
Abstract
Keywords
Introduction
Intellectual disability is a neurodevelopmental condition characterized by lower intellectual ability and impaired adaptive functioning, originating during childhood. It is categorized as mild, moderate, severe, or profound, based on intelligence quotient (IQ) and functional independence in daily activities, as defined by the National Institute for Health and Care Excellence (NICE) guidelines and the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (Cooper, 2017). Intellectual disability is frequently associated with “challenging behaviours”, a term used to describe culturally atypical behaviours that may threaten the safety of the individual or others, or significantly limit access to community resources (NICE, 2015). These behaviours can manifest as physical aggression, verbal hostility, self-injury, property destruction, inappropriate sexual behaviours, and pica.
Challenging behaviour affects an estimated 17–20% of adults with intellectual disabilities who are known to services (Bowring et al., 2019). These behaviours often arise as forms of communication, particularly for individuals with limited verbal expression. They may reflect underlying mental distress, unmet physical needs, or environmental stressors (Wolkorte et al., 2019). Lower adaptive functioning and limited communication skills have been associated with greater likelihood of challenging behaviour, underscoring the importance of behavioural and environmental interventions (Nicholls et al., 2023). As such, the emergence or escalation of challenging behaviour should prompt a comprehensive, multidisciplinary assessment to identify and address contributing factors before considering pharmacological strategies.
Challenging behaviour significantly disrupts the lives of individuals and their caregivers, leading to an increased risk of physical and mental health issues, financial strain, and reduced quality of life for caregivers (Hastings, 2002). The presence of challenging behaviour has been found to increase the likelihood of families seeking out-of-home placements for their children with challenging behaviour (Llewellyn et al., 2005). Moreover, in managing challenging behaviour families and carers can resort to inappropriate strategies to control behaviour, including unnecessary physical restraint (Jones et al., 2007). This can have further mental and physical health repercussions (Bush, 2006). Effective management of challenging behaviour is, therefore, vital for three main reasons. Firstly, to improve mental wellbeing and quality of life of the affected individual and their family or carers. Secondly, to mitigate the risk of physical harm to the person exhibiting challenging behaviour and to those that look after them. Thirdly, to reduce the risk of placement breakdown, which can create or worsening mental health disorders, and additionally have a dramatic effect on the quality of life of the individual and their family.
Optimal management of challenging behaviour, as outlined in the NICE guidelines, involves a stepwise, approach that prioritises non-pharmacological interventions to identify and address the underlying drivers of behaviour (NICE, 2015). This typically begins with a multidisciplinary assessment to identify contributing factors and the development of a comprehensive behavioural support plan. Positive Behavioural Support (PBS) forms a core component of this model, offering a proactive and holistic framework that integrates functional behavioural assessment with strategies to reduce behaviours of concern and improve quality of life (Konstantinidou et al., 2023). These strategies aim to improve quality of life and reduce behaviours of concern while promoting autonomy and social inclusion. Effective delivery relies on multidisciplinary coordination, consistency across care settings, and regular review.
Antipsychotics are commonly used to manage challenging behaviour in individuals with intellectual disabilities (Sheehan et al., 2015). However, there is mixed evidence as to the efficacy of antipsychotics in challenging behaviour, in the absence of underlying severe mental illness (De Kuijper et al., 2014; Tsiouris, 2010; Rapp et al., 2007; Sheehan & Hassiotis, 2017; Tyrer et al., 2008). The reason for conflicting evidence may be due to the difficulties conducting studies on heterogenous population and the lack of consensus on outcome measures. Antipsychotics have well documented adverse effects, including movement disorders, metabolic syndromes, hormone dysregulation, anticholinergic effects, and sedation. Furthermore, there is evidence that those with intellectual disabilities are more susceptible to the some of the adverse effects of antipsychotics (Ramerman et al., 2018; Sheehan et al., 2017). For this reason, NICE guidelines state that these medications should only be used if non-pharmacological methods have failed or if there is an immediate and severe risk to the individual, their carers or from placement breakdown (NICE, 2015). Despite this, antipsychotics are often inappropriately prescribed first line. Indeed, Public Health England estimated that in 2015 approximately 23,800 adults in England with an intellectual disability were prescribed antipsychotics in the absence of a psychotic illness (Gyles Glover and Rachael Williams, 2015). Another study also found the prevalence of antipsychotic prescriptions overall to be far greater than the prevalence of psychotic illness in those with intellectual disability, indicating the extensive use of these medications (Sheehan et al., 2015). Indeed, the prevalence of antipsychotic use in adults with learning disability in primary care was seen to be 29% in one study performed in Wales, and 21% in another earlier study performed in England (Idaiani and Suhardi, 2006; Molyneux et al., 1999). In rare cases, antipsychotic medication has been used to abuse individuals with intellectual disabilities. In 2011, staff at the Winterbourne View Hospital, an in-patient for individuals with intellectual disabilities, were found to be abusing patients, in part via the overprescription of antipsychotics. In response to this, the Winterbourne Medicines Programme and Report were commissioned to investigate and improve overprescription of antipsychotics for challenging behaviour (Winterbourne Medicines Programme: Improving the Use of Medicines in People with Learning Disabilities – NHS Improving Quality Report, n.d.). In addition, the ‘stopping over-medication of people with learning disabilities’ (STOMP) campaign within the UK aims to reduce the use of antipsychotics for challenging behaviour in those with intellectual disabilities (Stopping over Medication of People with a Learning Disability, Autism or Both (STOMP), n.d.). There is appetite amongst clinicians who look after those with intellectual disability to reduce reliance of antipsychotics for challenging behaviour. This is shown by a recent survey of UK psychiatrists working in intellectual disability. Over half of respondents stated that since the launch of the STOMP campaign they were less likely to prescribe antipsychotics for challenging behaviour (Deb et al., 2020). However, in the same survey, only 4.5% of respondents had successfully discontinued antipsychotic use in over half of their patients.
Despite national efforts such as the STOMP initiative and growing awareness of the harms associated with overprescription, concerns persist about the continued use of antipsychotics in people with intellectual disabilities, particularly when prescribed without a co-occurring psychiatric diagnosis. While prescribing trends have been well documented, there is comparatively less research into how prescribing decisions are made in day-to-day clinical practice, especially from the perspective of multidisciplinary teams who work directly with individuals displaying challenging behaviours. This gap in understanding is particularly important given that prescribing practices are often shaped by contextual, relational, and systemic factors that are not captured in administrative data. Understanding the perspectives of frontline practitioners may help illuminate the practical and organisational complexities that influence antipsychotic use, and identify opportunities for more tailored, sustainable improvements in care.
This gap in understanding is particularly important because prescribing decisions are often influenced by contextual, relational, and systemic factors that escape capture in administrative data. Multidisciplinary teams play a central role in navigating these complexities, yet their perspectives remain underrepresented in the literature. The intellectual disability partnership examined in this study operates within the UK NHS, delivering community-based specialist care for adults with intellectual disabilities of varying severity. The team includes professionals from psychiatry, nursing, psychology, occupational therapy, speech and language therapy, and physiotherapy, who collaborate to support individuals presenting with complex behavioural needs. While physical health is not managed directly, the team works closely with primary and secondary care to investigate and address medical contributors to behaviour. The stated aim of the partnership is to contribute to care planning in line with NICE guidelines, aiming to follow a person-centred, non-pharmacological approach to considering medication. This setting therefore offers a valuable lens to understand how everyday clinical realities influence the implementation of best practice around antipsychotic prescribing.
The aim of this paper was to explore views of the multidisciplinary team of antipsychotic prescription for challenging behaviour at one London intellectual disability partnership and to use the results of this analysis to propose solutions to reduce overprescription of antipsychotic. We analysed multidisciplinary team views via an online meeting and survey to create a driver diagram containing proposed solutions. We describe current beliefs regarding the appropriateness of such prescriptions and explore avenues towards, and barriers to, the reduction of the rate of antipsychotic prescription in challenging behaviour for service users with intellectual disabilities.
Methods
Research design
We conducted a cross-sectional qualitative study following COREQ reporting guidelines, which standardise qualitative reporting to improve rigour and transparency (Tong et al., 2007). This design allowed for an in-depth exploration of multidisciplinary team perspectives on antipsychotic prescribing for challenging behaviour in adults with intellectual disabilities, within a single NHS partnership in London. We used Braun and Clarke’s reflexive thematic analysis, selected for its ability to capture both implicit and explicit patterns across diverse data, while accommodating the complexity of real-world clinical contexts (Braun and Clarke, 2006). Both inductive and deductive coding approaches were employed to ensure findings were grounded in both participant perspectives and existing literature.
Study population
All multidisciplinary team members across disciplines (psychiatry, nursing, psychology, occupational therapy, physiotherapy, speech and language therapy, and administrative staff) were invited to participate via email. The invitation was sent in October 2021 by a doctor working with the psychiatry team. Convenience sampling was used due to feasibility constraints. Approximately 50 staff members were invited to participate, although the exact number cannot be determined due to reliance on multiple informal channels for distribution and the absence of a centralised distribution list. Participants could choose to join a structured online meeting or complete an aligned survey; some individuals participated in both. The service is a multidisciplinary community intellectual disability (ID) team supporting adults with varying degrees of intellectual disability and complex needs, including those presenting with challenging behaviour. Referrals for challenging behaviour are typically made for individuals whose behaviours pose significant risk to themselves or others, or where existing strategies have failed, meaning the team is more likely to see moderate to severe cases rather than all individuals with challenging behaviour. Support may include psychiatric input, behavioural planning, and coordination with social care providers. While the service does not employ behavioural analysts, behavioural interventions are delivered by clinical psychologists and other multidisciplinary team members trained in PBS. We report discipline-level representation to contextualise findings.
Data collection
Two tools were used: a structured online meeting and a web-based survey. Both explored understanding of current prescribing practices, challenges to reducing antipsychotic use, and perceived solutions. The meeting was chaired by a clinician and followed a semi-structured guide to promote consistency. The discussion was recorded, transcribed verbatim, and anonymised. The survey included Likert-scale questions and open-text boxes, piloted with multidisciplinary team members for clarity. Questions aligned with meeting prompts to enable triangulation. The full survey is provided in Appendix 1.
Analysis
Transcripts and open-text responses were analysed thematically using Braun and Clarke’s six-phase framework (Braun and Clarke, 2006). A combination of inductive coding and deductive coding based on prior literature was used. Deductive codes were informed by themes drawn from systematic reviews on antipsychotic deprescribing and barriers to behavioural intervention uptake. Qualitative data from the meeting and survey were integrated during theme development to synthesise overlapping perspectives. Coding was conducted in Microsoft Word and reviewed independently by two researchers. Both coders have clinical and research experience in intellectual disability services. Discrepancies in theme identification were resolved through discussion, enhancing analytical rigour. Descriptive statistics and figures for quantitative data were generated in R.
Ethics
All participants gave informed consent for recording, transcription, and use of anonymised data. As the study focused on staff feedback, ethical approval was not required under local guidelines, but ethical principles were upheld throughout.
Results
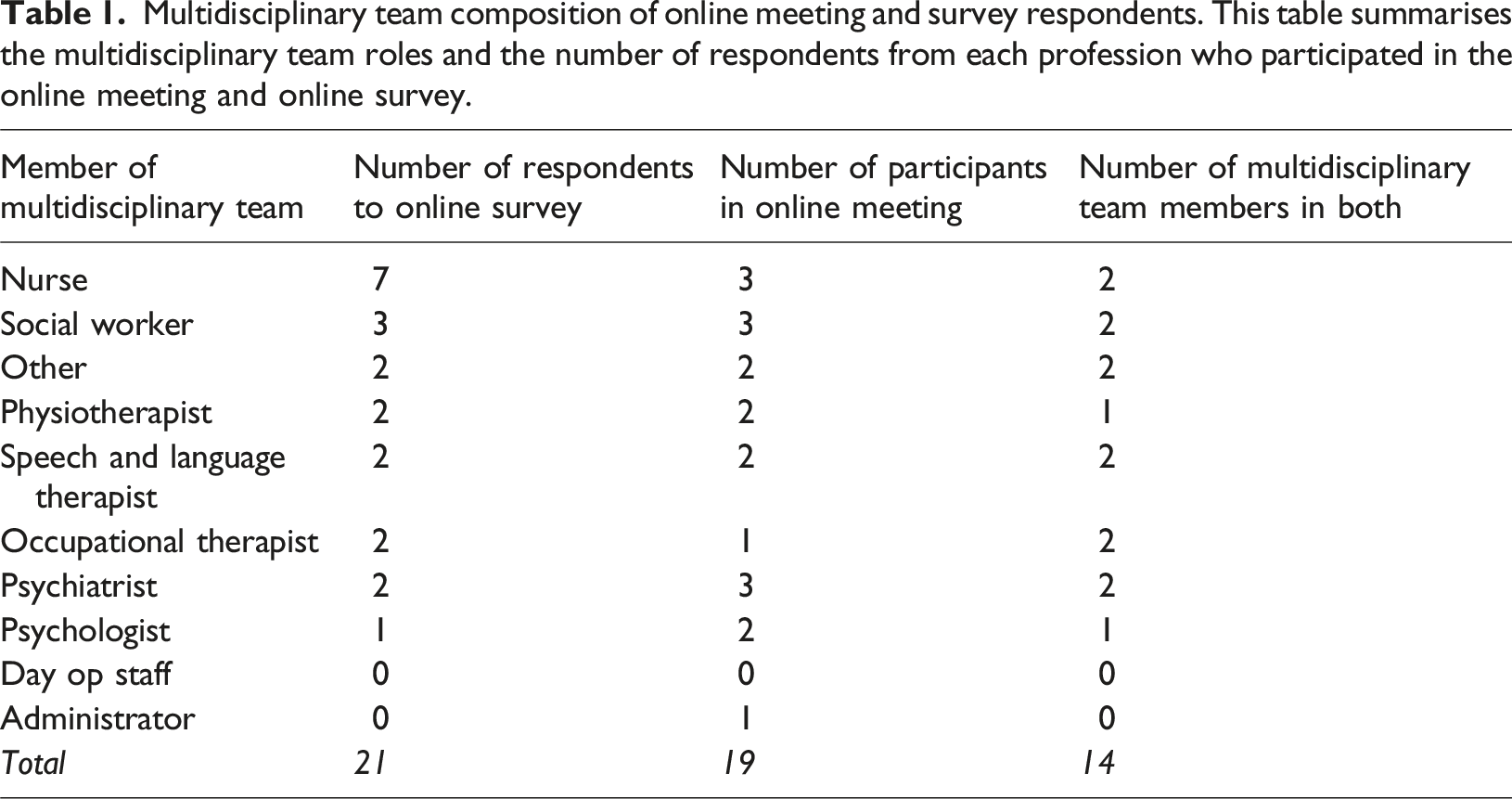
Multidisciplinary team composition of online meeting and survey respondents. This table summarises the multidisciplinary team roles and the number of respondents from each profession who participated in the online meeting and online survey.
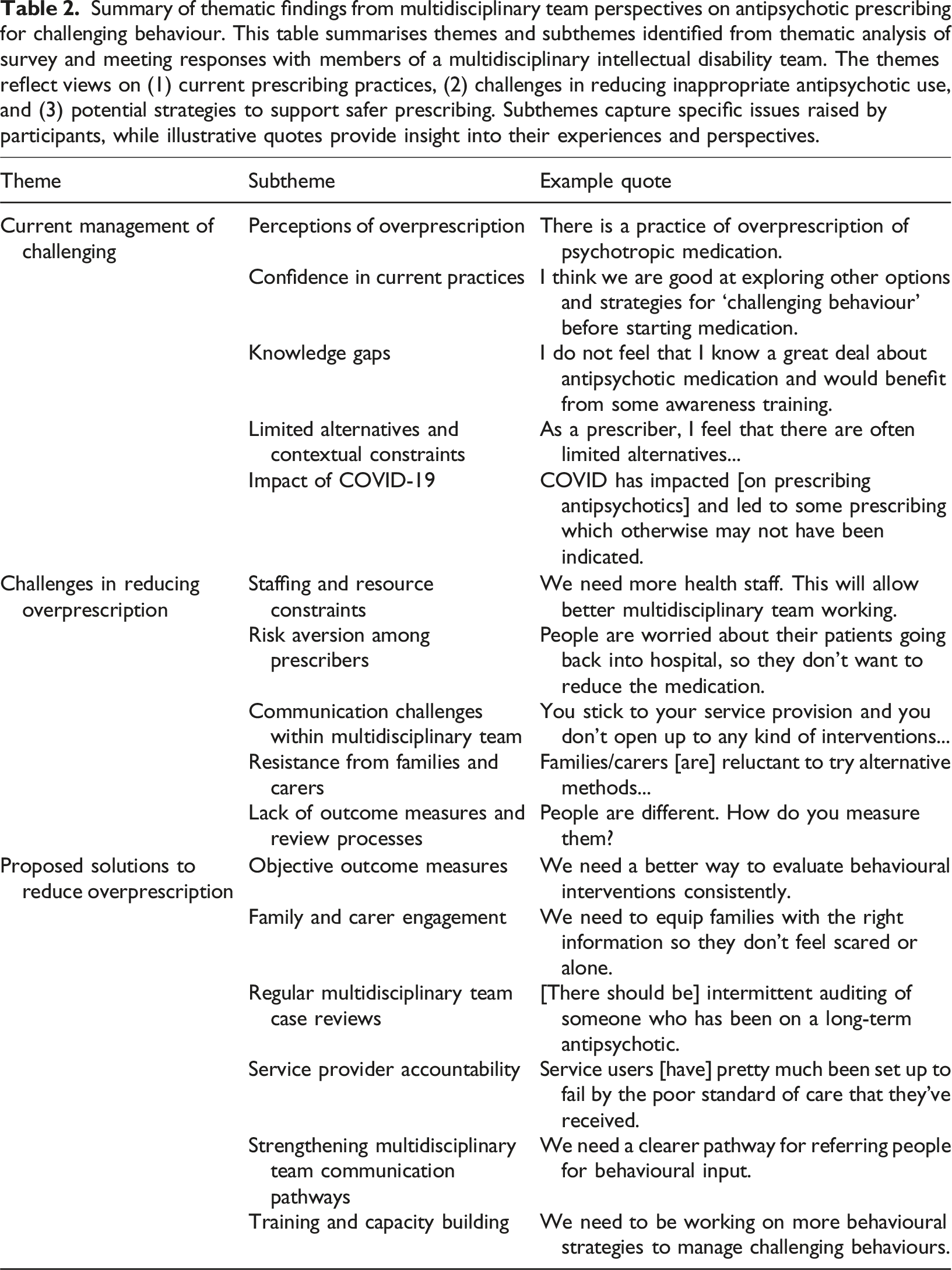
Summary of thematic findings from multidisciplinary team perspectives on antipsychotic prescribing for challenging behaviour. This table summarises themes and subthemes identified from thematic analysis of survey and meeting responses with members of a multidisciplinary intellectual disability team. The themes reflect views on (1) current prescribing practices, (2) challenges in reducing inappropriate antipsychotic use, and (3) potential strategies to support safer prescribing. Subthemes capture specific issues raised by participants, while illustrative quotes provide insight into their experiences and perspectives.
Theme 1: Current management of challenging behaviour
This theme captures multidisciplinary team views on the appropriateness and rationale behind current antipsychotic prescribing. Subthemes include: perceptions of overprescription, confidence in current practices, knowledge gaps, limited alternatives, and COVID-related changes.
Perceptions of overprescription
Survey responses showed a broad range of views on current prescribing practices. In response to the statement “Antipsychotics are overprescribed in our service,” 17 of 21 respondents (81%) selected scores between 6 and 10, indicating agreement, with 4 respondents (19%) strongly agreeing (scores 9 or 10). Only one respondent strongly disagreed (score 1). This range reflects ambivalence and diversity in perceptions within the team. As one participant noted: “There is a practice of overprescription of psychotropic medication.”
Several participants described witnessing service users on long-term antipsychotics without regular review: “Over the years clients are prescribed antipsychotics and not been reviewed for several years.”
Confidence in current practices
Despite concerns, some participants expressed confidence in their current approach to prescribing. This confidence was largely grounded in perceived adherence to guidelines and efforts to explore non-pharmacological interventions prior to prescribing: “I think we are good at exploring other options and strategies for 'challenging behaviour' before starting medication.” “I feel [the] psychiatry [team] works towards reducing antipsychotic medication where possible.”
However, these views were not universally shared and appeared to reflect differences between teams or disciplines.
Knowledge gaps
Participants reported varied familiarity with guidance on antipsychotic prescribing. Figure 1(B) shows a neutral distribution of scores on the statement “I am familiar with current prescribing guidelines for challenging behaviour.” Twelve respondents (57%) disagreed or strongly disagreed with this statement, and several admitted they had never seen such guidelines: “I have not seen any written guidelines.” “I’m not aware or [have] seen the guideline.” “I have read them previously but I am not up to date with them.” Responses to online survey questions. Responses out of 10. 1: strongly disagree. 10: strongly agree. This figure presents responses from 21 multidisciplinary team members regarding antipsychotic prescribing practices within an intellectual disability partnership. Panel A addresses views on whether antipsychotics are overprescribed. Panel B examines respondents’ awareness of the risks and benefits of antipsychotics. Panel C explores opinions on whether more should be done to reduce overprescription. Panel D assesses familiarity with challenging behaviour guidelines. Panel E evaluates confidence in the partnership’s ability to reduce overprescription.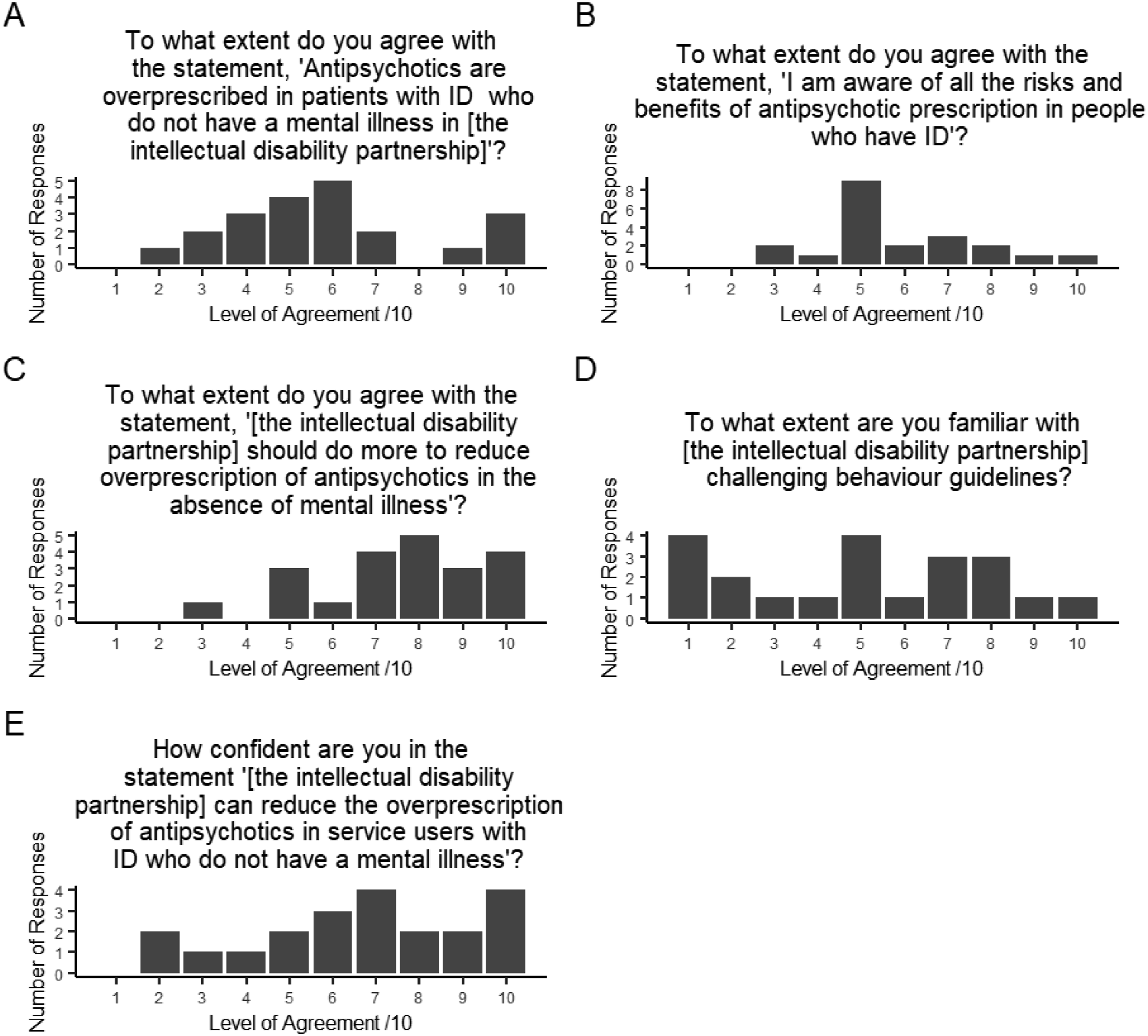
Perceived lack of knowledge also extended to understanding risks and benefits. As one participant acknowledged: “I do not feel that I know a great deal about antipsychotic medication and would benefit from some awareness training.”
Limited alternatives and contextual constraints
Several participants, particularly prescribers, raised concerns about the lack of non-pharmacological options available in the service. This was seen as a key reason for continuing antipsychotic use even when not clinically ideal: “As a prescriber, I feel that there are often limited alternatives. I would prefer to be prescribing less but have to balance this against the risks involved, such as placement breakdown, harm to self and others, [and] lack of community access.”
This theme echoed throughout multiple responses and was linked to staffing shortages, limited psychology availability, and systemic under-resourcing: “There is a combination of minimal psychology provision, lack of case management due to few permanent social workers, and the multidisciplinary team often not doing face-to-face work.”
Impact of the COVID-19 pandemic
The pandemic introduced additional strain on service provision, further compounding reliance on pharmacological management. Participants described an increase in prescribing during this period: “COVID has impacted [on prescribing antipsychotics] and led to some prescribing which otherwise may not have been indicated.” “There has been a spike [in prescribing antipsychotics] over the pandemic.”
One respondent described the cascading effect of service disruptions: “Difficulty with accessing meaningful activities during COVID may have impacted the increased prescription.”
Theme 2: Challenges in reducing overprescription
This theme outlines perceived barriers to safely reducing antipsychotic use, with the following subthemes: limited staff capacity, risk aversion, interprofessional communication barriers, resistance from families, lack of objective outcomes.
Staffing and resource constraints
Participants frequently cited systemic under-resourcing as a barrier to deprescribing. One respondent stated simply: “There's not enough of us.”
Another elaborated: “We need more health staff. This will allow better multidisciplinary team working.”
A shortage of psychological input was specifically flagged, limiting the feasibility of alternative behavioural interventions. These challenges were seen as foundational barriers to implementation of NICE-guided practice.
Risk aversion among prescribers
Clinicians reported reluctance to reduce medications due to fears of destabilising service users. These concerns were particularly acute around the risk of readmission or placement breakdown: “People are worried about their patients going back into hospital, so they don’t want to reduce the medication.” “There’s a general fear about what might happen—this can be a barrier to having the conversation about reducing [antipsychotics].”
Some participants acknowledged this risk aversion was understandable but believed it reinforced dependency on pharmacological management.
Communication challenges within the multidisciplinary team
Fragmentation of care across disciplines emerged as a theme. Participants felt that opportunities to collaborate on behavioural strategies were sometimes missed: “You stick to your service provision and you don’t open up to any kind of interventions out there that you could explore.” “Speech and language therapy would really like to be more involved than we are in some of the behavioural work that goes on.”
The absence of regular structured communication, such as formal case review meetings, was seen to limit holistic planning.
Resistance from families and carers
Several participants reported that family members and paid carers were hesitant to reduce or change medications: “Families/carers [are] reluctant to try alternative methods [to manage challenging behaviour].” “They’re scared of taking [the service user] off [antipsychotics] or demanding they are put on them.”
This resistance was often attributed to a lack of education about side effects and the evidence base for behavioural interventions.
Lack of outcome measures and review processes
The lack of objective tools to track behavioural outcomes made it difficult for teams to evaluate the success of interventions or justify reductions in medication:
“People are different. How do you measure them? Is it effective for them and for their carers?”
Participants suggested that regular reviews and clear metrics could support safer and more transparent decision-making: “[There should be] intermittent auditing of someone who has been on a long-term antipsychotic [such as an] [multidisciplinary team] case review.”
Theme 3: Solutions for reducing overprescription
This theme summarises solutions focused around key problem areas and solutions identified by the multidisciplinary team. Solutions were classified into six actionable areas for improvement: monitoring and outcome metrics, family education, multidisciplinary team case reviews, provider accountability, communication pathways, staff training. These are summarised in a driver diagram (Figure 2). Driver diagram illustrating proposed solutions to reduce overprescription of antipsychotics for challenging behaviour. This driver diagram outlines key areas for intervention identified through thematic analysis of multidisciplinary team survey and meeting responses. The aim is to reduce inappropriate antipsychotic prescribing in individuals with intellectual disabilities. Six primary drivers were identified: improved measurement, family engagement, multidisciplinary team case reviews, provider accountability, communication across the team, and staff training. Each primary driver is supported by secondary drivers, which are specific actions or mechanisms that facilitate change. These proposed solutions reflect participants’ insights on challenges and potential solutions for better care of challenging behaviour.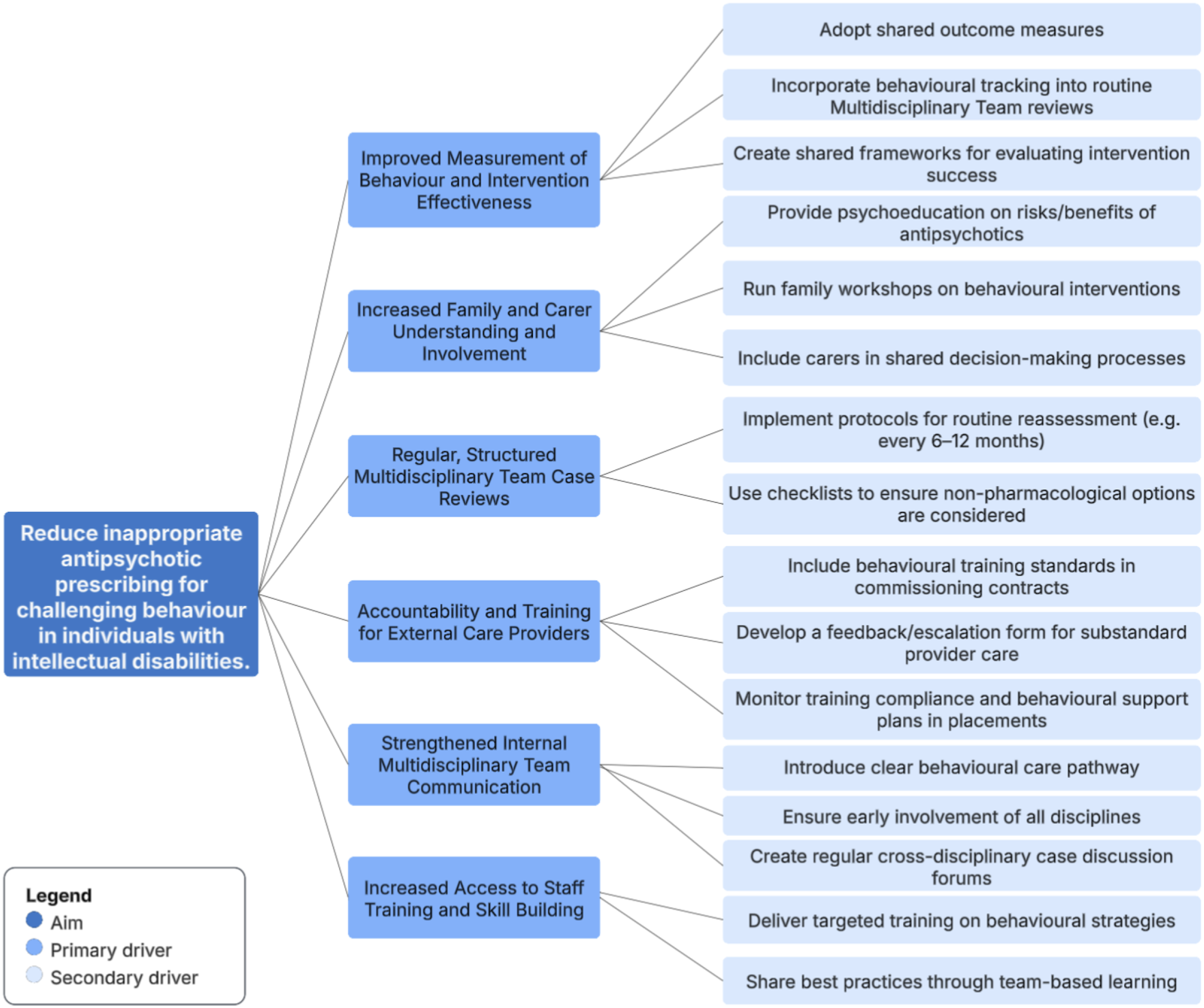
Introduction of objective outcome measures
Participants emphasised the absence of structured, shared tools to assess behavioural outcomes and evaluate intervention effectiveness. This lack of measurement was seen as a barrier to justifying dose reduction and promoting confidence in non-pharmacological alternatives. “We are unsure of the outcomes or effectiveness of our interventions and approach.”
The adoption of validated scales such as the Modified Overt Aggression Scale (MOAS) could help track changes in behaviour and inform case review discussions. Establishing standardised outcome metrics would not only support clearer evaluation but also create shared reference points across professionals, carers, and commissioners.
Enhanced family and carer engagement
A recurring theme was the influence of families and carers—both as a barrier and a potential facilitator of deprescribing efforts. Participants described how reluctance or fear among families could lead to resistance against reducing medications, particularly when no alternative supports were available or well understood. “Families/carers [are] reluctant to try alternative methods [to manage challenging behaviour].” “We need to equip families with the right information so they don’t feel scared or alone.”
Targeted psychoeducation and structured engagement, such as family workshops or shared decision-making meetings, to demystify behavioural interventions and support trust in deprescribing processes.
Regular multidisciplinary team case reviews
Participants noted the absence of consistent review mechanisms, particularly for individuals who had remained on medication for many years. Structured, multidisciplinary case reviews were seen as a solution for identifying inappropriate long-term antipsychotic use and ensuring that prescribing decisions were regularly revisited. “[There should be] intermittent auditing of someone who has been on a long-term antipsychotic.” “Input and interventions from the [Multidisciplinary Team] is invaluable in enabling dose reduction.”
Formalising case reviews would create accountability, enable more holistic care planning, and offer a clear mechanism for escalating concerns or testing reductions in a monitored setting.
Service provider accountability
External care providers, such as supported living services and residential homes, were frequently mentioned as both critical partners and barriers to best practice. Participants expressed concern that some services lacked the training or ethos required to manage challenging behaviour without overreliance on medication. “It seems very much that the service users [have] pretty much been set up to fail by the poor standard of care that they’ve received from their provider.”
Commissioning standards for behavioural competence, clearer escalation pathways for concerns, and a standardised proforma to report poor-quality provision to local authorities or care commissioners could increase service provider accountability.
Strengthening multidisciplinary team communication pathways
Participants described fragmented working practices across professional groups, with limited opportunity for coordinated behavioural planning. Some disciplines, such as speech and language therapy, reported being underutilised in behaviour-focused care.
“Having [Multidisciplinary Team]input at the right time to explore alternatives to medication [will improve outcomes]”
Improved internal referral processes and shared care pathways are ways to integrate contributions across the team and reduce default reliance on pharmacological approaches.
Training and capacity building
A lack of confidence in non-pharmacological management strategies was noted and training was seen as a solution to equip all involved with a shared framework and skillset for addressing challenging behaviour proactively. “There is a lack of training and sharing of skills across the team.” “We need to be working on more behavioural strategies to manage challenging behaviours.”
Discussion
This study explored multidisciplinary team views on the management of challenging behaviour in individuals with intellectual disabilities, the barriers to reducing antipsychotic overprescription, and potential solutions. Thematic analysis identified three overarching themes. First, current management was marked by divergent views on prescribing practices, with some confidence in existing approaches but substantial knowledge gaps and limited access to alternatives. Second, barriers to deprescribing included inadequate resources, risk aversion, fragmented communication, lack of outcome measures, and resistance from families or carers. Third, participants proposed a range of actionable solutions, including implementing objective behavioural metrics, regular multidisciplinary team case reviews, clearer pathways for escalation, staff training, and enhanced family engagement. These solutions are visually summarised in a driver diagram.
Our findings align with a growing body of literature that documents the persistent barriers to reducing antipsychotic medication use in people with intellectual disabilities. In a national survey, Deb et al. found that while most UK psychiatrists supported antipsychotic reduction in principle, many encountered practical obstacles, including difficulty accessing consistent multidisciplinary input, limited availability of behavioural alternatives and lack of clear local guidelines (Deb et al., 2020). Risk aversion was also a prominent concern: psychiatrists reported fears about relapse or deterioration in behaviour, particularly in the absence of strong team support. These concerns are echoed in qualitative studies such as Adams et al., which found that both clinicians and families feared worsening behaviours if medications were withdrawn, and that people with intellectual disabilities themselves expressed similar anxieties about returning symptoms (Adams et al., 2024). Similar to our study, family and carer resistance to deprescribing has also been highlighted in several studies, often rooted in past negative experiences or lack of trust in alternative interventions (Adams et al., 2023; De Kuijper et al., 2022; ). Fragmented team communication and unclear responsibility for initiating reviews further contributed to delays. This finding partially echoes insights from Kleijwegt et al., who reported that support staff often felt underinformed and anxious during discontinuation, and highlighted the importance of prescriber communication with the wider team (De Kuijper et al., 2022). Deb et al. also note that psychiatrists viewed the lack of multi-agency input as a key factor in failed withdrawal attempts (Deb et al., 2020).
Multiple studies have emphasized that effective antipsychotic medication reduction requires a collaborative, multidisciplinary approach and active stakeholder engagement, which our findings strongly support. Participants in our study stressed the value of clear, ongoing communication within the multidisciplinary team, as well as with family caregivers and the individuals themselves. This mirrors conclusions by Adams et al. that implementing deprescribing initiatives “requires a multidisciplinary collaborative care approach and education for stakeholders” (Adams et al., 2024). When all members of the team are involved in planning and monitoring a withdrawal, and when roles are well-coordinated, participants felt more confident managing the process. Prior research suggests such teamwork is associated with better outcomes: the systematic review by Adams et al. (2023) found that deprescribing interventions had more positive behavioural and health effects when delivered via an interdisciplinary model, as opposed to a lone practitioner (Adams et al., 2023).
When comparing our results with the literature, we find not only convergence on problem areas but also pointers toward solutions. A common theme is the need for better training, guidance, and systemic support to empower teams to change prescribing practices. Participants in our study suggested more education for staff, clearer protocols for gradual dose reduction, and readily available specialist input (e.g. psychologists or pharmacists). Such proposals are well-aligned with recent recommendations. For example, Deb et al. concluded there is an “urgent need” for formal guidelines and systematic medication reviews to support antipsychotic withdrawal in this population (Deb et al., 2020). National initiatives like NHS England’s STOMP have raised awareness and set expectations for reduction, but our findings and others suggest more practical tools are needed to translate policy into practice. Encouragingly, some tools are emerging, such as SPECTROM training program for staff to reduce overprescription of antipsychotic medication in intellectual disability services (Barratt et al., 2023). That toolkit provides structured resources and training for support staff and clinicians, aiming to bolster skills in positive behaviour support and risk management during deprescribing, and has been shown to increase staff knowledge (Limbu et al., 2025). Our participants’ calls for clearer pathways and skill-building reflect a readiness to embrace such resources. In practice, this means not only upfront planning but also monitoring and follow-up, for instance, having the multidisciplinary team conduct regular review meetings post-reduction to promptly address any behavioural or mental health concerns.
Beyond these established themes, our study contributes novel insights that extend the current literature. One striking finding was the emphasis some participants placed on service provider accountability - the idea that organizations or clinical leads should be answerable for high rates of antipsychotic prescribing and should champion reduction efforts. This may reflect growing frustration with slow progress, but also a recognition that top-down commitment could drive practice change. Another relatively unique theme from our data was a sense of optimism for change. Despite acknowledging barriers, many multidisciplinary team members in our study expressed cautious optimism that prescribing culture is beginning to shift. The optimism in our cohort may stem from the concerted efforts and policy attention in recent years; it’s possible we are witnessing the early impact of initiatives like STOMP leading increased awareness. It could also be related to the diverse composition of our focus groups: having a mix of disciplines brainstorming together may have reinforced a problem-solving attitude that is less evident when one role (e.g. support staff alone) is interviewed in isolation. Indeed, the team’s optimism is supported by evidence from a pilot randomised controlled trial, which demonstrated that reducing antipsychotic use in challenging behaviour is feasible and can decrease adverse effects without significant behavioural or mental health deterioration (McNamara et al., 2017) .
A key strength of this study is its inclusion of multiple stakeholders from various disciplines within the multidisciplinary team, offering a comprehensive understanding of the diverse perspectives and challenges professionals face in managing challenging behaviour. This multidisciplinary approach supports collaborative problem-solving and the development of targeted interventions to address the root causes of overprescription. However, the study’s focus on a single intellectual disability partnership in London means the findings are context-specific and may not fully reflect practices in other settings. Additionally, while the study highlights professional perspectives, incorporating input from patients and caregivers would provide a more comprehensive understanding of the impact of antipsychotic use and alternative strategies.
Future studies should include multiple intellectual disability partnerships from diverse regions to provide a broader perspective on the challenges and strategies for managing challenging behaviour. Research should also assess the effectiveness of the proposed solutions in reducing antipsychotic overprescription in individuals with intellectual disabilities. Further studies could explore additional interventions, such as introducing independent prescribers (e.g., qualified pharmacists or nurses) to facilitate timely medication reviews and offer a second opinion on antipsychotic use. Establishing a dedicated coordinator for the challenging behaviour pathway could also enhance accountability and improve communication within the multidisciplinary team.
This study highlights persistent challenges in reducing antipsychotic overprescription for people with intellectual disabilities, while identifying practical solutions grounded in multidisciplinary collaboration, structured review processes, staff training, and stakeholder engagement. Our findings reaffirm the importance of systemic support, cross-sector accountability, and team-wide ownership of change. As momentum builds through national initiatives and emerging training tools, there is an opportunity to embed these practices more consistently. Realising this potential will require ongoing investment, evaluation, and co-production with individuals and families, to ensure that future care is not only less reliant on medication, but more person-centred, inclusive, and sustainable.
Supplemental Material
Supplemental Material - “I would prefer to be prescribing less”: Perceptions on antipsychotics and challenging behaviour
Supplemental Material for “I would prefer to be prescribing less”: Perceptions on antipsychotics and challenging behaviour by Caitlin Norris-Grey, Aileen Carmen in Journal of Intellectual Disabilities
Footnotes
Acknowledgments
We extend our gratitude to the staff at Haringey Learning Disabilities Partnership for their participation and contributions to this study. We also thank Dr. Ken Courtenay for his invaluable support and guidance.
Declaration of conflicting interests
The authors declare no conflicts of interest related to this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.