
Abstract
Pain is a multidimensional and subjective experience, and an ideal pain management regime needs to be comprehensive, integrative and involve all relevant persons. Multimodal interventions may include pharmacological, physical, social, psychological and spiritual approaches in order to address pain management at a molecular, functional, behavioural, cognitive and affective levels. Pain management interventions will vary according to pain aetiology, patient characteristics and preferences. In keeping with best practice guidelines for effective pain management, a structured approach incorporating an effective assessment of pain by the healthcare professional, identification of the source and type of pain and accurate documentation is essential. This article focuses on pharmacological and non-pharmacological pain management for individuals with intellectual disability.
Keywords
Introduction
In ancient times, pain was considered to be an emotion or even a visitation from an evil spirit and this view persisted until the latter half of the 17th century when Descartes (1664) described what is today still referred to as a ‘pain pathway’. Descartes illustrated how particles of fire, in contact with the foot, travel to the brain and he compared pain sensation to the ringing of a bell. This theory remained largely unchallenged until 1965 when Melzack and Wall published the gate control theory, which significantly revised and redirected our understanding of pain and its management (Carr and Mann, 2000). It has been established that people with intellectual disability are at an increased risk of experiencing pain (Beacroft and Dodd, 2010; Blyth and Lee, 2011). Given the complex nature of pain (Faull et al., 2012), it follows that the management of pain for individuals with intellectual disability is challenging and frequently unaddressed or poorly addressed (Breau and Camfield, 2011; Massaro et al., 2013). This poor outcome is not surprising, given that in pain management communication and self-report is key (Findlay et al., 2014). However, the apparent lack of determination to overcome such obstacles reflects poorly on society and a health service that professes to uphold the individual right to equality, justice, fairness and access to health (McGuire and Kennedy, 2013; Ward et al., 2010).
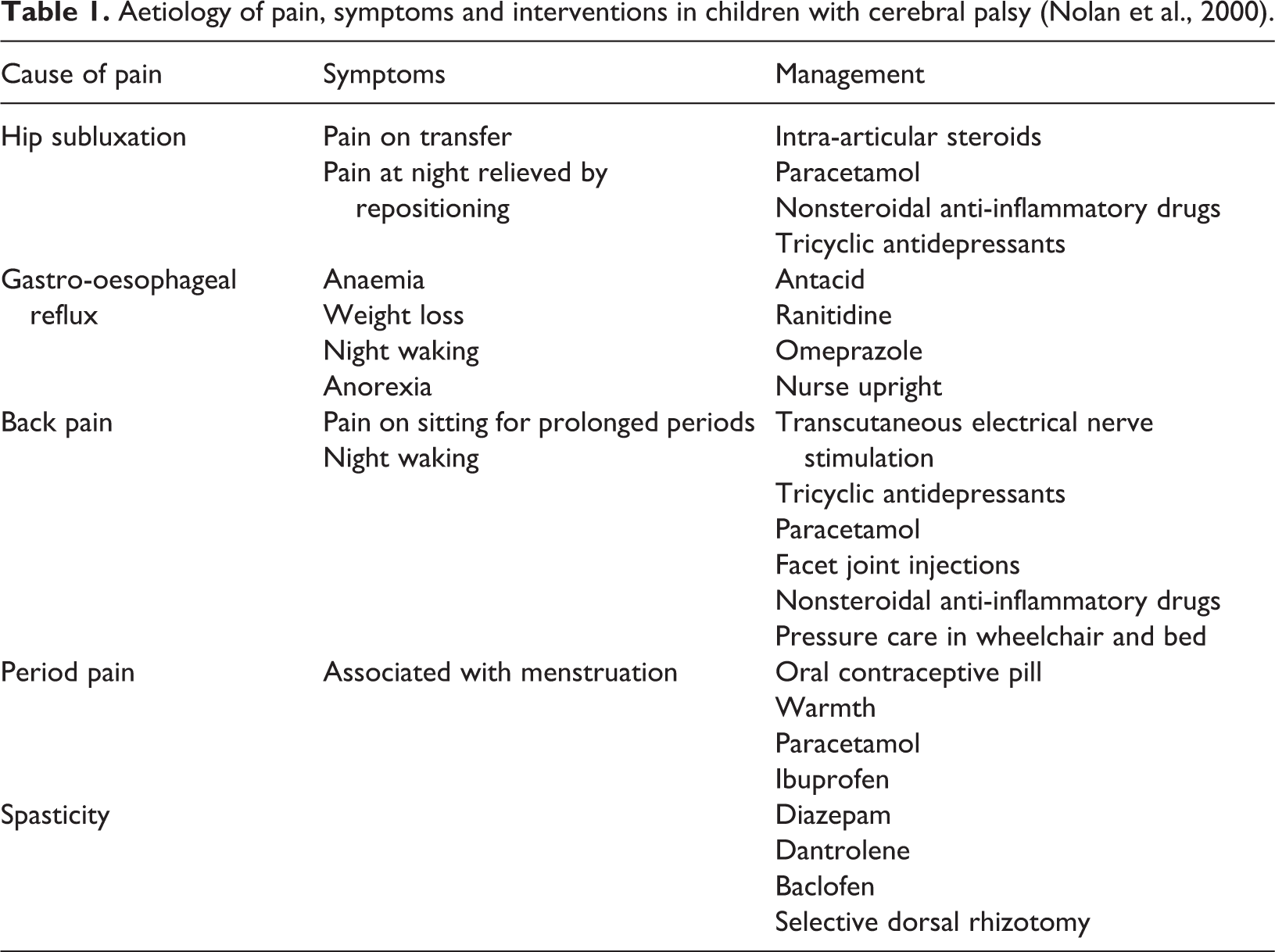
Pain assessment and management have been the focus of interest internationally; however, research into pain assessment among non verbally communicating intellectually disabled people has been very limited (Kankkunen et al., 2010). Nurses have difficulties in interpreting the individual’s behaviour and, as a consequence, pain among individuals with intellectual disability often remains unidentified (Breau and Burkitt, 2009; McKenzie et al., 2012). Pain management for this group is difficult (Malviya et al., 2005, Zwakhalen et al., 2004) and compounded by insufficient assessment methods and nurses’ insufficient knowledge and education (Breau et al., 2003; Kankkunen et al., 2010). An understanding of the aetiology of pain is essential for effective management. Nolan et al. (2000) identified aetiology of pain, symptoms and treatment in children with cerebral palsy, which are helpful when working with this population (Table 1). However, Kankkunen et al. (2010) identified that only 8% of the nurses working with people with intellectual disability had undertaken education for pain management.
Aetiology of pain, symptoms and interventions in children with cerebral palsy (Nolan et al., 2000).
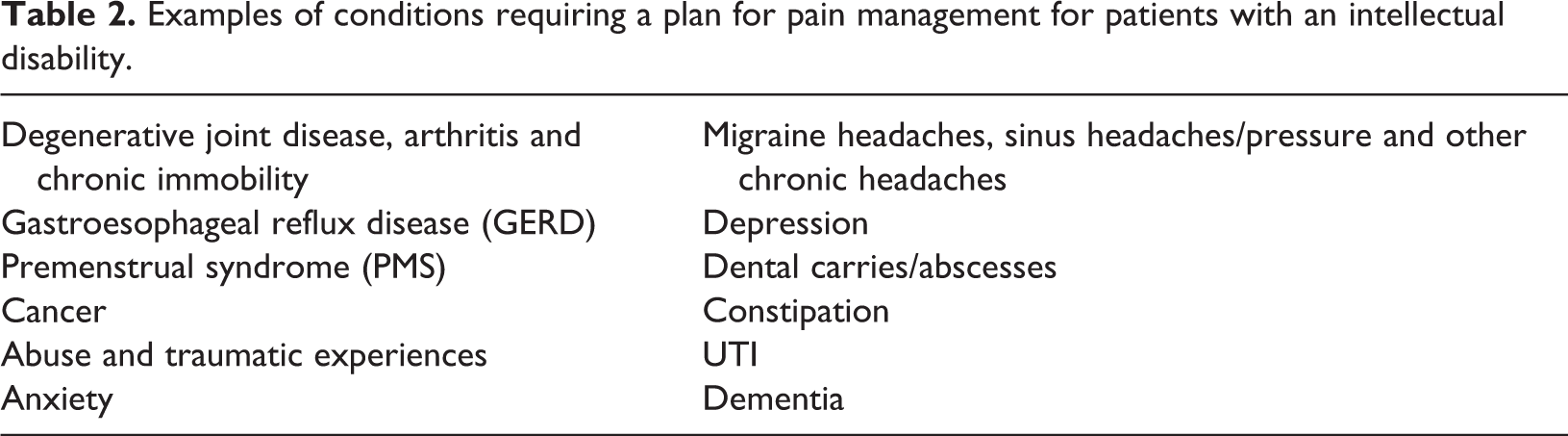
The authors identify several common conditions for which individuals with intellectual disability require a pain management plan (Table 2). Awareness of these conditions is important as individuals with intellectual disability experience pain often on a daily basis (Stallard et al., 2001), which becomes chronic (Breau et al., 2003) for a long duration before it is recognized (Hadden and von Baeyer, 2002). To effectively manage pain, the skills of the nurse and family are important in identifying and managing pain in this vulnerable group of individuals (Davies, 2010). Heath (1998) argued that treatment of pain may be classified as the three Ps for the one big P namely physical, psychological and pharmacological treatment of pain. While this is a useful pneumonic, it is important to also consider Saunders (1967) concept of total pain and include social and spiritual influencing factors. These five factors interweave to create the complex picture of an individual’s experience of pain.
Examples of conditions requiring a plan for pain management for patients with an intellectual disability.
Within pain management, when working with individuals with intellectual disability as is the case generally, it is important to first identify the cause of pain and implement appropriate intervention incorporating the administration of appropriate analgesia relief. While the cause of pain may be identified, for example, acute pain as exhibited by a sudden change in behaviour, it may not be possible to immediately identify the source or specific location of the pain for the individual, given the nature of intellectual disability and presence of communication difficulties. As the presence of pain is common in individuals with intellectual disability and it is not always easy to identify the cause/source, when pain is suspected, treatment with analgesia should commence with observation to see if behaviour improves. When behaviour improves, pain is then the likely cause and analgesia administration continues until the cause can be identified and treated. In addition, non-pharmacological treatments can enhance pain management regimes and while the evidence base is difficult to prove, the subjective nature of pain often leads to the subjective nature of pain management. This article considers pain management for persons with intellectual disability, utilizing the concept of total pain and is the third in a series that also addresses pain physiology and pain assessment.
Pain management interventions
Acute pain works as a defence mechanism and alerts the person to injury and/or disease (Taverner et al., 2014). Pain is often difficult to treat and frequently requires ongoing assessment, review and titration and/or trial of drugs before a satisfactory outcome can be achieved (Taverner, 2014). Faull et al. (2012: 126) describe seven approaches in the management of pain, the first of which is explanation, ‘a patient who understands the cause of their pain and the nature and expectations is likely to cope better’. However, individuals with intellectual disability may not be able to understand explanations and drawings, and pictures or models may assist where appropriate. The other pain management approaches include raising the pain threshold and increasing tolerance, modify lifestyle – assess for aids and adaptations, modify pathological processes, modify pain perception, less frequently – interrupt pain pathways and psychological interventions. However, the applicability of these to individuals with intellectual disability needs to be considered according to the individuals’ level of understanding and communication.
The first step in the management of pain is a comprehensive assessment (Breau and Burkitt, 2009). Following assessment and prior to establishing any intervention strategy, a management plan needs to be developed in partnership with the person and his/her carers (Dubois et al., 2010; Herr et al., 2011). It is important that everyone understands the difficulty of managing pain and that trial of several therapies may be required before a favourable outcome is achieved (Attal et al., 2006; Fink and Gates, 2010). In addition, it is particularly important not to try more than one new therapy/intervention at a time so that the intervention may be reviewed and evaluated (Wells et al., 2008). In other words, multiple interventions at any one time may render the nurse unable to distinguish the appropriateness and usefulness of an intervention (Helms and Barone, 2008). Pain management requires a multidimensional approach that includes pharmacological and non-pharmacological treatment modalities to manage pain and associated comorbid medical, psychological and psychosocial conditions (American Academy of Pain Medicine 2013; Chou et al. 2009). A multidimensional approach to the management of pain ensures that nurses focus on quality of life indicators and not just reduction of pain, for example, an individual may have a mood, anxiety, depression or sleep disorder that need to be addressed (Gore et al., 2012; International Association for the Study of Pain, 2010). In addition, relevant individuals such as family/carers and the individual with intellectual disability themselves should be included in the assessment, management and evaluation (Fink and Gates 2010; Lester et al., 2011).
Pharmacological interventions
The goal for effective pain management with medication is to relieve pain while minimizing side effects. All medications used to treat pain have side effects, including over-the-counter drugs. Many patients will experience ‘mixed pain’, a combination of both neuropathic and nociceptive pain, and this undoubtedly adds to the complexity of pain management. Assessment is therefore key in selecting the appropriate analgesic. For chronically painful conditions, long-term use of medication may be necessary and the non-medication techniques become even more important. A clear pain management plan cognizance of the different factors influencing the persons’ perception of pain should be documented and all persons involved in the individuals’ care should be familiar with it. An essential element of this plan is that regular review should be evident and the term ‘regular’ should be identified in terms of frequency. The intention of this article is not to provide directions to the pharmacological management of pain but to highlight the need for effective assessment in establishing the type and source of pain in order that the most effective analgesia and intervention for the pain type can be commenced.
The guidelines for the pharmacological management of neuropathic pain published by National Institute for Health Care Excellence NICE (2013) recommend the use of co-analgesics such as antiepileptics and antidepressants, as well as topically applied capsaicin products. According to the NICE (2013), first-line treatment for all neuropathic pains except trigeminal neuralgia (TN) should be tricyclic analgesics (TCAs), for example, amitriptyline, selective serotonin and norepinephrine reuptake inhibitors (SSNRIs), for example, duloxetine and anti-epileptics, for example, gabapentin and pregabalin. For patients with TN, NICE (2013) recommends carbamazepine as initial treatment and notes that if this is not effective or tolerated, the patient should be referred to a pain specialist for review and treatment. For neuropathic pain, surgical intervention on appropriate nerves may provide further pain relief if drugs are not wholly effective. Evidence suggests that neuropathic pain can be more severe than nociceptive pain, and it may also be less responsive to conventional analgesic techniques (McQuay, 2002). Management of neuropathic pain may require a trial of several strategies and should include pharmacological and non-pharmacological approaches (Attal et al., 2006; NICE, 2013).
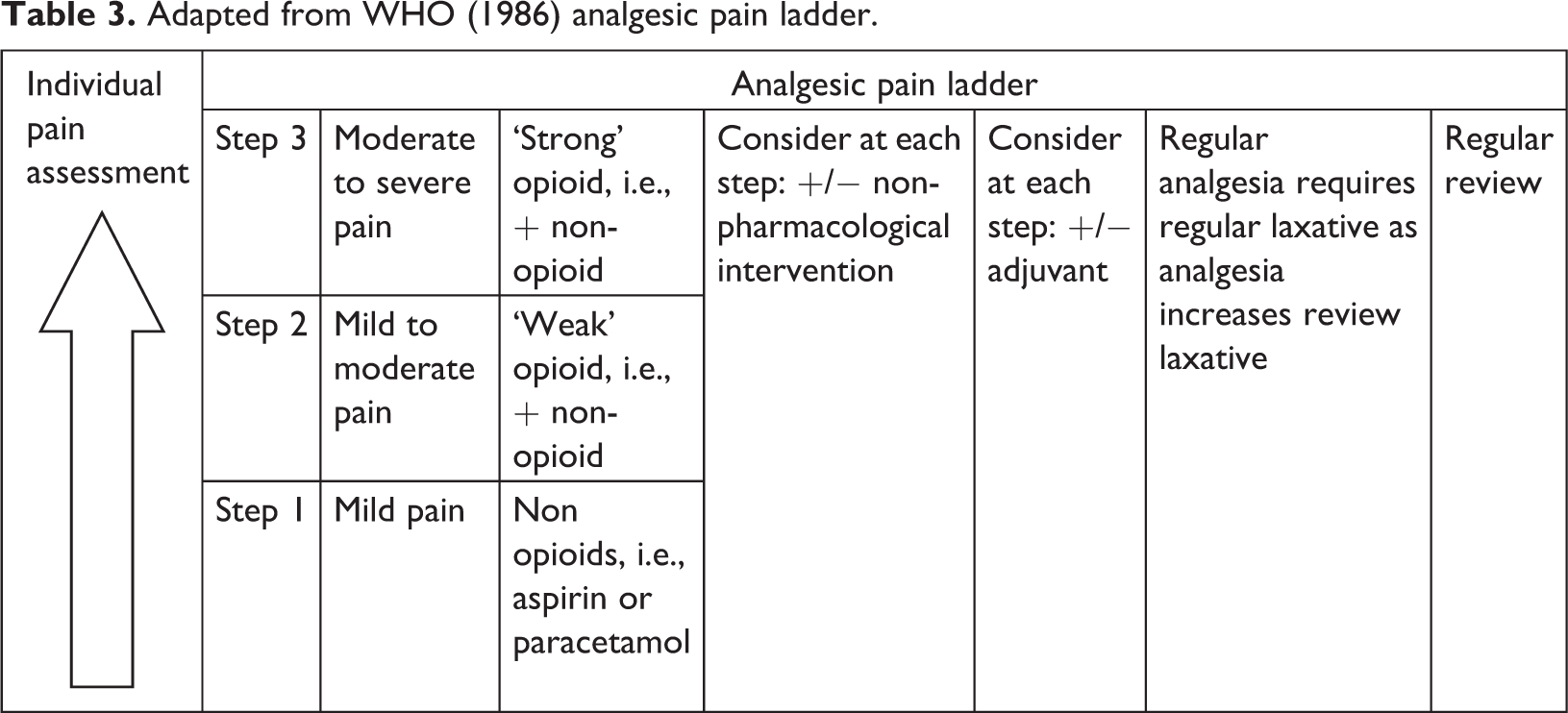
The World Health Organization (WHO) (1986, 1996) developed the analgesic pain ladder, which is based on a set of principles aimed to originally guide the prescribing of analgesia in cancer pain. The principles are to administer analgesia ‘by the clock’ (regularly), ‘by the mouth’ orally and ‘by the ladder’ with additional phrases as ‘for the individual’ ‘attention to detail’ and ‘frequent review’. It is recommended that pain should be reassessed and reviewed 30 min after administration of analgesics (Gordon et al., 2008). Over the years, the ladder has provided an effective guide in the management of cancer pain either nociceptive or neuropathic and the stepwise approach using a limited number of drugs is equally applicable to the management of chronic pain (Bennett et al., 2005). If pain occurs, there should be prompt assessment using a recognized and appropriate pain scale for the individual according to the analgesic pain ladder (Table 3). For mild pain, step 1: ‘non’ opioids are prescribed. If pain persists or increases, move to step 2: ‘weak’ opioids, that is, codeine in addition to non-opioid); finally, step 3: strong opioids such as morphine, until the patient is free of pain. From step 1 upward, in order to reduce symptoms that the patient may experience concurrent with pain, additional drugs described as ‘adjuvants’ – should be used (Pasero and McCaffery, 2011). Medications, whose primary action may not be analgesia, may be used according to the type of pain being treated, that is, TCAs, anticonvulsants, nonsteroidal anti-inflammatory drugs, SSNRIs and steroids. More recently, it is advised that non-pharmacological approaches to pain management should be included from step 1 and upwards (Faull et al., 2012). For some patients where pain is severe, the physician may move directly from step 1 to step 3 (Faull et al., 2012).
Adapted from WHO (1986) analgesic pain ladder.
To move towards freedom from pain, drugs should be given ‘by the clock’, that is every 3–6 h, rather than ‘on demand’ and a laxative introduced and increased accordingly when the individual is taking regular analgesics. This three-step approach is inexpensive and 80–90% effective (WHO, 1996). However, given that this tool was introduced almost 30 years ago, it should also be recognized that knowledge of pain, opioid analgesia and other pain management options have developed considerably, hence there have been calls in the literature for the revision of this tool (O’Connor and Dworkin, 2009). For example, it has been argued that the designation of ‘weak’ and ‘strong’ opioids may not be as meaningful as understanding the characteristics of specific opioid agents and their appropriate doses. O’Connor and Dworkin (2009) note that this does not negate the value of the generalized WHO analgesic pain ladder, but they advise that healthcare professionals should use it according to the needs of the individual patient and modify accordingly.
While the WHO ladder is a suitable guide for pain management, Cringles (2002) identified that while 64% (n = 49) of nurses were aware of the WHO ladder, only 49% (n = 37) used the recommendations. Furthermore, documentation of pain management and its effectiveness is based on systematic use of a validated pain assessment tool and nurses should be competent in the use of pain assessment tools appropriate for the client group and appreciate the importance of evaluating the effectiveness of the pain intervention (Herr et al., 2011; Kankkunen et al., 2010). It is essential that pain assessment and interventions are well documented as documentation of pain assessment and management provides the basis for continuity of care (Kankkunen et al., 2010).
Although there is little research examining the pharmacological treatment of pain in individuals with intellectual disability, medication choices should be dictated by the individual’s symptoms and based on the same principles applied to those without intellectual disability (Breau et al., 2011). However, Koh et al. (2004) and Long et al. (2009) identified that individuals with intellectual disability have similar opioid requirements to a matched group undergoing surgery and individuals with intellectual disability received less opioid intraoperatively as compared to non-intellectual disability individuals.
Non-pharmacological interventions
Non-pharmacological pain management interventions are methods to decrease pain without medication or as a supplement to medication and each person may respond to these interventions differently. They aim to treat affective, cognitive, behavioural and sociocultural dimensions of pain (Demir, 2012; Fink and Gates 2010). The body’s naturally occurring painkillers known as endorphins are released, for example, following a period of exercise and these endorphins interact with receptors in the brain that reduce the perception of pain. Endorphins are manufactured in the nervous system to be released in response to stimulation by neurotransmitters and diminish the perception of pain. The neurons that receptor endorphins bind to are the same ones that bind some pain medicines. However, unlike with morphine, the activation of these receptors by the body’s endorphins does not lead to addiction or dependence (Briggs, 2010). Endorphins also trigger a positive feeling, similar to that of morphine, where the person may feel euphoric and energized with a positive outlook on life (Helms and Barone, 2008).
From a mathematical perspective, the benefits of triggering release of endorphins could be simply explained as follows: 1000 pain messages start out from an injured toe on their way to the brain. If endorphins block 90%of them, only 100 messages may get through the spinal cord gate. Of those, approximately 20 will make it through to the conscious brain. So the injured toe generated 1000 ‘ouches’ worth of pain, but the brain registered only 20 of them. This is why it is so important for nurses to encourage individuals to produce as many naturally produced endorphins as possible. Examples of naturally producing these endorphins would be exercise, laughter, music and dance. Other non-pharmacological methods of managing pain include social, spiritual, psychological and physical techniques.
Social techniques
Social interventions for people with intellectual disability experiencing pain may relate to changing or altering the environment, having familiar carers available, distraction, humour, leisure activities, divisional therapy, oils and supporting the person through any changes in school or work (Breau et al., 2011; Slifer et al., 2011). These serve to promote comfort, relaxation and engagement of the person with intellectual disability so they may perceive less pain. Also for an individual with intellectual disability staff turnover, lack of continuity and change can cause anxiety and worry, making the person more susceptible to social pain (Turk et al., 2010). As continuity, consistence, familiarity and knowing the person are important aspects for person with intellectual disability. Distraction works by moving the attention away from the pain to reduce its severity, and methods include listening to music, watching television or reading a book (Demir, 2012; Slifer et al., 2011). This may help increase energy levels and improve mood and thereby trigger the release of endorphins. Use of oils or aromatherapy has been shown to help relieve pain by aroma oils reaching the lymph system by means of blood circulation and providing recovery by means of intercellular fluids (Deng and Cassileth, 2005; Jennings, 2004) and also providing means of relaxation.
Spiritual techniques
Spiritual interventions enable the person with intellectual disability to express him/herself through a medium that affords pleasure, comfort, peace and tranquillity, such as, music, singing, gardening, art, religious practices, and so on (Briggs, 2010). Carson (1989) describes spirituality as a universal human dimension that expresses itself through relationship, creativity, emotions and religion. Narayanasamy (1991) relates that a belief in self and others is characterized by the need for love and harmonious relationships and describes the concept as ‘the essence of our being’. These definitions appear to be universal in that they may be applied to persons who, due to cognitive impairment, cannot understand the term but require spiritual care none the less. For individuals with an intellectual disability, spirituality appears to be a neglected element of their pain management within the literature. However, given the overlap between the factors affecting the perception of pain (Saunders, 1967), the authors would argue that spiritual needs are frequently addressed albeit that the impact of spiritual caring on the perception of pain may go unobserved by the nurse. The need for love is a fundamental need, which begins at birth and continues to old age (Maslow, 1968). In addressing the spiritual needs and spiritual dimensions of pain, music, art, dancing, humour, leisure, religious practices and observations and prayer may be beneficial (Focht-New and Kelly, 2012; Masterson, 2011).
Psychological techniques
Psychosocial interventions aim to increase self-management, behavioural and cogitative change rather than directly eliminating the locus of pain (Kerns et al., 2011) and may include relaxation, breathing exercises, visualization and cognitive behavioural therapy (CBT). Like many chronic illnesses, persistent pain is complex and often does not respond fully to pharmacological management (Lewis et al., 2007; Melzack and Wall, 1965). As a consequence, a mixed approach is recommended that promotes a holistic approach to care (Temple et al., 2012). The gate control theory (Melzack and Wall, 1965) postulates that a ‘gating mechanism’ within the central nervous system can be open or closed, allowing or inhibiting the transmission of pain signals. The theory also proposed that the pain signal transmission can be influenced by emotions and thoughts. Psychological pain gates can be closed in numerous ways including by massage, distraction, work, music, humour, leisure activities, biofeedback, breathing exercises, visualization, guided imagery and relaxation, and these techniques are advised to increase control over pain and reduce distress (Breau et al., 2011; Engel et al., 2004). Within the general literature, a review of the use of complementary and alternative medicine for neuropathic pain concluded that evidence of the effectiveness of treatments such as acupuncture, herbal medicine, magnets, electro-stimulation and supplements was inconclusive and that no consensus could be reached (Pittler and Edzard, 2008).
Psychological management of chronic pain often incorporates a cognitive behavioural approach to care (White, 2001). A person who believes ‘my pain won’t harm me’ will experience less distress than someone who believes ‘my pain will drive me crazy’. There is growing evidence that belief about pain (Lame et al., 2005), fear of movement (Lewis et al., 2007; Vlayen et al., 1995) and pain-related fear (Crombez et al., 1999; Lewis et al., 2007) are actually more disabling than the pain itself and should therefore be considered throughout treatment. Clinical care of people with chronic conditions such as persistent pain should include providing information about the condition, coordinating services and helping the person/family set appropriate goals (Lewis et al., 2007; Stein 2005). Providing information has been found to affect learning, behaviour, self-esteem and person/family functioning (Lewis et al., 2007). The subjectivity of pain and the recognition of the complexity of pain perception, including significant intrapersonal and interpersonal variation, are recognized in contemporary models of pain such as the gate control theory, in which the emotional and cognitive aspects of pain perception are equally important, alongside the physical/biological aspects (McGuire and Kennedy, 2013). This has led to the development of a range of effective psychological interventions for pain management (Eccleston et al., 2009; McGuire and Kennedy, 2013). Evidence within the intellectual disability field includes the use of snoezelen for relaxation (Schofiled, 2002), relaxation for treating headaches (Michultke et al., 1988), biofeedback-assisted relaxation (Engel et al., 2004) and Cautela and Groden (1978) manual for progressive muscle relaxation addresses children with disabilities.
CBT has become the most widely used and widely researched psychological intervention for pain management. A number of major reviews (including Cochrane reviews) have confirmed the efficacy of behavioural and cognitive behavioural interventions for typically developing adults (Eccleston et al., 2009) and children with chronic pain (Eccleston et al., 2012). Although CBT has been used in modified format for the treatment of anxiety (Lindsay et al., 1997), depression (McCabe et al., 2006) and anger problems (Taylor et al., 2000; Willner et al., 2002), minimal research has been reported evaluating CBT for chronic pain in people with an intellectual disability. However, a novel case report on the treatment of a person with a mild intellectual disability, who had chronic pain, pointed to the potential for psychological treatments (Lewis et al., 2007). In addition, while McManus et al. (2014) highlight positive results for five participants with mild intellectual disability who received CBT for chronic pain, these gains were generally not maintained at follow-up. Generally, CBT programmes and strategies have yielded some success when used to manage neuropathic pain (Jensen et al., 2009; Turk et al., 2010).
Physical techniques
Physical interventions aim to reduce the perception of pain, and for persons with intellectual disability, this might include the application of ice or heat, positioning of a limb or seating position, cushioning and splinting, massage, acupuncture, vibration and transcutaneous electrical therapy (TENS).
The experience of physical pain may be increased by treatment, medication, side effects, concurrent debilities and the underlying disease itself such as malignancy. For people with intellectual disability, they often have conditions that require painful medical procedures (Bottos and Chambers, 2006; Malviya et al., 2005). Physical techniques in reducing perception of pain are frequently underestimated for their value in minimizing pain (Briggs, 2010; Heath, 1998). For persons with intellectual disability, this might include the application of ice or heat, positioning of a limb or seating position, cushioning and splinting, massage, vibration and TENS and acupuncture, addressing environmental causes such as lighting and ventilation.
The use of heat treatment moves the reflex arcs that inhibit pain by means of heat receptors and through vasodilatation to reduce pain. Similarly, cold treatment increases the pain threshold and reduces oedema, inflammation and pain experienced (Demir, 2012). Positioning can be an important treatment especially when a physical disability coexists or issues of gastric reflux. Positioning or repositioning by position change can prevent the development of pain, reduce pain, increase blood flow and prevent muscle contractions and spasms. The use of massage, vibration, acupuncture and TENS reflect our understanding of Melzack and Wall’s (1965) gate control theory. However, their use for persons with intellectual disability must be measured against the individual’s ability to understand and tolerate their use as they are invasive and in themselves inflict what might be considered as procedural pain (Halimaa, 2003). TENS works by transmitting lots of non-painful messages to the same place in the dorsal horn of the spinal cord that receives the pain messages and in so doing reduces the pain messages that are received and interpreted in the brain. The unit itself is a small battery-operated pack with electrodes that are attached to the skin in the location of the pain. In the general population, the individual controls the ‘volume’ of the stimuli that is sent. Within the general literature, it has been difficult to test TENS efficacy in patients with neuropathic pain because trials have a low fidelity associated with inadequate TENS technique and infrequent treatments of insufficient duration (Johnson and Bjordal, 2011). However, Naka et al. (2013) in their systematic review highlight that most studies revealed an analgesic effect in various painful conditions, confirming the usefulness of TENS in clinical practice. Massage is asserted to be effective in inducing relaxation and reducing challenging behaviours in persons with intellectual disabilities (Chan and Tse, 2011). However, evidence-based literature demonstrating the effectiveness of massage therapy in supporting clinical practice is extremely limited (Chan and Tse, 2011).
Conclusion
In the management of pain for individuals with an intellectual disability, a multimodal approach using both pharmacotherapy and non-pharmacological management is often most beneficial and should be considered depending on the person’s response and preference (Norrbrink Budh et al., 2006). Pharmacological approaches are widely used across all populations as a frontline treatment of pain and medications side effects need to be considered and monitored. While the evidence may be lacking for many non-pharmacological approaches, their use needs to be considered based on the fact that pain is subjective and an individual’s response to treatment may be subjective also. Pain management needs to incorporate pharmacological, self-management, coping resources and emotional well-being techniques to enable the person feel in more control of their pain, live as normal a life as possible and empower the person to become an active participant in the management of their pain and life. Given the complexity of pain management, there is a need for a comprehensive assessment and empathic support of the individual. This complexity is reinforced by family/carer knowledge, understanding, assessment and ability to understand the individual’s verbal/non-verbal communication. While effective pain management requires a multi-modal approach, there is also a need to investigate the appropriateness and suitability of all management modalities within the intellectual disability population and create an evidence base for each pain management intervention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.