
Abstract
The oral health of people with intellectual and developmental disability is poorer than that of the general community. Any solution for people with intellectual and developmental disability living in residential services needs to include disability support workers (DSWs). Previous studies have used either didactic or train-the-trainer approaches to enhance DSW knowledge and skills. Taking a different approach, a novel program used DSWs as embedded oral health champions. This model provided educational opportunities for DSWs to learn about good oral health and then share with peers and provide benefits to people with intellectual and developmental disability that they support. Interviews with a sample of these champions were conducted and analysed using content analysis. Findings suggest that DSWs are capable of affecting change with the right type and depth of training, management and organisational support. A DSW-led champions model has merit, however requires ongoing expert support to help maintain and sustain benefits over time.
Background
Compared to the general population, people with intellectual and developmental disability have poorer oral health status, including higher plaque levels, more severe gum disease, higher rates of untreated tooth decay, higher number of teeth removed, and fewer natural teeth (Ward et al., 2019; Wilson et al., 2019b). Loss of a functional dentition has serious consequences, including problems with chewing, swallowing, nutrition, speech, pain, and systemic health conditions. Poor oral health is largely preventable through proactive oral care support. Although people with intellectual and developmental disability experience many health inequalities compared with the general population, inequalities in oral health may be the inequalities most likely to reduce with improvements and personalisation in direct care and support (Wilson et al., 2019a). Where people are dependent on paid disability support workers to meet their health needs, any intervention must address the disability support worker’s knowledge and behaviour to improve oral health outcomes (Frenkel et al., 2002; MacEntee et al., 2007). Insights into novel ways that disability support workers can provide better oral health support will help build the evidence base in this area of practice.
A functional and infection-free face is generally accepted as a broad expression of good oral health. Glick et al. (2016) defined oral health as “the ability to speak, smile, smell, taste, touch, chew, swallow and convey a range of emotions through facial expressions with confidence and without pain, discomfort and disease of the craniofacial complex” (p.793). Impaired oral health is not only associated with lower quality of life, but also a higher prevalence of systemic diseases (Wilson et al., 2019a). Poor oral health is largely preventable through proactive oral care support. An important aspect of this involves supporting nutrition and food choices which promote oral health. For instance, Kabil and Eltawil (2017) reported that dental caries are a multifactorial disease and, as such, have several risk factors in their development. These include inadequate tooth brushing, poor oral hygiene, and excessive consumption of sugar, as well as factors such as eating disorders and atypical diets (Lee and Chang, 2021).
A recent study by Tenelanda-López et al. (2020) on the relationship of eating habits to oral health of young people in school found that consumption of vegetables and greens significantly reduced the risk of Decayed, Missing and Filled Teeth (DMFT) index, as did the consumption of fruits. The beneficial effect of fruit consumption has also been reported in a randomised study on the effect of eating fruit on periodontal inflammation (Fridell et al., 2018). The researchers attributed this effect to the antioxidants commonly present in fruits and their anti-inflammatory properties. A systematic review and meta-analysis on the effect of sugar-sweetened beverages (SSB) on oral health (Valenzuela et al., 2020) revealed a significantly increased risk of caries, decayed, missing and filled teeth, and erosion with moderate to low consumption of SSB. The food we eat influences the types of bacteria that inhabit the oral cavity, many using the sugars to synthesise enamel corroding acids under the protection of plaque. The profile and health of the person’s oral microflora is among the strong predictors of dental caries and periodontal diseases; managing the resident oral microflora can therefore help to improve oral health (Marsh and Devine, 2011). Many people with intellectual and developmental disability rely largely on disability support workers for the planning, shopping for and preparation of, their meals. This dependence, together with the high prevalence of eating disorders reported in this group, puts people with intellectual and developmental disability at greater risk of poor nutrition, and subsequently poorer oral health, if left unmanaged (Humphries et al., 2009).
Disability support workers are in a unique position to influence oral health among people with intellectual and developmental disability. Due to their close relationship, they have the potential to promote healthy oral hygiene habits and screen for early signs of dental disease (Wilson et al., 2019a, 2019b). However, there are numerous barriers for disability support workers to undertake this role. These include factors associated with the person with intellectual and developmental disability such as a lack of understanding about the importance of oral health (Chadwick et al., 2018), difficulty adhering to oral hygiene care (Thole et al., 2010), and anxiety about dental treatment (Versloot et al., 2008; Chadwick et al., 2018). Challenges accessing dentists who are skilled to treat people with intellectual and developmental disability have also been noted (Pradhan et al., 2009). There are numerous barriers from the disability support workers perspective as well such as time constraints (Thole et al., 2010), fatigue (Wiener et al., 2016), caregiver burden (Chi et al., 2014), and a lack of knowledge and training in oral health among disability support workers (Chadwick et al., 2018; Eijsink et al., 2018; Wilson et al., 2019a).
Several strategies have been explored to capacity build disability support workers in promoting oral health care. Studies of didactic education programs have reported some successes in improving knowledge and confidence of support workers immediately following training (Glassman and Miller, 2006), with a general improvement in attitudes and behaviours (Faulks and Hennequin, 2000; Mac Giolla Phadraig et al., 2013). Some other education programs have resulted in significant increase in the frequency of toothbrushing among people with intellectual and developmental disability and improved ability of disability support workers to assist with this important oral hygiene task (Faulks and Hennequin, 2000; Binkley et al., 2014). Nevertheless, there is a lack of larger studies, particularly in Australia, into the post-educational impact of oral health training for disability support workers on their practices over time, and its influence in the workplace with respect to dental care routines. Further, there is no evidence about the appropriateness, feasibility and effectiveness of novel approaches, such as disability support worker led, and peer-based, champions approach.
Aims
This qualitative study will help fill this gap by exploring disability support worker insights from a novel approach to oral health using disability support workers as peer-led “champions”. Further, the qualitative data will offer insights into how the program can be enhanced in the future, as well as help identity the range of outcome measures that could be explored in a future experimental study. This study aims to explore the champions’ perspectives of the oral health champions program, their influence as champions within disability services, and to document their perception of successes and limitations of the program.
Methods
Research Design and Study Overview
As the nature of this study was exploratory and based directly on the individual insights of disability support workers who acted as oral health champions, and their practices, a qualitative descriptive design was used with content analysis selected to methodically analyse interview data. Qualitative description is best used when seeking to interpret qualitative data, but not moving too far from a literal description of the data, and to provide a rich description of the participant’s experience that is unpacked in easy to understand language (Bradshaw et al., 2017). Individual interviews were conducted with a group of oral health champions from a single disability service in Victoria, Australia. A semi-structured interview schedule was designed to gain insights into the following areas of inquiry: (a) motivation to become an oral health champion, (b) understanding of oral health and the oral health status of people with intellectual and developmental disability in their care, (c) perspectives of the oral health champions program, (d) local initiatives as a result of the oral health champions program, and (e) summary of time being an oral health champion. The COREQ checklist (Tong et al., 2007) was used in both the design and write up of the study results.
Ethics and Consent
Ethics approval was granted from the Western Sydney University Human Research Ethics Committee in April 2020 (Approval ID: H13784). Written informed consent was gained from all participants prior to conducting an interview; verbal consent to record each interview was obtained before proceeding with the interview. No adverse events were reported and no participants withdrew from the study.
Program Description and Context
In Victoria, the lead state public oral health agency, Dental Health Services Victoria, partnered with a disability service (gen-U) to develop approaches for improving the oral health outcomes of people with a disability living in shared accommodation. Through discussion it was decided that an approach worth pursuing was an oral health champions program. The aim of the program was to shine a light on oral health for gen-U and to support the development and implementation of oral health policies, procedures, and practices within the adult specialised accommodation service. The role of oral health champions was to: • Promote and role model behaviours which are good for oral health such as healthy eating and drinking tap water • Help their teams to identify risk factors for poor oral health in residences and work to address them • Share basic oral health information with residents and families that can build their understanding of how to prevent oral disease • Encourage appropriate and consistent oral health care for every genU resident by supporting the development of Duty Care statements for each person • Make sure new staff know about champions and their role, and • Look for opportunities where things can be done better for better oral health.
Intervention Description, modified using TiDieR criteria (Hoffman et al., 2014).
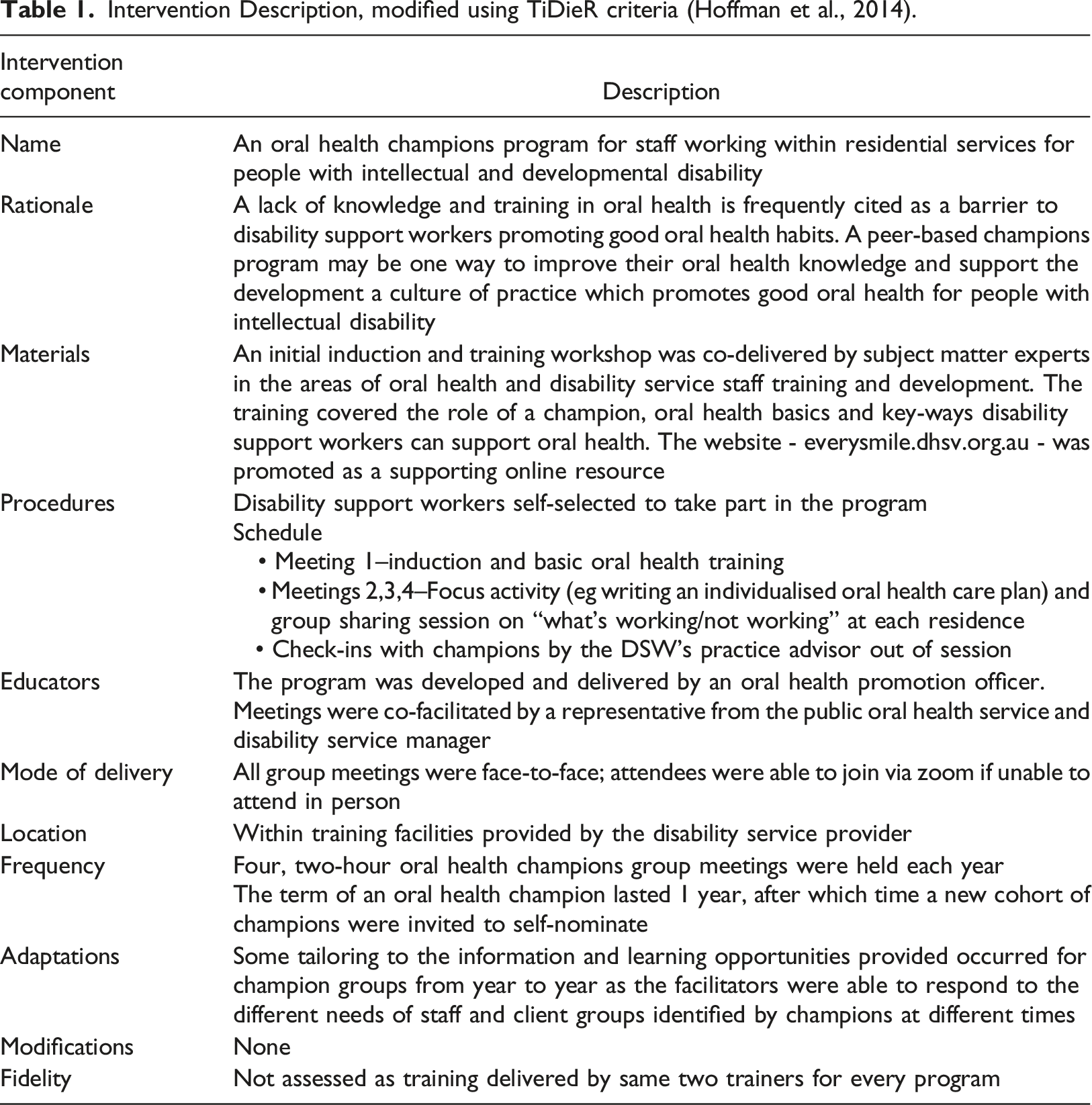
At the time of writing, gen-U provides specialised accommodation to approximately 200 adults with disabilities across approximately 40 different geographical contexts in Victoria, Australia. Not all sites have been involved in the program as the number of services have doubled in size over the last couple of years. The accommodation model consists mainly of community-based group homes for mostly between three and six adult clients with intellectual and developmental disability and/or other lifelong disabilities. All homes are staffed by disability support workers, who have the qualification Certificate IV in Disability Work that usually takes 12 months to attain from a registered vocational training provider. Gen-U does not offer the services of a specialised health team - consisting of registered health professionals such as registered nurses or occupational therapists – to its clients, rather all clients are supported to access mainstream health services in their community.
A disability support worker associated with each residence served as that house’s oral health champion for the period of 1 year. Program content was developed by an oral health promotion professional (fourth author) which required approximately 8 hours of time to research and repurpose existing training resources to suit this particular cohort. A further 8 hours of the oral health promotion professional’s time was taken up in co-delivering all of the face-to-face sessions. The program involved an initial face-to-face induction workshop (to identify what it means to be a champion, to better understand oral health basics, and to identify ways that oral health can be supported), followed by three other meetings within the year to discuss progress, challenges and successes. Workshop content included basic information on the teeth and mouth, signs and impacts of poor oral health, key factors that promote good oral health (including good diet, regular cleaning of teeth, gums and any dentures), and the factors which increase a person’s likelihood of oral disease. At the end of a champion’s 1 year term, the position was filled in most cases by a different disability support worker at each residence.
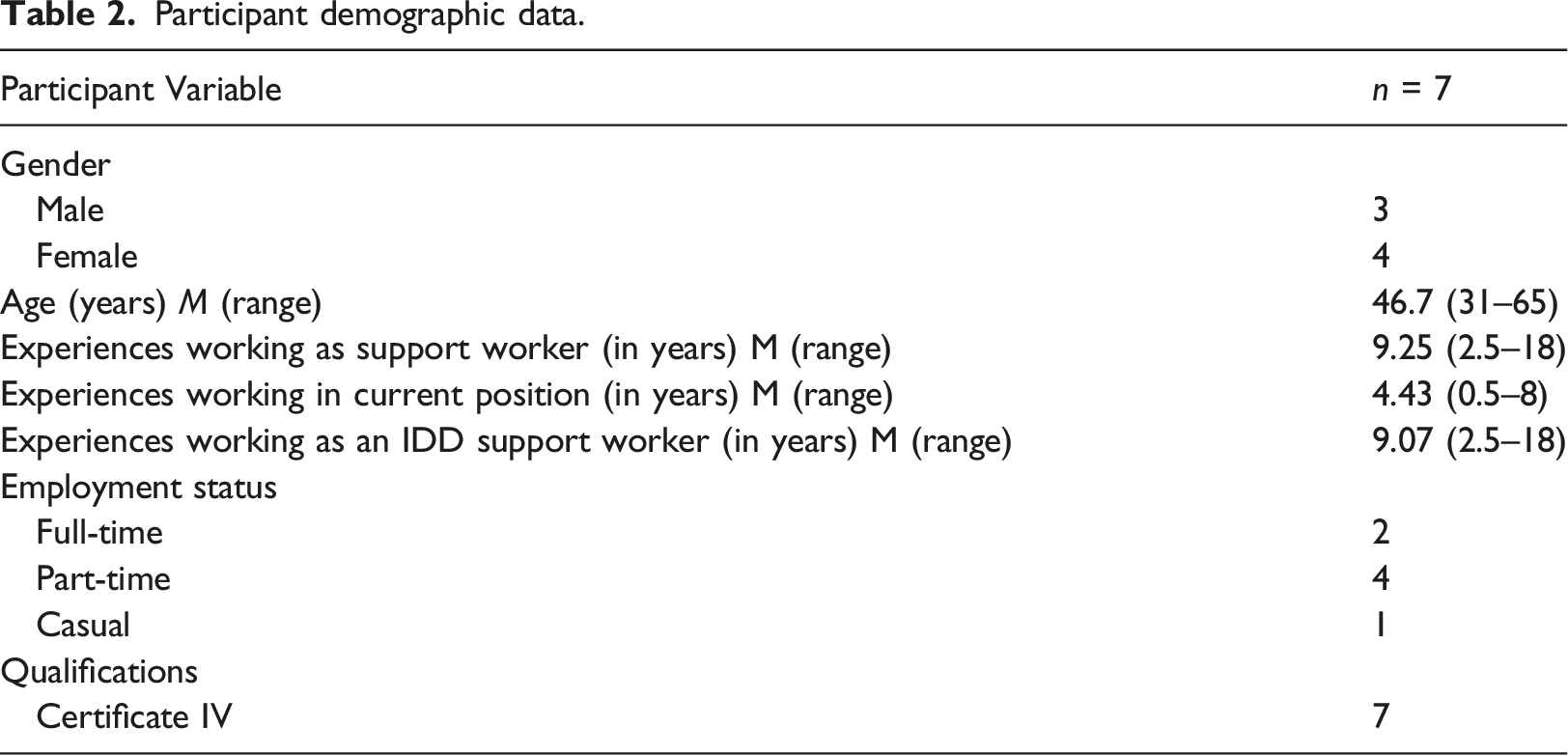
Participants
Participant demographic data.
Procedure
Recruitment was at arms-length from the lead researchers; the third author, a manager with the disability service, disseminated via an internal email the participant information sheets to all current and past oral health champions (approximately n = 40), which included all relevant documentation about the study and an invitation to contact the lead researchers via email with a view to participating in an individual interview. All interviews were conducted using video conferencing software. Interviews were conducted between June and July, 2020 and lasted on average 29.7 minutes, with a range from 21 to 39 minutes in duration. All interviews were digitally recorded and transcribed verbatim by a professional transcription service; participant names were replaced by pseudonyms.
Data Analysis
Data were analysed using content analysis as a more objective summary of the interview data was desired rather than a more interpretive creation of themes as would be the case with thematic analysis (Neuendorf, 2019). First, a series of codes and an Excel codebook were developed by the first two authors based directly on the concepts within the semi-structured interview schedule. Next, the second author led the interview analysis by reading each transcript line-by-line and adding content that matched each code, into the codebook. The next stage involved inter-coder reliability checks where the fifth author double-checked the content of all codes after first conducting their own line-by-line review of all transcripts.
Trustworthiness
All authors have a unique interest in oral health and finding ways to enhance the oral health status of people with intellectual and developmental disability and to create systems that work for these people and the support networks around them. The third and fourth authors were not involved in any of the data collection or preliminary analyses as they were responsible for the design and delivery of the program. Interviews were conducted by the first and second authors, both registered nurses skilled in interviewing based in a different Australian state to the participants and were not known at all to the participants. The first, second and fifth authors reviewed all verbatim transcripts and collaborated on decisions relating to each descriptive category. Finally, agreement on the content of all codes was reached at a team meeting where the first, second and fifth authors discussed the data analysis in detail. The varied professional and vocational backgrounds of the entire research team–two registered nurse researchers (one male and one female) with expertise in intellectual and developmental disability, one female clinical dental health professionals, one male oral health researcher, one female educational expert working within the disability service, and one male nutrition academic and expert-contributed to theoretical triangulation of the interpretation of results. No member checking was conducted as the study used content analysis, rather than a thematic analysis, rendering member checking of limited value.
Results
Motivation to be an Oral Health Champion
Although all participants were reportedly happy about being an oral health champion, very few were driven by a direct desire to counter the poor oral health status of their clients or to change substandard practices. Rather, most took advantage of a serendipitous vacancy within their house or an invitation from senior staff, for example: “It is just a coincidence because the house I was working on was just taken over by the new management, so it was just good time for me to step into that role” (participant_05) and “I got asked by the previous champion and because we have had new staff come in [to work at the house]” (participant_06). Some did, however, use the invitation as an opportunity to provide a focus on oral health: “I guess it [oral health of clients] is not something that I really thought too much about … until I guess it was brought to our attention that this program would benefit everyone … I thought yes that is something I can do, as I guess oral health sometimes is a bit forgotten about.” (participant_02)
Perceived oral Health Status of Clients Prior to Program
When asked about the oral health status of their clients prior to the program commencing, very few participants responded specifically about the issues that constitute one’s oral health status, rather participants talked in more general terms about service processes and barriers. For example, one participant referred to there being “…no routine for the residents to brush their teeth or take care of their oral health … sometimes they were left out for a couple of days” (participant_05) and another participant declaring that “ they [the clients] would still brush their teeth but … not as good as it should have been” (participant_04). Oral health plans were previously not universally present for all clients, unlike now where every client has a duty statement: “there used to be [oral health] duty statements for some residents” (participant_03). Noted barriers to better oral health included not having “the communication to tell us where I have a sore tooth” (participant_04) and that “some residents [clients] will not like to brush their teeth” (participant_03).
Reflections on Understanding of Oral Health Prior to Program
In order to ascertain participant’s knowledge about oral health prior to the program, they were asked to reflect upon how they might have defined it beforehand. Responses showed a limited conceptualisation of oral health, however participants reflected on some personal limitations prior to the program, for instance: “Prior to do[ing] the oral health champion [program], I wouldn’t have thought that within the house it was of very high importance and for myself personally … I had a lot of misconceived ideas” (participant_07) and “before I went to that meeting at the workshop, I used to brush my teeth only in the morning and never brushed my teeth before bedtime” (participant_05).
Reflections on Initial Program Training Day
Recollections about the structure of the initial program training day was that it was based on three key points: “what we are doing and do we need to keep doing [it], the second one, what we can do better, and [thirdly] what are the challenges?” (participant_03) Participants reported learning a number of new and important facts from the training, such as “flossing is very important, I knew it was, but the mouthwash that was a big eye opener, not to use it because … it can damage the enamel” (participant_06), that “it was a big eye opener for me as well so like the amount of sugar in drinks, daily intake that was discussed, you know they were explaining how good is the tap water” (participant_05) and that “some toothpastes have got not enough fluoride” (participant_06). Nutritional issues, and that “diet impacts on your oral health” (participant_01), were also key learnings: “they have educated us on what fruits and veggies are better for you … fruits like grapes are high in sugar, the bananas are high in sugar, apples are good because they are crunchy and hard so the softer fruits don’t clean your teeth as good as the harder fruits … [that] sort of act like a bit of an abrasive and brush your teeth as well.” (participant_06)
Reflections on follow-up meetings over the 12 months of being an oral health champion
In addition to gaining added knowledge from the oral health experts who were facilitating these follow-up sessions, participants reported learning added information and tips–“sharing stories and sharing strategies”-from their colleagues working in other parts of the disability service. Nevertheless, there was an apparent tension between what seemed possible within the meetings, and what was actually achievable as sometimes “in the staff’s [non-champions] minds you had the resistance that no that is not the way it is done” (participant_07). For instance, some initiatives met resistance in different workplaces: “you gain the knowledge from the experts themselves and then you are able to listen to what is happening in other areas and things that they have done to be able to implement it, and that is all good knowledge to have, but imparting that knowledge onto your fellow co-workers within the house that you are working and also trying to implement changes for residents, that is where it breaks down” (participant_07).
Specific client characteristics, as well as “the point that the residents at the end of the day have the right to say no” (participant_07), were other noted barriers to implementing strategies that worked in one area, but perhaps not in others: “The houses that had staff on board were able to do things like take away cordial, put water on the table, all of those sorts of things but when the house that I worked in, we had four residents at the time but we had one resident who was very or could be very aggressive so if he didn’t get what he wanted you could have behaviours so therefore even though we tried to implement things that other houses had done, it was because of the resident’s aggression that we often failed.” (participant_07)
What Initiatives were Implemented?
Participants reported a number of broad-ranging initiatives, mostly group home initiatives that served to enhance the oral health of their clients. The need for every client to have an oral health care plan, contained within a duty statement, was achieved by allocating “… a key worker and from then that person would then complete the duty statement, dental appointments, follow up with the dental and other sort of things” (participant_05). Group home initiatives included adding an oral health agenda item to both staff and house meetings to “… share with the team, and I also have a recap of what we have shared before, how that has been implemented so far, and what are the things we need to do” (participant_03). One participant talked about inviting a client along to a staff meeting to help convey a stronger message about pride and participation: “I would take one of my residents [to the staff meeting] as well, just to share how she or he was before this particular thing was introduced, how he/she is feeling about the whole process at the moment and what they are struggling with, what their experience are … let them share” (participant_03).
The creation of checklists and charts where clients and/or staff can “put a tick mark” to indicate that oral health has been undertaken/supported for each client were also reportedly added along with some posters “on the bathroom doors and the toilet area [stating] have you cleaned your teeth?” (participant_03). Nutritional initiatives included having “less sugar in the house, getting them [the clients] to drink healthy options, eating healthier, more fruit, less junk, more vegies” (participant_06) as well as buying “a water bottle for every resident which they introduced when they went out wherever possible” (participant_03). Procedures to replace worn out brushes were also implemented: “at least every 3 months each resident was going out and purchasing a new toothbrush, and making up like a roster and putting it in the house diary of when they are due for a new toothbrush” (participant_02). Some strategies were reliant on every team member to implement, which wasn’t always achievable: “we tried to encourage the drinking of water at meal times … but again it was up to the individual support workers and what their beliefs were as to whether they were implementing and implemented correctly” (participant_07).
Some individualized behavior changes were noted by participants, and included a young autistic woman who needed to increase the amount of time spent brushing her teeth as it generally only last for 5-20 seconds. The staff worked with the OT to develop an individualised strategy that leveraged off the young woman’s interest in looking in the mirror. Teeth cleaning was altered from during a morning shower to when using the mirror after the shower “where she is more willing to do it [brush her teeth] for longer” (participant_04). A second example related to a young man with intellectual and developmental disability who also used a wheelchair and could not only brush his teeth, but quite enjoyed doing so with support. Prior to the program, he would request to do this only in the morning, but after the program staff added an evening tooth brushing session: “we weren’t aware that is something he would like to do [brush his teeth twice a day] because he never told us and because he cleaned his teeth in the morning we were on the understanding that as long as he cleaned his teeth in the morning that was all that was required and after the oral health champion, [we were told] they should be cleaning [their teeth] at least twice a day … when he was given the opportunity to do so, he thoroughly enjoyed it!” (participant_07)
Summary of oral Health Champions Program
Participants were asked to sum up the program as whole, and comment on what worked well, and what didn’t work so well. Most significantly, there was widespread agreement that many changes had occurred, there was “a lot more conversation on oral health”, and in addition to the nutrition and drink choices mentioned previously, specifically that teeth brushing had become a more important and discussed topic: “yes I think that is it, the culture, the brushing teeth culture has changed” (participant_05) and “people are more aware of the importance of brushing their teeth” (participant_06). Edentulism and oral health was another area of new knowledge: “one of the gentlemen had … dentures, but never wore them so we never ever understood before I became dental health champion that it was just as important to him to clean his gums as what it was for others to clean their teeth” (participant_7). In addition, awareness of individual need in relation to appropriate dental practitioners was noted: “it also brought up the conversation around dentists and suitable dentists for particular people … some residents who are more than fine to go to a normal dentist, but others I really find the community health centre dentists [are best]” (participant_04). In terms of what presented the greatest challenge, the reported reluctance of some staff to adjust to new routines and/or initiatives was the most common issue: “Well I had personally got him from drinking cordial and coke and soft drinks at meal times to drinking a glass of water … perseverance [was critical to this success], but then that perseverance was always, and can always be, undermined by others because as soon as someone else relents, then that creates another pattern of behaviour so when you go back to do it you get the resistance again.” (participant_07)
Likewise, clients could also present champions with difficulties when trying to implement change: “Overall it [the changes in the house] was smooth, but again the residents choice will be bit of a challenging at times, some residents choose not to follow the changes, sometimes part of staff as well, we need to be consistent in supporting the residents.“(participant_03)
One participant clarified that this resistance was quite deeply ingrained: “it is not only the fact you have support workers who don’t believe in what you are doing, they also don’t believe we have a right to make someone do something” (participant_07). Participant seven also referred to the challenges of trying to alter what were often lifelong routines, such as new knowledge that rinsing after brushing was not needed and, unless recommended by an oral health professional, using mouthwash was not effective: “… that is really difficult … it is something they have done all their life and now all of a sudden we are telling them no, they don’t do that anymore and very difficult to break the cycle and very difficult for families to get on board and other staff members because it is something they instilled in you all your life and then all of a sudden one person comes along and says no you are not supposed to do that”.
Discussion
For the first time, this research provides an insight into a novel, disability support worker-led champions-based, approach to improving the oral health of people with intellectual and developmental disability. The qualitative findings from seven oral health champions, all employed as disability support workers with a trades-level, vocational Certificate IV in Disability Support, suggest that while the program had enhanced individual knowledge and led to a number of reported benefits to the people with intellectual and developmental disability that they support, underlying these benefits were various challenges of being a champion and effecting change in settings where routines and practices were sometimes entrenched. Importantly, it seems clear that the initial, and follow-up, workshops promoted awareness that oral health was more than just cleaning teeth and in fact altered the personal practice of some of the champions. That is, similar to other oral health educational interventions (e.g., Selbera et al., 2021), the workshop increased knowledge by raising awareness of the multitude of interacting factors related to oral health such as the importance of nutrition, guidelines on the frequency of brushing, timeframes for when to change toothbrushes, reducing consumption of sugary drinks, and caring for dentures.
Insights about and changes to nutrition, in particular snacks, were commonly reported and will have important longer-term impacts, in particular as any improvements to reportedly low nutritional status is vital to promoting overall health and wellbeing (Humphries et al., 2009). The disability support workers have taken the initiative to educate and encourage the people with intellectual and developmental disability who they support to replace sugary drinks with water, and made fresh fruit more accessible for snacks between meals. Nevertheless, the broader awareness of what constitutes nutritious diets across all meals that are most supportive of oral health, has reported to be lacking among disability support workers (Hamzaid, et al., 2018), and adding this to their educational training in this regard would be beneficial for the oral health of the people with intellectual and developmental disability. Further, nutritional and swallowing screening could also be helpful in identifying people with intellectual and developmental disability who require more urgent dietary adjustments (Stewart, 2003) and the expertise of a dietitian could value-add any future champions program.
Oral health champions were provided with a range of strategies to improve the oral health of the people with intellectual and developmental disability they support. Many of the strategies to improve oral health were about group-home procedures and routines, such as posters, shopping lists and checklists, as well as some individually-focussed interventions to ameliorate specific problems. While the oral health champions generally had a positive response to the program and felt that the workshops were worthwhile and beneficial to improving their support of others, it remains difficult to know to what extent any of the changes to procedures and routines had a notable effect on the oral health status of any individuals with intellectual and developmental disability. Notably, other programs have reported a significant increase in caregiver oral health knowledge, but not for oral health behaviours and attitudes (Selbera et al., 2021). Although the routine-led description of most strategies were within the expected scope of practice of a vocationally-trained disability support worker, it still prompts reflection on what, and how much, can be expected from disability support workers with respect to health-specific interventions given that they are not trained and registered health professionals. In particular, where some of the key messages from the training were actually more nuanced or carried far less weight of importance than some of the participant’s recollection suggested. For instance, suggesting that mouthwash was universally not good, was not a key message of the training, rather it was a more brief reference to the fact that the alcohol in many easily available mouthwashes can be detrimental to oral health, while in fact fluoride-containing mouthwashes may be beneficial to some people, and can be used on the advice of an oral health professional. Further, rich descriptions by some participants about particular fruits and vegetables being better or worse for oral health, is also not in line with what was covered in the training. This is an important finding as the risk of misunderstandings offers an opportunity to reflect on the program and the need to keep future key messages clear and straightforward, provide opportunities to assess understanding as part of training as well as the use of refresher training/quizzes as reminders of these key messages over time.
An apparent greater focus on group home procedures and routines rather than interventions at the individual level, could be a reflection of the audit-heavy world of the disability support worker, where procedures, checklists and task analyses provide auditors with much of the evidence for quality service provision. That being said, no participants mentioned the oral health policy that gen-U had developed at the start of this program, which further reinforces the notion that the disability support worker worldview is more focussed on procedures and direct tasks within their working context, or indeed that increased knowledge doesn’t equate to increased behaviours or attitudes (Selbera et al., 2021). Hastings (2010) discussed the characteristics of research about disability support workers, and argued that there had been many problem-led studies about describing or remediating disability support worker behaviour through targeted training strategies, and a suite of studies about disability support worker stress and burnout. Arguably, one could also add to Hasting’s summary the myriad of studies describing staff attitudes toward and responses to the sexuality and sexual expression of people with intellectual and developmental disability (Wilson and Frawley, 2016). Missing, suggested Hastings (2010), was a focus on three areas: measuring the dimensions and quality of staff-client relationships, allowing clients with intellectual and developmental disability to report on their perspectives of these relationships, and exploring the range of outcomes from these relationships in terms of the wellbeing of people with intellectual and developmental disability. This study falls into the third area suggested by Hastings (2010), and although this was a descriptive study with no outcome measures as such, it does raise some questions about the way that disability support workers perceive their role, as well as the relationships of disability support workers to each other and their clients, to affect the types of positive change needed to produce better outcomes. That is, a sense of the disempowerment within disability support workers when they are unable, or lack the skills, to take other disability support workers on a journey of change, in this instance, related to oral health. Ultimately, the reported resistance of some disability support workers to participating in some new routines and initiatives highlights their agency as possible gatekeepers against positive change. The disability support worker scope of practice also needs to be considered here, and in particular a balanced view of what should be expected of a disability support worker with regard to oral health. Although disability support workers should not be pressured into feeling like they are a health professional with expertise in oral health, there are many things that they can do on a day-to-day basis that can minimise downstream problems.
The literature describing staff training approaches to oral health and people with intellectual and developmental disability has primarily been based on didactic and practice-based approaches to disability support worker oral health knowledge and practical technique (Binkley et al., 2104; Faulks and Hennequin, 2000; Fickert and Ross, 2012) as well as a train-the-trainer approach to oral health knowledge and practice where group home managers were trained to train their disability support worker staff (Mac Giolla Phadraig et al., 2013). Using a peer-based champions program is novel, and in the absence of any outcomes data, the question arises did it work and, if so, what could be improved. In the absence of any reported data about a champions program specific to oral health, a review of some studies from the wider health literature raise concern about the perception of a named champion being an actual expert, when in fact they are not, and the burden of unrealistic expectations on these champions (Brown et al., 2018). Although none of the seven participants in this study reported feelings of others having unrealistic expectations of them, they did report frustration at not being able to affect some straightforward procedural/routine changes, related to a lack of buy-in from other disability support workers, clients and families.
An alternative approach could be to consider whether a funding stream within the Australian National Disability Insurance Scheme (NDIS) would fund an actual oral health promotion professional, who does have the authority and expertise that disability support workers may not possess. For instance, a role similar to allied health professionals who are funded by the NDIS to consult, assess and draft plans of care that are delegated to disability support workers to follow. In this champions program, the oral health promotion expertise was funded through time-limited government health promotion funding rather than the disability service, and it was the time and associated cost of the gen-U manager to oversee, organise and keep the program going that better reflects the true cost to a disability service. That is, funding which supported the involvement of the oral health promotion expert no longer exists, and without the gen-U manager, who although highly skilled and who fulfilled the role of the champion’s champion but was not a health professional, the likelihood of the program collapsing would be high. Although new government funding would be needed as the previous oral health promotion funding no longer exists, would a directly funded health professional, with expertise in oral health and operating like other health professionals in the disability sector, be a more efficient and effective use of overall taxpayer funds?
Implications for a Future Champions Program
The study findings highlight the potential benefits of an oral health champion program to capacity build disability support workers to promote oral health among disability services. That is, a novel peer-based program to act as an agent of culture change, as much as procedural changes, as well as giving ownership to disability support workers. However, various strategies need to be considered to enhance the feasibility and sustainability of such programs into the future. Firstly, the resistance from some non-champion disability support workers towards making oral health routine and practice changes needs to be managed through organisational leadership and culture change from a grass-roots level. Policy makers may need to explore potential incentives to facilitate such a change. The program could also be complemented by facilitating access to dietitians who can provide valuable nutritional advice to maintain good oral health. In addition, linking in with dental professionals through an integrated approach could assist disability support workers dealing with clients who have severe oral health problems and help better monitor oral health of individuals. It could also alleviate some of the concerns of disability support workers regarding their scope of practice in oral health promotion. Future intervention studies are also needed to assess the impact of the program on the knowledge and confidence of support workers to promote oral health as well the oral health status and behaviors of their clients. Key outcome measures would include measurement of change in the champions level of knowledge, confidence and competence in the area of oral health, detailed mapping and measurement of the impact of change with respect to the number and range of new plans, processes, procedures and strategies, and finally measurement of the oral health status of people with intellectual and developmental disability before and after the advent of such a program. Finally, as one aspect of the program was to seek to be an agent of culture change across the entire organisation, measuring what and how cultural issues may change, over time, would yield interesting insights into the wider impact across the whole disability service.
Limitations
The main limitation of this study is the possibility that those who consented to participate, may not be reflective of the overall cohort of oral health champions, nevertheless we recruited information rich participants who gave detailed accounts of their experiences. How being in the research was perceived by participants and how invested they actually are in promoting oral health is unclear. Having totally independent interviewers and researchers involved also means that the potential for response bias is real. For instance, although few instances of individualised interventions were reported by participants, authors three and four ran the program and attended all workshops and can attest to a range of innovative and significant individual interventions that would not have occurred without the oral health champions program. As with all qualitative studies, the findings cannot be generalised to all service settings for people with intellectual and developmental disability in different contexts. Finally, that champions came from different annual programs that occurred over a three-to-four-year time span, could explain some of the misunderstandings related to key messages where the passage of time might distil previous learnings.
Conclusion
In this article, the perspectives of disability support workers who participated in a novel oral health champions program were unpacked, with a focus on their influence as champions and to reflect on key successes and limitations of the program. This study has shown that disability support workers are capable of affecting change with the right type and depth of training, management and organisational support. A peer-led champions model has merit, however requires ongoing expert support to help maintain and sustain benefits over time. Although a range of positive changes to routines and individuals were reported where champions acted as agents of change, it appears that many other disability support workers remain the gatekeepers to the consistent application of best oral health practice for people with intellectual and developmental disability who rely heavily on staff care and support. This is a challenging field and area to affect positive change; this novel approach can be considered a success that resulted from great partnership working between agencies, staff in varying roles, and a commitment by champions to enhance practice and outcomes. Nevertheless key learnings for future programs are quite clear, in particular the need to acknowledge that disability support workers are not health professionals and so although they can have an impact at a localised level by making small changes, keeping key educational messages focussed and clear for them is vital to ensure that what occurs in practice is grounded in evidence.
Footnotes
Acknowledgments
The authors would like to thank gen-U, DHSV and the participants for making this small research project possible. All participant quotes and the discussion herein, do not necessarily represent the views, or values, of gen-U.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethics approval was granted from the Western Sydney University Human Research Ethics Committee in April 2020 (Approval ID: H13784).