
Abstract
This cross-sectional study explored stressful situations of caregivers related to life events of their children suffering from neurodevelopmental disorders along with potential contributing factors. A total of 906 caregivers of children with diagnosed neurodevelopmental disorder, from eight administrative districts and two city corporation areas in Bangladesh were interviewed. The Family Stress and Coping Interview scale was used to evaluate parenting stress. The diagnosis of neurodevelopmental disorder at the outset, feelings about the cause of the disorder, future planning for employment and accommodation for the child and dealing with child sexuality were some important stressful situations for parents. Parenting stress is found to be higher among female [regression coefficient (B) = 5.09, p < 0.001] and less educated caregivers [B = 2.69, p < 0.01]. Increasing age of child [B = 0.82, p < 0.001] and diagnosis of neurodevelopmental disorder before child’s second birthday [B = 4.22, p < 0.001] are also associated with higher parenting stress.
Keywords
Introduction
Parenting stress develops when parents’ perception of the demands of parenting exceeds their available resources (Raphael et al., 2009). Parents from all socio-economic strata experience some degree of stress in the process of child upbringing (Deater-Deckard, 2004). However, they generally cope up with such stress by making necessary adjustments to maintain family stability (Minnes, 1988). On the other hand, caregivers of children having neurodevelopmental disorders such as intellectual disability, autism spectrum disorder, attention-deficit hyperactivity disorder, and cerebral palsy are more vulnerable to stress and crisis (Dykens, 2015). Studies showed a higher level of depression, anxiety, stress, hopelessness, guilt, and less marital satisfaction among caregivers of children with neurodevelopmental disorders (Almogbel et al., 2017; Dervishaliaj, 2013).
The level of stress experienced by the caregivers having children with neurodevelopmental disorders is partly influenced by child’s characteristics, severity of the disorder, presence of comorbid conditions, and inappropriate behaviors of the affected child (Craig et al., 2016; Falk et al., 2014). Several other factors like caregiver’s sex, education, economic condition, physical well-being, perceived and actual stigmatization, and availability of social support are also identified as predictors for parenting stress (Bitsika and Sharpley, 2004; Falk et al., 2014; Farrugia, 2009; Gray, 2003; Parkes et al., 2015). Researchers have emphasized the importance of caregiver’s psychological well-being as it has a secondary impact on the child’s health, development, and functioning (Catalano et al., 2018; Davis, 1985; Dervishaliaj, 2013; Falk et al., 2014). Parenting stress often results in low parent-child interaction and parental support (Garner et al., 2011) and can negatively affect the outcome of an intervention program for children (Dervishaliaj, 2013). Before planning effective support services for children with neurodevelopmental disorders and their families, Falk et al. (2014) placed emphasis on understanding parenting stress and its contributing factors.
Neurodevelopmental disorder has emerged as a significant public health problem across the world. In a meta-analysis, Bitta et al. (2017) revealed that the median pooled prevalence per 1,000 for any neurodevelopmental disorder was 7.6 in lower- and middle-income countries, while neurological disorders were 11.3 and ADHD was 3.2. A cross-sectional study in a rural area of Bangladesh reported that the prevalence of autism spectrum disorder and cerebral palsy were 0.75 and 5.6, respectively, per 1,000 children aged between 18 to 36 months (Akhter et al., 2018). However, the caregivers’ burden related to these children remains mostly unexplored. It is believed that caregivers of children with neurodevelopmental disorders in Bangladesh remain in a stressful situation because of the social stigma associated with having intellectually challenged children and limited support systems at both governmental and private levels. Therefore, this study aimed to explore the level of parenting stress regarding different life events of the children with neurodevelopmental disorder, and identify the potential contributing factors for higher parenting stress. The result of this study is expected to provide a clear understanding of life stress that parents of children with neurodevelopmental disabilities experience in Bangladesh which can be considered while planning any initiative to alleviate this parenting stress.
Materials and methods
Study design and settings
This cross-sectional study included caregivers of children aged 2 to 18 years with neurodevelopmental disorders from all administrative divisions and city corporation areas of Bangladesh. There are eight administrative divisions in Bangladesh with 64 districts and 12 autonomous city corporation areas. Eight districts, each from one administrative division and two city corporation areas were selected randomly (lottery method) as study sites.
Information about children with neurodevelopmental disorder residing in the study areas was collected from the nearest Child Development Centers (Shishu Bikash Kendro). There are 15 state-run Child Development Centers in 15 government medical college hospitals of Bangladesh and there is at least 1 in each administrative division. These are specialized health facilities for the assessment, diagnosis, and management of children with neurodevelopmental disorders (Khan et al., 2017). A multi-disciplinary group of experts (child health physician, child psychologist, and developmental therapist) provides healthcare services in these centers. Children attending these centers are primarily screened for neurodevelopmental disorders using Independent Behaviors Assessment Scale, Rapid Neuro-developmental Disorder Assessment, and other psychometric tests. Diagnosis of neurodevelopmental disorders along with different ranges of intellectual disability (F70-F79) is confirmed by thorough psychological evaluations following International Classification of Disease (ICD) guidelines (Khan et al., 2017).
Sample size
The data used in this study were obtained from a large cross-sectional survey that evaluated the psycho-social well-being of the parents of children suffering from neurodevelopmental disorders comprehensively. The sample size was calculated based on mean and standard deviation values of physical (M = 52.1, SD = 18.7), psychological (M = 55.5, SD = 14.6), social (M = 54.6, SD = 24.6) and environmental (M = 39.8, SD = 18.2) domains of quality of life obtained from a previous study (Alhazmi et al., 2018) using the following formula (Charan and Biswas, 2013):
Here, Z is the value of standard normal deviation, reflecting the confidence interval (CI) that was used (Z = 1.96 for 95% CI), σ is the standard deviation of outcome variable and E (5.05) is the desired level of precision. Thus, a sample size of 90 was estimated using this formula. A 10% dropout rate was considered. Sample size was increased by a factor of (1/[1 − 0.10]) or 1.11 (Browner et al., 2007). So, the adjusted sample size for each study area was 100.
A total of 1000 caregivers, 100 from each study site, were enlisted and approached for interview from January to June 2019.
Participant recruitment and data collection
Information on children with neurodevelopmental disorders including their age, diagnosis, residential address, and cell phone number of their caregivers, was collected from the registers of Child Development Centers. Based on this information, a list of children was prepared and considered as the sampling frame of this study. A simple random sampling method was employed to select children from the sampling frame. Caregivers of the selected children were then contacted over phone and an appointment was fixed.
A total of 15 university graduates from social science background were recruited to collect data for this study. A 10-day training session was arranged where data collectors were trained on introducing themselves, explaining the purpose of the study, obtaining informed consent, administering data collection tools and devices, preserving confidentiality, and recognizing possible negative reactions to respond accordingly. After completion of training, data collectors visited each of the participant’s houses for interview. One caregiver was interviewed from each household. To select participant, primary caregivers (father and mother) were approached first, where only interested participant was interviewed. In case of unavailability of the primary caregiver, any family member who is mostly responsible next to the primary caregivers like grandparent, aunt, uncle, or elder sibling was approached. Face to face interview technique was followed to collect data in an isolated place within the household using computer assisted personal interviewing (CAPI) mode.
Data collection tool
Perceived parental stress in the upbringing of children was determined by Family Stress and Coping Interview (FSCI), an internationally well-validated tool (Nachshen et al., 2003). Permission was taken from Patricia Minnes, author of FSCI, for using this tool. A standard back-to-back translation process was conducted to translate the original English FSCI tool to Bengali language (native language of Bangladeshi people). Three focus group discussions (FGD) were conducted separately, one with subject specialists, another with male parents and the other with female parents to sensitize vocabulary and thinking patterns of the population. FGDs were audio-taped, transcribed verbatim and necessary modifications were carried out in the tool.
The FSCI (see appendix) measures perceived stress related to caregiving in families of children with developmental disorders across their lifetime through 23 items (Nachshen et al., 2003). Two questions related to dealing with legal professionals and financial and insurance issues were excluded from the original FSCI tool as they were found to be culturally not appropriate. Exclusion of two items did not affect the internal consistency of the tool as we found a coefficient alpha of 0.874 for the scale. Caregivers were asked to rate the level of stress related to each item on a five-point Likert scale ranging from 0 (not stressful) to 4 (extremely stressful). The individual items were then summed up to get a total score ranging from 0 to 84, with higher scores indicating high parenting stress. Apart from FSCI, the Perceived Stress Scale (PSS-10) and the World Health Organization’s Quality of Life scale (WHOQoL-BREF) were also used in this study to evaluate individual stress and quality of life, but the data are not presented in this paper.
Caregivers’ information, such as age, sex, educational status, employment status, marital status and type of family, and children’s information like age, birth order, sex, age at diagnosis, number of neurodevelopmental disorders and any other neurodevelopmental disorders affected their sibling/s, were also collected.
Ethical considerations
Ethical approval for this study was obtained from the Institutional Review Board of Bangabandhu Sheikh Mujib Medical University, Bangladesh (memo no: BSMMU/2019/6025). In Bangladesh, patients’ information in any Government hospital records are regarded as confidential and can only be accessed for research purpose with permission from responsible authorities. We attained permission from the Directorate General of Health Services of Bangladesh and respective hospital directors to use hospital records. Informed written consent was obtained from every participant before commencement of interview procedure.
Data analysis
Socio-demographic characteristics of the caregivers and children were described using mean and standard deviation (SD) for continuous variables, and frequency and percentage for categorical variables.
The association of socio-demographic characteristics of the participants and children with parenting stress was measured using independent t-test. Multiple linear regression analysis was done to determine to what extent independent variables explained the outcome variable, and which variables were the most important explaining factors. The caregiver’s sex, employment status (employed vs. unemployed), educational status, and family type (nuclear vs. extended), and the children’s age, sex, birth order, age at diagnosis, and number of neurodevelopmental disorders (single vs. multiple) were considered as independent variables, while parenting stress was considered as outcome variable. All independent variables that showed a significant association with the outcome variable in bivariate model were entered into the multivariate model. No multicollinearity among variables was seen. Normal P-P Plot of regression standardized residuals of the dependent variable was acceptable.
Statistical Package for Social Sciences (SPSS-23) was used for data analysis. A p-value less than .05 was considered as a level of significance.
Results
A total of 906 caregivers of children with neurodevelopmental disability participated in this study. Among them, approximately 64% were mothers, 32% were fathers, and 4% were other family members. The mean age of the caregivers was 35.1 (SD = 9.2) years. The overall mean of stress score among the caregivers was 53.3 (SD = 11) with a minimum of 14 to a maximum of 80. The much stressful situations for the caregivers were the moment of initial diagnosis of neurodevelopmental disorder (M = 3.34, SD = 0.73), and thoughts surrounding the reasons for neurodevelopmental disorder (M = 3.16, SD = 0.75), arranging employment (M = 3.17, SD = 0.92) and long-term accommodation (M = 3.12, SD = 0.98) for the child. Meanwhile, fulfilling the spouse’s needs, maintaining friends, taking care of personal needs, and visiting health professionals for the child were less stressful situations (Figure 1).
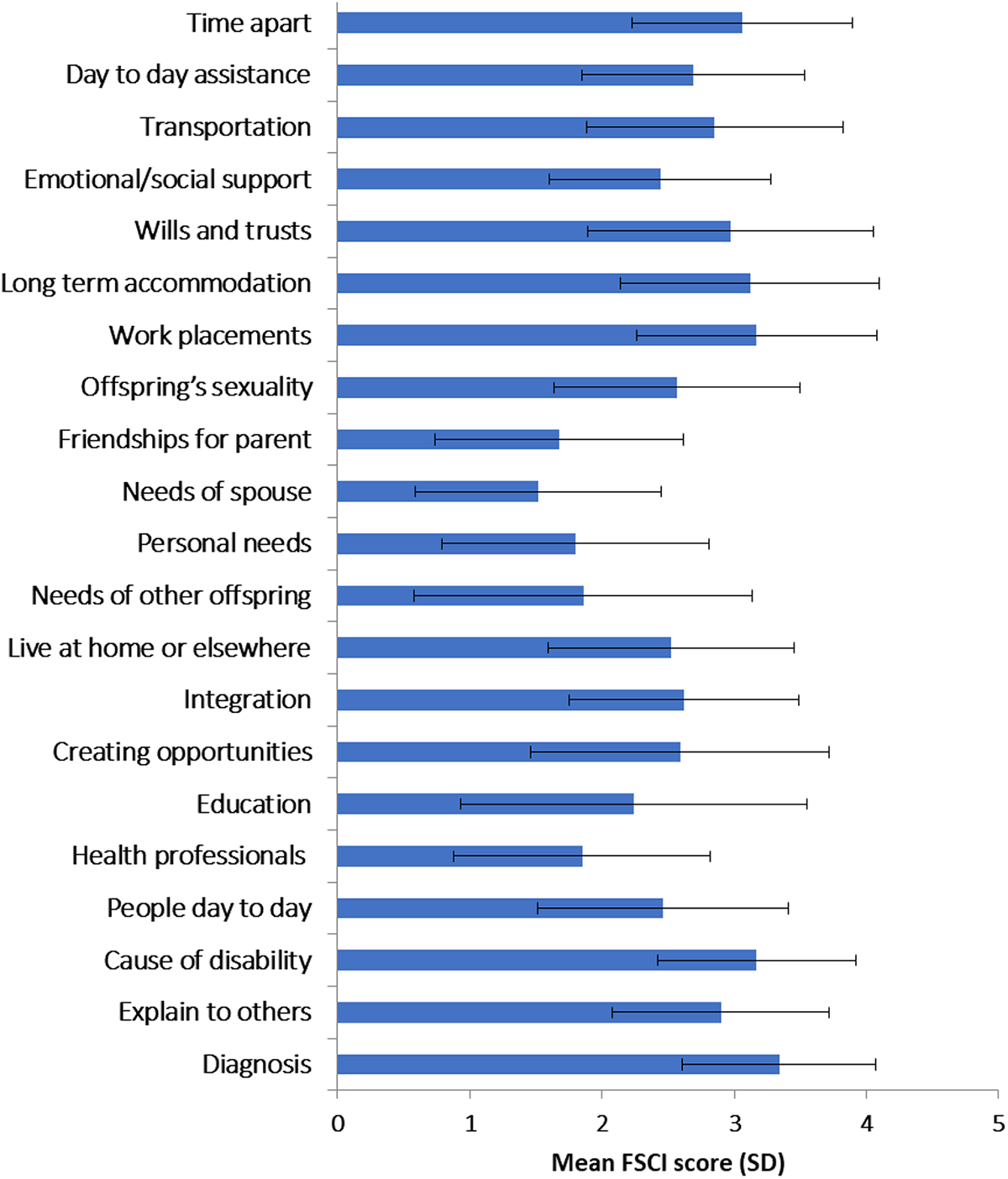
Parental stress score on Family Stress and Coping Interview scale among caregivers having child with neurodevelopmental disorder.
In bivariate analysis, significantly higher parenting stress was observed among caregivers who were female, unemployed, and less educated. Among the child characteristics, female sex, lower age at diagnosis and presence of more than one disorder among the children were significantly associated with more parenting stress. Birth order of the child, presence of intellectual disability, or having sibling with neurodevelopmental disorders did not show any statistically significant relation with parental stress outcome (Table 1). The age of children with neurodevelopmental disorder and parenting stress was positively correlated (r = 0.27, p < 0.01).
Distribution of parenting stress (FSCI score) in different socio-demographic characteristics of parents and children (n = 906).
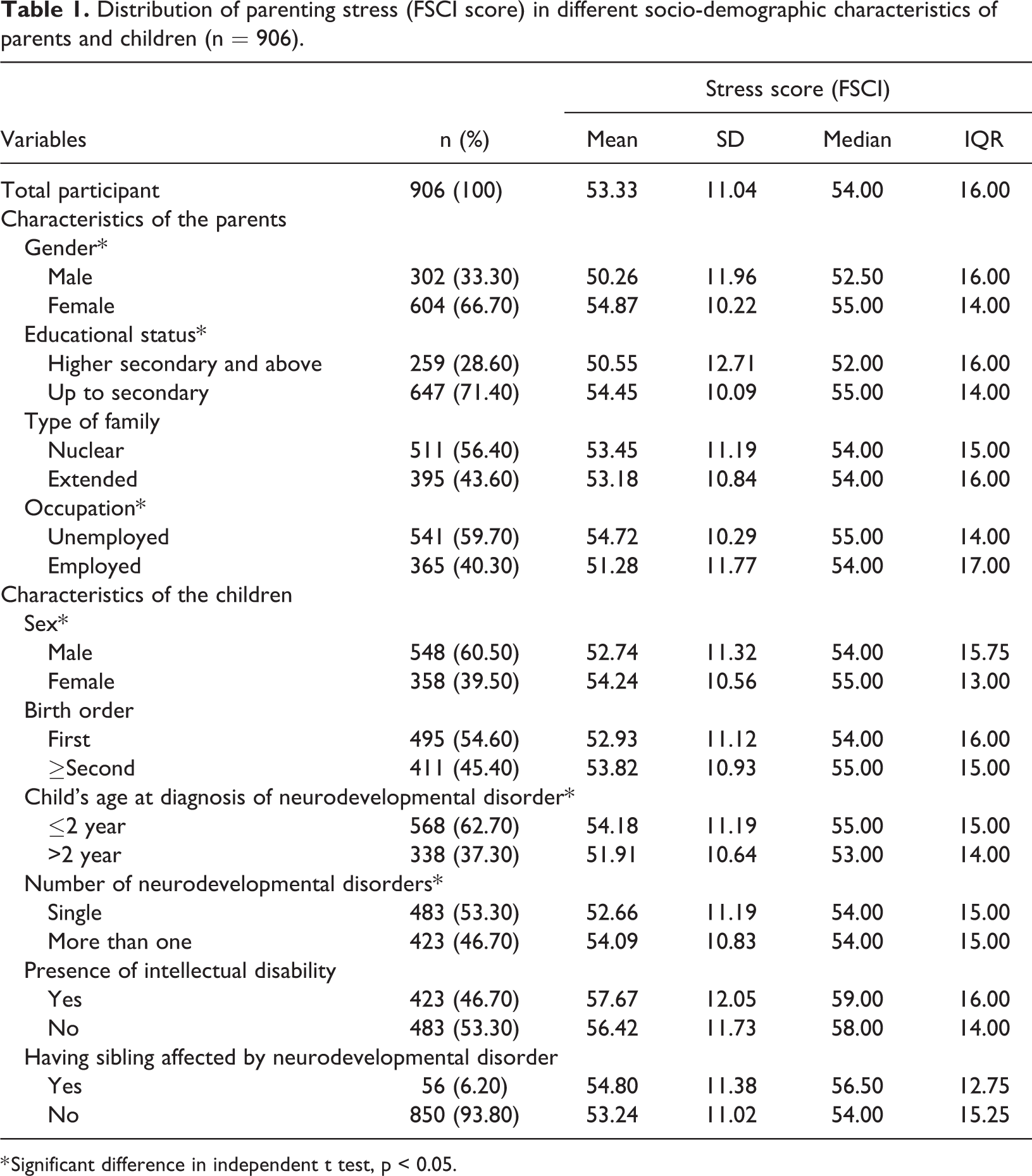
* Significant difference in independent t test, p < 0.05.
All statistically significant variables in bivariate analysis were entered into a linear regression model (Table 2). The regression model indicated that 15% of the variability in the mean FSCI score was explained by the caregiver’s sex and education level, age of the child, and child’s age at diagnosis. The linear model showed that the female caregivers (B = 5.09, p-value < .001) are at increased risk of getting stressed as compared with their male counterparts. The mean FSCI score was significantly higher among caregivers whose educational attainment was up to secondary level while comparing to caregivers with higher secondary educational attainment [B = 2.69, P = 0.001]. Child age was found to be the most important factor in explaining parental stress. With every 1-year increase in the age of the child, the mean FSCI score increased by 0.82. Diagnosis of neurodevelopmental disorder before 2 years of age increased parenting stress by a score of 4.22 in comparison to children who were diagnosed later (Table 2).
Factors associated with parenting stress among the participants of the study: Linear regression model (n = 906).
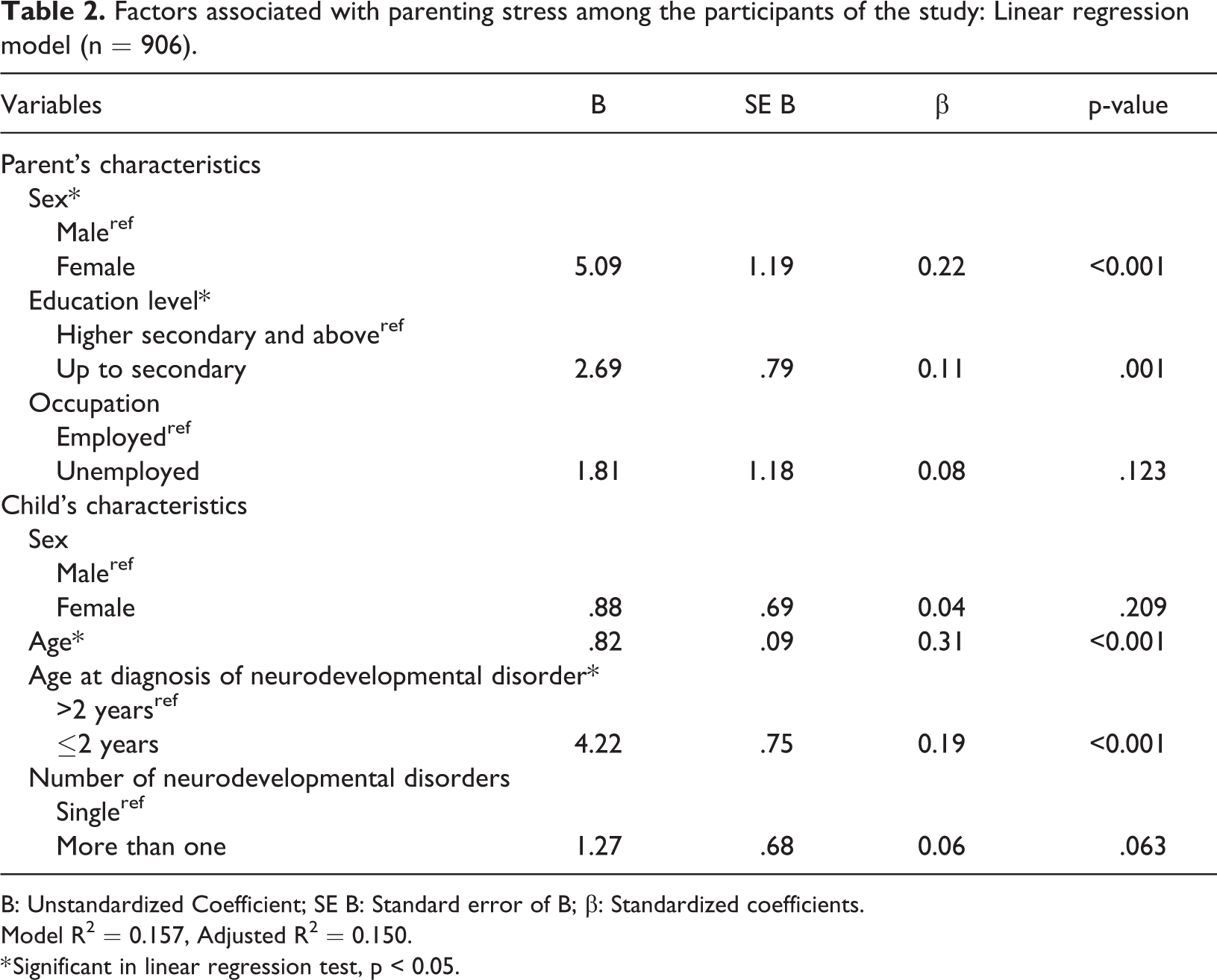
B: Unstandardized Coefficient; SE B: Standard error of B; β: Standardized coefficients.
Model R2 = 0.157, Adjusted R2 = 0.150.
* Significant in linear regression test, p < 0.05.
Discussion
This study addresses parents' stressful experiences related to different life events of their children suffering from neurodevelopmental disorder in Bangladesh. The diagnosis of neurodevelopmental disorder at the outset, feelings about the cause of the disorder, future planning for employment and accommodation for the child and dealing with child sexuality were some important stressful situations for parents as found in this study.
In comparison to our finding of receiving news of diagnosis as being one of the most stressful events for parents, Fernández-Alcántara et al. (2015) revealed a similar picture of distress for parents about their child’s diagnosis of neurodevelopmental disorder in Spain. The reason behind parental stressful response to the diagnosis can be explained by the disparity between parental desire for a healthy child and the diagnosis of a disability resulting in the feelings of child loss, grief, and anger (Fernández-Alcántara et al., 2015). In a review paper, Bonis (2016) also described that this stressful situation is related to the feeling of confusion, denial, decision-making doubt, helplessness, and failure as a parent.
Given the exact etiology of neurodevelopmental disorders yet to be explored, thoughts surrounding the causes remain shrouded in misconceptions. According to UNICEF (2014), there is a stigmatized belief in Bangladesh that disability is a curse and a punishment for the sinful behavior of parents, and this might be a cause of some parental stress found in this study. In addition, blaming each other and considering them guilty when thinking about the origin of a child’s disability may increase stress among parents, as reported by Mercer et al. (2006) in Canada and the United States.
Our finding of parenting stress in relation to the uncertainty of children’s future employment and accommodation can be linked to the inadequate livelihood opportunities and support services for such children in Bangladesh. Barriers for employment are limited inclusive educational facilities, inadequate professional and vocational training, and skepticism of the employers about hiring such people (Directorate General of Health Services, Ministry of Health and Family Welfare, Bangladesh, 2016). Similarly, Kiernan et al. (2017) described that children with intellectual disability in United Kingdom face the threat of exclusion from employment and community events as a result of their special behavioral needs. Khan and Anisuzzaman (2011) reported that only 11% of the children with disabilities are enrolled in schools in Bangladesh and a large portion of them drop out before completion of primary education. Inaccessible transportation, absence of trained teachers, lack of accessible toilets, prejudice and bullying on the part of teachers, parents, and other children have been reported as the reasons for dropping out.
This study also shows substantial parenting stress regarding child sexuality among the caregivers of children with neurodevelopmental disorders. Studies show that developmentally disabled children are more vulnerable to sexual abuse (Westcott and Jones, 1999), and abuse can further worsen their disability (Hibbard et al., 2007). A community-based study in United States shows that about 17% of the children with autism had been sexually abused (Mandell et al., 2005). Hence, parental concern about dealing with their child’s sexuality is justifiable and should be addressed in-depth.
Our study revealed that female caregivers are at significant risk for higher parenting stress. Congruent with our study, Pisula and Porębowicz-Dörsmann (2017) and Shin and McDonaugh (2008) found that mothers suffer more distress due to their child’s disability. Although our study could not bring in the reasons why mothers remain more stressed in upbringing a disabled child, Gray (2002, 2003), in an Australian study, suggested that removing inequal distribution of power in relation to gender and minimizing traditional gender role of child caring may help mothers be in less stressed. Traditionally in Bangladesh, women oversee taking care of children although less than 10% of the mothers enjoy the power of decision-making for their children’s health (Mainuddin et al., 2015). More studies should be done to explore the relation between parenting stress and women’s decision-making power in Bangladesh.
Our study found that caregivers’ low education level is a significant risk factor for higher parental stress. Almogbel et al. (2017) reported that education helps caregivers to have a more realistic and better understanding of their children’s situation and cope better with stress. Besides, education facilitates the caregivers to ensure multi-faceted management combining medication, professional therapy, social assistance, and rehabilitation for the child (Bakare et al., 2014; Dardas and Ahmad, 2014; Ferreira and Ribeiro, 2014).
The caregivers reported higher stress when their children were diagnosed at an earlier age. It can be assumed that children with visible and severe form of disabilities were diagnosed earlier. This has also been suggested by Emerson and Neece (2016) and Fountain et al. (2011).
Parenting stress increases with the child becoming older, as was found in this study. This can be related to the increasing need of caregiving, deterioration of the child’s health, and physical and sexual maturity as the child enters adolescence, as described in previous studies (Gray, 2002; Sabih and Sajid, 2008). Besides, Lopez et al. (2008) discussed that it is relatively difficult for parents to find opportunities to make friends for their children and participate them in social activities when the child with a developmental disability gets older.
Participants enrolled in this study were caregivers of children with neurodevelopmental disorder who visited Child Development Centers at government medical college hospitals. Not all children suffering from neurodevelopmental disorder in Bangladesh are registered in the Child Development Centers. So, the findings may not be generalized to the entire population.
Although this study utilized a fair number of predictors, some of the potential stressors were missing. Inclusion of a wider range of predictors, such as caregiver’s physical well-being, marital dysfunction, external support, range of child’s behavioral problem, and severity of the disorder could provide a better understanding of parenting stress. Even though FSCI is an internationally validated and reliable tool, answering questions about intimate relationship with the spouse and dealing with the child’s sexuality might be uncomfortable to the caregivers in the cultural context of Bangladesh, and this could lead to certain response bias. However, data collectors were trained thoroughly to address the sensitive issues in a socially acceptable way to minimize any chance of response bias.
Conclusion
Caregivers in Bangladesh face considerable parenting stress while encountering different issues in the lifespan of their children with neurodevelopmental disorders. This study identifies some significant life events that are particularly stressful for the caregivers, such as the initial diagnosis of disability, reasons behind the disability, long-term accommodation and employment of the child, and child sexuality. Female and less-educated caregivers endure higher parental stress. Besides, diagnosis of neurodevelopmental disorder at an early age and increasing age of child add substantially more parental stress to caregivers. Presence of intellectual disability or the number of neurodevelopmental disorders did not show any association with parenting stress. Future research needs to be directed to find appropriate coping strategies for these stressful life events and potential stressors.
Supplemental material
Supplemental Material, sj-docx-1-jld-10.1177_17446295211002355 - Parenting stress among caregivers of children with neurodevelopmental disorders: A cross-sectional study in Bangladesh
Supplemental Material, sj-docx-1-jld-10.1177_17446295211002355 for Parenting stress among caregivers of children with neurodevelopmental disorders: A cross-sectional study in Bangladesh by M Atiqul Haque, Marium Salwa, Sarmin Sultana, Anika Tasnim, Muhammad Ibrahim Ibne Towhid, Md Rizwanul Karim and Mohammad Abdullah Al Mamun in Journal of Intellectual Disabilities
Footnotes
Acknowledgements
The authors want to acknowledge the personnel from Institute of Paediatric Neurodisorder and Autism, Bangladesh Protibondhi Foundation and Child Developmental Centers for their expert assistance in skill development and data collection. The authors also want to show their gratitude to the caregivers and the families of children with neurodevelopmental disorders for their cooperation and keen participation in this study.
Author contributions
Study concept and design: M Atiqul Haque and Marium Salwa. Analysis and interpretation of data: M Atiqul Haque, Marium Salwa, Sarmin Sultana, and Anika Tasnim. Drafting of the manuscript: Marium Salwa, Sarmin Sultana, and Anika Tasnim. Critical revision of the manuscript for important intellectual content: M Atiqul Haque, Marium Salwa, Muhammad Ibrahim Ibne Towhid, Md Rizwanul Karim, and Mohammad Abdullah Al Mamun. Obtained funding: Md Rizwanul Karim and Mohammad Abdullah Al Mamun. Study supervision: M Atiqul Haque, Marium Salwa.
Data accessibility statement
Relevant data set will be archived in a well-known data repository after acceptance for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
Ethical permission was obtained from the Institutional Review Board of Bangabandhu Sheikh Mujib Medical University (BSMMU/2019/6025). Prior to interview, purpose of the study was explained, and informed consent was taken from each participant. Study procedures were designed to protect the participant’s privacy through voluntary participation and anonymity.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received grant from Directorate General of Health Services, Ministry of Health and Family Welfare, Dhaka, Bangladesh (Award no: ![]() ) and, logistic support was provided by Chi Research & Infotec Ltd, Dhaka, Bangladesh.
) and, logistic support was provided by Chi Research & Infotec Ltd, Dhaka, Bangladesh.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.