking test. The American Thoracic Society (2002) suggests a 30-m flat surface for optimal performance as shorter distances increase the amount of turns needed, therefore potentially negatively affecting the distance walked. However, findings from a multicentre study revealed no significant effect on walking distance of straight courses ranging from 15 to 50 m (Weiss, 2000). The current study used a 20-m flat surface for logistical purposes. The authors of this study recommend the modified 6-minute walk test as a straightforward and practical test with minimal time, space, measurement and equipment requirements.
In relation to BP, only 4% of the participants in the current study had a BP measurement in the hypertensive range. While acknowledging the limitation of single measurement, it is surprising that the majority of this population had BP in the normal or pre-hypertensive range because individuals who present as overweight or obese, like the majority of this study sample, are considered more at risk of having hypertension (Sturm, 2002). These findings are consistent with findings from the TILDA study, however, which found that rates of hypertension were 50% lower in individuals with intellectual disabilities (18%) than the general population (37%) (McCarron et al., 2014). The findings from the current study are promising in that having a lower BP may be associated with the high physical activity levels of individuals in the study. Previous research has shown that like the general population, physical activity can reduce BP for individuals with intellectual disabilities (Calders et al., 2011; Pett et al., 2013).
Within the current study, 86 participants provided information on all four categories that made up the health profile scores including BMI, BP, fitness test and meeting the recommended >30-min moderate to vigorous physical activity per day. This score is considered meaningful in that it could potentially be an important indicator of overall health and quality of life of individuals with intellectual disabilities, as such indicators can gather comparable health information and thus identify health inequalities within this population (Walsh, 2008). It is worthwhile noting that those in SOI had a significantly (p = 0.013) more positive health profile score (2.18 ± 0.81) than those not in SOI (1.64 ± 0.70). To the authors’ knowledge, there are no similar studies available in the literature to make direct comparisons.
Similarly, to the best of the authors’ knowledge, no studies have been published investigating the impact of SOI participation on physical activity and fitness levels of individuals with intellectual disabilities in Ireland. Previous studies have examined the effect of physical activity on different aspects of health in persons with intellectual disabilities (Bartlo and Klein, 2011; Escobar et al., 2013; Rimmer et al., 2004) and have consistently shown a positive impact of physical activity participation in health and well-being. For example, Pett et al. (2013) conducted a 12-week healthy lifestyle intervention with 30 obese home-dwelling young adults with intellectual disabilities. The intervention consisted of health education and physical activity sessions that took place twice per week (1.5 h/session) for a total of 36 h. Compared with controls, at a 3-month follow-up, the intervention group demonstrated significant improvements in BP, weight and balance (p = 0.05). To surmise, physical activity participation has been shown to have a positive physical health impact on the lives of people with an intellectual disability.
In the current study, sample size was small (n = 146), which was primarily due to recruitment challenges. There was also a lack of representation of people with severe and profound intellectual disabilities. As the main focus of the study was on SOI participants and recruitment resulting in mainly people with mild to moderate intellectual disabilities, generalizability of findings to the boarder intellectual disability population is limited. However, causality cannot be determined as it could be argued that people who take part in SOI do so because they are fitter and more physically active. Further longitudinal research is warranted to determine whether those with increased physical activity and better health profiles opt to participate in SOI, or whether this increased physical activity and better health profile and is as a result of participation. Future research, with a representative sample of people with intellectual disabilities, is essential to further examine the physical activity habits and fitness levels of adults with intellectual disabilities ranging from mild to profound intellectual disabilities and to further assess the health impact of SO participation for the intellectual disability population. The health profile score or a similar tool may be useful for future research to assess and compare the health status of individuals with disabilities and other groups. It may highlight inequalities in health and therefore be useful when planning interventions and indeed evaluating their effectiveness. Research is also needed to obtain the most effective objective measure of physical activity for individuals with intellectual disabilities. Consideration also needs to be placed on creating validated questionnaires for self-reporting within the heterogeneous intellectual disabilities population, highlighting specifically the population for which the instrument is designed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Authors received funding from the Iris O'Brien Foundation.