
Abstract
The prevalence of psychiatric disorders in people with intellectual disability is statistically higher than in the general population. There is a lack of consensus on the role that epilepsy plays in psychiatric disorders in people with intellectual disability. We carried out a systematic review of articles published between 1960 and 2022, focusing on high-quality, case-control original research studies that only included adult populations. The primary outcome was the prevalence of psychiatric disorders in people with intellectual disability with and without epilepsy. Six articles were finally included. Results were varied; some reported a statistical increase, whereas others did not find any statistical difference. Due to the current controversy on the role of epilepsy in psychiatric disorders in people with intellectual disability and the small number of publications on the topic, we cannot affirm a relationship between epilepsy and psychiatric disorders in people with intellectual disability.
Introduction
Intellectual disability affects 1-2% of the general population (American Psychiatric Association, 2013). Intellectual disability starts during the early developmental period and includes intellectual and adaptive functioning limitations (World Health Organization, 2001).
Epilepsy is a chronic disease characterized by a predisposition to generate seizures unprovoked by any central nervous system direct insult and the neurobiological, cognitive, psychological, and social consequences secondary to the seizure recurrence (Fisher et al., 2005). The lifetime prevalence of epilepsy in the general population is about 7.60 per 1000 people (Fiest et al., 2017) while, in people with intellectual disability, the prevalence of epilepsy approaches 25%. Nevertheless, prevalence can be as high as 41% in those cases where the intellectual disability is severe (Robertson et al., 2015).
In the general population, the estimated prevalence of psychiatric disorders is 17% (Steel et al., 2014) whereas, in people with intellectual disability, the estimated figure is 30 to 50% (Mazza et al., 2020); the observed difference is statistically significant (Koskentausta et al., 2007). Cooper et al. (2007) studied 1023 individuals with differing degrees of intellectual disability and found a prevalence of mental disorders ranging from 15.7% to 40.0%, depending on the assessment tools, classification system, and the inclusion or otherwise of behavioral problems such as psychiatric disorders.
Recent evidence (Lu et al., 2021), (Gurgu et al., 2021) showed a higher prevalence of anxiety (25.6%) and mood disorders (35.0%) among patients with epilepsy compared to those in the general population (6–8%) (Alonso et al., 2004); (4.2-7%) (Steel et al., 2014). Moreover, the association between autism spectrum disorders (ASD) and epilepsy is especially strong (Lukmanji et al., 2019).
Two systematic reviews discussed the possible role that epilepsy plays in increasing the risk of mental disorders among people with intellectual disability. While Van Ool et al. (2016) concluded that epilepsy is not a clear determinant of neuropsychiatric comorbidity amongst patients with intellectual disability; Akrout Brizard et al. (2021) noted an increase in psychotic disorders, depressive disorders and anxiety disorders in the non-epilepsy control group compared with the epilepsy group.
Considering the lack of consensus on the topic and its great relevance, we decided to carry out a systematic review of high-quality case-control original research studies that exclusively examined the adult population.
Methodology
We based the protocol and search strategy on the International Prospective Register of Systematic Reviews (PROSPERO) guidelines. We registered the study with PROSPERO, under registration number CRD42020154120 and used the following electronic databases: PubMed, PsycINFO, and Web of Science. The electronic search focused on articles published in English, Spanish and German between 1 January 1960 and 07 April 2022. We only included quantitative studies.
Search terms
We conducted the search using three main concepts: Epilepsy, Mental Disorders, and Intellectual Disabilities. The date of the search was 07.04.2022. Search strategies are detailed in Supplementary files.
Inclusion and exclusion criteria
The review inclusion criteria were (a) epilepsy and intellectual disability in the case group compared with intellectual disability without epilepsy in the control group and (b) adult participants.
All participants were adults with intellectual disability (regardless of severity) and at least one psychiatric comorbidity.
We excluded non-human studies, studies involving children and people without intellectual disabilities. We did not set a minimum sample size as an exclusion criteria.
Outcome
The main outcome was prevalence of psychiatric disorders in people with intellectual disability with and without epilepsy. The secondary outcome was the prevalence of different types of psychiatric disorders between groups.
Study types
We included those studies that compared the frequency of psychiatric disorders in adults with intellectual disability and epilepsy with adults with intellectual disability but without epilepsy.
We only accepted those studies with either a matched or non-matched intellectual disability control group. We considered both randomized and non-randomized research studies as valid.
The study did not require ethical approval since we did not collect individual patient-related data for the analysis.
Selection process
Rayyan software was used to generate a database after completing the search using the previously mentioned criteria and to identify and remove duplicates.
C. Peña-Salazar and M. Alfonso-Ramos independently screened the remaining abstracts using pre-piloted eligibility criteria; C. Peña-Salazar and M. Alfonso-Ramos were blind to each other’s scores. They also identified and discussed the differences until consensus was reached. Subsequently, we gathered the full text of the studies that met inclusion criteria and those marked as uncertain. C. Peña-Salazar and M. Alfonso-Ramos reviewed and assessed the texts with the same criteria used for screening abstracts (the flow diagram (Figure 1)) explains the selection process. A third review author (SD) was not necessary for arbitration. Flowchart of study selection process.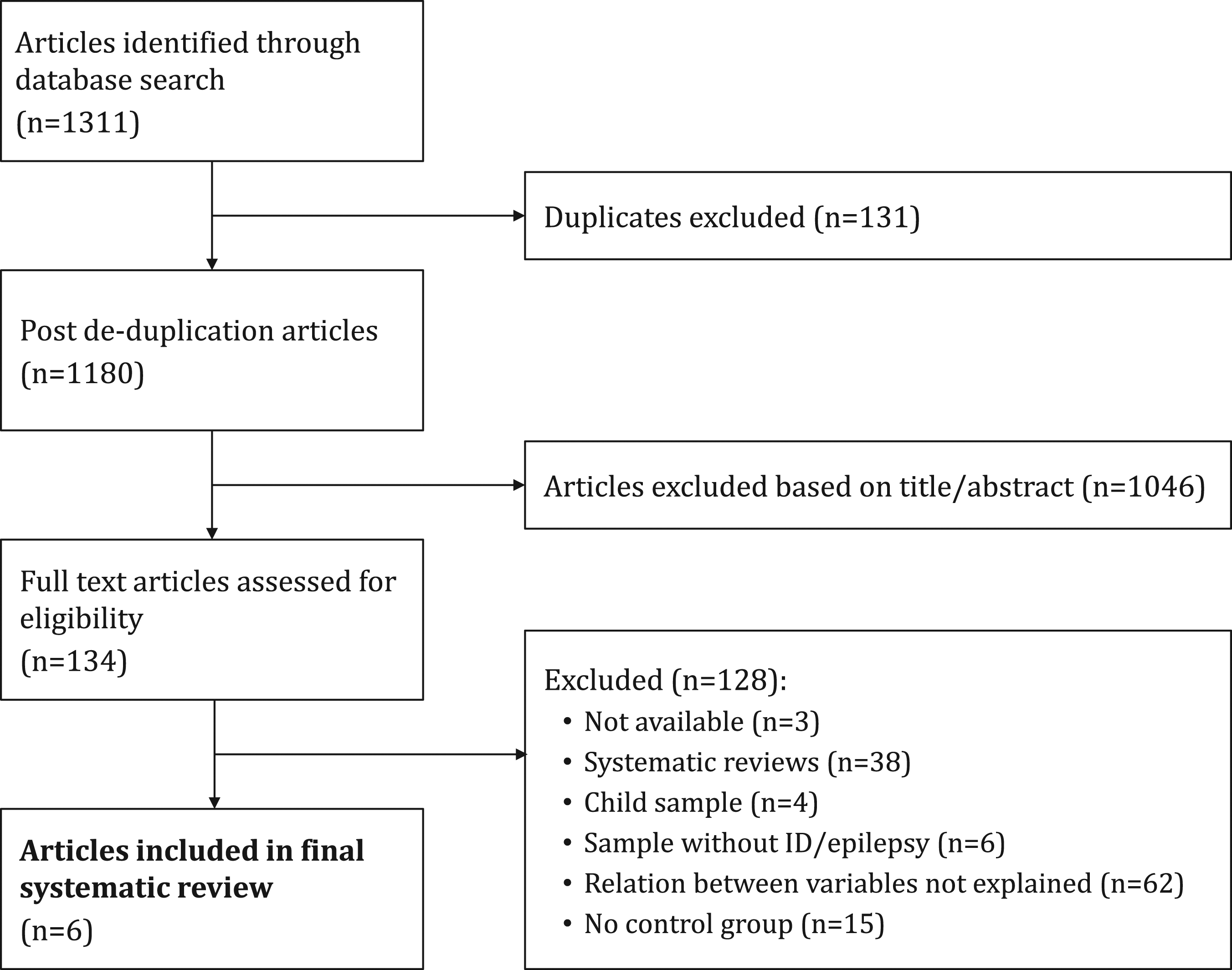
We assessed the remaining articles using the “Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE) to improve the quality of reporting in observational studies. STROBE guidelines consist of a checklist of 22 items related to the title, abstract, introduction, methods, results, and discussion sections of articles. Eighteen items are common to cohort studies, case–control studies, and cross-sectional studies, and the remaining four are specific to the three study designs. STROBE guides authors on improving the reporting of observational studies and facilitates critical appraisal and interpretation by reviewers, journal editors, and readers. We also extracted additional data: country, study setting, intervention or population group, control group, mental disorder approach (how was it considered), measure outcomes, study design, aim, results, and potential risk of bias.
Results
Search findings
The initial selection included one thousand three hundred eleven articles, from which we excluded one hundred thirty one duplicated papers. We then excluded one thousand forty six titles and abstracts based on eligibility criteria. After screening the remaining one hundred thirty four articles, we excluded those that did not report the association between the variables of interest, systematic reviews, and those that lacked control groups. Finally, we used the six remaining articles for the systematic review (see Figure 1).
Included studies
We included six papers in our systematic review. All were studies in solely adult populations and included a control group to compare the overall rate of psychiatric disorders (two of which were matched by gender and intellectual disability level). In two studies (Deb, 1997) and (Matthews, 2008)), the number of participants remained the same in both the epilepsy and control groups; in the remaining studies (Arshad et al., 2011), Turky et al. (2011), Smith & Matson (2010) and Fitzgerald et al. (2011)), the study and control groups were not fully matched.
Data from studies that compared information on the overall rate of psychiatric disorders in adults with intellectual disability and epilepsy, and adults.
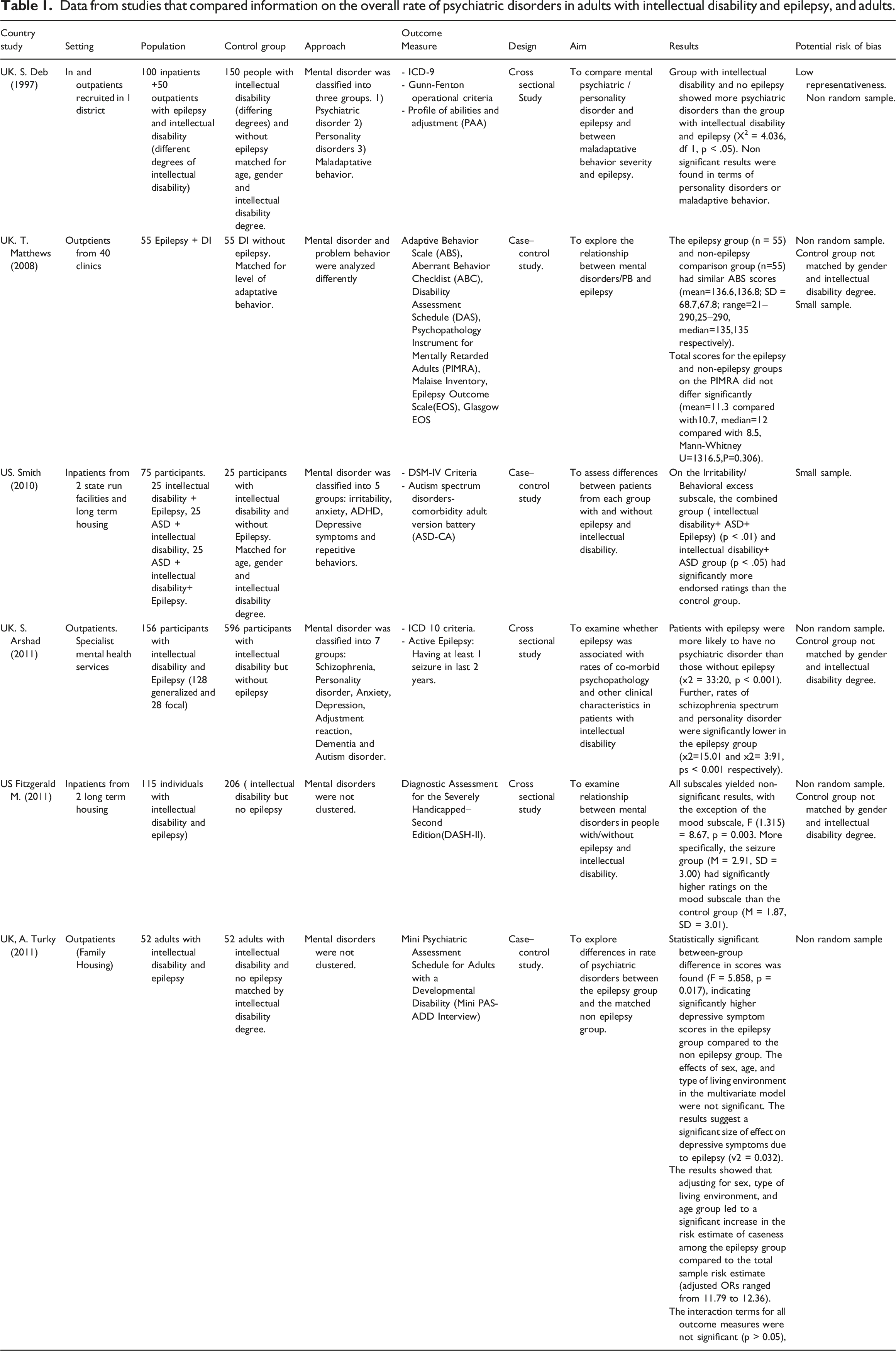
Four of the included studies (Deb (1997), Matthews (2008), Arshad et al. (2011) and Turky et al. (2011)) originated in the UK, and two (Smith & Matson (2010) and Fitzgerald et al. (2011)) came from the US. The studies present a data sample of one thousand six hundred eighty seven adults with intellectual disability, five hundred seventy eight with epilepsy and one thousand one hundred nine without epilepsy.
Study characteristics
Diagnosis
For the diagnosis of intellectual disability, one of the studies used ICD-9 criteria (Deb, 1997), one ICD-10 (Arshad et al., 2011), a third used DSM IV (Smith & Matson (2010), and the three remaining studies collected the intellectual disability information from medical records (Matthews (2008), Turky et al. (2011), Fitzgerald et al. (2011). Epilepsy diagnosis criteria varied among the different studies. One study used Gunn-Fenton operational criteria (Deb, 1997), another used the Epilepsy Outcome Scale (EOS) (Matthews (2008), and the four remaining studies collected this information from medical records (Smith & Matson (2010), Turky et al. (2011), Fitzgerald et al. (2011), (Arshad et al., 2011).
For the diagnosis of psychiatric disorders, one original study used ICD-9 criteria (Deb, 1997), another ICD-10 (Arshad et al., 2011), and a third used DSM-IV criteria (Smith & Matson (2010); the remaining three studies used specialized instruments for intellectual disability (PIMRA (Matthews (2008), DASH-II Fitzgerald et al. (2011), Mini PAS-ADD Interview Turky et al. (2011)). One of the studies used the autism spectrum disorders-comorbidity adult version battery (ASD-CA) (Smith and Matson (2010)) as a complementary tool for a psychiatric diagnosis of autism.
Outcomes
We identified six controlled studies which compared the rate of psychiatric disorders between epileptic and non-epileptic adults with intellectual disability. Deb (1997) and Matthews (2008) did not find any statistical difference between groups while Arshad et al. (2011) reported that patients with epilepsy were more likely to have no psychiatric disorder than those without epilepsy. On the other hand, Fitzgerald et al. (2011) and Turky et al. (2011) found statistically higher depressive symptomatic scores in the epilepsy and intellectual disability group. Smith & Matson (2010) found a statistical increment in the frequency of irritability among patients with epilepsy, intellectual disability, and ASD. The results are detailed in Table 1.
Discussion
This systematic review aimed to explore the association between epilepsy and psychiatric disorders in adults with intellectual disability. From an initial total of one thousand three hundred eleven records, we included six studies with high quality or an acceptable risk-of-bias evaluation, consisting of one thousand six hundred eighty seven adults.
Two previously published systematic reviews focused on this topic although one, Van Ool et al. (2016), collected studies that mixed children and adults and included behavioral problems such as neuropsychiatric disorders while, in the other (Akrout Brizard et al., 2021), the authors focused their review on adults with intellectual disability but also included cross-sectional studies without control groups. We specifically focused on original research studies looking at the difference between adults with intellectual disability and epilepsy and adults with intellectual disability and no epilepsy.
Our results are somewhat controversial. On the one hand, Fitzgerald et al. (2011) and Turky et al. (2011) found significantly more symptoms in the depressive symptomatology scores of the intellectual disability + epilepsy group. Aligned with these results, Gurgu et al. (2021) and Lu et al. (2021), in two recent independent systematic reviews, reported a higher prevalence of psychiatric disorders in patients with epilepsy compared to the general population. This relationship proved to be more intense in cases of generalized and temporal lobe epilepsy (Gurgu et al., 2021).
On the other hand, Deb (1997) and Matthews (2008) did not find a statistical difference in the frequency of presentation of psychiatric disorders among adults with intellectual disability with and without epilepsy, and Arshad et al. (2011) described a statistically significant reduction of psychiatric disorders in the epileptic group.
A possible explanation for the varied results observed in our review could be related to the heterogeneity in genetic syndromes in the sample, the differing brain damage sites, most of which are of uncertain etiology (Chiurazzi & Pirozzi, 2016); (Mehregan et al., 2016). It is important to highlight the inclusion of individuals with intellectual disability and ASD, since adults with ASD and intellectual disability tend to present a closer relationship with epilepsy (Amiet et al., 2008), (Jokiranta et al., 2014) and a higher prevalence of psychiatric comorbidity (McCarthy et al., 2010), (Bakken et al., 2010).
Similarly, Smith & Matson (2010) found more irritability among patients with intellectual disability, ASD and epilepsy versus those with intellectual disability and ASD without epilepsy, although they did not find a higher prevalence of psychiatric disorders. Considering that depression is the most frequent psychiatric diagnosis among people with intellectual disability and ASD (McCarthy et al., 2010), irritability could be considered a depressive symptom in this subset of patients (Eaton et al., 2021), (Davis et al., 1997).
Due to the lack of publications on this topic and the current controversy, we cannot assert that a clear relationship exists between epilepsy and psychiatric disorders in people with intellectual disability. Several confounding factors, such as 1) psychotropic medications, which can trigger psychiatric disorders (Piedad et al., 2012); 2) antiepileptic medications, which can lead to psychiatric disorder stabilizations (Piedad et al., 2012); 3) antipsychotic medications, which can produce epileptic seizures (Hedges et al., 2003); 4) change in the prevalence of epilepsy or psychiatric disorders due the inclusion of ASD patients in the population sample (Strasser et al., 2018), (Loussouarn et al., 2019); and 5) great heterogeneity in the population sample of intellectual disability studies (Anazi et al., 2017), which produces essential differences in the prevalence of psychiatric and neurological disorders, may alter the results of any systematic review on this subject with the currently available data.
It is also essential to consider that patients with frequent seizures may present, via forced normalization, an improvement in some psychotic symptoms (Kawakami & Itoh, 2017), (Krishnamoorthy et al., 2002) since this could decrease the prevalence of psychotic symptomatology. Moreover, the use of antiepileptic combinations in drug-resistant epilepsy, which is very frequent in people with intellectual disability (D’Alessandro et al., 2017), could induce a therapeutic effect by reducing affective or anxiety symptoms, thus creating a false figure on the pervasiveness of psychiatric disorders (Piedad et al., 2012).
It is thus fundamental to carry out studies with separate population samples, including epilepsy + ASD as an independent variable from epilepsy + intellectual disability, to achieve more precise results in the relationship between psychiatric disorders, ASD, and epilepsy. Considering the prevalence of psychiatric disorders and epilepsy by differing degrees of intellectual disability, we also see great relevance in studying epilepsy and psychiatric disorders matched by degree of intellectual disability to homogenize the population sample properly.
Limitations
There are several limitations to our study. Grey literature and abstracts were excluded, as they would not fit our eligibility criteria and risk of bias assessment. It is not easy to pool data for a systematic review from such heterogeneous studies.
The available literature on the subject is minimal in scope and the total number of patients is comparatively small, which limits data validity and representativeness. Three articles were not available and did not include author correspondence addresses to establish contact. However, these articles were old (from the 1960s), and we do not think they could affect the final results.
The samples in the selected original research studies included in our review are highly heterogeneous and this generates selection bias which, in turn, complicates data analysis. The research studies do not differentiate between intellectual disability levels, so they include, without differentiated analysis, patients with ASD, which evidence shows have higher rates of epilepsy and specific psychopathologic comorbidities. The absence of an appropriately matched control group in most studies included causes a high degree of bias.
Future research should focus on using solid methodology with appropriately matched control groups and standardized instruments to establish definitive conclusions on the relationship between psychiatric disorders and epilepsy in adults with intellectual disabilities.
Conclusions
The results of this systematic review were limited but varied; whereas some studies found an increased risk of psychopathology among patients with intellectual disability and epilepsy, others did not, and one original research study even found an inverse association. The main methodology used in the studies had significant flaws, specifically by not properly selecting homogeneous populations, mixing patients with markedly differing degrees of intellectual disability and not taking into account the specificities of Autistic Spectrum Disorder which may act as an important confounding factor. Consequently, in our opinion, it is not currently possible to establish a clear relationship between epilepsy, intellectual disability and mental disorders.
Footnotes
Acknowledgements
We would like to thank Stephen Kelly for his contribution to English language editing. We thank the CIBERESP (Centro de Investigación Biomedica en Red de Epidemiología y Salud Pública, CB16/02/00322) and the Research Network on Preventive Activities and Health Promotion (redIAPP) [RD16/0007/0012] for their support in the development of this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.