
Abstract
Introduction
Over recent decades, the demographic landscape of disability and ageing has undergone a profound transformation. Advances in healthcare, improved living conditions, and the gradual consolidation of disability rights frameworks have significantly extended the life expectancy of people with intellectual disabilities (Herge, 2024; Reppermund et al., 2020; Tyrer et al., 2022). For the first time in history, many individuals with intellectual disabilities are reaching older adulthood, a milestone that demands rethinking traditional models of support, care, and inclusion across the life course (Wark, 2024).
However, this demographic success reveals structural tensions that remain largely unresolved. The systems historically responsible for supporting people with intellectual disabilities were not designed to accommodate the specific needs, aspirations, and rights of an ageing population (De Leeuw et al., 2022; El Mrayyan et al., 2025). As a result, older adults with intellectual disabilities continue to face significant barriers to full participation, autonomy, and recognition as subjects of rights, particularly in later life stages when dependency and vulnerability are often assumed rather than critically examined (Araten-Bergman and Bigby, 2024; McCausalnd et al., 2021).
Contemporary definitions of intellectual disability emphasize its relational and contextual nature. It is understood as a condition involving significant limitations in intellectual functioning—encompassing reasoning, learning, and problem-solving—and in adaptive behaviour, which includes the practical, social, and conceptual skills necessary for everyday life (Schalock et al., 2021). Modern perspectives reject deficit-centered views, highlighting instead the dynamic interaction between individual characteristics and environmental barriers or supports. From this standpoint, disability is not a fixed trait but the result of mismatches between personal capabilities and the demands or opportunities offered by social contexts.
The process of ageing among people with intellectual disabilities exhibits distinctive features compared to the general population. Biomedical research has consistently documented a pattern of premature ageing, manifesting in earlier onset of chronic diseases, sensory deterioration, functional decline, and dementia-related syndromes (Jacinto et al., 2023; Tena-Bernal et al., 2021; Tyrer et al., 2022). This biological vulnerability is compounded by cumulative social disadvantages across the life course, such as lower educational attainment, restricted labour market participation, limited access to preventive health care, and precarious housing conditions (Smith et al., 2024; Wark, 2024). These layered inequalities generate accelerated pathways to dependency, exclusion, and invisibility in later life.
Beyond biological ageing, recent studies highlight that the meaning and practice of self-determination in later life differ substantially from earlier stages of adulthood (Jormfeldt and Tideman, 2021; Álvarez-Aguado et al., 2024). In young and middle adulthood, self-determination is often associated with autonomy in employment, independent living, and the pursuit of personal goals (Cegarra et al., 2023; Sinclair et al., 2024). In contrast, for many older adults with intellectual disabilities, autonomy is experienced more as interdependence, negotiated daily within relationships of care, family expectations, and service routines (Parchomiuk et al., 2025). These ways of exercising agency are deeply influenced by social and cultural norms concerning care, respect for older people, and shared decision-making within close relationships (Cvijetić et al., 2024). Understanding self-determination in later life therefore requires examining how personal preferences, relational dynamics, and cultural values interact to shape the ways in which older adults with intellectual disabilities exercise choice and control in their everyday lives (Schiettecat et al., 2024).
Nevertheless, the trajectories of ageing in people with intellectual disabilities are not uniform. Growing evidence highlights the role of environmental, relational, and attitudinal factors in shaping highly diverse ageing experiences (Connolly, 2024). Some individuals maintain active social lives, exercise autonomy in daily decisions, and continue to contribute meaningfully to their communities. Others experience rapid loss of agency, social isolation, and disengagement from valued activities (Belperio et al., 2024; Holmgren and Ahlström, 2024; McCausland et al., 2023). These divergent trajectories underscore that vulnerability in ageing is not inevitable but socially mediated and, to a large extent, modifiable.
In this complex landscape, self-determination emerges as a key concept for understanding and promoting well-being in older adulthood. Defined as the ability to act as the causal agent of one’s own life, making choices and decisions based on personal preferences and goals (Wehmeyer, 2000), self-determination is strongly associated with emotional resilience, higher life satisfaction, stronger self-esteem, and sustained community participation (Kuld et al., 2023; Mumbardó‐Adam et al., 2023; Vaucher et al., 2020; Wehmeyer, 2020). It plays a protective role against the psychological and social risks associated with ageing, such as loss of control, institutionalization, and disengagement.
The conceptualization of self-determination has evolved from early models that focused primarily on individual skills—such as autonomy and self-regulation (Wehmeyer, 2000)—to relational and dynamic models, such as the Theory of Causal Agency, which emphasizes that self-determined action arises through volitional, agentic, and empowered processes embedded in social environments (Shogren et al., 2015; Shogren and Raley, 2022). This theoretical shift highlights that promoting self-determination requires not only strengthening personal capacities but also transforming the relational and systemic conditions that facilitate—or hinder—autonomous action.
International research consistently shows that ageing tends to be associated with a decline in self-determination opportunities among people with intellectual disabilities. Studies in Europe, North America, and Oceania report that as individuals age, there is a tendency for decision-making power to shift away from the individual toward families, caregivers, or service providers (e.g., Jormfeldt & Tideman, 2021; Sexton et al., 2016; Vaucher et al., 2020). This process is often reinforced by risk-averse service cultures and organizational priorities centered on protection rather than empowerment (Bigby and Putnam, 2021). As a result, older adults with intellectual disabilities may experience a progressive erosion of their ability to make decisions about daily routines, living arrangements, social participation, and healthcare, affecting their sense of agency and well-being (Álvarez-Aguado et al., 2021).
Moreover, the unequal distribution of opportunities for self-determination across different groups within the population has been consistently documented. Older women with intellectual disabilities, individuals with higher support needs, and those living in institutional or group home settings face greater barriers to exercising autonomy (Kuld et al., 2023; Mumbardó-Adam et al., 2023; Álvarez-Aguado et al., 2024). These intersecting vulnerabilities expose the limits of person-centered frameworks when they are not accompanied by systemic transformations that genuinely prioritize individual will and choice.
Evidence also underscores the importance of promoting self-determination throughout the life course. Individuals who develop skills related to goal-setting, problem-solving, self-advocacy, and informed decision-making earlier in life are more likely to maintain higher levels of autonomy, independence, and emotional well-being in older adulthood (Frielink et al., 2021; Wehmeyer and Shogren, 2020). Conversely, when these capacities are not supported, the risks of institutionalization, social isolation, and passive dependency increase markedly.
Despite these significant insights, research on self-determination in older adults with intellectual disabilities remains limited and geographically concentrated. Most available studies have been conducted in high-income countries with consolidated welfare systems, leaving important gaps regarding how these dynamics unfold in different cultural, economic, and policy contexts (e.g., Albuquerque and Carvalho, 2020; Heller et al., 2011; Vaucher et al., 2020; Wong and Chow, 2021). In Latin America—and specifically in Chile—empirical knowledge about ageing and self-determination remains scarce, fragmented, and poorly integrated into public policy design (Vega et al., 2023; Álvarez-Aguado et al., 2021, 2023).
Although national legislation, aligned with the principles of the Convention on the Rights of Persons with Disabilities (United Nations, 2006), formally recognizes the right to autonomy and independent living, the translation of these principles into practice remains inconsistent. Service models often prioritize care over empowerment, and cultural attitudes favouring familial authority and overprotection persist, limiting opportunities for personal agency in older adulthood (Vega et al., 2023; Álvarez-Aguado et al., 2024).
Against this backdrop, there is an urgent need to investigate how older adults with intellectual disabilities living in community settings in Chile experience and construct self-determination in their daily lives. Exploring these experiences is essential not only to expand empirical knowledge but also to inform the design of inclusive, rights-based public policies that promote dignity, personal agency, and full participation throughout the ageing process.
This study seeks to contribute to this objective by analysing the self-determination experiences of older adults with intellectual disabilities living in diverse community contexts in the Chilean setting. Through their narratives, the research aims to shed light on the personal, relational, and structural factors that facilitate or hinder autonomy, and to generate evidence that guides the development of more inclusive, person-centred support models in later life.
Materials and methods
Participants
The study included 105 older adults with mild or moderate intellectual disabilities, recruited from community programs, day centers, and residential facilities located in two regions of Chile: the Metropolitan Region and the Region of Valparaíso. Participants were selected through purposive sampling, seeking to maximize variability in living arrangements, levels of support needs, and health conditions, in order to capture a broad spectrum of experiences related to self-determination.
Eligibility criteria required individuals to: (a) have a formal diagnosis of mild or moderate intellectual disability, established according to the diagnostic criteria set forth in the DSM-5; (b) be aged 45 years or older at the time of participation, acknowledging that people with intellectual disabilities often experience ageing-related changes earlier than the general population (Tena-Bernal et al., 2021); and (c) demonstrate basic communication skills, either verbal or supported, to meaningfully engage in the interview process. Individuals with severe intellectual disabilities, profound disabilities, severe uncorrected sensory impairments, or acute medical conditions at the time of data collection were excluded to ensure the reliability and depth of the qualitative data.
The final sample consisted of 57 women (54.3%) and 48 men (45.7%), with chronological ages ranging from 45 to 85 years (M = 68.7, SD = 7.2). Regarding living arrangements, 29.5% of participants lived in family homes, 23.8% in community-supported living programs, and 46.7% resided in long-term residential facilities.
Educational attainment was generally low: 81.9% of participants had not completed primary education, reflecting the historical exclusion from formal schooling experienced by people with disabilities in Chile. Only 11.4% had completed primary education, and 6.7% reported partial experiences in secondary education, primarily through nonformal or special education programs.
Participants exhibited varying levels of support needs. Based on caregiver and service provider reports, 42.9% required intermittent or limited supports for activities of daily living, while 57.1% required extensive or pervasive supports. Regarding health status, 65.7% of participants reported at least one chronic condition, with hypertension (42.8%), type 2 diabetes (28.5%), and sensory impairments (36.1%) being the most prevalent. Additionally, 13.3% had received clinical diagnoses of early-stage dementia or mild cognitive impairment.
Social networks varied widely. Regular contact with immediate family members was reported by 38.1% of participants, while 21% maintained sporadic relationships with extended family. Notably, 40.9% of participants relied primarily on formal support staff or peers within their living environments for emotional and practical support. Participation in community-based recreational or social activities was limited, with only 17.1% reporting involvement in external group activities.
In economic terms, 84.7% of participants depended on public disability pensions or state subsidies as their main source of income. Only a minority had histories of intermittent, informal employment. Financial management was generally overseen by family members or residential staff, with very limited personal financial autonomy.
Instrument
Data collection was conducted through semi-structured interviews specifically designed to explore self-determination experiences among older adults with intellectual disabilities living in community settings. The interview guide was developed using the Causal Agency Theory (Shogren et al., 2015; Shogren and Raley, 2022) as the conceptual framework, incorporating its three core dimensions: volitional action, agentic action, and empowered action. Based on these dimensions, the interview questions were organized into thematic areas that aimed to capture participants’ experiences of autonomy, goal-setting, and perceived control, as well as the barriers and supports influencing self-determined action.
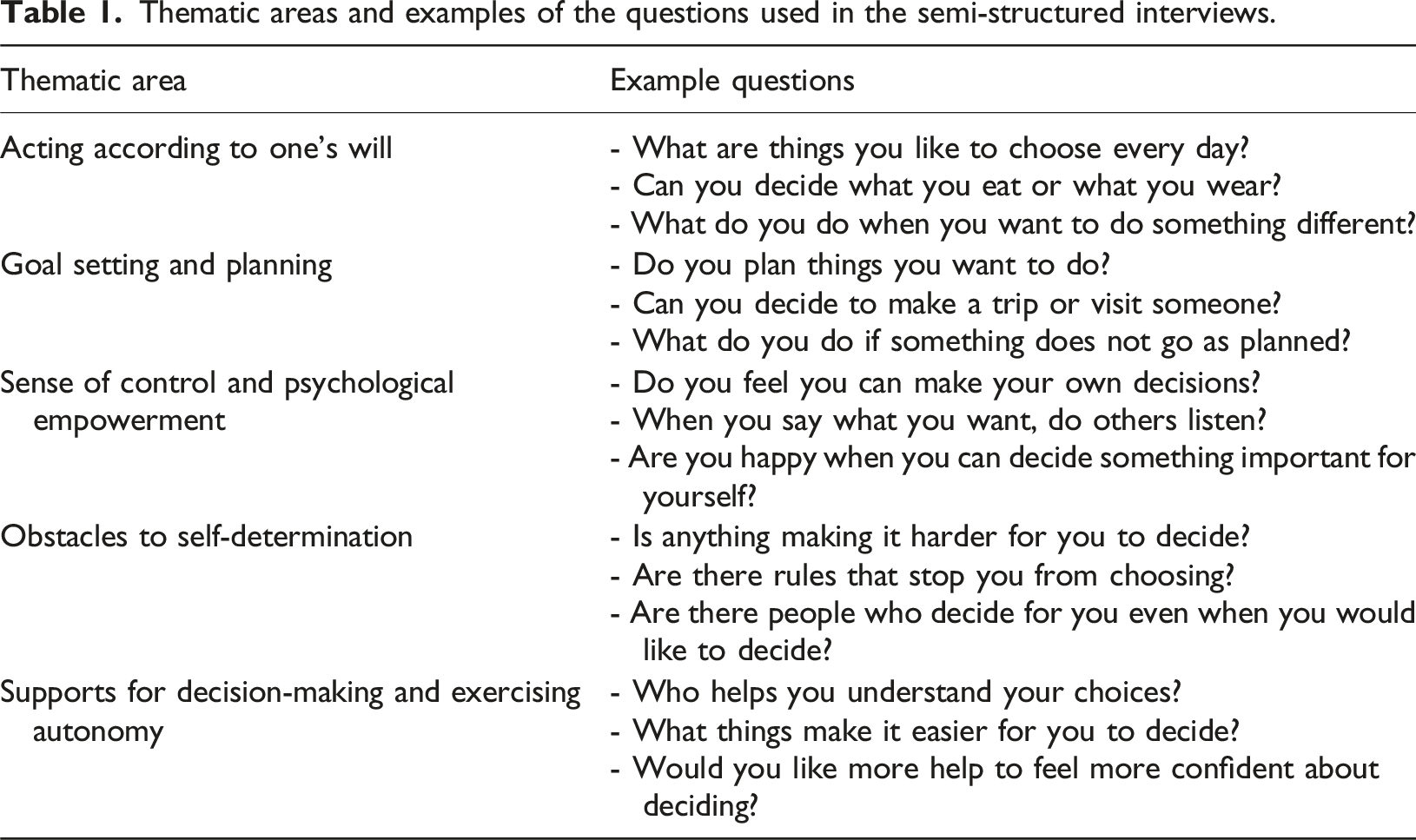
The instrument included 24 open-ended questions, distributed across five thematic areas: (a) Acting according to one’s will: explored the extent to which participants made daily decisions based on personal preferences and interests, such as choices related to food, clothing, leisure, and routines; (b) Goal setting and planning: examined participants’ abilities to set personal goals, plan activities, and solve problems to achieve desired outcomes; (c) Sense of control and psychological empowerment: addressed participants’ perceptions of their capacity to influence important aspects of their lives and the recognition they received from others regarding their decision-making rights; (d) Obstacles to self-determination: identified external or internal factors that limited the expression of volitional, agentic, or empowered actions, such as restrictive rules, lack of support, or environmental barriers; and (e) Supports for decision-making and exercising autonomy: explored the types of assistance participants used or desired to facilitate understanding, choice-making, and the exercise of control in their lives.
To ensure the quality, conceptual coherence, and practical relevance of the instrument, the interview guide underwent a two-step content validation process, the description of which has been made more explicit in the revised version of the manuscript.
In the first stage, the preliminary version was evaluated by a panel of five experts with recognized experience in the fields of intellectual disability, ageing, and inclusive research. Each expert reviewed the items in the guide using a 4-point Likert scale (1 = not relevant or clear at all; 4 = very relevant or clear), considering three main criteria: clarity of wording, theoretical consistency with the Causal Agency Theory, and practical relevance to the context of ageing and intellectual disability. The quantitative data from these evaluations were used to calculate the Content Validity Index (CVI), both for each item and for the instrument as a whole.
The initial CVI was 0.87, which indicated good content validity, although opportunities for improvement were identified. Based on the panel’s feedback, specific adjustments were made: reformulation of ambiguous items, linguistic simplification to enhance cognitive accessibility, and revision of the order and wording of questions to strengthen alignment with the three theoretical dimensions (volitional, agentic, and empowered action). In addition, pictorial supports and everyday examples were incorporated to facilitate comprehension among older adults with varying levels of literacy. After these revisions, the final version achieved an overall CVI of 0.92, representing an excellent level of agreement among experts regarding the clarity, relevance, and theoretical consistency of the items.
In the second stage, the revised guide was piloted with four older adults with mild intellectual disabilities who were not part of the final study sample. This pilot application allowed for the evaluation of the semantic comprehension and cognitive accessibility of each item. Based on this feedback, minor linguistic modifications were made to ensure that the questions progressed from concrete to abstract topics and that the visual supports (pictograms and photographs) effectively facilitated the recognition of situations and the evocation of personal experiences.
Thematic areas and examples of the questions used in the semi-structured interviews.
Data collection
This study employed a qualitative, exploratory, and descriptive design. All study procedures were reviewed and approved by the Scientific Ethics Committee of Universidad de las Américas, Chile. Data collection was conducted in collaboration with a total of 12 organizations, including 5 community-based programs, 4 day centers, and 3 residential services that provide support to older adults with intellectual disabilities across the Metropolitan and Valparaíso regions. Participating organizations included both public and private services operating under varied support models, ranging from family-based care to supported living programs and formal residential facilities. These organizations assisted in identifying potential participants and in coordinating interviews, spaces, and informed consent procedures.
Prior to fieldwork, a pilot study was conducted with eight older adults with mild or moderate intellectual disabilities who were not part of the final sample but shared similar sociodemographic profiles. This phase allowed evaluation of question comprehension, participants’ engagement, and the functionality of the communication supports provided. Based on feedback from participants and support professionals, minor adjustments were made to simplify wording, incorporate additional concrete examples, and organize questions from more concrete to more abstract topics. Visual aids (such as pictograms and photographs representing activities and emotions) were strengthened, particularly for participants with low functional literacy or memory difficulties.
In its final version, the interview lasted an average of 45 minutes, an appropriate duration to maintain participants’ attention and emotional comfort. When signs of fatigue, distraction, or anxiety were observed, participants were offered the option to pause, reschedule, or divide the interview into two shorter sessions, although the vast majority completed the interview in a single session without difficulty.
Fieldwork took place between April and July 2024. A total of 129 individuals were initially contacted across the collaborating services. Of these, 105 agreed to participate, resulting in a final response rate of 81.4 %. Recruitment was conducted gradually and adapted to the communicative and cognitive needs of potential participants. In the initial stage, service providers made the first approach, verbally explaining the study’s purpose in accessible language. Subsequently, the research team conducted individual meetings with interested participants (and their legal representatives when applicable) to provide detailed information about the study’s objectives, procedures, and the voluntary nature of participation. Easy-to-read consent forms were developed, accompanied by pictograms illustrating key concepts such as “you can say no” or “you can leave at any time.” Consent forms were read aloud when necessary, and participants were encouraged to ask questions or express doubts. In cases where a legal guardian was designated, informed consent was obtained from the guardian alongside the participant’s explicit verbal assent.
Interviews were scheduled at times convenient to participants, conducted in familiar, private, and quiet spaces within community centers, family homes, or residential facilities, ensuring privacy and emotional safety. Each interview was conducted by one of five trained researchers, all with extensive experience in accessible communication and working directly with individuals with intellectual disabilities.
Interviews followed a semi-structured format with flexible adaptations to meet each participant’s communication needs. Interviewers paraphrased or simplified questions, offered concrete examples, and used visual or gestural aids to facilitate understanding. Abstract concepts such as autonomy or empowerment were illustrated through relatable everyday situations (e.g., choosing between different activities or making decisions about personal care). Interviewers carefully monitored non-verbal signs of confusion, discomfort, or fatigue, adjusting the interview pace and style accordingly.
All interviews were audio-recorded with prior consent and supplemented by detailed field notes capturing contextual elements, emotional responses, level of engagement, and use of communication supports. Observations of participants’ body language, facial expressions, and tone were considered essential for accurate interpretation of responses.
At the conclusion of each interview, a verbal summary of the main topics discussed was provided as a form of member checking, allowing participants to confirm, clarify, or correct the researcher’s interpretation. After each session, interviewers expanded their field notes with reflective observations on the interaction process, the interviewer’s emotional reactions, potential biases, and methodological suggestions for subsequent interviews.
Data analysis
All audio-recorded interviews were transcribed verbatim to ensure fidelity to participants’ expressions. During transcription, any information that could potentially identify individuals or organizations was anonymized to protect confidentiality. In addition to the interview transcripts, detailed field notes produced by the researchers were incorporated into the analysis.
A reflexive thematic analysis was conducted following the six-phase framework proposed by Braun et al. (2017). The analysis was coordinated by the principal investigator and involved two additional independent coders with prior experience in qualitative research and disability studies.
The first phase involved an immersion process in which researchers repeatedly read the transcripts and field notes to familiarize themselves with the content, noting initial reflections, salient features, and potential patterns. In the second phase, using NVivo software, coding was performed by systematically organizing data segments into meaning units. A mixed coding strategy was employed, combining inductive identification of emergent concepts with deductive coding based on the interview guide structure and the core dimensions of the Causal Agency Theory (Shogren et al., 2015; Shogren and Raley, 2022). In total, approximately 950 significant data segments were coded across the dataset.
To ensure consistency in the initial coding process, 25% of the interviews were independently coded by two researchers. Inter-coder reliability was calculated only at this preliminary stage, using a simple agreement index that reached 87.9% consistency across independently coded segments. This calculation aimed to verify the degree of shared understanding of the emerging codebook and ensure transparency in the application of the coding framework, rather than to quantify thematic convergence. The reflexive thematic analysis approach does not rely on statistical reliability measures as a final validation criterion (Braun et al., 2017); instead, the calculation served as a procedural check during the early phase of coding. Discrepancies were discussed and resolved through consensus meetings, and the coding framework was iteratively refined to enhance conceptual clarity and coherence across coders.
The third and fourth phases focused on the systematic development, review, and refinement of themes, ensuring traceability between raw data and final interpretations. The 950 coded segments were initially clustered into 45 preliminary categories, which captured recurrent or contrasting meanings across participants. Through constant comparison and triangulation among three researchers, these categories were examined for conceptual proximity, empirical density, and relational overlap. They were progressively integrated into 15 subthemes, each representing a coherent analytical unit supported by sufficient data volume (18–24 coded excerpts per subtheme, involving at least five distinct participants).
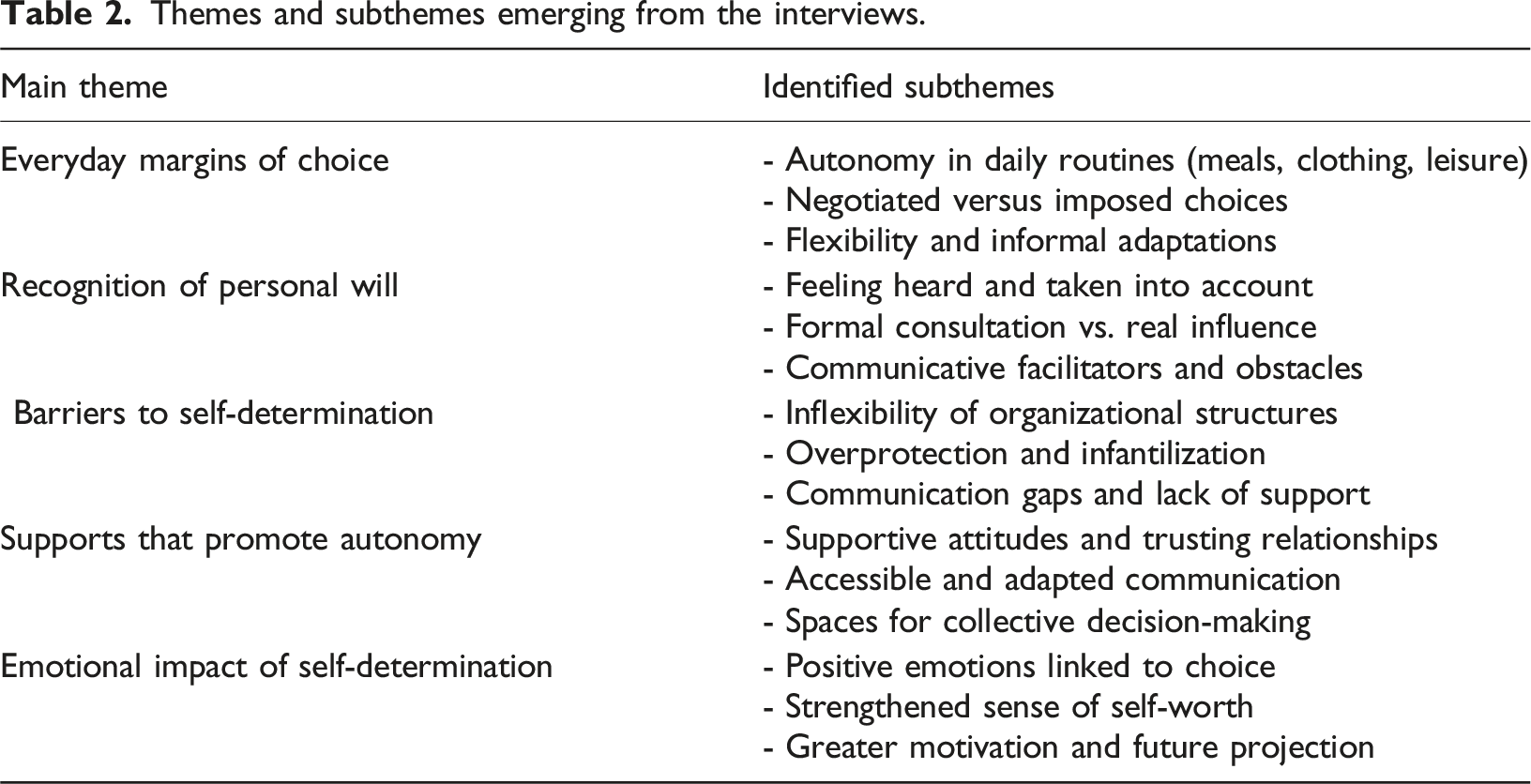
Each subtheme was evaluated according to three analytic criteria: internal coherence (consistency among quotations), conceptual distinctiveness (absence of redundancy across subthemes), and cross-representativeness (occurrence across gender, age, and residential contexts). A descriptive frequency analysis indicated that the themes with the greatest data density were Barriers to self-determination (27% of coded data) and Supports that promote autonomy (23%), followed by Everyday margins for choice (19%), Recognition of personal will (17%), and Emotional impact of self-determination (14%).
To enhance analytical credibility, three review rounds were conducted among the researchers: consolidating preliminary categories and confirming data saturation; refining conceptual boundaries and naming the 15 subthemes; and reviewing the five overarching themes in relation to the Causal Agency Theory (Shogren et al., 2015; Shogren and Raley, 2022), ensuring theoretical alignment and reflexive transparency. An internal audit of coding decisions was conducted to confirm consistency between empirical evidence and interpretive outcomes.
In the fifth phase, these five overarching themes were clearly defined and named, each comprising a set of three subthemes that captured the complexity and diversity of participants’ experiences related to autonomy, decision-making, goal setting, perceived control, barriers, and support systems. Efforts were made to preserve the richness and contextual nuances of participants’ voices throughout the theme development process.
Finally, the sixth phase involved the integration and writing of the analytical report. This process prioritized the inclusion of diverse, illustrative quotations alongside field note excerpts to offer a holistic and context-sensitive interpretation of the findings. Special attention was given to highlighting both convergent and divergent experiences across participants, thereby providing a nuanced understanding of self-determination in later life for people with intellectual disabilities in community environments.
Results
Themes and subthemes emerging from the interviews.
To safeguard confidentiality while maintaining analytical transparency, each participant was assigned a unique alphanumeric code. Quotations are presented using this code, followed by gender and region of residence (e.g., P15, woman, Metropolitan Region). This system was established during data analysis to enable contextual interpretation of participants’ statements without revealing identifiable information such as names or specific institutions.
Everyday margins of choice: navigating daily autonomy
Participants’ narratives reflected diverse experiences of autonomy in everyday decisions within community contexts. Making choices about clothing, meals, leisure activities, and personal routines was often described as a fundamental way of maintaining control over one’s life. For many, these decisions, although seemingly small, carried a deep symbolic value. As a woman from the Metropolitan Region (P15) expressed, “In the mornings, I choose what I want to wear. Sometimes it’s simple things like picking a scarf, but it’s my decision.” These daily acts were experienced as essential to preserving a sense of identity and agency.
Nonetheless, the degree of autonomy varied significantly across situations and support arrangements. While some participants reported that they were consulted regularly about their preferences, others described environments where their choices were limited or predefined. A man from Valparaíso (P42) noted, “At home, I decide my breakfast. But at the center, it's already made, and you just eat what’s there.” His account highlights how opportunities for decision-making could fluctuate depending on the setting or the nature of the support received.
Negotiated decision-making was a recurrent experience among participants. Many described processes where they could express a preference but within narrow options. As one participant (P33, Metropolitan Region) recounted, “When I go to the day center, they ask if I want to do painting or music, but those are the only choices.” While having options was appreciated, some participants felt that their real interests or spontaneous desires were often overlooked when choices were restricted to preselected activities.
Moreover, there were instances where the offer of choice appeared superficial. A woman from Valparaíso (P61) reflected, “Sometimes they say ‘you can choose,’ but if you don’t pick something quickly, they decide for you.” This kind of pressured or time-limited choice was experienced as stressful rather than empowering, suggesting that genuine self-determination requires not only offering alternatives but also creating conditions for thoughtful decision-making.
Despite these limitations, participants also shared experiences of flexible and respectful support that enhanced their sense of autonomy. A man from the Metropolitan Region (P5) recounted, “Last week, I didn’t feel like going to the park, and they said it was okay to stay home and watch a movie instead” These informal adaptations, although sometimes dependent on individual staff or family members, were described as essential for feeling respected and in control of one's own rhythm.
Some participants emphasized the importance of being able to adjust daily plans based on mood, health, or personal interests. A woman from Valparaíso (P24) shared, “If I’m tired, I tell my sister, and she says we can change plans. It makes me feel that what I want matters.” Such flexibility, grounded in trust and communication, was experienced as a powerful affirmation of their autonomy.
However, participants also recognized that the degree of flexibility often depended on the personal attitudes of those providing support. As a man from the Metropolitan Region (P30) remarked, “It depends who is helping that day. Some listen and adjust, and others just say ‘no, today is like this’.” This variability highlights the fragility of self-determination when it is contingent on interpersonal goodwill rather than embedded in consistent support practices.
Overall, while participants valued the daily spaces for choice they could access, these opportunities were often negotiated, partial, and uneven. Autonomy in daily life remained a complex interplay between personal preferences, organizational or familial structures, and the attitudes of those providing support, emphasizing the need for environments that consistently respect and nurture individual decision-making.
Recognition of personal will: the value of being heard
Feeling that their preferences were acknowledged emerged as a fundamental aspect of participants’ experiences of self-determination in community life. Many participants emphasized that being consulted about everyday matters—even seemingly minor ones—reinforced their sense of dignity and self-worth. A woman from the Metropolitan Region (P12) reflected, “When they ask me if I want to go out or stay home, it feels like they care about what I think.” For participants like her, the simple act of being asked was not merely procedural; it carried significant emotional meaning, affirming their status as autonomous individuals.
However, experiences of being genuinely heard were not universal. Some participants described situations where consultation existed in form but lacked real influence. A man from Valparaíso (P38) shared, “They tell me ‘you can say what you want,’ but in the end, they already have everything planned.” This experience of symbolic participation—where opinions were solicited but disregarded—generated frustration and reinforced a sense of invisibility.
Communicative accessibility played a decisive role in shaping whether participants could effectively express their preferences. Several participants noted that when support persons used clear, simple language or visual aids, it greatly facilitated participation. As one woman explained (P71, Valparaíso Region), “When they show me pictures or explain things slowly, I can really say what I want. If they talk fast, I just nod and say yes to anything.” Such testimonies highlight that supporting self-determination is not only about offering choices, but also about ensuring the conditions necessary for expressing and understanding them.
Nonetheless, even when communication supports were available, some participants reported that expressing disagreement remained difficult. Fear of negative reactions often constrained their ability to assert preferences. A man from the Metropolitan Region (P44) described, “Sometimes I want to say no, but I think maybe they’ll get upset, so I end up saying yes.” This dynamic suggests that relational trust is fundamental to enabling authentic choice, beyond merely providing accessible communication formats.
Participants also expressed that genuine recognition involved not only listening but responding meaningfully to their input. A woman (P57, Metropolitan Region) recalled with satisfaction, “I told my brother I wanted to go to the market instead of the park, and he said ‘okay, let’s do that’. It made me feel important.” Moments like these, where preferences shaped actions, reinforced feelings of agency and respect.
In contrast, when participants’ expressions were disregarded or overridden, feelings of resignation and diminished self-worth were common. A man from Valparaíso (P63) stated, “After a while, you stop saying what you want. It’s easier to just go along with what they plan.” Such experiences reveal the cumulative effect of unacknowledged voices, leading some individuals to internalize passivity as a survival strategy within systems that nominally promote inclusion but often fall short of genuine responsiveness.
Moreover, the emotional tone of interactions played a fundamental role. Participants highlighted that the attitude with which support persons asked and responded to their choices shaped whether they felt respected. A woman (P9, Valparaíso Region) noted, “When my neighbour asks me what I want to do and smiles, I feel relaxed. When people ask without looking at you, it feels like they don’t really care.” This observation underscores that fostering recognition of personal will requires not only structural practices of consultation but also relational quality, warmth, and authenticity in interactions.
Overall, participants’ narratives suggest that recognition of personal will is a dynamic, relational process. It is not simply about offering choices, but about creating communicative and emotional conditions that validate individuals’ preferences, respect their rhythms, and translate expressed desires into meaningful actions whenever possible. In community contexts, where family members, support workers, and peers play pivotal roles, this recognition constitutes a key pillar for sustaining self-determination throughout later life.
Barriers to self-determination: constraints in community life
While many participants identified opportunities for exercising autonomy, they also described persistent barriers that limited their capacity to make and act upon decisions. One of the most frequently mentioned obstacles was the rigidity of schedules and service structures, even within community-based supports. Participants often spoke of feeling trapped within routines that allowed little room for personal preference or adaptation. A man from the Metropolitan Region (P22) explained, “At the day center, everything is set. Breakfast at nine, workshop at ten, lunch at one. You just follow the times, even if you feel different that day.” His experience reflects how standardization, intended to provide structure, can unintentionally suppress individual agency.
The weight of overprotective attitudes also emerged as a major constraint. Many participants perceived that family members or support workers, despite good intentions, made decisions for them out of fear for their safety or well-being. A woman from Valparaíso (P39) shared, “My sister always says, 'better not go alone, you might fall.' So she decides where I go, even when I feel fine.” Although rooted in concern, these protective dynamics often resulted in participants feeling infantilized and excluded from decisions about their own lives.
Communication barriers compounded these relational challenges. Participants noted that not being given enough time to process information or not having explanations adapted to their understanding often led to passivity. As one man described (P17, Metropolitan Region), “When they explain fast or use complicated words, I just say yes. I don’t want to seem dumb.” Such accounts highlight how inaccessible communication can quietly erode self-determination, leading individuals to acquiesce simply to avoid embarrassment or frustration.
Lack of individualized support was another recurrent theme. Several participants emphasized that while formal supports existed, they often did not cater to their specific ways of understanding or expressing choices. A woman (P52, Valparaíso Region) reflected, “At the workshop, they give everyone the same papers to choose activities, but I don't read very well. No one asks me if I need help.” Without adjustments to accommodate different communication needs, opportunities for real choice remained out of reach for many.
Beyond formal service settings, participants also experienced barriers within family contexts. Some reported that even decisions about small daily activities were subtly controlled by relatives. As one man from the Metropolitan Region (P34) explained, “My brother says I can decide, but if I pick something he doesn’t like, he convinces me to change.” Such dynamics illustrate how influence and persuasion, even when gentle, can undermine the authenticity of participants’ choices.
In addition, several participants internalized these barriers over time, describing a gradual withdrawal from trying to assert their preferences. A woman (P28, Valparaíso Region) admitted, “Before I used to ask to go places or do things, but now I just go with the flow. It’s easier that way.” This resignation suggests that repeated experiences of not being heard or having decisions overridden can lead to a learned helplessness that further restricts opportunities for self-determination.
Likewise, participants emphasized that inconsistencies in support practices created uncertainty about when and how they could exercise autonomy. Some days choices were respected; on others, they were ignored. As one man (P49, Metropolitan Region) summarized, “One day they say, 'you decide,' and the next they already decided for you. You never know.” This unpredictability eroded trust and made participants hesitant to express their preferences, fearing their voices might be disregarded again.
In general, participants' accounts depict barriers to self-determination as multifaceted, encompassing structural rigidity, relational dynamics, communication challenges, and psychological adaptations to long-standing patterns of limited choice. Overcoming these barriers would require not only procedural changes but also a cultural shift toward consistently valuing and facilitating the voices of older adults with intellectual disabilities within community life.
Supports that promote autonomy: enabling everyday self-determination
Amid the barriers described, participants also shared multiple experiences where specific forms of support strengthened their ability to make decisions and exert control over their lives. One of the most valued elements was the presence of support persons—whether family members, community workers, or neighbours—who engaged with them through respectful listening and patience. A woman from the Metropolitan Region (P6) described, “When my sister asks what I want to do on Sunday and really waits for my answer, I feel calmer and can think better.” Such interactions, based on genuine interest and the willingness to give time, were fundamental for building participants’ confidence in expressing preferences.
Accessible communication strategies were equally essential. Participants emphasized that using clear language, visual aids, or step-by-step explanations allowed them to understand options and participate meaningfully in decisions. A man from Valparaíso (P46) explained, “When they show me pictures of activities, it’s easier to see what I want. Words alone confuse me sometimes.” These adaptations were not perceived as infantilizing but rather as empowering tools that respected different ways of processing information and decision-making.
The establishment of collective decision-making spaces also contributed to promoting self-determination. Some participants reported that in community centers or group activities, meetings were held where everyone could propose ideas and vote on upcoming activities. As a woman from the Metropolitan Region (P21) recounted, “We have meetings every month. They ask us what we want to do, and if many of us want the same thing, they organize it.” Being involved in these participatory processes fostered a sense of agency and belonging, showing that decisions could emerge from dialogue and negotiation rather than being imposed unilaterally.
Importantly, participants noted that the way support persons framed decision-making made a significant difference. When options were presented without pressure, with respect for their tempo and emotional state, participants reported feeling more secure and valued. A man (P9, Valparaíso Region) shared, “They ask me if I want to join, but they always say it’s okay if I don’t feel like it. That makes me less afraid to say what I really want.” Respecting participants’ right to decline without fear of reprimand was experienced as a critical dimension of authentic support.
Participants also highlighted the importance of having emotional anchors—trusted people they could turn to when feeling uncertain about choices. Some described family members or staff who helped them think through decisions without imposing opinions. A woman from the Metropolitan Region (P58) explained, “Sometimes I doubt what’s best, and my cousin listens and helps me sort my ideas. She doesn’t tell me what to do, just listens and asks questions.” This form of relational support promoted reflection and strengthened participants’ sense of ownership over their decisions.
Lastly, flexibility in everyday arrangements was seen as a decisive factor in enabling self-determination. Participants appreciated when plans could be adjusted to accommodate their feelings, health, or changing interests. As a man from Valparaíso (P40) expressed, “If I don’t feel well, they let me rest without pushing. If I feel good later, I can join the group. It’s my choice.” This flexibility not only respected their right to decide but also recognized the fluctuating nature of personal needs, particularly in later stages of life.
On the whole, participants’ experiences suggest that promoting self-determination in community contexts is not solely about offering formal choices, but about embedding practices of respect, adaptation, and relational trust into everyday interactions. Support that is responsive to communication styles, emotional states, and evolving interests creates fertile ground for autonomy to flourish authentically in the lives of older adults with intellectual disabilities.
Emotional impact of self-determination: well-being, motivation, and future projection
Participants’ narratives consistently reflected the deep emotional resonance of having opportunities to make decisions about their lives. Being able to express preferences, choose daily activities, or influence personal routines was associated with positive emotions such as happiness, pride, and a renewed sense of personal worth. A woman from the Metropolitan Region (P13) shared, “When I decide what I want to eat or where I want to go, I feel like I matter. It makes me happy, like I’m someone important.” These moments, even when linked to small everyday choices, contributed significantly to strengthening participants’ self-esteem and emotional security.
In contrast, the absence of opportunities for decision-making was often associated with feelings of frustration, resignation, or emotional withdrawal. Several participants described how being excluded from decisions gradually diminished their motivation. A man from Valparaíso (P35) reflected, “If everything is decided already, after a while you stop wanting things”. This loss of agency over time seemed to erode not only interest in activities but also participants’ broader engagement with their environment.
The link between exercising self-determination and maintaining or enhancing motivation was particularly evident when participants spoke about setting small goals or planning future activities. A woman from the Metropolitan Region (P74) recounted, “After I chose to start the cooking classes, I felt excited again. Now I think about other things I want to learn.” These accounts highlight how opportunities for autonomous decision-making can reignite aspirations, counteracting the apathy and passivity often associated with aging and social exclusion.
Moreover, participants often connected feelings of pride and satisfaction not simply to the outcomes of decisions, but to the mere fact of being recognized as capable of choosing. A man (P18, Metropolitan Region) explained, “Even if it’s just deciding what movie to watch, when they ask me and respect my answer, I feel strong, like I can do more.” The psychological empowerment derived from these experiences appeared to extend beyond the immediate choice, influencing broader feelings of competence and confidence.
Conversely, the emotional toll of being disregarded or overruled in decision-making processes was palpable. Participants who reported that their preferences were systematically minimized described feelings of sadness and insignificance. A woman from Valparaíso (P55) shared, “When no one asks me what I want, it feels like I’m invisible.” Such testimonies illustrate how the lack of recognition can deeply affect emotional well-being, reinforcing isolation and low self-worth.
Another important dimension that emerged was the role of social validation in amplifying the emotional benefits of self-determined action. Several participants emphasized that having their choices supported by others—family, friends, or staff—enhanced their feelings of belonging and relational trust. A man (P7, Valparaíso Region) stated, “When I say I want to go to the park and everyone supports me, I feel part of the group, not left out.” This dynamic shows how emotional well-being linked to self-determination is not purely individual but deeply embedded in social recognition and communal bonds.
Finally, opportunities for choice often served as catalysts for future-oriented thinking, even among participants facing significant health or support needs. Being able to make present decisions was linked to imagining and planning for new experiences. A woman from the Metropolitan Region (P26) reflected, “Since I started choosing more things, I even dream about going on a trip. Before, I didn’t think about tomorrow.” This illustrates how self-determination in daily life can activate hope, ambition, and a renewed sense of future possibilities, reaffirming the enduring human drive for growth and fulfilment at all stages of life.
Discussion
This study explored the experiences of self-determination among older adults with intellectual disabilities in Chile. The findings show that self-determination is not a fixed individual attribute but a relational, dynamic, and context-dependent process, deeply influenced by the quality of interpersonal relationships, the flexibility of support systems, and the accessibility of communication environments.
From an ecological and contextual perspective, aligned with the Theory of Causal Agency (Shogren et al., 2015; Shogren and Raley, 2022), the results highlight that the exercise of self-determination depends less on personal skills and more on how environmental factors enable—or restrict—the expression of will. Concrete opportunities for choice, the presence of appropriate and individualized supports, and the respect for personal rhythms and preferences largely determine whether an individual can exercise control over their life. In this sense, self-determination must be understood not only as an individual capacity but as a structural condition of justice.
Beyond disability-related aspects, the findings also reveal how ageing processes intersect with self-determination in later life. Participants described that ageing brought both new constraints and new forms of agency: physical and cognitive changes sometimes limited autonomy, yet ageing also fostered stability, emotional maturity, and clearer self-knowledge that allowed more deliberate decision-making. In this stage of life, autonomy was often expressed through interdependence rather than independence, negotiated daily within relationships of care, reciprocity, and social belonging. These results echo previous research showing that, in older adulthood, self-determination is not lost but redefined through adaptive and relational forms of control (Jormfeldt and Tideman, 2021; Kuld et al., 2023; Álvarez-Aguado et al., 2021). In this sense, ageing and self-determination should be understood as intertwined trajectories that depend on the quality of support environments and cultural expectations around dependency, dignity, and participation.
One of the most significant findings is the marked variability in daily decision-making margins. While some participants described choosing activities, meals, or clothing, others encountered predefined structures where autonomy was limited to constrained or negotiated options. These findings are consistent with studies by Cudré-Mauroux et al. (2020) and Vaucher et al. (2020), who emphasize that the promotion of self-determination in people with disabilities depends largely on the relational culture and the flexibility of support services rather than on individuals’ cognitive profiles.
In this context, being heard and having one’s preferences taken seriously emerged as critical dimensions of agency. Participants attributed substantial emotional value to being consulted and having their opinions influence daily life. Expressing preferences—and witnessing their consequences—was perceived as an affirmation of dignity and recognition. These results align with previous research that links self-determination with higher self-esteem, motivation, and psychological well-being (Mumbardó-Adam et al., 2023; Vicente et al., 2020; Wehmeyer, 2020). Conversely, the absence of consultation, or the perception that opinions are systematically disregarded, was associated with feelings of frustration, resignation, and emotional disconnection, echoing findings from Iriarte et al. (2024) and Vega et al. (2023).
The analysis also identified persistent barriers that undermine the exercise of self-determination in community settings. Rigid schedules in support programs, overprotective attitudes from family members, inaccessible communication strategies, and limited individualized support emerged as key constraints. Although often framed as protective or efficient practices, these approaches tended to suppress opportunities for decision-making and reinforced passive roles. Consistent with other studies (McCausland et al., 2021, 2023; Vaucher et al., 2020), the findings suggest that focusing primarily on care and protection can inadvertently weaken personal agency, making it harder for individuals to develop and exercise their will in meaningful ways.
Nevertheless, participants also described experiences where enabling supports were in place. Respectful listening, flexibility to adjust daily routines, the use of visual aids, and participatory planning processes were identified as factors that strengthened self-determination. Even among participants requiring higher levels of support, autonomy could be meaningfully exercised when environments were adapted to their communicative and cognitive needs. These findings are consistent with recent work by Álvarez-Aguado et al. (2021, 2024) and Mumbardó-Adam et al. (2023), who demonstrate that, under appropriate conditions, older adults with intellectual disabilities can sustain and expand their self-determination capacities in community settings.
Finally, the findings reveal a strong link between self-determination and emotional well-being. Participants who could exercise choices, even in small matters, reported greater happiness, motivation, and a renewed sense of purpose. Decision-making not only had practical outcomes but also carried symbolic weight: it reaffirmed personal identity, strengthened agency, and facilitated positive future-oriented thinking. Conversely, participants who lacked opportunities for self-determination often described emotional withdrawal, reduced aspirations, and feelings of diminished personal worth. These results align with the conclusions of Belperio et al. (2024), Sexton et al. (2016) and Wehmeyer (2020) who argue that guaranteeing the right to decide is fundamental for ensuring dignified and meaningful aging.
Study limitations
Despite the richness and depth of the findings, this study has several limitations.
First, the sample was drawn exclusively from community settings in two Chilean regions (Metropolitan and Valparaíso), which may limit the transferability of the results to other regions or to different cultural contexts with distinct support systems. Future studies could expand geographically and culturally to enhance comparative analyses.
Second, although purposive sampling allowed the inclusion of diverse experiences, it does not permit generalization to the broader population of older adults with intellectual disabilities. Furthermore, individuals with more profound disabilities or communication barriers might have been underrepresented despite the use of accessible methods, which could bias the results toward more verbal or socially active participants.
Third, while the study foregrounded the direct voices of older adults, it did not systematically integrate the perspectives of family members, community support workers, or broader social networks. Including these actors could provide a more comprehensive and triangulated understanding of the facilitators and barriers to self-determination in community contexts.
Lastly, the cross-sectional design limits the ability to observe changes over time. Longitudinal approaches would be valuable to explore how self-determination evolves across different stages of aging and in response to environmental changes.
Practical implications and future research lines
The findings have important practical implications for community support systems, policy design, and professional practices aiming to foster autonomy and dignity among older adults with intellectual disabilities. As recent research indicates, the quality of contextual and relational environments plays a decisive role in predicting self-determination, often more than individual characteristics such as cognitive level or functional independence (Vicente et al., 2023).
At the policy level, it is fundamental to explicitly recognize self-determination as a core right in aging-related programs and to design services that actively promote decision-making opportunities across daily life areas. Flexibility in support structures, the creation of deliberative spaces, and the systematic incorporation of individuals’ voices into service planning are essential steps toward this goal.
This perspective is consistent with the Convention on the Rights of Persons with Disabilities (United Nations, 2006), which defines autonomy, participation, and self-determination as non-negotiable human rights that must be operationalized in policy frameworks for aging and disability.
Support organizations should prioritize relational environments based on trust, respect, and recognition of individual agency. This implies training support teams in human rights, accessible communication, supported decision-making, and person-centered planning. Attitudes of support staff are not neutral; they play a decisive role in either enabling or constraining personal agency.
As Thalen et al., 2023 highlight, emotional well-being, interpersonal relationships, and self-determination are central dimensions of quality aging among people with intellectual disabilities, underscoring the need for relational and communicative environments that promote choice and voice.
In terms of accessibility, it is necessary to implement and mainstream cognitive and communicative adaptations—such as easy-to-read materials, visual supports, and augmented communication strategies—to ensure that all individuals, regardless of their support needs, can understand options and express their preferences effectively.
These findings echo the recommendations of Álvarez‐Aguado et al., 2024, who stresses that self-determination in aging women with intellectual disabilities depends on communicative accessibility, flexible supports, and recognition of agency across daily contexts.
Future research should explore self-determination through longitudinal and comparative designs, considering the evolution of agency over time and differences across community-based living arrangements. It is also essential to include the perspectives of family members, support providers, and policymakers to capture the complex ecosystem that shapes self-determination processes.
Additionally, developing validated instruments to systematically assess the degree of self-determination in community living contexts could provide valuable tools for monitoring, evaluation, and continuous improvement of support practices.
Conclusions
The findings of this study affirm that self-determination is not a secondary issue nor a theoretical ideal; it is a fundamental human right that shapes the quality of life, emotional well-being, and dignity of older adults with intellectual disabilities. Creating daily opportunities for choice, ensuring communicative accessibility, and fostering relational trust are not ancillary strategies but essential conditions for dignified and meaningful aging.
However, significant barriers persist, linked to rigid routines, overprotection, communication barriers, and inconsistent support practices. Overcoming these challenges requires deliberate action at all levels—policy, organizational, and relational—to create environments where the will of individuals is recognized, respected, and sustained. Recent studies reinforce that such environments—characterized by flexible supports, participatory planning, and communicative accessibility—are decisive in sustaining agency and well-being in later life (Álvarez‐Aguado et al., 2024; Thalen et al., 2023; Vicente et al., 2023).
Ultimately, the right to decide does not diminish with aging or disability; rather, it becomes even more critical. As Wehmeyer (2020) and Araten-Bergman and Bigby (2024) argue, protecting the right to self-determination across the lifespan is both an ethical imperative and a structural condition for social justice. Guaranteeing this right is not only a matter of personal fulfilment but also a profound ethical obligation toward building inclusive, just, and humane societies.
Footnotes
Acknowledgments
Millennium Institute for Care Research (ICS2019_024).
Ethical Considerations
This study was approved (CEC_FE_2023006) by the Ethical-Scientific Committee of Universidad de las Américas, Chile.
Consent to Participate
All participants voluntarily signed an informed consent form before taking part in the study.
Funding
This work was supported by the Anid Fondecyt Iniciación under Grant 11230525.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to ethical supporting data is not available.