
Abstract
Down syndrome (DS) is a chromosomal condition that is affecting an increasing number of infants born in Saudi Arabia. This study investigates the needs of families with children with DS in Saudi Arabia from mothers’ perspectives and in a cultural and religious context. An exploratory qualitative research design was used, and semi-structured interviews were conducted with 14 mothers of children with DS. Interview data were thematically analyzed. The most important need was found to be financial or tangible support. An increase in benefits or monthly financial allowances and social security insurance would address these concerns. Societal support is also needed; mothers want DS to be perceived differently and require more support, including better rehabilitation and education services. Informational support is needed to improve the conditions of children with DS. Recommendations for improving the quality of life of children with DS are discussed.
Introduction
Mothers of children with Down syndrome (DS) in Saudi Arabia work to create an inclusive environment and sense of normalcy for their children without state assistance. They are more likely to experience stress, financial challenges, insufficient information, and a sense of social separation, than mothers of children without DS (Muir and Strnadová, 2014). Saudi Arabian Sharia laws exacerbate the problem by focusing on medical disability but ignoring the socioeconomic consequences of DS (Mulazadeh and Al-Harbi, 2016).
DS is associated with extra genetic material: instead of 46 chromosomes, a person with DS has a full or partial extra copy of a chromosome, delaying their development (Nadel, 2003; Wishart, 2005). It is linked to other noticeable characteristics, including stunted growth, behavioral phenotypes, health complications, and challenges completing day-to-day tasks (Huiracocha et al., 2017). Its cause is unknown, and no family is precluded from having a child with this syndrome (Bird and Buckley, 1994). People with DS can live a relatively normal life if they are provided with certain resources (Laws et al., 2000). The term DS is used interchangeably with “intellectual disability” and “learning difficulties.”
There is limited research on the needs of Saudi mothers of children with DS. According to The Voice of Down Syndrome Society (SAUT, 2020), DS is the most common chromosomal disorder in Saudi Arabia, and social policies must be developed to support children and mothers affected by this syndrome. While Sijeeni (2016) identifies different ways that mothers realize their capacity to care for a child with DS, specifically in Saudi, other studies show these families’ needs remain unclear. DS occurs in 18 per 10,000 live births in Saudi Arabia (Niazi et al., 1995); the rate of children with DS in some Arab countries exceeds the norm for industrialized countries, which is 12–17 cases per 10,000 live births (Al-Gazali et al., 2006). Of the 25,000 people with DS living in Saudi Arabia in 2009, 85% were not receiving schooling (SAUT, 2020).
Views on disability vary significantly by culture. In Saudi Arabia, religion affects all aspects of life and protects people with disabilities (Al-Gain and Al-Abdulwahab, 2002). Muslims’ understandings of disability differ widely and are influenced by their social and economic background, cultural context, and religious commitment (Al-Aoufi et al., 2012). Unlike other Islamic countries, all Saudi legislation is derived from Sharia law (Al-Aoufi et al., 2012; Moaddel, 2002).
One in 554 children in Saudi Arabia is born with DS (Niazi et al., 1995). Al-Sughair (2016) notes that 20,000 Saudi children younger than 17 years have DS. People with DS have limited comprehension abilities and require medical care tailored to their needs. Investing in national health services will enable people with DS to exercise their rights such as the right to medical care.
Increased maternal age increases the likelihood that a baby will be born with DS (Cuskelly et al., 2009; Kimura and Yamazaki, 2013; Marshall et al., 2015), as older ova pose a greater risk of abnormal chromosomal cell division (Alabri, 2017). The increase in the birth rate of children with DS in Saudi Arabia could be a result of the prohibition of abortion according to Sharia law; if a pregnant woman learns her child will have genetic defects, she is forbidden from aborting the fetus. Moreover, Saudi women are expected to continue having children into their forties (Laws et al., 2000). Healthcare progress in the country also reduced the death rate of children with DS, and increased their life expectancy (Alabri, 2017).
The teachings of Islam seem to have aided the reduction of the death rate of children with DS. Islam urges family members to help each other, regardless of disability (Alkohaiz, 2018). Despite the emergence of the nuclear family, the extended family system is still prevalent in Saudi villages (Al-Naami et al., 2010). Even in cities, fathers and sons live next to each other, indicating that family commitment remains common. People with disabilities are supported by siblings, not placed in homes, after their parents die (Alkohaiz, 2018), and the entire family help in caring for disabled children (Cook, 2004).
Family friends are expected to offer sympathy to the families of the disabled (Alkohaiz, 2018). However, some believe children with disabilities to be a punishment from God. They may be embarrassed by their children’s disabilities, resulting in them hiding their children (Al-Gain and Al-Abdulwahab, 2002) or keeping them secret to avoid shame, embarrassment, or even future marriage arrangements (Williams and Heslop, 2005).
In Saudi, children with moderate disabilities can enroll in mainstream schools in a separate class. However, children with more profound difficulties must be enrolled in day-care centers or institutions (Alabri, 2017). This policy illustrates the prejudices against these children and why parents often withdraw their children from school (Williams and Heslop, 2005).
Services for people with disabilities are provided by rehabilitation centers and hospitals. Some villages lack these services, perhaps because of the widespread use of wasta (an Arabic word meaning “using influence for gain”); for example, villages that have influence with the authorities find that they have these services (Barnett et al., 2013; Hutchings and Weir, 2006). Other reasons include the lack of accurate statistics on the number of people with disabilities in the villages, widespread stigma that leads families to hide their disabled children, and even governmental failure to help these children (Alkohaiz, 2018).
The stigmatization of children with disabilities extends to relatives, especially when the disability is noticeable from birth (Cuskelly et al., 2009). Consequently, the family may exclude themselves from social activities, be unwilling to discuss concerns, or avoid seeking assistance outside the family (Williams and Heslop, 2005). Accordingly, research on families of children with DS is shifting from pathology to family strength and flexibility (Cuskelly et al., 2009).
The uncertainty that comes with having a child with DS may cause domestic conflict, either between the child’s parents or other family members (Carr et al., 2016). Families should have opportunities to participate in rehabilitation programs that advance the well-being of the child and the whole family (Alsem et al., 2014).
Saudi Arabian school principals face challenges in implementing DS inclusion policies because they lack funds, infrastructure, and time (Alabri, 2017), complicated by the lack of inclusive education reforms. The Ministry of Education provides sufficient annual funding, as guided by Saudi Arabia’s Rules and Regulations of Special Education Programs (Alquraini, 2011); inadequate learning opportunities for students with DS are compounded by insufficient accountability, rather than insufficient funding. Individual principals have tried to raise money for materials for students with DS (Alabri, 2017); however, improved implementation would allow the government to use available resources to advance inclusive education.
Families with children with DS are more likely to suffer stress, family collapse, financial challenges, and social separation, compared to other families have DS (Muir and Strnadová, 2014), affecting their social welfare and quality of life (Barr et al., 2016; Buzatto and Beresin, 2008; Zuurmond et al., 2015). Nevertheless, parenting a child with DS is often a positive experience (Norwich, 2013), expanding parents’ social networks to include other parents in the same position, (Kimura and Yamazaki, 2013), and improving their quality of life (Buzatto and Beresin, 2008). Such parents also report increased appreciation for their children and gratitude for social support, compared to parents of children with other disabilities (Esbensen et al., 2010). Professionals need to ensure that parents have sufficient social support (Huiracocha et al., 2017). People with DS also benefit from increased socializing and early access to resources that can improve their chances of living a good and long life (Marshall et al., 2015).
Some countries have increased efforts to identify and respond to the needs of families of children with disabilities (Alsem et al., 2014); however, in other countries, comparatively few studies have focused on the specific needs of families of children with learning difficulties (Hu et al., 2015). These families’ needs differ depending on the child’s level of ability and interests (Vitello and Mithaug, 1999). Parents with developmentally delayed children need understanding and support, and when parents work with professionals, teachers, and other parents, they can positively respond to their children’s needs. They can also share ideas to help others (Stroh et al., 2008).
Many parents of children with disabilities experience their needs to be unmet and doubt they will ever be met (Alkohaiz, 2018; Heller and Caldwell, 2006). Access to appropriate information regarding diagnoses and available services (Carr et al., 2016) may reduce the anxiety of families with children with disabilities by enhancing their ability to plan (Heller and Caldwell, 2006; Heller and Factor, 1993; Muir and Strnadová, 2014).
Creating a healthy environment tailored to an individual’s disability is a complex task, as each child and their family experience the disability differently, with substantial effects on one’s life (Serafica, 1990). This study used a qualitative approach to explore the needs of families of children with DS, as perceived by Saudi mothers in the Eastern Province. From the mothers’ perspectives, what are the needs of Saudi families who have children with DS, and what aspects of religion and culture impact these needs? The findings should contribute to improving support for Saudi Arabian children with disabilities.
Materials and methods
Research design
Following a qualitative approach, this study sought to gain a comprehensive understanding of the daily needs of families of children with DS in the context of Saudi Arabian religion and culture. Data were collected through interviews.
Researcher’s perspective
The researcher’s context is vital in investigative studies (Costley et al., 2010). In qualitative research, the researcher’s experiences inevitably influence the research. Therefore, before beginning a study, the researcher must understand that (a) participants’ feedback must be considered carefully, and (b) all findings are subjective. Any limitations of past research should guide this study in circumventing potential bias (Murray and Lawrence, 2000).
The researcher’s personal experience informs this study. The researcher has volunteered to support children with DS since the birth of his daughter, who has this condition, by answering families’ questions telephonically or in person. This issue is significant to the researcher and will be handled sensitively so that these families can receive more help in the future.
Participants
Mothers from different social backgrounds, living in a multicultural city in eastern Saudi Arabia, were recruited through a rehabilitation center, using a purposive sampling strategy. Inclusion criteria, agreed upon between the researcher and the center’s advisor, were mothers who were older than 35, so that they have sufficient maternity experience with their children with or without DS; they should have a child with DS, who is enrolled in the study and older than 3 years; they should participate in conjunction with the center; and they should agree to be interviewed telephonically. Another important condition, compatible with Saudi culture, is the consent of the husband to his wife’s participation in the study; if not, she would be excluded from the study.
Accordingly, the researcher handpicked the participants he believed could provide the most relevant information. Mothers were chosen as subjects because they act in the interest of their children and play a large role in managing the Muslim family (Murray and Lawrence, 2000). Even though it is challenging for men to conduct research with women—and almost impossible in Saudi Arabia—owing to the researcher’s positive relationship with the center advisor as well as the mothers, it became possible for women to participate. A total of 14 mothers directly agreed to participate. It was also agreed with the center’s advisor that further participants could be recruited if the need for more data arose. However, data saturation was achieved after 14 interviews. According to Guest et al. (2006), the amount of data is likely to be adequate after six interviews, especially when the sample evinces a specific phenomenon.
Ethical considerations
All participants provided verbal informed consent; participants preferred not to sign a written form due to cultural barriers. According to Hutchings and Weir (2006), verbal consent is typical in this culture, and to ensure this approach did not breed further bias, all participants were assigned a code. To avoid institutional barriers in data collection, the researcher utilized the rehabilitation center, which already had the participating mothers’ details. The researcher obtained approval from the rehabilitation center to conduct the study. Once the participants were selected, their phone numbers were collected, and interviews were organized to clarify the participants’ role in the study and explain the research objectives. Participants were assured that no identifying information would be shared. Although no participants were forced to respond, some were encouraged to answer through probing questions, informal conversations, and by explaining the importance of the study for their families. Respondents were assured that they could terminate the interview if they wished, and they were urged to verbalize any concerns so they could be addressed.
Data collection
All interviews were conducted telephonically because Saudi culture limits face-to-face interviews between women and male researchers. As the data were not meant to be statistically evaluated, a formal questionnaire was not needed. The interviews were conducted with the mother—the family leader—to study the decision-making process related to their children with DS, and a formal questionnaire would have restricted the discussion. A semi-structured interview format was implemented, and it was vital that all questions were posited in a clear, concise, and friendly manner. The questions largely concerned the family’s daily needs and whether those needs were being met. The researcher shares the same culture as the mothers, which allowed him to notice their hesitation to respond to some questions and topics. The researcher respected such reservations, regardless of the potential value of their withheld responses.
All interviews lasted 15–25 min. Owing to Saudi culture, the mothers categorically demanded that their interviews should not be recorded. When recording devices are not used, participants feel more comfortable expressing their opinions. None of the participants were uncomfortable with the researcher taking notes of their answers, and to ensure there had been no miscommunications during the interview, all notes were reviewed and approved by the participants (Chong, 2008). They were also informed that their interviews would be translated into English and included in this study.
Data analysis
In this study, the researcher used interviews, a qualitative data collection method. The interviews were recorded by hand and then captured electronically, using Word software. The interview notes were written in Arabic, which was also used during the interviews. Only extracts included in the final text were translated into English. To ensure high accuracy, translated extracts were reviewed by an Arabic-English translation specialist.
Each interview was coded with a letter and number. For example, to ensure the confidentiality of the participants, participating mothers were coded as Mother 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, and 14. To ensure confidentiality, data were stored on the researcher’s personal computer, which is secured by password, as well as on OneDrive.
The researcher started analyzing the data immediately after each interview, as this enabled the identification of new issues to be explored with the next participant. This method also enabled the researcher to verify participants’ statements and to develop temporary themes (Ritchie and Spencer, 2002). After completing the investigation phase, the data were analyzed more objectively, using thematic analysis (Atkinson and Hammersley, 2007). Atkinson and Hammersley (2007: 212) suggest that there is no standard rule for analyzing data, but it is important is to move “back and forth” between ideas and data, testing it repeatedly, and then develop ideas to fit more data.
After extensive and repeated reading of the data, the researcher classified and coded the data, and divided it into themes, each possibly containing a number of sub-themes. By employing manual coding, the researcher felt confident that no key data would be missed. In this way, the researcher became more involved in the lives of mothers of children with DS, as well as with the children themselves and their families, enabling the identification of family needs from the perspectives of the mothers.
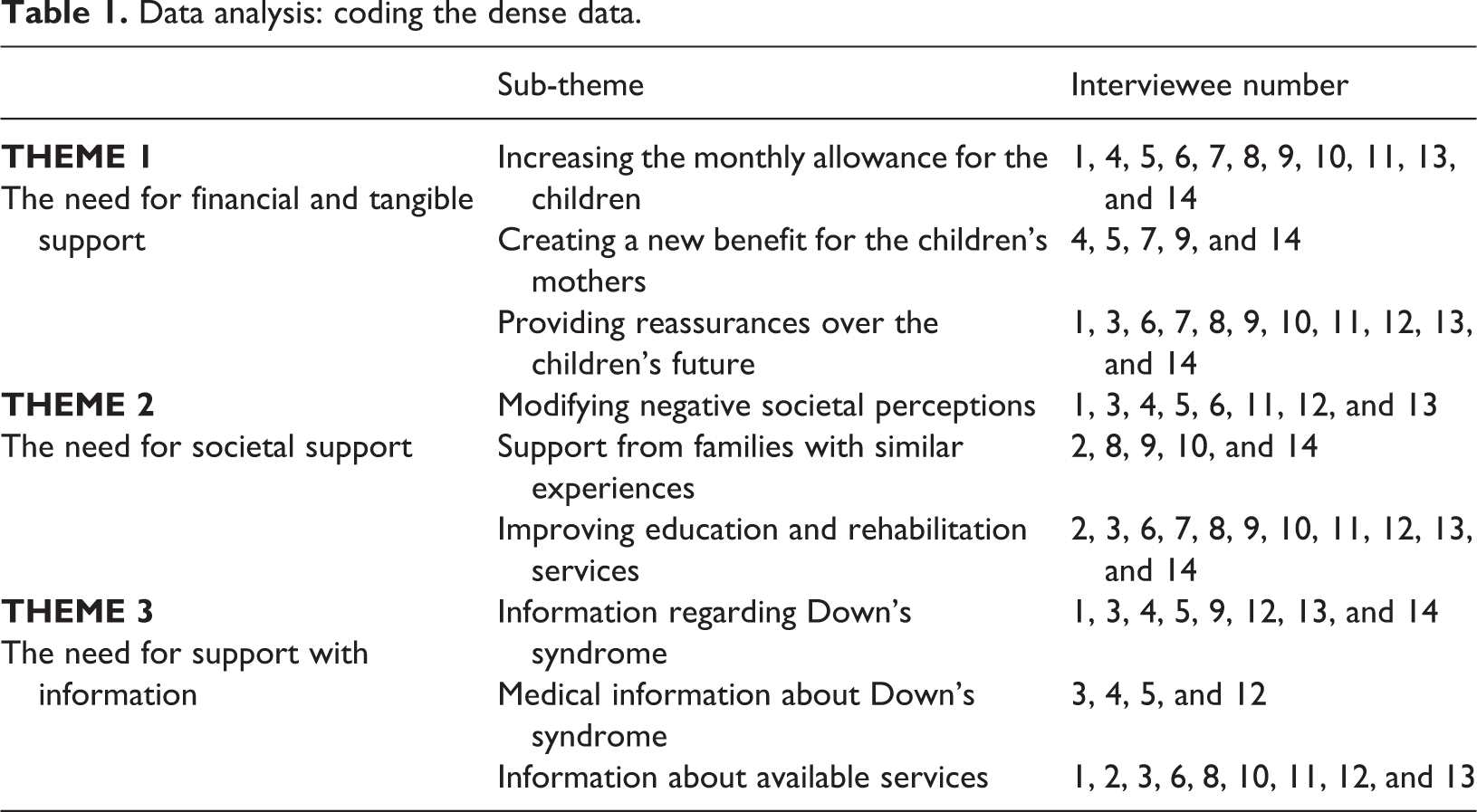
The data were presented and categorized into themes and sub-themes, according to similarities and differences. By displaying the data on a page, associations and sequences were identified and novel concepts discovered, thus drawing out and supporting conclusions. Extracts representing similar concepts were placed in appropriate categories. For example, all responses related to increased amounts of money were placed in the sub-theme “increasing children’s monthly allowance,” emanating from the main theme “the need for financial and tangible support.” These stages were repeated again and again, with fruitful and novel results. Table 1 shows the data coding.
Data analysis: coding the dense data.
Reliability of the findings
To enhance the reliability and rigor of the study, the researcher used reflexivity and member checking. Considering reflexivity, the researcher noted his position as the father of a child with DS and extensively considered the creation and analysis of the data. For example, the researcher defined the goals of the study in advance to avoid influencing the data to reflect pre-existing issues. Additionally, the researcher did not share the interview questions in advance, and during the interviews, the researcher emphasized that the participants could talk about anything regarding their needs as mothers (Sijeeni, 2016).
Member checking occurred throughout the interviews, as the researcher asked the mothers questions to verify that they understood the questions. This reassured the researcher that participants’ needs were collected reliably (Krefting, 1991).
Results
The researcher used the unique background of Saudi religion and culture to understand and contextualize the study’s findings. In the following sections, the researcher will elaborate on these themes and sub-themes.
Theme 1: Financial and tangible support
In the US, any child with a confirmed DS diagnosis is covered under the National Disability Insurance Scheme (NDIS), with access to early intervention therapies and education (Raising Children Network, 2020). In the UK, children with a disability younger than 16 receive composite financial support (Down’s Syndrome Association, 2020). Lower-income families in the UK can claim Universal Credit or Child Tax Credit; younger individuals can qualify for the Disability Living Allowance (DLA); and individuals who have stopped working to care for someone with a disability can apply for Carer’s Allowance (Down’s Syndrome Association, 2020). Individuals aged 16 and older who are still students can qualify for financial benefits, including Child Benefit, Carer’s Allowance, Child Tax Credit, or Universal Credit, until they are 20 years old. They can also claim Personal Independence Payment (PIP) instead of DLA when they turn 16, to compensate for disability costs; PIP can be spent on anything that benefits the child (Down’s Syndrome Association, 2020). International standards include Employment and Support Allowance (ESA) for individuals over 16 years old who cannot work because of a disability. Individuals with DS 16 and older qualify for ESA while they are in high school or college and can claim PIP. ESA provides funds for obligations rather than simply a wage. However, claiming that ESA automatically removes the Child Tax Credit (Down’s Syndrome Association, 2020).
Throughout the interviews, the participants were asked, “Is everything OK with you?” The answer invariably referenced financial or tangible support: The government is responsible for paying her rehabilitation fees. She also gets treatment for free. I would like to see an increase in this type of assistance…Yes, I am satisfied that my daughter is among us. We pray to God that she rewards us with heaven. (Mother 10) My son needs extra speech therapy by fee…. The ministry is reducing benefits, and we need to increase them. (Mother 4) My daughter’s speech sessions are far from our home. It would be a good idea if they gave benefits to the mothers. (Mother 7) I have diabetes and many household tasks. So, if the Ministry of Social Development could offer me a monthly allowance…I could hire other domestic workers. (Mother 1) I am satisfied with what God has blessed me with, but some benefits must be increased; I am worried about what will happen to my child after I die. (Mother 5) I am OK with my current money situation. Also, her siblings love her. Her older sister is helping me, I only worry about the future…I do not want her brothers to bear the burden when I die. (Mother 3) Yes, some children with DS were employed in the factories by the wasta. However, the employment is not real, and they are given salaries while they are in the homes because the factories obtain the benefits for the employment of the disability. (Mother 13)
Theme 2: Societal support
Societal support ensures the social functioning of children with DS. According to Bosc (2000), social functioning comprises interactions between an individual, their environment, and their ability to fulfill their role in that environment. Næss (2016) states that social functioning allows children with DS to function in a “normal” way.
Regarding the need for societal support, the mothers were asked, “What societal support do you need to maintain your children’s social functioning in the environment you live in?” Some of the answers are provided below. The children of others run away from my child, and do not play with him…mothers are afraid of my son. Bias is not just from children, but from mothers. (Mother 11) Society gives you unbearable torture. Some say that having this child is a punishment from God. In fact, I find that the mothers of my daughter’s friends are my best friends. (Mother 9) We still live in one house; my husband and his brothers are in one big house, and the truth is, once our family learned about my son’s condition, they were very supportive and talk to me daily, and they consider the child in their prayers. (Mother 2) The principal of the rehabilitation center is very respectful, and she fears God in everything she does, so I noticed that she encourages my daughter to receive great care so that her life remains as normal as possible. (Mother 7) I used to think that non-Muslim nurses would not treat my child well, but the nurse very much welcomed my child. (Mother 14) My son used to travel a hundred kilometers a day, so we moved to the city, there is a bias in the city against my son…I think about returning to our hamlet. (Mother 8)
Theme 3: Support with education and information
Saudi Arabia has ambitious policies to improve education for children with special needs. The education policy adopted best practices from the US (Alabri, 2017). However, the lack of well-qualified staff may make it difficult to provide these services.
People with disabilities in Saudi society are seen as unproductive, dependent, housebound, and unable to get a good job (Al-Shehri et al., 2008). However, there are attempts to provide many parent training programs with information on how to care for children with disabilities. Additionally, Saudi electronic media have arranged programs for parents to help them cope with DS. However, the productivity of these programs for improving disability care is undetermined (Al-Naami et al., 2010).
The researcher found that some answers reflected mothers’ desires for information: In fact, it was some negative beliefs about these children that made me not know anything about DS before my baby was born. (Mother 12) No one was available to give me more information; I am surprised, where is the honesty in the work that has been urged by our Islamic religion? How did they leave me like this without information? (Mother 4) I would often ask, how is he going to recover? I was lucky to meet my cousin, a nurse, and she was ready to provide better information than others. (Mother 5) Rehabilitation services are available in cities for children with disabilities…no place where my child can be rehabilitated close to my home…we do not have wasta to open, but in some villages, they do. (Mother 8) I did not know about the benefits or how to apply for them, and even when I learned, I did not want to go to apply; the community still asks me, when they see my daughter, what kind of disability does your daughter suffer from. (Mother 2) Children with DS are not getting access to special services such as speech therapy. The only service provider I know is a center at the military hospital, but you must have vitamin W [wasta] to get your son registered. (Mother 6)
Discussion
Having a child with DS places unique demands on mothers. The family, represented by the mother, is vital in Islam for social cohesion (Banu Az-Zubair, 2007). Therefore, mothers repeatedly mention their families with phrases like “my family,” “my son,” “my daughter,” and “for the sake of my family.” Mothers also repeatedly use religious and cultural phrases—religious words like “God,” “paradise,” “punishment,” and “supplication” and cultural words like “older sibling,” “wasta,” and “stigma.”
The Saudi Arabian government provides social development initiatives and social protection programs, and additional financial support comes from the Saudi royal family and other donations (JICA, 2002). The National Guard, military hospitals, and social security also offer extended support services. Despite the apparent abundance of support, government and private institutions are likely more concerned about the number of people with disabilities that they appear to help than those they have helped, leading to data distortion (Sijeeni, 2016). Most training programs are conducted by charity organizations under the auspices of the Ministry of Social Development (Al-Gain and Al-Abdulwahab, 2002). However, whether these programs improve disability care is still undetermined, and more attention is paid to health services than to education.
Intellectual and developmental disabilities can constitute a great risk where needs are not met (Heller and Factor, 1993). The participants identified their unmet needs across three categories: (a) need for financial and tangible support, (b) need for societal support, and (c) need for support with information.
Mothers enjoy parenting their children with DS, and they hope to gain entrance to heaven in exchange for caring for their children, according to the Islamic religion (Al-Gain and Al-Abdulwahab, 2002). However, the participants primarily needed financial and tangible support, which is often overlooked in the literature (Muir and Strnadová, 2014).
The Islamic Sharia emphasizes that people with disabilities should be able to live with dignity and benefit from welfare as other people do. People with DS can access a subsidy of SR 10,000 to convert their cars to meet their needs (JICA, 2002). The Council of Ministers Resolution Act 219 annually donates SR 30,000 to projects by disabled individuals through the General Department of Rehabilitation (JICA, 2002). The Council of Ministers Resolution Act 187 gives disabled individuals a 50% discount on public transportation (JICA, 2002).
The Provision Code of 2000 for Persons with Disabilities in the Kingdom of Saudi Arabia gives disabled people equal access to social, psychological, educational, and rehabilitative services through government-funded institutions (Alquraini, 2011). The Saudi Building Law of 2007 provides building accessibility measures to aid disabled individuals, although its applicability is unknown (Mulazadeh and Al-Harbi, 2016). Some criticize the Sharia laws for mostly focusing on medical disability but ignoring the social stigma experienced by disabled people (Mulazadeh and Al-Harbi, 2016).
The researcher found that some mothers of children with DS get a monthly allowance from the Ministry of Social Development, right from the child’s birth (Laws et al., 2000). However, the mothers must present their financial needs to the government and provide evidence that the monthly allowance they receive is still insufficient for their needs. They may need financial assistance or an additional allowance to cover their needs and provide for their families (Muir and Strnadová, 2014). Providing financial support to families can improve the quality of life for children with disabilities (Buzatto and Beresin, 2008). Although the Saudi government provides child benefits and free treatment to the disabled, mothers need financial benefits for other treatments, such as enabling their children to see a private speech therapist. Zuurmond et al. (2015) stress the importance of receiving individual treatments for these children.
Some previous studies disagree with this study’s conclusions. For instance, financial support is not the main concern for respondents in a similar study by Heller and Factor (1993). Nonetheless, the mothers in this study verify that caring for a child with DS can drain resources, particularly in families with many other children (Muir and Strnadová, 2014). Surprisingly, some mothers do not request for benefits, perhaps, because of shame attached to having a disabled child (Al-Gain and Al-Abdulwahab, 2002). In this study, only 3 of the 14 mothers were comfortable in asking for benefits without fear of shame.
In Saudi, the mothers play a major role in the family; therefore, they often suffer from exhaustion and need financial assistance to bring in a domestic worker (Alkohaiz, 2018). This finding is supported by previous research by Muir and Strnadová (2014) and Zuurmond et al. (2015), both of which found that financial support affects the families’ psychological, physical, and social well-being. Therefore, in Saudi culture, the role of the nanny is considered important for assisting the mother with her domestic tasks.
The second most vital need noted by the participants is societal support. One of the specific needs noted by the mothers was changing the cultural stigma associated with disability (Al-Gain and Al-Abdulwahab, 2002). Owing to the negative stigma surrounding DS, the mothers also noted that they need more social support from others (Clements and Read, 2008). Therefore, the participants would like society’s perceptions of children with DS to change. This would enable families to socially integrate in a better manner, which may lead to more positive attitudes toward people with DS (Huiracocha et al., 2017).
Furthermore, mothers would like to benefit from the experiences of other families who have overcome similar circumstances. This need was especially necessary when the mothers heard negative comments about their families or were told that their child was a punishment from God (Al-Gain and Al-Abdulwahab, 2002). Families tend to develop relationships with other families whose children share the same condition, likely because they better understand each other’s needs. In previous studies, mothers with children who have DS have reported great satisfaction from parental support groups (Marshall et al., 2015).
Children with DS may facilitate the support for their parents owing to their friendly nature, and the interviewed mothers were satisfied with the support they received from teachers, nurses, and other families (Esbensen et al., 2010). This indicates that people with DS seem to have become more acceptable to society, which is in line with previous studies that have concluded that families of children with DS may receive kindness and support from others (Huiracocha et al., 2017).
The researcher concludes that families experience challenges in their villages due to a lack of essential facilities such as established centers or programs and specialized hospitals for their disabled children. This forces families to relocate to bigger cities where these resources are available, leading to a potential lack of social support in smaller societies (Muir and Strnadová, 2014; Zuurmond et al., 2015). It seems that wasta is why some villages have disability service centers, while others do not (Hutchings and Weir, 2006).
The third need the participants expressed is knowledge-based support. Mothers need medical information and knowledge of service availability. However, mothers ranked this as the lowest need in this study. This is likely because all information requests for the Ministry of Social Development are now handled online, and the family’s older children can use the internet.
It is important to determine why some mothers are unaware of the services available at different doctors. Similar to the conclusions of Buzatto and Beresin (2008), the information that doctors provide focus solely on health and excludes other related information. Likewise, educational professionals only provide information on educational guidance without other types of guidance. Supporting the conclusions of previous studies (e.g., Alsem et al., 2014), this paper finds that educational guidance is often the only need that is met, whereas other needs are generally overlooked. However, one of the mothers’ cousin is a nurse who provided useful information, giving further evidence of the depth of Saudi families’ social cohesion (Alkohaiz, 2018).
This study concludes that mothers do not receive adequate information about services. Inadequate information results from negative views of DS, which can lead to a lack of knowledge of important resources, including rehabilitation centers, available government services, benefits, or early therapy. Heller and Factor (1993) also argue that families generally suffer from a lack of information regarding services for people with disabilities. Thus, the researcher agrees with the conclusion of Carr et al. (2016) that families need general information regarding the services and resources they can access.
Conclusions
One of the strengths of this study is the use of a qualitative approach to provide conclusions of maternal perceptions and link the findings to the unique religious and cultural context of Saudi Arabia (Gargiulo and Bouck, 2018). However, there are some limitations as well as strong implications for further research.
Several limitations should be considered in interpreting the results. The first relates to the small sample, related to the exploratory nature of this study, as well as its limited timeframe and resources. As the sample is not representative of mothers of children with DS in all regions of Saudi Arabia, the current results should be interpreted with caution. Similar studies in other regions may be useful for making comparisons. Second, the small sample size also impacts the generalizability of the results. However, the study did not aim to produce generalizable results, but rather to identify emerging issues and directions for future research, and to provide recommendations for those supporting families of children with DS. Future studies aimed at producing more comprehensive results, using larger and a more representative sample size, are recommended.
Third, the research did not determine the needs of mothers with children too young to be enrolled in an education program. While this omission is not significant enough to alter the research findings, more research is needed to determine the needs of families of children with DS aged 1–3 years.
Fourth, interviews were conducted without the presence of any other family members. Thus, the results should be understood as only the mothers’ perceptions of their families’ specific needs. The reason for the researcher’s focus on mothers is that, according to Saudi culture, mothers take care of the home, and are responsible for the children. They are also expected to understand the needs of the whole family, including children with DS. The researcher’s position, as the father of a daughter with DS, plays a supportive role, similar to that of other Saudi fathers, i.e. providing support to meet the needs of the family, rather than knowing the needs of the family. However, there may be a demand for further research regarding the difficulties parents have in meeting the needs of a family with a DS child.
Another limitation is that the researcher is a man interviewing women in conservative Saudi society. However, owing to the importance of the subject of the study, the researcher succeeded in conducting telephonic interviews, as it is more respectable for interviews between men and women to be conducted telephonically, rather than in person, which is acceptable in Saudi society. The researcher, as mentioned earlier, is the volunteer mothers contact telephonically after the birth of their children with DS, to ask for advice related to their children or their families, resulting in a trusting and respectful relationship between the researcher and participants. Despite the sensitivity of the research topic, and known to the mothers, the researcher does not have any authority in the Ministry of Social Development, which is responsible for benefits and services for disabled children and their families in Saudi Arabia, and the mothers did not link the researcher to this authority. Hence, the mothers could discuss the topic frankly, without fear of negative consequences arising from any of their statements. However, it may be useful to consider a similar study conducted by a female researcher to verify the effect of the researcher’s gender on the results.
For cultural reasons, the interviews were conducted telephonically, with some drawbacks, such as not being able to see facial expressions and gestures; occasional breaks in communication; and the possibility of disturbance from the children in the mothers’ care. In addition, some questions generated short answers, while some responses were interrupted by the researcher mid-thought, believing that the participant had stopped speaking. Despite this limitation, the use of the telephone allowed the male researcher to reach mothers of children with DS. Although the telephone interview provided flexibility and comfort to the participating mothers, it could be eliminated in a similar future study conducted by a female researcher with interviews being conducted face to face.
Finally, the study sample was recruited from the Eastern Province of Saudi Arabia. This is a multicultural region and was the first in Saudi Arabia to have developed due to the location of oil company ARAMCO in the region. As many residents work for ARAMCO, which offers Corporate Social Responsibilities, they tend to have access to better educational services. Therefore, similar research may yield different findings in other regions.
Regardless, this study is significant in considering the needs of families of children with DS through the mother’s perspective and expands the literature, demonstrating the unique needs of these mothers in Saudi Arabia’s cultural and religious context.
In conclusion, the study found that mothers’ needs are ranked as follows: financial and tangible support, societal support, and knowledge-based support. This research has great significance for policymakers who can use these findings to implement appropriate policies to meet the needs of children with DS and their families, such as the financial demands of both the family and the child, an increase of families’ monthly allowances, and implementing a new benefit for mothers.
It is recommended that the government increase centers for family activities to help societally integrate these families. This process could be aided by researching each village’s needs and limiting the wasta when opening centers. Information regarding financial and tangible available support, medical information about DS, and information on the services available to children with disabilities should be readily available. Policymakers must aim to meet these needs within Saudi’s religious and cultural context to limit any clashes between system development and religious and cultural aspects.
The current findings provide a starting point for understanding the needs of families of children with DS, advancing support for these families, and improving their quality of life. The researcher looks toward officials to transform these recommendations into reality.
Footnotes
Acknowledgments
The researcher thanks Shumua Al Amal from the Special Needs & Rehabilitation Center, Dammam, Saudi Arabia for their interest in the study and for providing the study sample. The researcher also thanks all mothers who participated. Finally, the researcher would like to thank Editage (![]() ) for English language editing.
) for English language editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.