
Abstract
People with intellectual disabilities who experience mental health difficulties often have high levels of self-criticism and shame. Compassion-focused therapy is a therapeutic modality effective in working with such feelings. This article follows on from a previous compassion-focused therapy group study exploring the impact of two compassion-focused therapy-based groups on how participants felt about themselves. Utilizing a mixed method design, the study illustrated that participants experienced higher levels of compassion and, overall, saw themselves more favourably by the end of the groups. They were also able to understand the basic concepts of compassion-focused therapy which reinforced previous study findings, suggesting that it is adaptable and clinically useful for people with intellectual disabilities.
Introduction
Both the current and historic discrimination experienced by people with intellectual disabilities give insight into ongoing discourses on and attitudes towards disability within society. These attitudes often relate to negative beliefs about what it means to be disabled (Bramston et al., 1999) with discriminatory practice common. For example, there is often less access to timely and effective healthcare (Michael, 2008) and they are more likely to be exposed to unemployment, poor housing and other social adversities (The Marmot Review, 2010).
As one the most excluded groups in society, people with intellectual disabilities are at a higher risk of shame-related distress (Marriott et al., 2019). Experiences of discrimination, social rejection, exclusion and humiliation are common shaming experiences within the intellectual disability population (Li et al., 2006), contributing to both psychological distress (Ali et al., 2012, 2015) and physical health problems (Mays et al., 2007; Williams and Mohammed, 2009). In the words of people with intellectual disabilities, social rejection by others is suggested to contribute to feeling ‘bad’ (Li et al., 2006) and stigma often appears to become internalized, with people reporting feelings of ‘oddness’, feeling ‘not good’ or being seen as ‘troublemakers’ (Chen and Shu, 2012). These experiences often contribute to feelings of both internal (how we view ourselves) and external (how we fear we are viewed by others) shame (Clapton et al., 2018a).
Prejudice, discrimination and abuse have a significant negative impact on self-esteem (Paterson et al., 2012). More specifically, people with intellectual disabilities experience high levels of self-criticism (e.g. Dagnan and Waring, 2004; Esdale et al., 2015) and are more likely to focus on the feelings of blame internally and believe the criticism they receive (Esdale et al., 2015). There is a tendency to use downward social comparisons when people with intellectual disabilities compare themselves negatively to others (Finlay and Lyons, 2000), particularly on domains of attractiveness and capability (Paterson et al., 2012). This increases the likelihood of depression, feelings of exclusion (Dagnan and Sandhu, 1999) and loneliness (Petrovski and Gleeson, 1997).
One therapeutic option, commonly used to support people experiencing high levels of self-criticism and shame, is compassion-focused therapy (Gilbert, 2005, 2009, 2010). This is an approach influenced by theories from social psychology, evolutionary psychology, attachment theory, developmental psychology and Buddhist psychology (Gilbert, 2014). It is well evidenced in treating people with a range of difficulties such as shame, self-criticism, depression, anxiety and eating disorders (Gilbert and Procter, 2006; Goss and Allan, 2010; Welford, 2010) and across a range of populations (e.g. Beaumont and Hollins, 2015; Mills et al., 2007). The main premise of compassion-focused therapy is to help the individual develop compassionate flow to and from others as well as towards themselves so as to develop a greater sense of warmth, safeness (Gilbert, 2009) social affiliation and trust (Cowles et al., 2018). People experiencing high shame and self-criticism often connect to alternative beliefs cognitively but struggle to do so on an emotional level (Cowles et al., 2018; Gilbert, 2010).
Developing this emotional connection is what compassion-focused therapy aims to address. The focus of compassion-focused therapy on alleviating feelings of self-criticism and shame is welcome in an intellectual disability population who experience high levels of both (Bramston et al., 1999; Hughes et al., 2012).
A review of the literature highlights that there are a limited number of studies exploring the impact of compassion-focused therapy for people with intellectual disabilities. This therapeutic modality has been historically less commonly used within this population with a previous focus on skills training or behavioural work (Royal College of Psychiatrists, 2004). One study reports the results of a single case design (Cooper and Frearson, 2017) in relation to a person with low mood and eating difficulties. The study suggested that although there appeared to be little change according to the outcome measures, the idiosyncratic self-report measure showed an improvement in mood. Additionally, a small scale study investigating the impact of compassion-focused therapy on anxiety (Hardiman et al., 2018) has suggested that the intervention contributed to an increase in compassion and a decrease in levels of anxiety. Most recently, a study reporting the experiences of compassion-focused therapy interventions with people with intellectual disabilities who have had traumatic experiences have suggested a qualitative improvement in traumatic symptomology after the intervention although it was acknowledged that for one participant further therapeutic support was indicated (Cowles et al., 2018).
Of published group interventions, Clapton et al. (2018b) facilitated a six-session compassion-focused therapy group for people with intellectual disabilities and suggests that there was a significant reduction in self-criticism and negative social comparisons. It was also reported that participants had experienced positive emotional changes, particularly in relation to the flow of compassion.
Delivering compassion-focused therapy in a group format may enhance the process of compassion in the group (Clapton et al., 2018b) which may relate to the ability to share experiences in a de-shaming and relational context (Bates, 2005). Group settings also allow the flow of compassion between group members with group members receiving and directing compassion from and to other individuals in the group (Gilbert, 2014).
Aim
Given the potential positive impact of safe group settings on feelings such as loneliness and shame (Bates, 2005), this study aims to evaluate a compassion-focused therapy group intervention for people with intellectual disability experiencing low mood, high self-criticism and feelings of shame. Outcomes will centre on a measure of social comparison, mood and self-compassion alongside a qualitative component to extend the work already completed by Clapton et al. (2018b).
Methods
Ethics
Ethical approval for this evaluation was approved by the Surrey and Borders Partnership NHS Foundation Trust research and development department and local NHS committee.
Recruitment procedure
Participants were recruited from an NHS Community Team for People with Intellectual Disabilities in the south of England. Multidisciplinary meetings were used to identify and refer service users who met the inclusion criteria (see Table 1) and where the group was deemed to be appropriate.
Inclusion criteria.
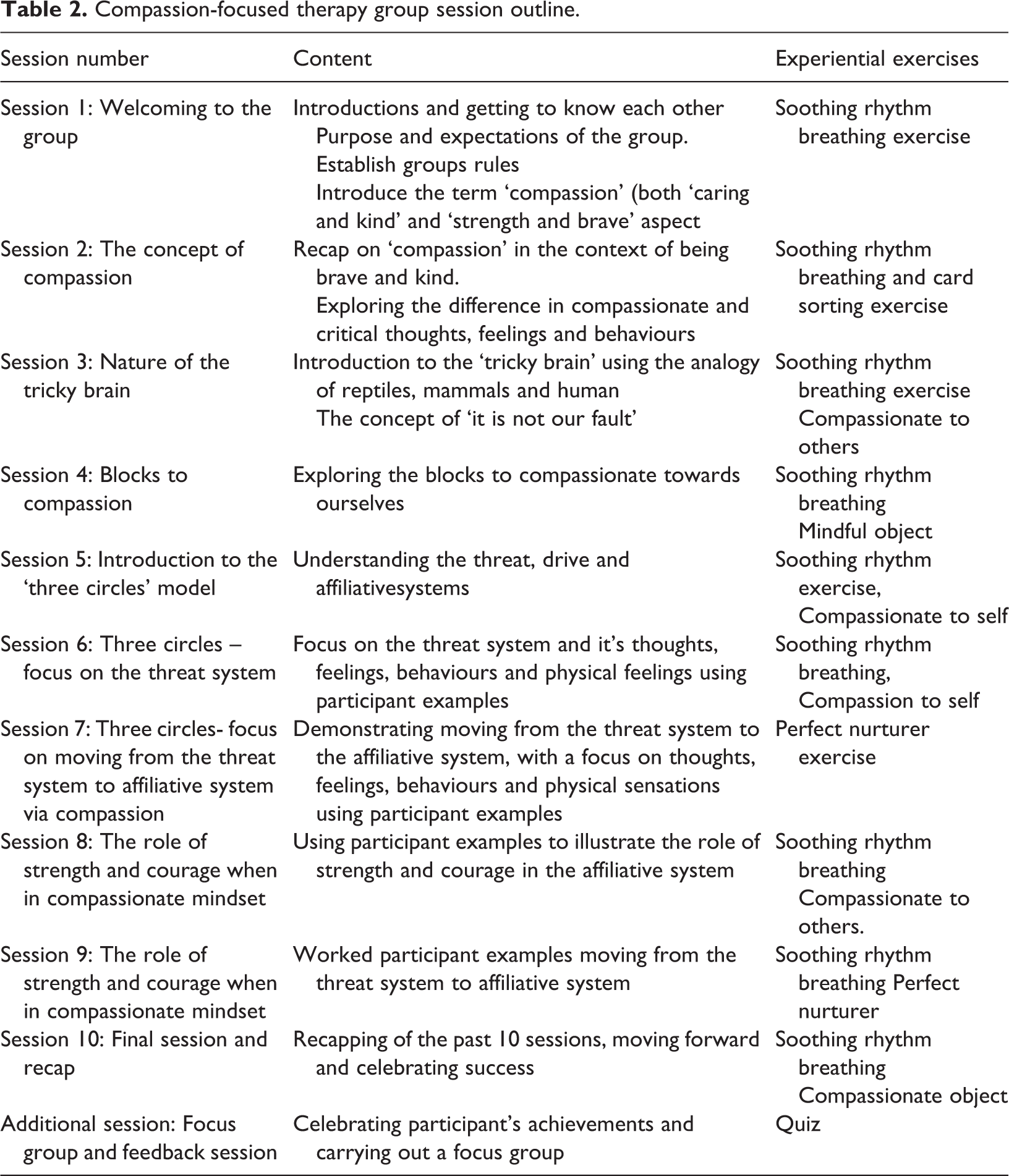
To build on the current literature, this study was designed to evaluate a further adapted version of the compassion-focused therapy group study published by Clapton et al. (2018b). The original group was a six-session group covering the key theoretical concepts and experiential elements of compassion-focused therapy. An outline of the original protocol can be found in the original study (Clapton et al., 2018b). The adapted version relevant to this study is outlined in Table 2.
Compassion-focused therapy group session outline.
Two groups were run at separate time points throughout the year, one at each community base to enable easy access for service users living across the county. The groups were adapted and extended by the first author. Both groups were run by the first author who is a Senior Clinical Psychologist and who has attended numerous compassion-focused therapy workshops, training and conferences alongside using it regularly in clinical practice. The second author was an Assistant Psychologist supervised by the first author.
Participant recruitment
Group 1
Six service users were initially identified as meeting the referral criteria and had expressed their interest in attending. Each participant was provided with an accessible information sheet and a leaflet during a pre-group assessment session with the facilitators to ensure informed consent was gained. Of original six referrals, only three attended on the first session but all three were retained and completed the group. Of the 10 group sessions, one participant attended all 10 sessions, the second attended 9 sessions and the final participant attended 7 sessions.
All three participants were aged between 25 and 40 years, with a mean age of 33 years. The group consisted of two females and one male, and all participants had a diagnosis of a mild intellectual disability. Each participant was offered the choice to be supported by a carer throughout the group, but all three chose to attend alone.
Group 2
Five service users were initially identified as meeting the referral criteria and had expressed their interest in attending the group. The same process was followed as for group 1. Of original five referrals, all attended the first session, but one found the group setting overwhelming and the second had to stop attending due to a deterioration in their physical health after the first session. Of the remaining three participants, all were retained and completed the group. Of the 10 group sessions, two participants attended all 10 sessions and the third person attended 6 of 10 sessions.
All three participants were aged between 19 and 32 years with a mean age of 23 years and 7 months. The group consisted of two males and one female, and all participants had a diagnosis of a mild intellectual disability. Each participant was offered the choice to be supported by a carer throughout the group, but all three chose to attend alone.
Capacity and consent
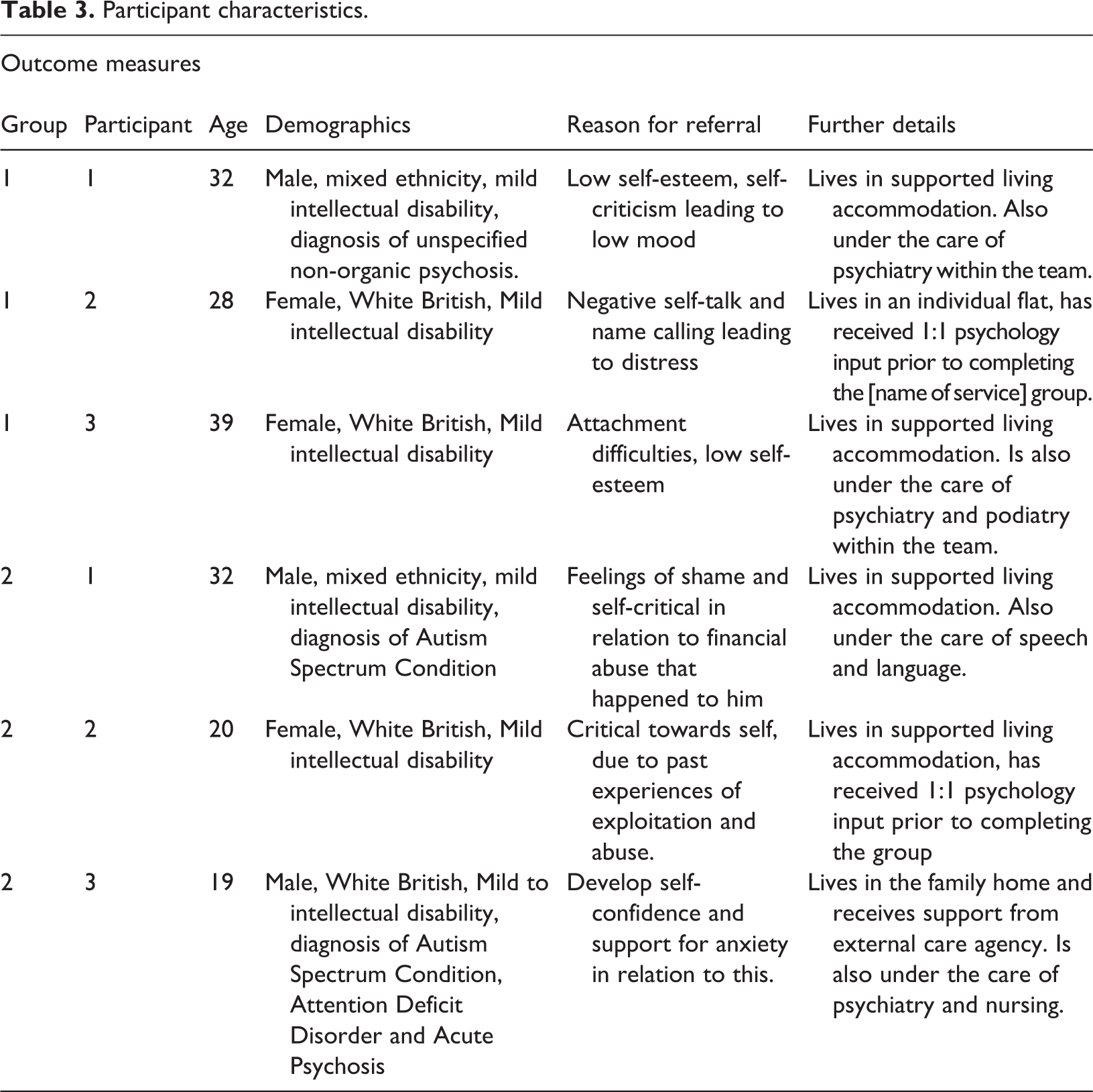
All six participants had mild intellectual disabilities and were deemed to have capacity to decide whether to attend the group or not. As such, with the full information about the group offered in an accessible format, informed consent was obtained.
The participant characteristics are illustrated in Table 3.
Participant characteristics.
Outcome measures
A combination of quantitative and qualitative outcome measures were used to evaluate the impact of the group on the participants. Three questionnaires were used including the CORE-LD (Barton et al., 2008), Adapted Social Comparisons Scale (Dagnan and Sandhu, 1999) and the Self-Compassion Scale–Short Form (SCF-SF) (Raes et al., 2011).
CORE-LD
The CORE-LD is a simplified and adapted version of the CORE-OM (Barton et al., 2008), a 14-item questionnaire designed to assess an individual’s mood. It does not yet have a set of referential clinical or non-clinical data, and thus, the scores are interpreted without reference parameters but alongside the qualitative data received from participants. It was chosen as it has been developed collaboratively alongside people with intellectual disabilities and forms part of the service protocol.
The adapted Social Comparison Scale
The adapted Social Comparison Scale was altered from its original (Allan and Gilbert, 1995) in order to be accessible to people with intellectual disabilities (Dagnan and Sandhu, 1999). It predominantly aims to measure how participants compare themselves across a range of domains. The psychometric properties have been examined, and the adapted version shows similar properties to the original scale (Dagnan and Sandhu, 1999).
Self-Compassion Scale–Short Form
The SCS-SF is 10-question version of the original self-compassion scale (Neff, 2003) and explores both self-compassion and self-criticism through the use of two subscales (Raes et al., 2011). Muris and Petrocchi (2016) have proposed that use of the total score is unreliable, but it has been suggested that the two separate subscales should be calculated (Costa et al., 2015). The version adapted by Clapton et al. (2018b) was used to ensure accessibility for an intellectual disability population. The original version has strong psychometric properties (Neff, 2016).
Focus group
A semi-structured interview schedule was developed from the original study (Clapton et al., 2018b) to better enable the exploration of participant experience of the group.
Statistical analysis
Each participant completed the three questionnaires both pre- and post-group to enable the analysis of change. Although traditional mean-based research methods are more commonly used to facilitate such analysis, reliable and clinically significant change are more appropriate for ideographic research where individual trajectories are the focus as supposed to generalizability (Zahra and Hedge, 2010). Change scores are ideal for any sample size, particularly small group research where t-tests need parametric assumptions unlikely to be met with small sample sizes.
However, reliable and clinically significant change analysis does rely on having the norms, means, standard deviations and co-efficient values for both clinical and non-clinical populations (Zahra and Hedge, 2010). In an intellectual disability population where validated outcome measures are less well established, this can prove difficult. As such, change statistically was calculated for the Adapted Social Comparison Scale (Dagnan and Sandhu, 1999) but only for the single-factor scale on the SCF-SF, rather than the more reliable two-factor scale, as the required psychometrics for each subscale were not available (Costa et al., 2015; Lopez et al., 2015). Descriptive statistics were calculated for the CORE-LD as there were no referential norms by which to complete a change analysis.
Thematic analysis was employed to analyse the data from both focus groups. The data from each group were analysed separately to provide the opportunity to compare themes across the groups more clearly. This was done in the context of an NHS service where outcomes for each intervention are required to ensure that the services provided are effective and safe. Analysing each group separately also enabled each service user to share more of their own voice within the analysis.
Results
As of yet, the psychometric data for the CORE-LD are not available and thus reliable and clinically significant change could not be calculated. However, the descriptive statistics for the CORE-LD pre- and post-scores for each participant are reported in Table 4.
Means (SD) for pre- and post-group 1 and 2 for the CORE-LD.

SD: standard deviation.
There is a reduction in scores for both groups from pre- to post-group mean. Although it is not possible to determine whether this was statistically significant with the data obtained, it does show some improvement.
Tables 5 and 6 illustrate the pre- and post-score means alongside the reliable and clinically significant change scores for groups 1 and 2 retrospectively.
Reliable change SCS-SF group 1.
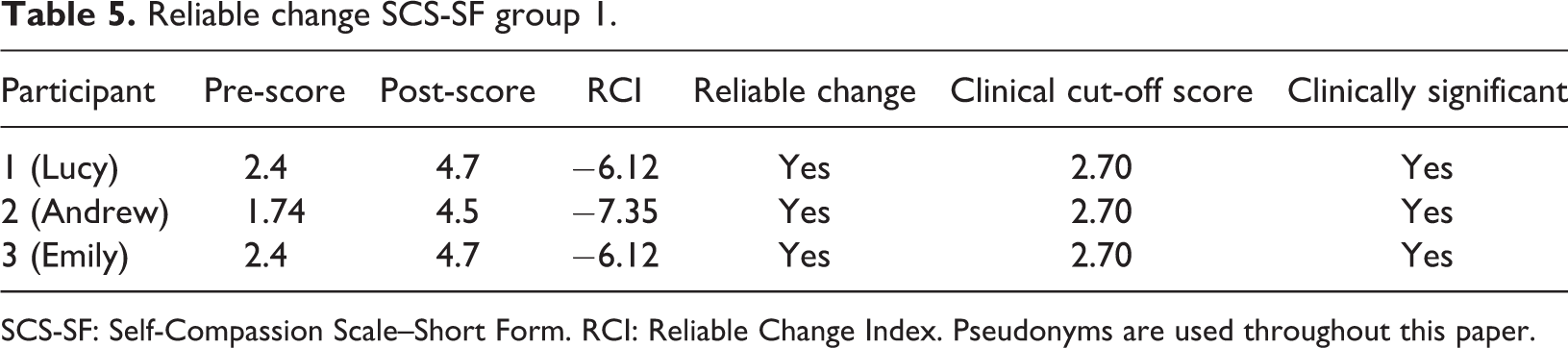
SCS-SF: Self-Compassion Scale–Short Form. RCI: Reliable Change Index. Pseudonyms are used throughout this paper.
Reliable change SCS-SF group 2.
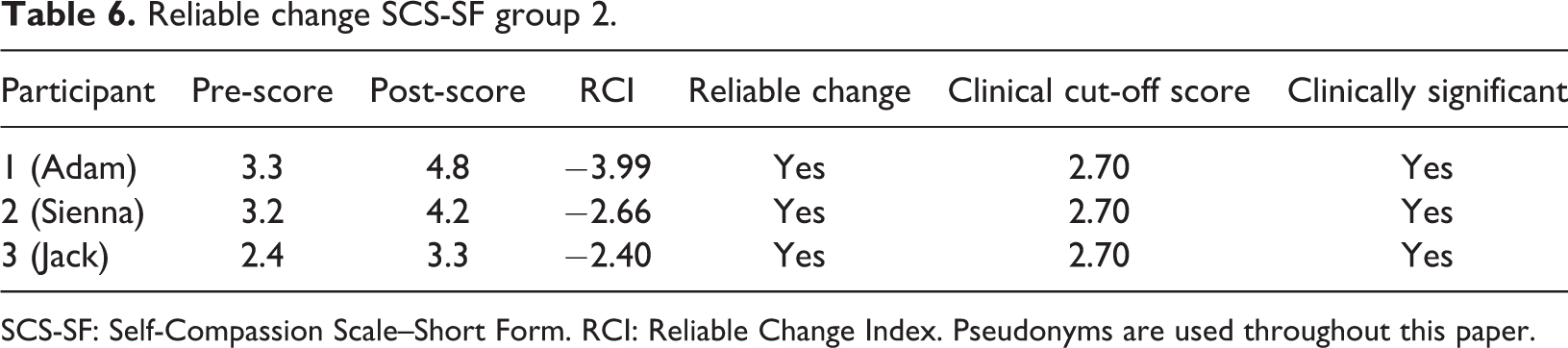
SCS-SF: Self-Compassion Scale–Short Form. RCI: Reliable Change Index. Pseudonyms are used throughout this paper.
Change scores over 1.96 in either direction are considered to indicate reliable change (Zahra and Hedge, 2010). On the SCF-SF, higher scores indicate higher levels of self-compassion. Post-scores have increased from pre-scores and thus across all six participants reliable and clinically significant change is indicated demonstrating an increase in self-compassion.
Tables 7 and 8 illustrate the pre- and post-score means alongside the reliable and clinically significant change scores on the Social Comparison Scale (Dagnan and Sandhu, 1999) for groups 1 and 2 retrospectively.
Reliable change scores for the Social Comparison Scale (Dagnan and Sandhu, 1999) group 1.
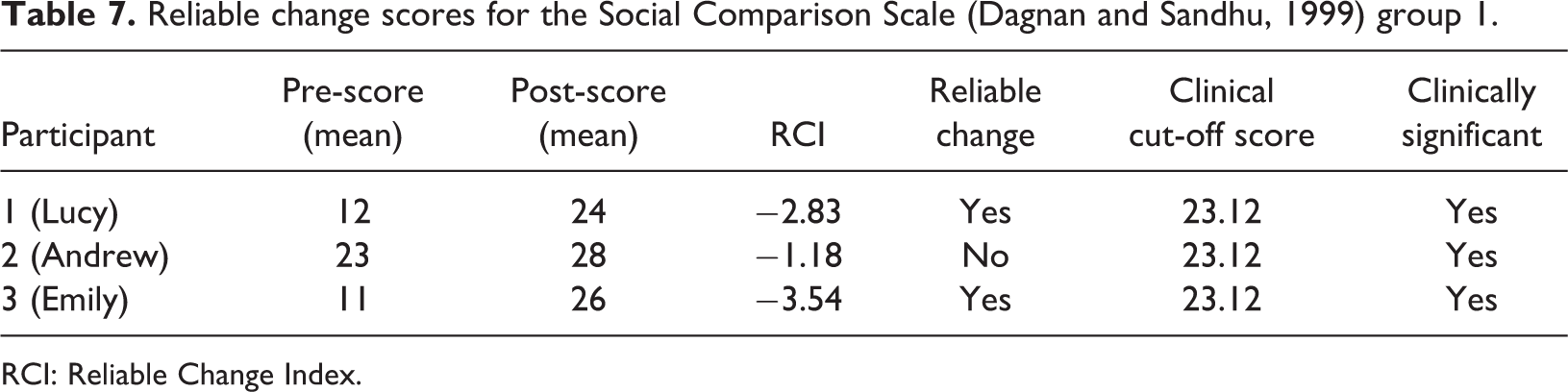
RCI: Reliable Change Index.
Reliable change scores for the Social Comparison Scale (Dagnan and Sandhu, 1999) group 2.

RCI: Reliable Change Index.
For the Social Comparison Scale, increased scores indicate more favourable comparisons in relation to themselves. Three participants' scores demonstrated reliable and clinically significant change from pre- to post-scores. Andrew’s pre-score was already relatively high and thus crossed the threshold of the clinical cut-off score easily reaching clinically significant change. However, the difference between scores was not reliable. Adam’s change scores exceeded the clinical cut-off score and thus were recorded as clinically significant, but the difference between pre- and post-scores were not different enough for this to be significant. Jack’s score demonstrated a reliable improvement but did not meet the clinical cut-off score and thus were clinically non-significant.
Qualitative analysis
A thematic analysis was utilized to analyse the data obtained from the two focus groups following the Braun and Clarke’s (2006) method of analysis. An inductive approach was employed with the development of themes linked strongly to the data (Patton, 1990). The analysis was completed on the transcriptions from each focus group separately after rigorous coding procedures were applied prior to the development of themes. This was completed by both researchers independently and then joint discussion about the main themes prior to arrival at the final themes.
Group 1
Five main themes were identified which included the following: feedback obtained; developing compassion to self and others; managing emotions; developing confidence; and developing connections.
Thematic narrative
Theme 1: Feedback obtained
Through the participants’ own evaluation of the group, feedback was shared about what was both helpful and unhelpful about the group. The first subtheme demonstrates areas that participants considered helpful, including the visual elements of the group:
‘just seeing the objects on the floor, that helped because it was just there ya know?’
‘I could see it, if that makes sense, so I could remember it more better’
‘having posters and picture and that, that’s easier than trying to remember lots of words…’
‘The exercises, like the breathing, easier to focus my mind than loads of words’
This may relate to the felt sense of compassion within the body when the affiliative system is activated. Although the experiential exercises appeared to be important to the participants, continuing to do them at home was more difficult. ‘It’s easy here when we do them together but it’s hard at home when no one can really help remind you or do them with you and that’.
In addition to what the participants valued about the group, they were also able to talk about areas that could be improved. For example, one participant said: ‘I think it got rushed a little bit…the writing on the white boards was hard to understand faster enough’.
‘I liked bubbles we used to do the breathing thing, and just the exercises, the soothing boxes, all of that stuff, can we do more of that rather than the stuff on the board and the writing?’
Theme 2: Developing compassion to self and others
Participants acknowledged becoming, ‘kinder to ourselves’ and ‘just giving myself a break’ like ‘I’d treat a friend right?’. They were also able to share explicit examples including being:
‘a bit fairer and I like myself a bit more’
Although not explicitly mentioned, there were elements of the second component of ‘compassion’, that of wisdom, courage and being able to sit with suffering mentioned in how they had managed to use their skills to ‘face fears’ in ‘real life’. One participant talked about how:
‘it’s helped me travel…its helped me get on the right buses, that scared me before but I did it anyway!’
‘my speech is a lot better and I don’t get as worried when I have a speech hiccup…it’s getting over that initial fear of winding through it’
‘if you’ve got something to say, its positive and it’s to that person, just say it. Don’t think of it, just say it…’and: ‘life is just better when everyone is nicer to each other yeah’.
Participants were able to reflect, not only on their experiences of being more compassionate towards themselves, but also on how compassion could be used to better the lives of other people too.
Theme 3: Managing emotions
All of the participants talked about how able they had been to feel ‘calmer’, ‘less angry’ and more ‘relaxed’:
‘I don’t get stressed or worried any more’
For example:
‘because I get very angry and the compassion, well it like makes me more calmer,’
Theme 4: Developing confidence
All of the participants talked about how they had become, ‘more confident’ and particularly how they had developed ‘confidence in situations that are difficult’.
‘it helped me to feel more confident in talking to three people I never met’.
‘because I know people that are confident on the outside like self-confident on the outside but self-conscious on the in. I was like that before and now I am confident all the way through.’
Theme 5: Developing connections
The final theme related to benefits of the group in relation to the participants connectedness to each other, for example: ‘joining the group meant I got to meet new people’ and ‘it feels good knowing others feel the same as you, like find stuff hard sometimes’.
‘I just, ya know, it’s not so much about what you learn but more just knowing people care…it gives you a warm feeling thing doesn’t it.’
Thematic analysis study 2
There were four main themes identified which included the following: Compassion to self Compassion to others Developing connection Obtaining feedback
Theme 1: Compassion to self
Participants initially talked about developing an increased level of compassion which they translated into their own feelings as illustrated below.
‘You feel better in yourself…I feel happier, excited, over the moon. Because I know I will have something to take my mind off things so then it will help me a lot more. Instead of feeling like low and tired.’
In addition to experiencing more affiliative-based feelings, the participants also talked about the basic concepts of the threat system and were able to use the three circles to explain the changes they were making as a result of this:
‘Keeping myself to not be negative about myself. Keep on thinking positive and obviously moving along from the threat system into my compassion system.’
Participants appeared to not only be acknowledging changes in their feelings, but were also cognitively reframing their threat-based thoughts using the affiliative system:
‘Oh in my compassion system. I was saying oh no Adam, It’s okay, you’re just tired. You had an extra two hours in bed. It’s my day off today, just saying, you know?’
‘I’m going to be teaching all of the staff and the tenants about compassion’ and also, ‘I am obviously doing the picture thingy, relaxing and all of that, it really helps.’
Finally, in addition to changes cited in their thoughts, feelings and actions, participants also talked about the physical changes within their own bodies experienced which included: ‘Not looking down at the floor all the time like this and now I am looking up at the future and down at the past and up at the future.’ Other participants talked about having ‘a big smile’ on their faces all of the time.
Theme 2: Compassion to others
There was evidence throughout the transcript of compassion towards others both in overt and in covert ways. For example, one participant talked of her experiences of sharing the breathing exercises she had learned with others:
‘I will do them with one of my tenants who lives in the home because obviously he keeps on thinking of negative things…. I sit there and help him to say, I said to him you need to sit there and just calm down, breathe in and breathe out and he does it and he says it really helps a lot. And now he is back to his smiley happy boy.’
Yet there were also more covert examples of where compassion to others was offered from participant to participant within the group sessions, demonstrated through their use of language when one of the others spoke, for example, ‘well done mate!’ and ‘wow, that’s amazing!’
And more specifically as one person explained that, ‘I’m recapping myself with what you guys say and now I am being very kind to myself’ another exclaimed’, Ah that’s incredible!’
This suggested that participants were not only talking about their compassionate flow towards others, but they were also demonstrating it in the room.
Theme 3: Developing connections
The compassionate flow from each participant in the group to another may have been helpful in enabling the development of connections with each other. Something that was identified as important in helping to create change:
‘All of you four lovely guys have taught me to be nice to myself, kind to myself. If I make a mistake or something has gone wrong, it’s not my fault. Just think, it’s okay, I can sort the problem…being with you all helped me with that.’
The benefits of meeting new people and making friends appeared to be acknowledged across all of the participants:
One participant enjoyed ‘meeting new people’ and another reported, ‘It is actually a really good group and it’s good to meet different people’. The third participant talked about the translation of connecting to others and using this to support coping outside of the group:
‘I talk to people, because I never usually talk to people about what I am feeling and now I can outside of here too’
Theme 4: Obtaining feedback
Overall, the participants talked about the group being ‘good and honest’ and suggested that they would recommend it to their friends: ‘I’d tell them I would say, you should go to it because it is a really good, honest group.’ They reported that they would ‘give it ten starts if I could…it’s a really good group and good to meet different people’.
‘I thought another girl could be nice’
S ‘Yeah, I feel like I’m all alone because I don’t have no girls to sit next to me’
There were also examples provided about how the content could have been delivered. For example, the participants were able to suggest more time to work through participant examples within the group setting:
‘Obviously talk to people 1:1 a bit more, like more time to go through the problem you bring, even maybe within the whole group sort of thing otherwise I liked it.’
Discussion
Across both groups, there were improvements from pre to post in mood on the CORE-LD, although change scores could not be calculated due to the lack of psychometric data. All six participants across both groups made a significant increase in self-compassion scores on the SCS-SF indicating both reliable and clinically significant change. Three of six participants across both groups illustrated reliable and clinically significant change on the Social Comparisons Scale. The remaining three participants made improvement in their scores, but the difference was either not great enough to be reliable or were reliable but not high enough to be clinically significant. These results indicate that the group had a positive impact on participants, particularly on levels of self-compassion.
However, the lack of psychometric data available for quantitative outcome measures validated in intellectual disability populations is problematic, an issue previously identified in other studies (e.g. Clapton et al., 2018b). Qualitatively, it is noticeable that participants found it difficult to complete the outcome measures despite them being adapted from the original versions. Significant facilitator support and question translation were needed to aid completion. For example, participants with a diagnosis of autism in addition to their intellectual disability found marking their response on a continuum line on the Social Comparison Scale difficult, preferring to choose their answers at one end of the scale or the other. The direct facilitator support to complete outcome measures may have led to an increase in acquiescence, particularly during the post-group measures which may also have created a bias in the results.
However, a mixed methods design was utilized to enable a richer understanding of the effects of the group. Interestingly, compassion was a strong theme across both groups in the qualitative analysis. There were narratives about an increase in compassion in both self and others as well as illustrations of how they were using compassion in its many forms, for example, in the action they took, the way they experienced it within their bodies and how they used it to reframe critical thoughts. This could suggest that the group were able to engage in and with both psychologies of compassion, engagement with their distress and the development of compassionate action to act upon it (see Gilbert et al., 2017). This shows promise in relation to participants being able to understand and integrate the principles of compassion-focused therapy in to their day-to-day lives, something which may, in part, relate to the highly experiential nature of the group, and which, by default, reduces cognitive load, focussing on more practical application. These findings have been reported across a range of studies previously including compassion-focused therapy (Clapton et al., 2018b) and mindfulness-related groups (Yildiran and Holt, 2015).
Connecting with others appeared to be an important theme in both groups. Bates (2005) writes about the positive impact of group settings on emotions such as loneliness and shame withimportance placed on sharing information with others who understood their struggles and the feelings of warmth that this evoked. The theme around developing confidence in one group also, in part, appeared to relate to this where some participants cited ‘talking about difficult things’ in front of new people as helping them grow in confidence. As Gilbert (2014) suggests, the group setting may have facilitated compassionate flow both from and to others, and experiencing warm and compassionate feelings in a safe environment may have been a first experience for some participants.
Both groups were able to provide positive and critical feedback. For example, positively valuing the visual material used to aid understanding but critically, occasionally finding that some elements still felt rushed especially when writing was used to display ideas. One participant also talked about considering a better gender balance which felt important in helping to ensure psychological safety within the group. Participants were able to understand the basic content and cited visual aids as supporting this process. However, as with the study evaluating the original group (Clapton et al., 2018b), it was difficult to know how much understanding of the key principles the participants had. It is possible that some of the more nuanced understanding was missed. For example, participants talked about the threat system being ‘bad’ but did not allude to ideas that the threat system can have both a helpful and unhelpful function. Alternatively, participants talked in dichotomy at times, for example, talking about ‘never being mean to myself ever again’. It may have been difficult to find the flexibility needed to hold the idea that we will all be self-critical sometimes, but self-compassion in relation to that may be what is needed.
Limitations and future research
Overall, the adaptations made to the group format between group 1 and group 2 helped to address some of the original limitations with the content by providing more breaks, increasing experiential exercises and visual materials. However, the quantitative outcome measures were still problematic in being understood by participants and by the complication of potential acquiescence. For future groups, it may be more helpful to incorporate person-specific goal attainment outcome measures to ensure they are more meaningful in addition to qualitative feedback. Despite people with intellectual disabilities generally experiencing high levels of shame (Clapton et al., 2018a), it was difficult to recruit enough people who were suitable to enable a large sample size. This particularly related to people being suitable for a group setting, level of intellectual disability and having the resources to get to the group location. Although the participants talked about the transferability of their skills to their day-to-day lives, future groups may consider inviting friends and carers to the last group session to provide shared intellectual and an opportunity for those at home to be able to support the continued development of learning skills.
Conclusions
Overall, the results across both groups were promising in suggesting that this compassion-focused therapy group might be helpful in increasing compassion in people with intellectual disabilities. The addition of four extra sessions comparable to the original (Clapton et al., 2018b), to enable additional repetition and trusting relationships to develop may have contributed to participants being better able to translate their skills to day-to-day life. The results, although preliminary, reinforce the idea already in the literature that people with intellectual disabilities are able to learn and use compassion-focused therapy-based skills. Further research could consider the addition of inviting friends and carers to the last session to support a shared understanding of the content and thus potentially enabling more support for participants in translating the skills in to their day-to-day life.
Footnotes
Acknowledgement
The authors would like to thank Dr Neil Clapton for providing original CFT protocol to develop this group. His compassion, continued support and kindness has been invaluable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.