
Abstract
People with intellectual disabilities, especially those who require care, are among the most affected by severe forms of COVID-19 and COVID-19- related deaths. In this study we investigated how care needs and other vulnerabilities influence the possibility COVID-19 infection among people with intellectual disabilities in Brazil.
Introduction
People with disabilities are among the most stigmatized, poorest, and least educated citizens in the world (Groce et al., 2011; WHO, 2011; United Nations, 2018). Lack of information is one of the bottlenecks that challenges health services management and the provision of quality care to for this population group (Groce et al., 2011; WHO, 2011; United Nations, 2018). The situation became even more complex during the COVID-19 pandemic for those who require caregivers and routine specialized health services due to their sudden need for social distancing (WHO, 2011).
People with disabilities were the human group most affected by the pandemic (United Nations, 2006). There are approximately 1 billion disabled people in the world. Of these, 80% live in developing countries and only 28% have access to disability benefits, while in poor countries only 1% have access (Groce et al., 2011). Twenty-four percent of Brazilian citizens state they have some type of disability. Of these, most are women or Black and mixed-race. Brazilians with disabilities have less opportunities to access the labor market and are less educated, which has negative implications for their financial independence. (IBGE, 2010).
According to the United Nations (2018), people with disabilities experience heightened vulnerability during humanitarian emergencies, extreme climate events, and natural disasters (United Nations, 2018). This is primarily due to the fact that they are often not identified because countries do not register them and lack qualified information. Additionally, they are poorly monitored by health and assistance services during these critical times (United Nations, 2018). Williamson et al. (2021) corroborates this information by demonstrating how the issue of disabilities has often been ignored and/or garnered little debate in the history of pandemics, thus increasing their vulnerability (Williamson et al., 2021).
Since 2009, Brazil has been a signatory of the Convention on the Rights of Persons with Disabilities (CRPD) of the United Nations (United Nations, 2006). Article 11 of the Convention states that member countries must ensure the protection of people with disabilities in situations of risk. The Brazilian Law of Inclusion (Lei Brasileira de Inclusão – LBI) regulates and provides priority actions for this population in the country (Brasil, 2015). It recognizes the vulnerability of disabled people and the need to adopt specific measures to promote health, prevent disease, and care.
Although represented in its Census, Brazil’s official data lacks information regarding people with disabilities, which is reflected in the pandemic database. The federal information systems for registering suspected cases of diseases caused by the coronavirus (e-SUS Epidemiological Surveillance) and confirmed cases of hospitalized severe acute respiratory syndrome (Influenza Epidemiological Surveillance Information System) do not contain fields for registering patient disability information. Thus, it is impossible to use government data to track how epidemics and diseases affect the health of disabled people. This lack of data causes systematic invisibility and thwarts the production of statistical information for this group in terms of health diagnoses and services, duration of hospitalization, needs for ICU beds, mortality rates, etc., which makes them invisible to health authorities and health service planning (Block et al., 2021; Pereira et al., 2021).
The complex lives of people with disabilities have been addressed by several authors who have demonstrated how an inaccessible society produces exclusions and directly affects the health of this population (Pineda and Corburn, 2020). The pandemic aggravated pre-existing barriers formed by environments, attitudes, communication, and others faced by people with disabilities and amplified their already proven vulnerabilities (Block et al., 2021; Jesus et al., 2020; Armitage and Nellums, 2020).
Vulnerability, disability and care
Vulnerability is a concept that has multiple interpretations. According to Parley (2010), vulnerability is the inability to safeguard one’s own well-being, property, rights, or other interests, and configures subjects that are more exposed to potential risks of physical and mental harm (Parley, 2010). Thus, they might require care services from others, whether family or community members, or those offered by the state according to the rights established for their protection (Parley, 2010).
Vulnerability can also be seen as a human condition. Human beings have bodily and material needs; are exposed to physical illnesses, injuries, disabilities, and death; and depend on the care of others at different stages of their lives. As social and affective beings, humans are emotionally and psychologically vulnerable to others in countless ways: loss and suffering; negligence, abuse, and lack of care; rejection, ostracism, and humiliation. As sociopolitical beings, they are vulnerable to exploitation, manipulation, oppression, political violence, and abuse of rights. Humans are vulnerable to natural violence and environmental impacts. In these and other ways, vulnerability is frequently connected to other concepts such as: damages, needs, dependence, care, and exploitation (Mackenzie et al., 2013).
Although vulnerability can be understood as a human condition that affects everyone at some point in different ways, vulnerabilities and disadvantages are often synergistic and mutually reinforcing to greater or lesser degrees depending on the audience, social group, political responses, or the lack thereof. In other words, it is important to observe vulnerability from the perspective of specific contexts and groups, like during the pandemic (Jesus et al., 2020).
Other authors have described vulnerability from an economic point of view, experienced by some social groups as the result of globalization, the ideology and influence of neoliberalism, and the effects of the worldwide financial crisis (Mackenzie et al., 2013).
The World Health Organization (WHO) has stated that people with disabilities are more vulnerable in situations of conflict or disaster. In the case of COVID-19, this was especially true considering that the responsibility to “keep oneself safe” was placed on individuals worldwide from the onset of the pandemic. Thus, when state responsibilities were transferred to individuals, disabled and “vulnerable” people were put at a disadvantage (Block et al., 2021). Block et al. (2021) described Hurricane Sandy, which affected New York in 2012, as an important example for reflecting on the vulnerability of people with disabilities (Block et al., 2021). According to the author, the responsibility of providing disability care in cases of emergencies and extreme events is left to family members and society, without professional support, even when their lives depended on mechanical breathing equipment that cannot be interrupted and that requires constant third-party care or technology (Block et al., 2021).
The need for care is a vulnerability factor for people with disabilities. A significant amount of people with disabilities require the care of others at different times in their lives, or to conduct daily tasks. This care is mostly provided by mothers or other women in the family, although it is not always enough for maintaining quality of life (Sharma et al., 2016; Mathias et al., 2018). In Brazil, the lack of policies for care executed by the state further reinforces the vulnerability of dependent people, in that the duty and responsibility of care is delegated exclusively to their family members.
Care is unquestionably an important part of the disability debate. Authors like Kittay (2019) have shown the need to question the socially accepted standards of dependence and to recognize that care is part of the human condition. For this reason, she proposes a discussion about the ethics of care (Kittay, 2019). In this sense, it is important to emphasize that the need for care and, in some cases, the absence of care can be a vulnerability factor for people with disabilities.
The experience with the HIV/Aids pandemic is also relevant to understanding how subjects in situations of vulnerability are more susceptible to infections, illnesses, or death, as well as to experiencing situations of negligence, abandonment, or discrimination. Additionally, it demonstrates a profound and important connection between reflections on vulnerability and human rights. Authors like Mann and Tarantola (1996) and Mann (2016) systematize the idea of vulnerability into three interdependent spheres: individual, which corresponds to the level of information people have for thinking and acting in daily life; social, which refers to socio-culturally produced elements that help make decisions or seek state actions; and programmatic, which is located at the state level, or the decisions/actions undertaken or not in response to a specific problem (Mann and Tarantola, 1996; Mann, 2016).
In March 2020, The Lancet published an article stating that people with disabilities are more susceptible to illnesses caused by the coronavirus and that the COVID-19 pandemic disproportionately affects these individuals and places them at risk of increased morbidity and mortality (Armitage and Nellums, 2020). This was corroborated by the UN, which indicated the urgent need to improve health care services for this group during the pandemic as part of a global commitment to people with physical, mental, intellectual, or sensorial disabilities (WHO, 2011). It is understood that this group has greater needs for health care services yet faces more difficulties to access it. In addition to worse outcomes, they also suffer under discriminatory and stigmatizing laws (Armitage and Nellums 2020).
Hence, different perspectives establish different markers that make this population with disabilities vulnerable. This group also requires care, whether privately from family members and friends, or publicly for assisted services and support (Block et al., 2021). During the pandemic, the way in which the authorities have considered the vulnerabilities and care needs of people with disabilities is possibly related to the outcomes of illness, infection, transmission of the coronavirus, as well as access to health services during the pandemic. This is in addition to interacting with notions of independence and autonomy related to their social isolation (Almeida and Fontes-Dutra, 2021; Turk and McDermott, 2020).
People with disabilities and the COVID-19 pandemic
Studies produced during the pandemic in Brazil and in different countries of the world have proven that people with disabilities, especially those with intellectual or mental disabilities, are more vulnerable to coronavirus infection, severe forms SARS-COVID-19, and death. They are also more vulnerable in terms of the effects on their mental health, accessing health services, and the evolution of comorbidities (Lunsky et al., 2019; Almeida and Fontes-Dutra, 2021; Turk and McDermott, 2020). Having some kind of disability can already be understood as being at risk for the most serious forms of COVID-19, either because of comorbidities or the particularities of daily routines, like needing a caregiver (Reichenberger et al., 2020).
There is a body of evidence that shows that adults with intellectual disabilities are 5 times more likely to be infected and hospitalized with COVID-19 and 8 times more likely to die (Williamson et al., 2021). Intellectual disability was the strongest independent risk factor for positive diagnosis and the second strongest independent risk factor for mortality from coronavirus infection, followed only by age factor (Gleason et al., 2021) People with Down Syndrome and developmental disabilities are also at higher risk to virus infections compared to the general population (Landes et al., 2021a; Landes et al., 2021b).
In Brazil, studies have also demonstrated that people with disabilities infected by COVID-19have higher fatality rates than groups without disabilities (Melo et al., 2020). Greater numbers of cases were found among Brazilian children and youth with physical, sensorial, intellectual, or mental disabilities. The proportion of disabled children that died is more than double compared to non-disabled children in cases of COVID-19and triple in cases of SARS (Severe Acute Respiratory Syndrome) (Almeida and Fontes-Dutra, 2021).
These results reinforce arguments about people with disabilities suffering more negative effects from the pandemic than the rest of the population. They confirm the need for specific health and social protection actions due to their high level of social vulnerability and their multiple chronic conditions (Turk and McDermott, 2020).
In this context, this study sets out to describe vulnerability from the perspective of needing the care of others, and to relate vulnerability to outcomes like COVID-19 infection and seeking access to health services during the pandemic period in Brazil.
Methods
This is a descriptive quantitative study. Primary data was collected from a convenience sample using an online questionnaire containing 79 questions related to the profiles of people with disabilities, COVID-19 infection, required and accessed services during the pandemic, and related challenges. Once ethically approved, the questionnaire was applied online between July 2020 and July 2021. It was distributed to disability associations, rights councils, and disability services who were asked to get the forms to their associates/users that filled them out with or without help.
The resulting database contained 14,113 entries. The data was treated for inconsistencies, accidental inclusions, and duplications, resulting in 764 discarded entries. In cases of homonyms, the data was validated using variables such as mother’s name, state and municipality of residence, and telephone number. Once inconsistent data was discarded, the sample had 13,349 respondents.
In this study, only people who stated they had intellectual disabilities were considered, which totaled 4,553 entries. However, for the purposes of this analysis, only data from individuals over the age of 16 (age of majority in Brazil) was used which totaled 2,800 participants, as seen in Figure 1. Data treatment and sample definition.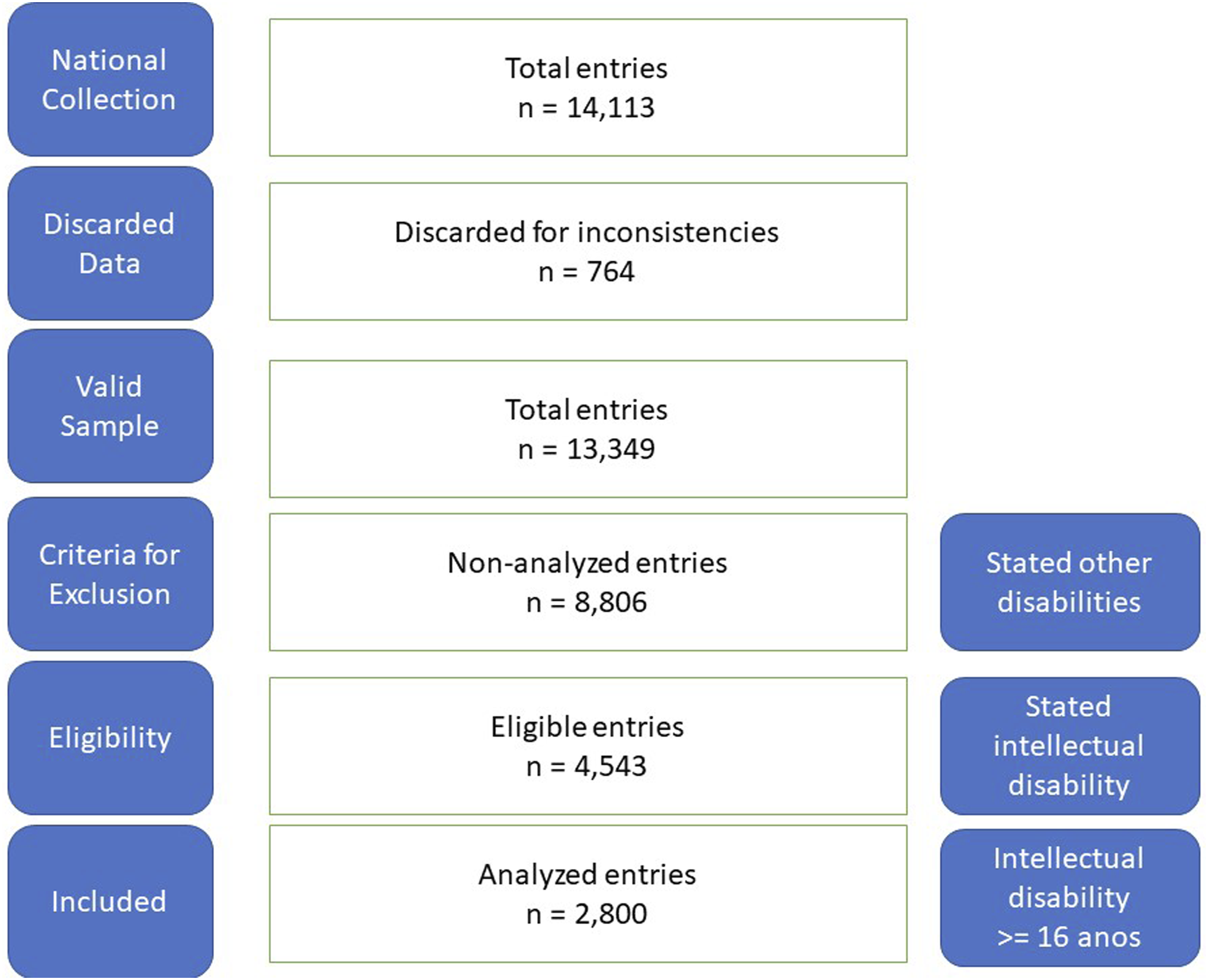
To recruit and engage people with disabilities and their families to respond to the questionnaire, we partnered with representative associations and service providers for people with disabilities. The survey was sent by instant messaging apps and email.
The participation of people with disabilities in answering the questionnaires varied according to mobilization power of the state and municipal councils and the representing associations or groups. The highest participation was from groups and associations of people with intellectual disabilities or their parents.
To build data on vulnerability for this analysis, we use the variable Need for Help from Others in Daily Routines. Thus, the frequency of the answers: never, not often, often, and always related to their required care from others is associated to other variables regarding the testing positive for COVID-19and seeking out health services.
The data was analyzed using Excel software, which was also used to prepare and format the tables. With Excel, we removed duplicate and incomplete data so that each participant was counted only once.
The numbers are a way to reflect on the reality of a population group that is still often invisible, whether in official systems or in public actions to contain and/or mitigate the consequences of the virus. The data is presented in tables with absolute and relative frequencies of the variables selected for this study that can support future analyses of vulnerability and care.
Results
Sample Profile.
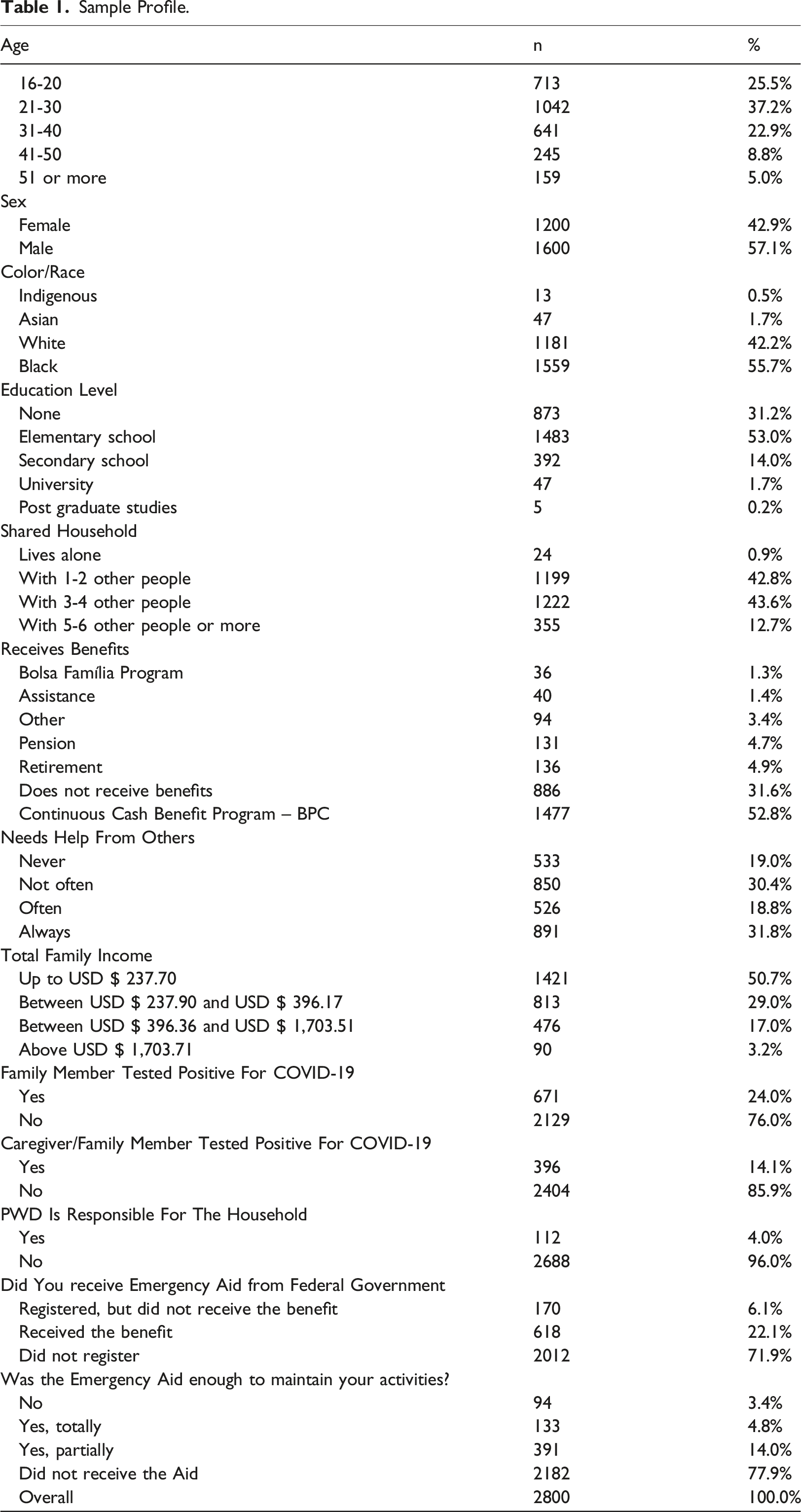
The Continuous Cash Benefit program, known in Brazil by its acronym “BPC,” is provided for in the Organic Law of Social Assistance (Lei Orgânica da Assistência Social - LOAS) and ensures a monthly minimum wage for low-income elderly and people with disabilities. Brazil’s Transparency Portal (Brazil's official website) informs that in 2019 the BPC had more than 4.7 million elderly and disabled beneficiaries (Brasil, 2019).
In terms of housing, 71% share their homes with between 2 and 4 other people. Only 4% of people with disabilities are responsible for their own household. The need for assistance in daily activities is seen in 81% of the sample. Those who always need assistance correspond to 30%. Seven percent of the respondents had a confirmed COVID-19diagnosis, 24% had family members diagnosed with the disease and, 14% had caregivers diagnosed. Of those who received Emergency Aid, 78% stated it was not enough to support their activities.
Emergency Aid was a temporary income transfer program that Brazil established to help workers in economically vulnerable situations because of the pandemic. The amount varied between R$ 300,00 and R$ 600,00 (US$ 58.00 and US$ 117.00) per month. In the US, this type of aid during the same period varied between US$ 1,200.00 and US$ 2,000.00 which according to current exchange rates would be approximately R$ 6.100,00 and R$10.250,00. The program was later replaced by Auxílio Brasil (Brazil Assistance) and underwent a series of changes related to the criteria of its target audience, which are established by law (Brasil, 2021)
It is important to note that the criteria established by the federal government for granting emergency assistance contained restrictions for people who already received BPC benefits or were already retired, which prevented most of the investigated sample from having access to this assistance. 1. Vulnerability and testing positive for COVID-19
The sample indicated that among those who most needed the help of others for daily routines (including personal care, feeding and hygiene) were also who most tested positive for COVID-19 (Table 2). 2. Vulnerability and seeking health services Vulnerability and COVID-19 Did The Person With Disability Test Positive for COVID-19?
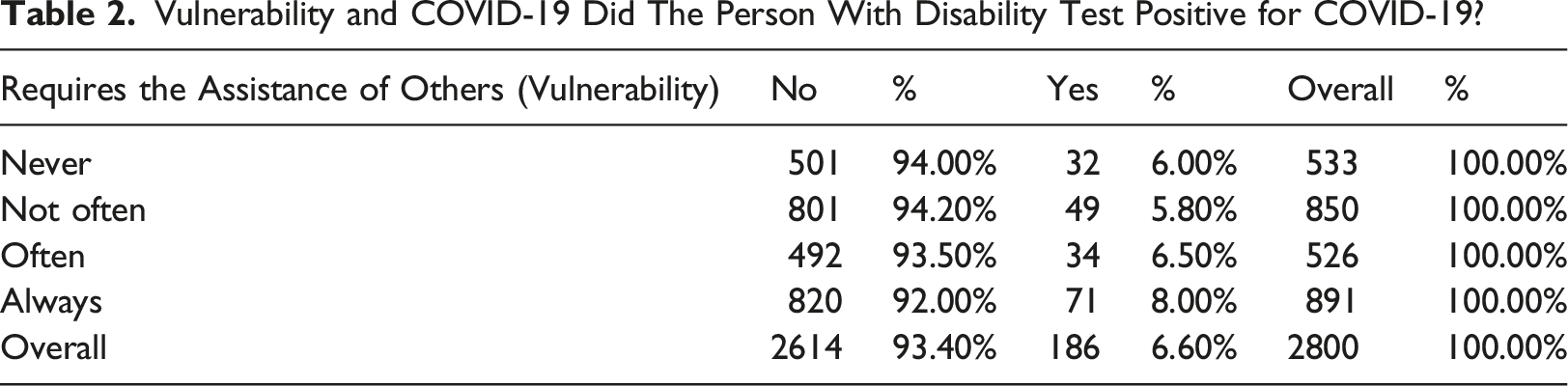
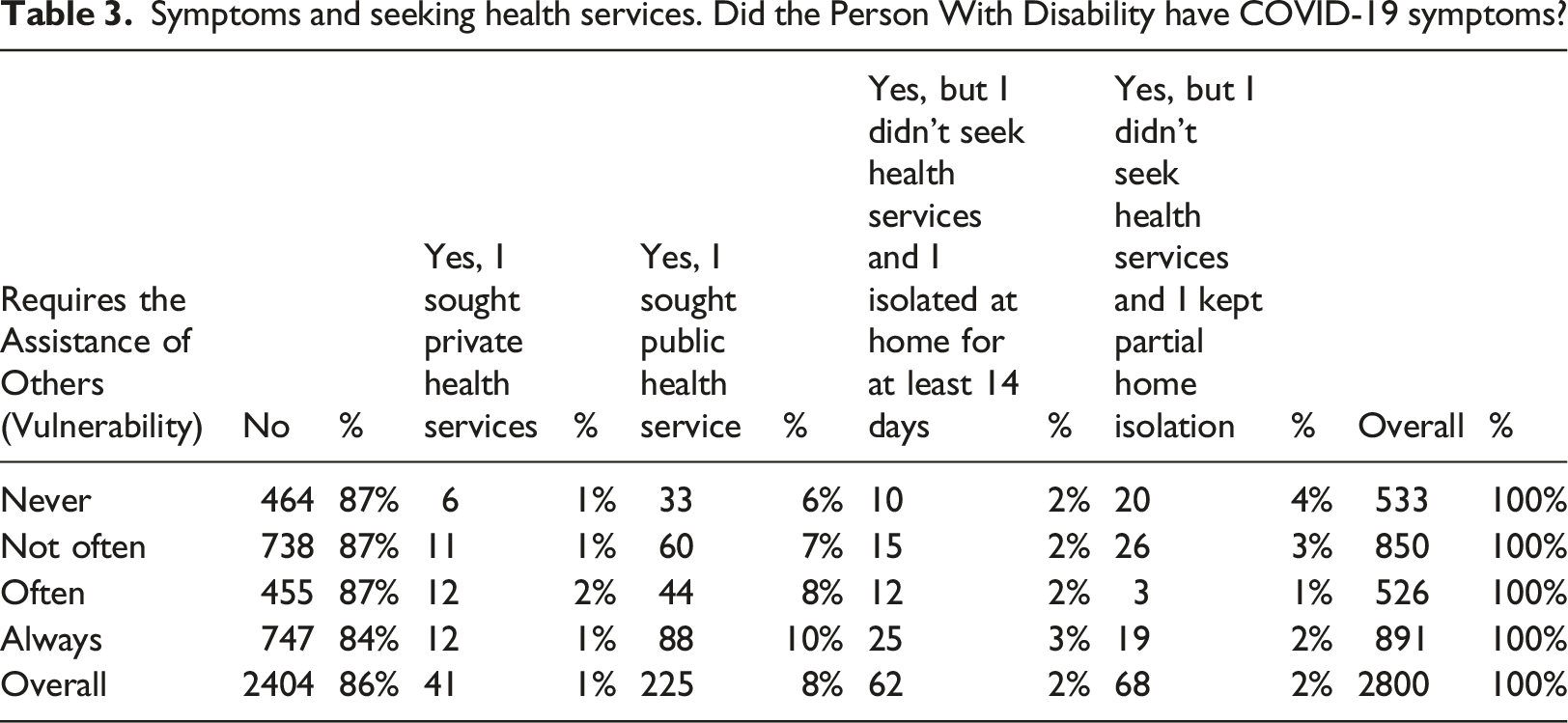
Table 3 shows that among those who were symptomatic, the ones who needed help from others (always or often) sought out health services the most, with public services being the predominant choice in all groups. It also shows that those who never need help from others were proportionally those who least sought out health services and who did not stay in isolation for 14 days. 3. Vulnerability and exposure to risk Symptoms and seeking health services. Did the Person With Disability have COVID-19 symptoms?
Exposure to COVID-19. Did a Family Member test positive for coronavirus?
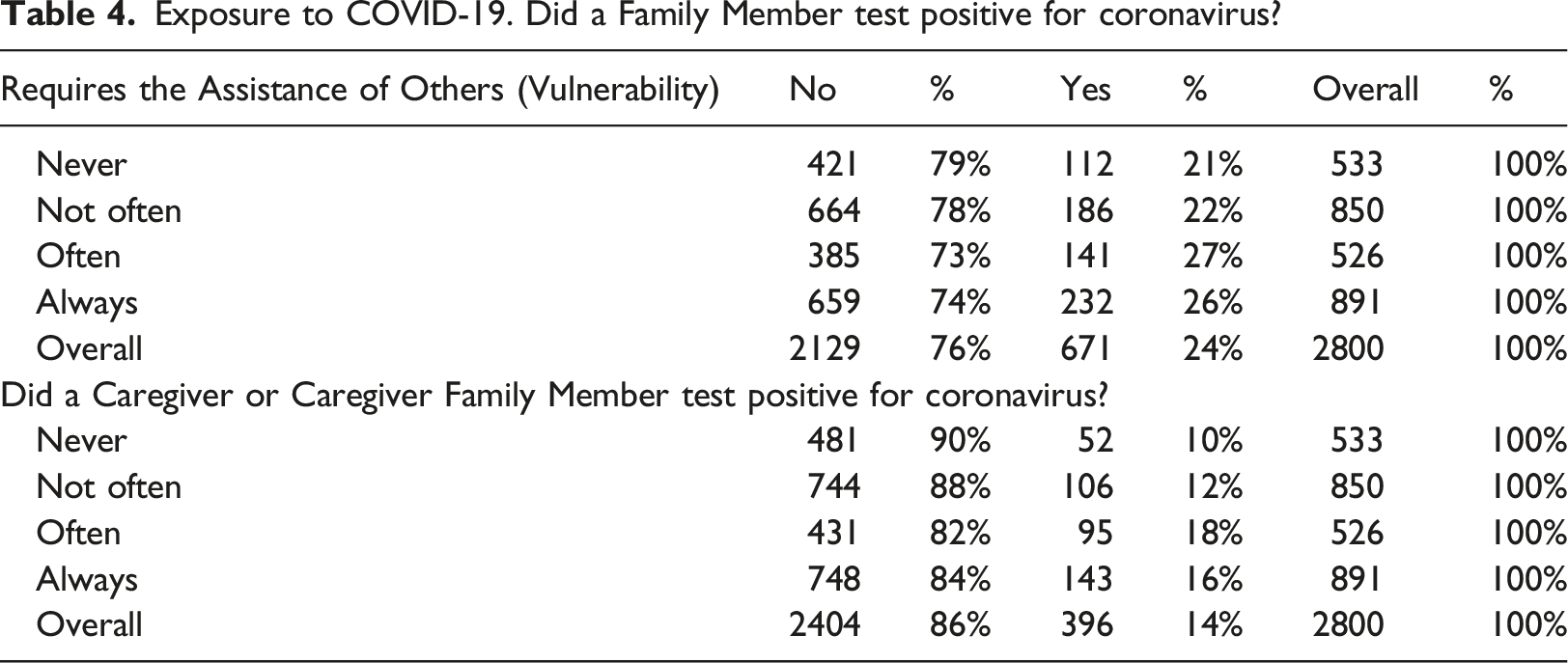
When observing the infection frequency among caregivers and family members, it can be noted that those who most need care have the highest rates of infection, reaching almost two times more for those who need care often in comparison with those who never need daily help. 4. A positive COVID-19 diagnosis for people with disabilities and their family members and caregivers
Cross-infections between People with Disabilities and Family Members/Caregivers. Did the Caregiver and/or Caregiver Family Member test positive for coronavirus?
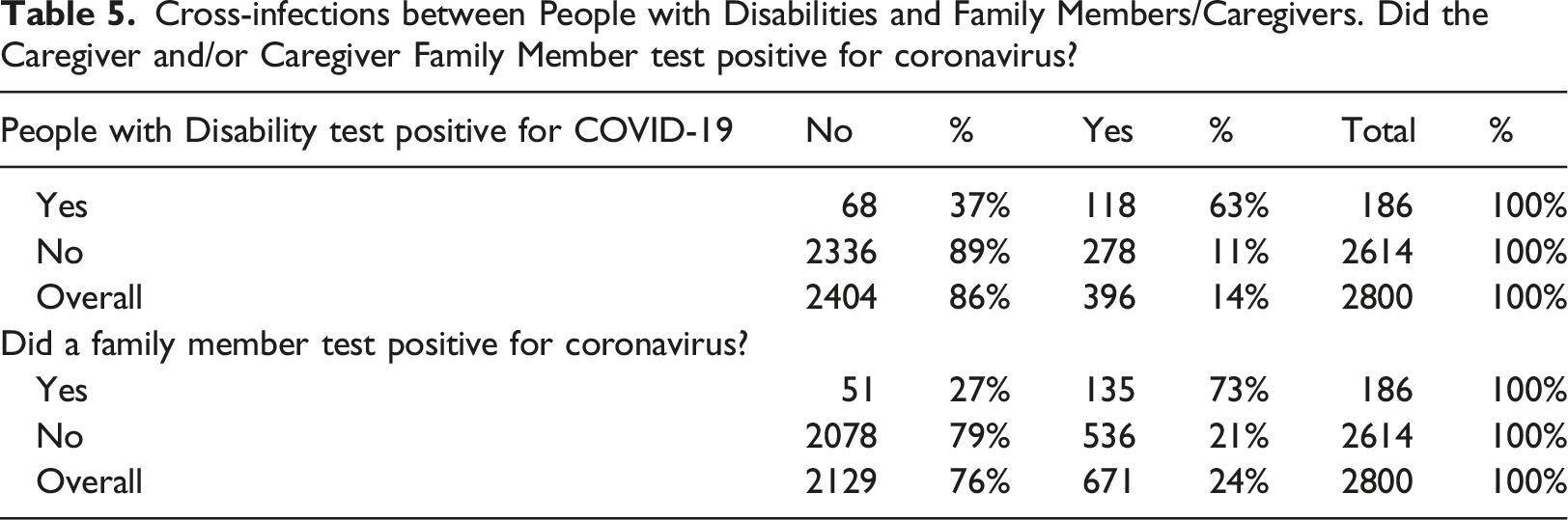
Table 5 shows that people with disabilities who contracted the disease had a frequency of being infected by family members that was approximately 6 times higher than those who did not contract COVID-19. Among caregivers, infection frequency was over 3 times more compared to those who did not have the disease.
Discussion
The socio-spatial dynamics of the COVID-19pandemic in Brazil have shown that vulnerability is a discriminating factor in how different groups responded to this health situation. In fact, the exposed by everyday routines are what determined the level of infection vulnerabilities and impact (Armitage and Nellums, 2020).
The measures taken by different countries to cope with the pandemic produced an individualization of the responsibility to “keep oneself safe.” This was detrimental to people with disabilities, especially those who require the care of others. From the beginning of the pandemic, various documents produced by national and global organizations that represent people with disabilities, human rights, and health, including the United Nations, the World Health Organization, the Economic Commission for Latin America and the Caribbean, have considered people with disabilities as vulnerable. Nevertheless, this does not seem to have been translated into effective state actions (Sakellariou et al., 2020).
The scientific community and health authorities around the world have also affirmed these vulnerabilities and have exposed the need for an inclusive response, thus placing the responsibility of protecting people with disabilities on states. And yet, what has been seen on a large-scale is the transposition of state responsibilities to individuals. For people with disabilities, this has reinforced their historic invisibility and increased their vulnerabilities, which are not exclusively individual characteristics but are primarily structural and multifactorial in nature (Block et al., 2021; Block, 2019).
Although there have been some positive measures, the needs of people with disabilities were not considered. Several countries published recommendations for disability-inclusive responses to COVID-19without ensuring their practice. Countries mainly took measures to provide access to financial support, while at the same time implementing policies that caused a negative impact on people with disabilities, like interrupting specialized rehabilitation services. The populations most exposed to the impacts of the pandemic, including people with disabilities living in institutional care, for example, were only protected by recommendations, not legislation (Sakellariou et al., 2020).
The data used here to confirm the diagnosis and present symptoms corroborate the expectations outlined by authors like Gleason et al. (2021), Landes et al. (2021a), and Williamson et al. (2021) insofar as larger proportions of infection were found precisely among the most vulnerable, as expressed in their need for daily assistance (Williamson et al., 2021; Gleason et al., 2021; Landes et al., 2021a; Landes et al., 2021b).
The proportions of cross-infections among people with intellectual disabilities, family members, and caregivers that are 3 to 6 times higher among those who most need care, thus the most vulnerable. These higher rates may contribute to the high fatality rates and severe forms of among people with disabilities as shown in studies conducted by Melo et al. (2020) Almeida and Fontes-Dutra (2021) in Brazil, with the number of deaths doubling or tripling when compared to people without disabilities (Almeida and Fontes-Dutra, 2021; Melo et al., 2020).
This indicates that, without specific measures for isolation or management, the people with intellectual disabilities in this study who live in situations of higher vulnerability were proportionally the most impacted by coronavirus, as predicted by Armitage and Nellums (Armitage and Nellums, 2020).
It is necessary to highlight that these individuals were already experiencing situations of social isolation due to their disability conditions. The fact that they lived in the poorest segment of the population in homes usually shared with more than three people may have also contributed to the high numbers of COVID-19infections among those who most need routine care.
Vulnerability in a pandemic context can be understood as being more exposed or at higher risk of being infected, as well as not having timely access to diagnostic tests for the disease. It can be seen as having to overcome barriers in order to access health care once infected, as well as being the result of more frequent and more severe health and socio-economic consequences (Jesus et al., 2020).
Even when not infected, people with disabilities have been more exposed to negative outcomes because of the need for contagion mitigation and for prioritizing people with respiratory syndromes in rehabilitation health services. Municipal and intermunicipal transportation services that allowed many people with disabilities direct access to necessary interventions were interrupted. Thus, the continuation of rehabilitation activities and health care for people with disabilities was suddenly and exclusively transferred to community support groups and family members (Block et al., 2021; Jalali et al., 2020). This shows how policies should also be directed toward containing the emotional impacts caused by social isolation and the interruption of their daily therapies, which are significant losses to people with different types of disabilities (Aquino-Canchari et al., 2020).
Still regarding individual protection measures, the results related to seeking out services demonstrate that those who do not require care from others sought health services less frequently when symptomatic. They also maintained less social isolation, which may have contributed to their exposure to and transmission of COVID-19, as well as to the underreporting of confirmed cases in this subgroup.
According to Parley (2010), Reichenberger et al. (2020), and Gleason et al. (2021), people with intellectual disabilities are already more prone to negative outcomes due to comorbidity and because the routine services they need to maintain their physical and mental health were shut down. The evidence gathered by this study shows that this situation, combined with the need for assistance from others, can explain the high rates of coronavirus contamination among people with disabilities, their caregivers, and family members (Parley, 2010; Reichenberger et al., 2020; Ross et al., 2021).
Evidence from this study shows that those who always require care (e.g., constant supervision, home care, or handling and conducting daily routine activities) proportionally tested positive for COVID-19with more frequency. This demonstrates that individualizing responsibilities during the pandemic without considering the social networks individuals belong to produced worse outcomes among the most vulnerable (Block, 2019). In other words, the individualization of care to mitigate and restrict contagion failed.
From another perspective, vulnerability seems to have made positive contributions in that those who most require care sought out health services when symptomatic. The opposite happens among those who never require care. This leads to thinking that the participants who never need care were more exposed to the risk of infection and transmission because they isolated less frequently when having symptoms. Economic needs may also have contributed to this situation, seeing as people with disabilities figure predominantly in the informal job market and were the group that most lost jobs and income during the pandemic (Hazans, 2011).
It is worth emphasizing that over one-third of this study’s sample stated they did not receive any benefits. Approximately 80% of those who received emergency assistance to mitigate the financial impacts of the pandemic considered the aid offered by the federal government insufficient for meeting their needs. This demonstrates, once again, how measures to address the pandemic failed among people with disabilities.
This leads us to the contributions of Sakellariou et al. (2020), who showed how countries published recommendations for inclusive disability responses to COVID-19but did not ensure the practice of those recommendations. Despite measures to provide financial support, like in the case of Brazil, adults with intellectual disabilities both transmitted more and were more exposed to the coronavirus because they could not maintain social isolation as recommended and/or did not seek health services when symptomatic (Sakellariou et al., 2020).
It is important to stress that public services were the most sought out by all the groups in the study, which confirms the important role of SUS (Brazil’s Unified Health System) and of health professionals during the pandemic. It also points to what Armitage and Nellums (2020) alerted to when they spoke of the need to qualify health services for this population during the pandemic and to maintain a global commitment to providing services to them during the health crisis (Armitage and Nellums, 2020).
By reading Landes et al. (2021b) and Gleason et al. (2021) and reflecting on the proportions of infection among caregivers and family members, one can suppose they played an important role as coronavirus vectors for the study participants (Gleason et al., 2021; Landes et al,. 2021a). It is important to consider that this dynamic was reinforced by the social isolation policy implemented without specific guidelines for this population, especially since approximately 81% of the sample require help from others, most live in shared households with up to four people and belong to low-income brackets, and over 95% are not responsible for their households. Thus, these increases in household populations produced by social isolation and the need for income (often through informal work) may have interfered in the dynamics of care, resulting in higher exposure to coronavirus and COVID-19infection among the group being studied.
Therefore, the discussion proposed here suggests that the combination of factors that define the vulnerability of people with disabilities (expressed in their need for care from others in daily routines) with factors related to the measures used to address the pandemic (which did not operationalize specific actions to protect this group) may have contributed to the results of this study. This is particularly evident in their higher exposure to risks of infection due to routine care actions by family members and caregivers, and sheds light on the contributing factors to higher lethality rates and severe forms of COVID-19in people with intellectual disabilities.
Final considerations
This study aims to contribute to the debate on the impact of COVID-19among people with intellectual disabilities. It addresses a gap in the literature on this topic and can assist in producing better strategies for this population during future health emergencies. Other analyses of people with disabilities in situations like this have already demonstrated a tendency for negative outcomes in this group. This study has shown that the issue of needing care from others – yet another level of vulnerability for this group – further complicates the situation and can bring about worse outcomes for this population during and after the pandemic.
Observing people with disabilities from the perspective of their vulnerabilities and emphasizing their need for care as one of the essential points for analysis can produce more effective scientific research responses. This can also contribute to the development of policies that better reflect the reality of this population. Brazil is one of the 126 countries in the world that signed the International Convention on the Rights of Persons with Disabilities. This is expressed in the Brazilian Law of Inclusion, where the word “protection” is used 12 times. These documents state that people with disabilities in situations of risk, emergency, or public calamity shall be considered vulnerable, and that the government must adopt measures for their protection and security.
Therefore, this study helps demonstrate that among the factors that contribute toward higher coronavirus infection rates, severe forms, and deaths among people with disabilities are routine actions of care and a negligent social isolation policy that did not consider the specificities of people with disabilities or their family members. The quantitative data presented in this study and the theoretical contributions of studies on vulnerability, care, disability, and COVID-19are helpful to understanding that vulnerability and care act as a pendulum for people with disabilities, where vulnerability can at times grant protection while care can lead to higher risks of illness.
The study has some limitations, such as the sample being one of convenience and the data being collected exclusively online. This means we cannot draw direct conclusions regarding the universe of all people with intellectual disabilities in Brazil. However, the absence of official systems to present this data for analysis and the national distribution of this sample allows this study to portray an important overview of the reality of this population during the COVID-19pandemic in Brazil.
It can be concluded that not taking specific steps to protect the lives of people with disabilities during the pandemic, as widely suggested and advised by representative organizations, the scientific community, and health professionals, has contributed to the fact that the measures that were used to address COVID-19failed to address the specificities of this group. Rather, it magnified their exposure to risks of infection and of becoming sick, especially within their home where family members and caregivers were potential vectors of infection while providing daily routine care and support actions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors Diego Ferreira Lima Silva and Éverton Luís Pereira disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Project: Knowledge Construction, Accompaniment, Care and Prevention Networks through the National Federation of Apaes (Fenapaes) scholarship under the number 5519652/2020