
Abstract
The aim of this study was to develop and validate the Maladaptive Stress Response Patterns Questionnaire (MSRP-Q), a new informant-based instrument for adults with intellectual disabilities in residential care. The MSRP-Q identifies seven maladaptive stress response patterns observable in daily life. The questionnaire consists of 34 items. Preliminary psychometric analyses (N = 80) showed sufficient to good internal consistency, with 76% of the items aligning with their intended subscales, but also indicate that the MSRP-Q is most suitable for individuals with mild-moderate intellectual disabilities. Construct validity was supported by moderate correlations between MSRP-Q scores and the scores on three instruments measuring childhood stressors, current stressful events, and chronic stressors. A weak but significant correlation was found with the Fear and Tension subscale of the ADESS. These findings suggest that the MSRP-Q may be a promising tool for the identification of person-specific stress response patterns.
Keywords
For individuals with intellectual disabilities, stress is a key factor in the development of mental health issues and behavioural problems (Esbensen and Benson, 2006a; Hamilton et al., 2005; Koritsas and Iacono, 2015; Reyes-Martín et al., 2022; Scott and Havercamp, 2014). They are frequently exposed to stressors both in daily life (Bramston et al., 1999; Hatton and Emerson, 2004; McMahon et al., 2019) and across the lifespan (Hulbert-Williams and Hastings, 2008; Mevissen et al., 2012; Vervoort-Schel et al., 2018), yet the impact of these stressors varies between individuals (Rouleaux et al., 2024).
The transdisciplinary stress model developed by Epel et al. (2018) offers a theoretical framework for understanding individual differences in responses to stressors. The model introduces the concept of maladaptive stress responses, which may develop into habitual response patterns shaped by a combination of factors, including genetics, developmental history, and cumulative exposure to stressors. The model integrates findings from epidemiological research, examining the life course and cumulative stress experiences, with findings from experimental research, focusing on acute stress responses. According to Epel et al. (2018), in most situations, individuals respond to stressors adaptively, meaning their response is well-matched to the demands of the situation and that the stress system returns to a homeostatic state once the stressor has passed. However, when exposed to acute or chronic stressors, stress responses can become maladaptive, characterised by an excessively strong or prolonged reaction (Juster et al., 2010; Lee et al., 2015). Maladaptive stress responses can develop into habitual patterns that may initially be context-dependent but, over time, evolve into more stable personal traits (Epel et al., 2018; McEwen, 1998). Investigating such patterns may help to explain individual variability in the mental health impact of stressor exposure.
Existing assessment tools mainly aim to assess either exposure to stressors or indicators of stress-related mental health problems (e.g. Hermans et al., 2008; Hermans and Evenhuis, 2008; Lunsky and Bramston, 2006), but not the stress response patterns through which individuals typically react to stress. Developing a reliable measure of these person-specific stress response patterns could contribute to a more precise understanding of how stress processes manifest in individuals with intellectual disabilities. Epel et al.’s (2018) transdisciplinary model has not yet been applied to individuals with intellectual disabilities. However, it has been widely cited across population and health sciences as a comprehensive framework for understanding stress processes (e.g. Pachankis and Clark, 2024; Vanderhasselt et al., 2025). To the best of our knowledge, no instruments have yet been developed or validated to conceptualise and measure maladaptive stress responses in individuals with intellectual disabilities.
This article presents the Maladaptive Stress Response Pattern Questionnaire (MSRP-Q), an assessment tool developed for health professionals to identify maladaptive stress response patterns based on observable behaviour patterns in individuals with intellectual disabilities. This article describes the development of the items and structure of the instrument and provides a preliminary analysis of its content and construct validity.
Experts in the field developed the questionnaire items to capture behaviours in individuals with intellectual disabilities, as observed by professional caregivers who interact with them daily. The items were constructed using the framework of seven maladaptive stress responses previously described by Epel et al. (2018). These responses are categorised into three groups; physiological responses (anticipation, reactivity, habituation, and recovery), cognitive responses (cognitive appraisal and perseverative cognition), and affective responses (affect contagion).
The first category, physiological responses, includes behavioural and physical responses to stressors. A stress response has four phases: anticipation, reactivity, habituation and recovery (Epel et al., 2018). Anticipation refers to the period before a stressor. Reactivity represents the peak of the stress response, while habituation describes the process by which the stress response decreases slightly during a prolonged stressful event. Recovery refers to the post-stress period, where the system attempts to return to a balanced state. Maladaptive stress responses in this domain include early initiation (anticipation), such as when a person exhibits heightened nervousness long before a medical appointment, excessively high peaks (reactivity), lack of habituation, or prolonged recovery.
The second category, cognitive responses, involves cognitive processes related to reacting to stressors. Cognitive appraisal is the process by which the brain evaluates whether a stressor is threatening, often influenced by core beliefs (Lazarus and Folkman, 1984). A maladaptive cognitive stress response occurs, for instance, when an individual perceives minor changes to a routine as highly threatening. Perseverative cognition refers to rumination, or the tendency to repeatedly think about a stressor even after it has passed, further prolonging the stress response (Epel et al., 2018).
The third category, affective responses, includes emotional processes such as affect contagion, where a person becomes stressed by observing another’s stress. For example, during an incident of aggression in the group home, an individual with intellectual disabilities may feel agitated simply by witnessing a staff member’s visible distress, even if they are not directly affected by the event (Waters et al., 2014, 2017).
According to Epel et al.’s (2018) stress model, maladaptive stress response patterns are primarily related to an individual’s historical exposure to stressors. Stressful experiences can accumulate over time and significantly influence the development of stress systems (Felitti et al., 1998; McEwen, 2003a; McLaughlin and Lambert, 2017; Nurius et al., 2015; Zeanah and Sonuga-Barke, 2016). Individuals with intellectual disabilities are known to encounter multiple stressors throughout life, both in childhood (Bowring et al., 2019; Hastings et al., 2013; Vervoort-Schel et al., 2018) and adulthood (Focht-New et al., 2008; Hermans and Evenhuis, 2012; Hulbert-Williams and Hastings, 2008; Mevissen et al., 2012; Murphy et al., 2007; Wigham et al., 2011).
Chronic stressors are also expected to be associated with maladaptive stress response patterns. Individuals with intellectual disabilities are often exposed to ongoing stressful conditions (Esbensen and Benson, 2006a; McMahon et al., 2019). Prolonged exposure to such stressors can lead to chronic stress, which alters the brain’s neural architecture for stress responses (Epel et al., 2018; Esbensen and Benson, 2006b).
Chronically activated stress systems and maladaptive stress response patterns have been associated with mental health problems such as anxiety and depression (Doan, 2021; Lee et al., 2015; McEwen, 1998, 2003a, 2003b). In individuals with intellectual disabilities, these problems have also been found to correlate positively with stress (Scott and Havercamp, 2014). Prevalence rates of anxiety and depression in people with intellectual disabilities range from 2% to 17% (Cooper et al., 2015; Reid et al., 2011; White et al., 2005).
The aim of this study was to develop and examine the content and construct validity of the MSRP-Q. Content validity was addressed through the theory-driven development of items and expert evaluation during the construction phase. Construct validity was examined through analysis of the scale structure using confirmatory factor analysis suitable for small samples (Stuive et al., 2008). Construct validity was further assessed by examining correlations between MSRP-Q scores and scores on questionnaires representing other variables within Epel et al.'s (2018) stress model, including childhood stressors, stressful events in adulthood, chronic stressors, and stress-related mental health problems, such as anxiety and depression. These correlations were used to determine whether the MSRP-Q captures a stress-related construct that is associated with, but conceptually distinct from, other components of the model. Demonstrating this distinction is essential for positioning the MSRP-Q within the broader framework of stress assessment tools.
The study addressed three key research questions: 1) What is the internal consistency of the MSRP-Q?; 2) Do the data show initial support for the proposed subscale structure of the MSRP-Q?; and 3) Do MSRP-Q scores correlate positively with scores on instruments measuring different variables within the stress model of Epel et al. (2018), including different types of stressors and problems in mental well-being?
Given that stress response patterns, as conceptualised in the transdisciplinary model by Epel et al. (2018), are shaped by multiple interacting influences, we expected no more than moderate positive correlations between MSRP-Q scores and measures of childhood stressors, stressful events in adulthood, chronic stressors, and stress-related mental health problems. Strong correlations would suggest insufficient differentiation between stress exposure and maladaptive stress responses as distinct constructs.
Method
Participants
A total of 80 individuals with intellectual disabilities took part in the study. Participants were recruited from four Dutch care organisations providing residential care for individuals with intellectual disabilities. These organisations offered similar types of care and supported individuals across all levels of intellectual disabilities. All participants were 18 years or older and lived in group homes. The average age was 41.20 years (range: 18–73); for eight participants, age was unknown. Of the 80 participants, 40 were male (50%), 38 were female (47.5%), and gender was unknown or undisclosed for two individuals (2.5%). Based on information in personal care files, 15 participants had mild intellectual disabilities, 20 had moderate intellectual disabilities, 21 had severe intellectual disabilities, and 10 had profound intellectual disabilities. Information regarding the level of intellectual disability was undisclosed for 14 participants.
Procedure
The participating care organisations randomly selected 66 residential group homes. The residents of the selected group homes received an informed consent form, which was sent either to the individual with intellectual disabilities or, in most cases, to their legal representative. In cases where the legal representative gave consent on behalf of the person with intellectual disabilities, this was done in accordance with Dutch legal guidelines for legal representation, and the request to participate in the study was discussed with the person themselves. An easy-to-read information letter, provided by the researchers, supported this process. When such a discussion was not possible due to limitations in communication or understanding, the legal representative ensured that the decision was in accordance with the person’s preferences. To minimise the burden on staff acting as informants, a maximum of two residents per group home were included in the study. If consent was obtained for more than two residents within a group home, a random selection was made. For each participating resident, two direct support workers who had been closely involved in their care for at least one year were invited to participate as informants. The questionnaires were administered by researchers in the form of interviews conducted via telephone or Microsoft Teams. This format allowed for more consistent and accurate ratings by ensuring clarification when needed. The researchers entered the responses directly into Qualtrics. The questionnaires were divided into two sets. One set contained the questionnaires for stressors and the MSRP-Q, and the other set contained questionnaires on problems in mental well-being. The reason for dividing the questionnaires in two sets was to limit spurious correlations (Hulbert-Williams et al., 2014). For this study, questionnaires were completed by direct support workers between April and October 2022. Ethical approval to conduct the study was obtained by the Ethics Committee of the Faculty of Social and Behavioural Sciences of Utrecht University (EC-22-0057).
Measures
Maladaptive stress response patterns
The MSRP-Q was originally developed by the second author following a three-phase procedure, including item pool generation, expert review for content validity, and item refinement through consensus (DeVellis, 2022). In the first step, the second author and two experienced professionals from a residential care organisation formed a working group. The second author presented the seven maladaptive stress response patterns described by Epel et al. (2018). The working group translated these theoretical patterns into recognisable and practically observable behavioural indicators reflecting how maladaptive stress responses manifest in the daily lives of adults with intellectual disabilities. All descriptions were newly constructed and not adapted from existing measures. Next, a broad group of university-trained professionals from the collaborating organisation, including behavioural scientists, psychologists, and educational specialists reviewed the behavioural descriptions for clarity and recognisability, particularly for use by carers in residential settings. Finally, the initial item pool was discussed by the first two authors and two additional researchers and refined through consensus. Redundant or overlapping items were removed, and the remaining statements were selected to ensure sufficient differentiation across the seven stress response domains while maintaining conceptual coverage and practical feasibility. A small pilot study conducted by master students provided preliminary feedback on item clarity and feasibility for direct support staff, which was incorporated into the final refinement step.
The resulting questionnaire (see Appendix A) consisting of 34 items was based on seven subscales, each representing a maladaptive stress response: Heightened Anticipation (HA, 5 items), Heightened Reactivity (HR, 6 items), Lack of Habituation (LH, 5 items), Prolonged Recovery (PR, 4 items), Cognitive Appraisals (CA, 4 items), Perseverative Cognitions (PC, 6 items), and Affect Contagion (AC, 4 items). Informants rated each item on a five-point Likert scale ranging from 'not at all true’ (0) to 'completely true’ (4). A Likert scale was chosen to capture nuanced responses reflecting the spectrum of maladaptive stress response patterns. Total scores on the questionnaire range from 0 to 136, with higher scores indicating more maladaptive stress response patterns. Scores can also be calculated for each subscale.
Childhood stressors
Stress experiences during childhood were measured by asking the informant firstly if there were any notes in the personal file of the individual with intellectual disabilities about stressful events during childhood. If the question was answered affirmative, the informant could choose the following events: fire, robbery, threatened or mistreated, a serious accident or injury, near drowning or suffocation, seeing someone die or being seriously injured, assaulted or raped, being in a hospital for more than a week, transferring to a crisis location due to mental health problems, transferring to a crisis location due to family overburden, and there was an option to fill in another type of event. The total score on childhood stressors indicated the number of stressful events in childhood an individual with intellectual disabilities experienced. Information on childhood stressors was obtained from existing files and informant reports, and because these data were based on available documentation, early life information may not have been complete.
Current stressful events
The Checklist Life Events (CLE) is a Dutch questionnaire for informants aimed to identify events that could potentially negatively affect the lives of individuals with intellectual disabilities (Hermans and Evenhuis, 2008). No precise data are known about reliability or validity, but the usability of the checklist has been demonstrated in at least one study in individuals with intellectual disabilities (Hermans and Evenhuis, 2012). This questionnaire lists 28 events that can negatively affect persons’ lives. An example is “structural change of staff in residential facility”. Informants were first asked whether any of these events had occurred in the past 12 months to the person with intellectual disabilities. If so, the informant was asked whether the individual with intellectual disabilities experienced a negative impact from it. Scores on the CLE can range between 0 and 28, with a higher score representing having experienced more life events.
Chronic stressors
Exposure to chronic stressors was measured with the Lifestress Inventory for informants (LI-inf.) (Lunsky and Bramston, 2006) designed to identify stressful life circumstances and potential stressful events. It was developed for informants of individuals with intellectual disabilities and has been extensively investigated for reliability and validity (Fogarty et al., 1997). The LI-inf. was translated into Dutch, following the guidelines from the paper by Beaton et al. (2000). For the present study internal reliability was acceptable (Cronbach’s α = .76). The questionnaire has three subscales: General worries, Negative interpersonal relations and Coping. The questionnaire contains 30 items. Seventeen items are positively formulated and were reverse scored for analysis. An example question of the subscale General worries is “Is he/she allowed to choose things that are important to him/her?”. On a 3-point Likert scale, the choices are yes, very much (2), sometimes or somewhat (1), or no, not at all (0). Scores can range from 0 to 60, with a higher score representing more life stress.
Anxiety, depression and mood
The Anxiety, Depression and Mood Scale (ADESS; Hermans et al., 2008) is a Dutch questionnaire for screening symptoms of anxiety and depression in individuals with intellectual disabilities, developed as a translation and adaptation of the ADAMS (Esbensen et al., 2003). The instrument is completed by proxy informants and consists of 28 items divided over four subscales: Depressive mood (13 items), Fear and tension (7 items), Social avoidance (7 items), and Other problems (11 items). The questionnaire contains 28 descriptions of behaviour such as “nervous or fidgety”. Each item is rated on a 4-point Likert scale ranging from 0 (=never/no problem) to 3 (=frequent/severe problem). A total score can also be computed, with higher scores indicating more problems.
The ADESS has demonstrated acceptable to good psychometric properties, including internal consistency, test-retest reliability, and interrater reliability (Hamers et al., 2019). However, its psychometric performance appears to be less robust in individuals with severe or profound intellectual disabilities Hermans et al. (2012). In the present study, internal consistency for the total scale was good (Cronbach’s α = .82).
Data analysis
Missing data occurred for 14 participants on background variables (age, gender, and level of intellectual functioning). These participants were included in the main analyses, except for the analyses involving background characteristics. One participant was excluded due to a missing MSRP-Q total score resulting in a total sample of 79. For another participant with one missing item on the MSRP-Q, item-mean imputation was applied (Patrician, 2002).
With N = 80 and α = .05 (one-tailed), a Fisher-z sensitivity check (Field, 2018) indicated approximately 80% power to detect correlations of r ≈ .28 in the hypothesised direction. Statistical power was therefore adequate for overall construct-level analyses but limited for subscale-level analyses and for detecting small effects.
To examine content validity, we first explored the psychometric properties of the MSRP-Q. Descriptive statistics (mean, SD, range) were calculated for each subscale and the total score, and normality of the total score was evaluated through visual inspection and distribution indices (Field, 2018).
To support the validity of the MSRP-Q across diverse populations, we examined whether total scores differed by gender and by level of intellectual functioning. For the latter, an independent-samples t-test was conducted comparing individuals with mild or moderate intellectual disabilities to those with severe or profound intellectual disabilities. Welch’s correction was applied when Levene’s test indicated unequal variances (p < .05).
Internal consistency was assessed using Cronbach’s α for each subscale and the total scale. Values above .80 were considered good, and values between .70 and .80 sufficient (Evers et al., 2013). Because all subscales consisted of fewer than 10 items, mean inter-item correlations were reported in addition to Cronbach’s α, as recommended by Pallant (2011). A range of .20 – .40 was considered desirable, <.10 insufficient, and >.50 indicative of redundancy (Briggs and Cheek, 1986).
To examine whether items of the MSRP-Q aligned with their intended subscales, we used the Oblique Multiple Group (OMG) method. This method was developed as a pragmatic alternative to conventional confirmatory factor analysis, particularly for use in small samples, and is described in Stuive et al. (2008) and elaborated in Stuive (2007), where a step-by-step procedure and worked example are provided. Unlike structural equation modelling techniques, the OMG method does not require strong distributional assumptions or large sample sizes, and it allows for the possibility that subscales may be conceptually related rather than statistically independent.
The procedure involved calculating item–subscale correlations for each item with all subscales, including its assigned one. Each correlation was first corrected for item overlap (“self-correction”) by correlating the item with the subscale score excluding that item, and subsequently for subscale length using Guilford’s change-factor formula (1954, p. 407), which adjusts correlations to a common base length. The average subscale length (4.86) was used as the base for this correction. An item was considered to align with its intended subscale if it showed the highest corrected correlation with that subscale. The proportion of items aligning with their intended subscales was used as a descriptive indicator of structural consistency (Nunnally and Bernstein, 1994; Stuive, 2007; Stuive et al., 2008).
Construct validity of the MSRP-Q was examined by correlating the MSRP-Q total score with the number of childhood stressors and with scores on the LI-inf., CLE, and ADESS domains. Because this is a preliminary, exploratory validation study, no multiplicity corrections (e.g., Bonferroni or FDR) were applied, which increases the risk of Type I error and should be considered when interpreting the findings. Directional, one-tailed tests were used, as positive associations between maladaptive stress responses and stress-related outcomes were expected based on Epel et al.’s (2018) model. All effects, particularly smaller ones, were interpreted with caution.
Data were analysed using IBM SPSS Statistics, Version 29.0.1.0 (IBM Corp., Armonk, NY, USA).
Results
Psychometric characteristics
Descriptive statistics
Means, standard deviations (SD), standard errors (SE), and ranges for the Maladaptive Stress Response Pattern Questionnaire (MSRP-Q) subscales and total score.
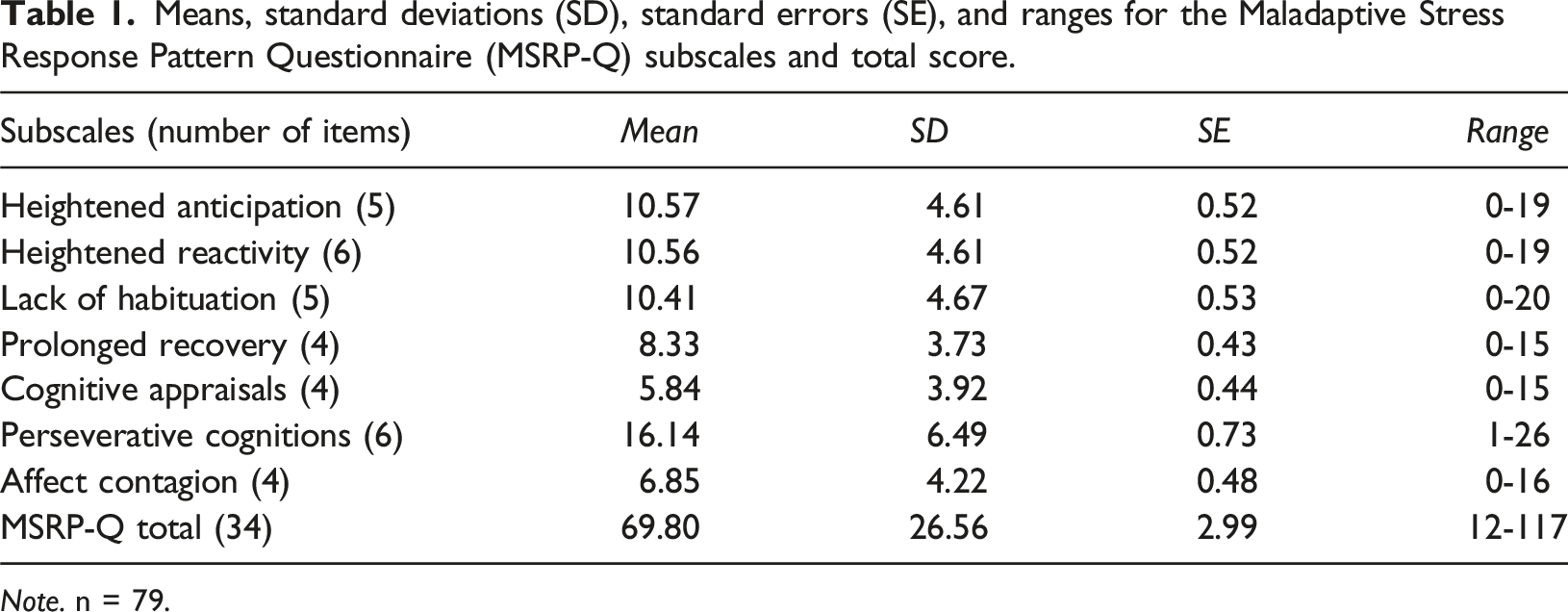
Note. n = 79.
Group differences
MSRP-Q scores among people with mild or moderate intellectual disabilities (M = 79.17, SD = 20.96) were significantly higher than those of people with severe or profound intellectual disabilities (M = 57.45, SD = 30.19), Welch’s t(52.62) = 3.35, p = .001. MSRP-Q scores did not significantly differ between men (M = 63.56, SD = 28.21) and women (M = 75.39, SD = 24.04), t(75) = −1.98, p = .052. There was no significant association between gender and level of intellectual disability, χ2(1, n = 66) = 1.60, p = .206.
Content validity
Internal consistency
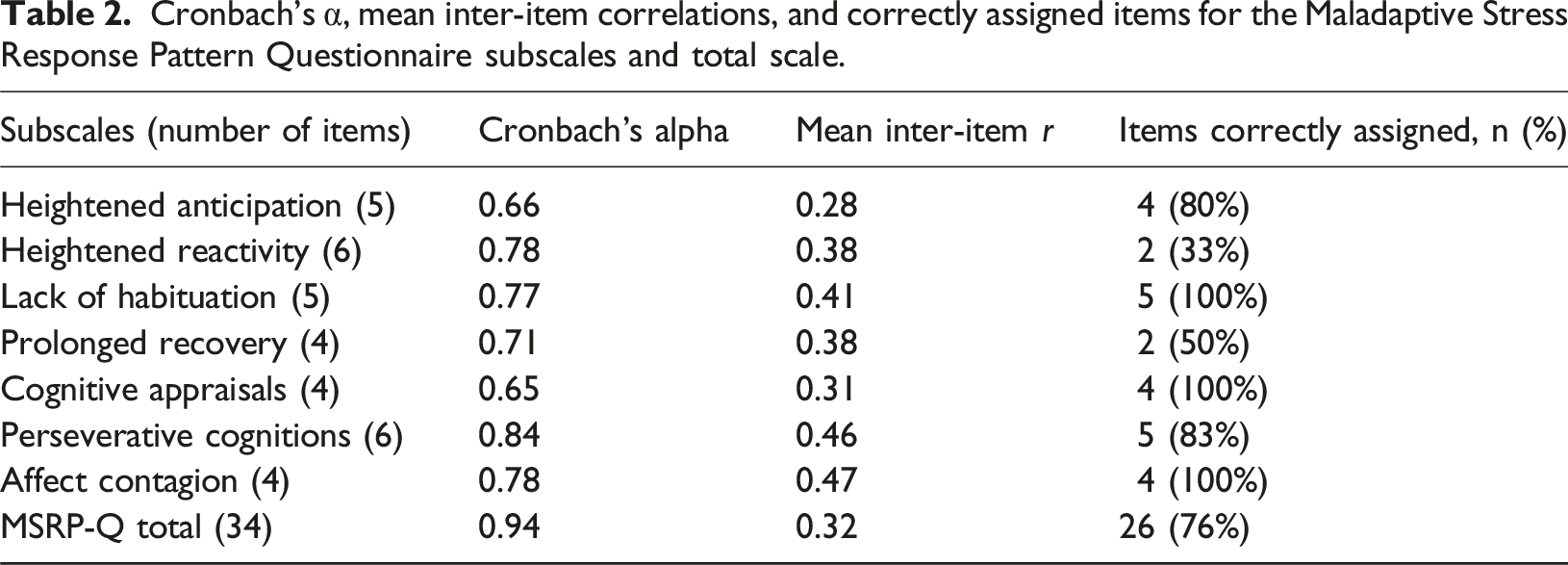
Cronbach’s α, mean inter-item correlations, and correctly assigned items for the Maladaptive Stress Response Pattern Questionnaire subscales and total scale.
Oblique Multiple Group method
The results obtained through the OMG method showed that 26 items (76%) were correctly assigned to their respective subscales (Table 2). Specifically, all items within the Lack of Habituation, Cognitive Appraisals, and Affect Contagion subscales were accurately assigned to their own subscale. Additionally, five out of the six items belonging to the Perseverative Cognitions subscale and four out of the five items belonging to the Heightened Anticipation subscale were correctly classified. However, the accuracy of assignment was less satisfactory for the subscales Heightened Reactivity and Prolonged Recovery.
Overall, these findings provided partial descriptive support for the proposed subscale structure. As the OMG method offers a descriptive verification of item–subscale associations, there are no formal thresholds for establishing statistical significance or definitive evaluation criteria.
Construct validity
Given the substantial intercorrelations between subscales and the partial support for the proposed subscale structure in the OMG analysis, the total score was retained as a single, conceptually coherent indicator of maladaptive stress responses. Moreover, the total MSRP-Q score demonstrated excellent internal consistency, thereby avoiding unnecessary multiple testing.
Correlation coefficients between total score on Maladaptive Stress Response Patterns-Questionnaire (MSRP-Q), number of childhood stressors, life events, chronic stressors and mental health problems.
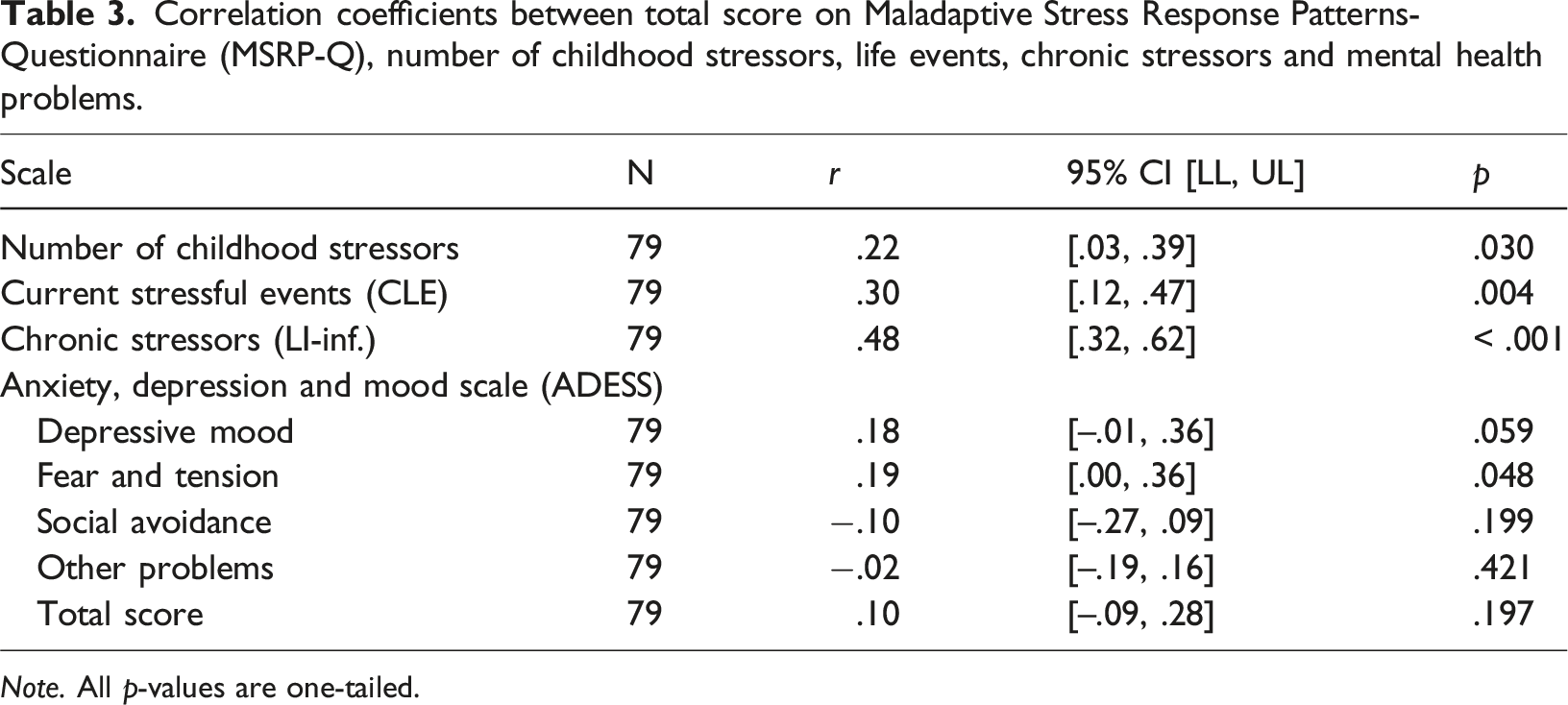
Note. All p-values are one-tailed.
Discussion
This study introduced the MSRP-Q, outlining the development of its items and subscales, and provided a preliminary evaluation of its content and construct validity. The MSRP-Q is a novel instrument designed to measure individual differences in the tendency to exhibit maladaptive stress response patterns among individuals with intellectual disabilities. It is hypothesised that a person’s vulnerability to stress is reflected in the way these maladaptive response patterns manifest in daily life.
The MSRP-Q consists of 34 items, divided across seven subscales. Results from the preliminary analysis demonstrated that the instrument shows sufficient to good internal consistency for both the total scale and its subscales. Most items (76%) were most strongly associated with their theoretically intended subscale. While these findings provide initial support for the proposed subscale structure, the results also indicate that some items may behave differently than intended. For some items, assignment to a different subscale may reflect conceptual ambiguity. For instance, the statement 'The person… tries to avoid tasks’ could indicate either a stress response to novelty (HR) or a cognitive appraisal of failure (CA).
It was found in this sample that individuals with mild to moderate intellectual disabilities scored higher on the MSRP-Q than those with severe to profound intellectual disabilities. This difference does not necessarily indicate that maladaptive stress response patterns are more prevalent in individuals with higher levels of functioning but may instead reflect the instrument’s greater sensitivity or applicability in this group. This may be explained by earlier studies (Bernheimer et al., 2006; Hulbert-Williams and Hastings, 2008; Vos et al., 2013), which suggest that stress responses in individuals with severe intellectual disabilities are more difficult to observe or report due to limited communicative and behavioural expression. These findings highlight the need to consider level of intellectual functioning when interpreting MSRP-Q scores, and to explore potential adaptations to improve item relevance and accessibility across different levels of functioning. Taken together, the present findings suggest that while the MSRP-Q was administered across the full range of intellectual disability, it currently functions most consistently among individuals with mild to moderate intellectual disabilities.
Furthermore, as expected, the findings revealed moderate and significant positive correlations between MSRP-Q scores and scores on measures assessing exposure to the three types of stressors defined in Epel et al.’s (2018) stress model: childhood stressors, stressful life events during adulthood, and chronic stressors. These results suggest that all types of stressors, including those experienced early in life, are associated with a heightened tendency to display maladaptive stress response patterns in daily life, which may indicate increased vulnerability to stress. The observed associations are consistent with the theoretical assumptions of the stress model (Epel et al., 2018) and supported by empirical studies demonstrating links between early and chronic stress exposure and maladaptive stress processing (Epel et al., 2018; Goddings et al., 2019; Koss and Gunnar, 2018; McLaughlin and Lambert, 2017). The proportion of participants with documented childhood stressors (62.5%) was lower than in comparable studies (Santoro et al., 2018; Vervoort-Schel et al., 2021), possibly reflecting underreporting due to reliance on informant reports and file information rather than life-history interviews.
Contrary to expectations, only one significant but weak correlation was found between maladaptive stress response patterns and mental health symptoms: namely the Fear and Tension subscale of the ADESS. Although statistically significant, this association was small, suggesting limited practical significance. No significant correlations were found with Depressive mood, Social avoidance, or Other problems. Given the limited sample size, small or non-significant correlations should be interpreted cautiously. One explanation may be that the current sample lacked sufficient power to detect such associations. However, it is also possible that maladaptive stress response patterns are not directly linked to mental health symptoms but exert their influence in interaction with other variables. For instance, affective relationships with supportive caregivers may buffer the psychological impact of maladaptive stress responses (Janssen et al., 2002). This highlights the need for further research examining potential moderators and mediators in the relationship between stress response patterns and emotional well-being in people with intellectual disabilities.
Overall, the content and construct validity of the MSRP-Q appear promising. The significant yet weak to moderate correlations between the total MSRP-Q score and the score on measures of stressors suggest that the instrument captures unique aspects of the stress process. This provides preliminary evidence that maladaptive stress response patterns may represent a transdiagnostic risk factor, a factor that contributes to multiple forms of psychopathology and comorbidity (Sauer-Zavala et al., 2017). Within Epel et al.’s (2018) transdisciplinary stress model, a wide range of risk factors is organised that influence the development of mental health problems. Maladaptive stress response patterns are regarded as one such risk factor, linking stressor exposure to mental health outcomes, and may help explain the heightened vulnerability to stress-related problems observed in individuals with intellectual disabilities. Further research is needed to test this hypothesis.
The MSRP-Q might be an addition to existing assessment tools that measure different aspects of stress, such as experiencing stressful events or exposure to stressors (Bramston et al., 1999; Hermans and Evenhuis, 2012). Other tools and methods also focus on the individual’s stress response, such as measuring physiological stress responses (e.g., heart rate variability), perceived stress through self-report, and behavioural observations by others (de Witte et al., 2021; Scott and Havercamp, 2018; Simons et al., 2021). However, the MSRP-Q focuses specifically on identifying individual differences in stress response patterns. This makes the MSRP-Q a unique addition to existing assessment tools.
Limitations and strengths
This study has several limitations. First, the sample size was relatively small in relation to the number of items and subscales, which constrained statistical power, particularly for subscale-level analyses, and reduced the generalisability of the results. The correlational analyses were exploratory and uncorrected for multiple testing, which increases the risk of Type I error. Consequently, the present findings should be viewed as preliminary indications of construct validity and replication in larger samples is warranted. Another limitation concerns the lack of a 'not applicable’ response option in the MSRP-Q. Some informants noted that certain behaviours could not be assessed in individuals with limited verbal and cognitive abilities. This may have affected the validity of the responses, particularly for people with severe or profound intellectual disabilities. Therefore, separate norms for individuals with lower levels of functioning, or even two different versions of the instrument, may be necessary (Flynn et al., 2017). Finally, because autism is often associated with emotional dysregulation and intolerance of change (e.g. Mazefsky et al., 2013), future studies could examine whether maladaptive stress response patterns manifest differently in individuals with autism.
Future research should also examine the inter-rater reliability of the MSRP-Q to ensure that it is robust to subjectivity in scoring. In addition, it would be valuable to investigate the temporal stability of maladaptive stress response patterns by testing test-retest reliability. Given that the MSRP-Q was administered in an interview-based format with structured response options, future studies should also assess whether the instrument produces comparable results when used as a self-administered questionnaire without interviewer involvement.
An important strength of this study is the theoretical basis of the MSRP-Q. The questionnaire was developed based on the interdisciplinary stress model of Epel et al. (2018), which provides a solid framework for understanding individual differences in stress responses. Although this is the first study to explicitly apply this model to individuals with intellectual disabilities, it offers a promising step toward extending its relevance to this population. Another strength is the data collection by independent informants. The use of two separate informants to complete the MSRP-Q and the questionnaires on stressors and mental health problems, respectively, minimised the likelihood of spurious correlations. This increased the reliability of the reported associations.
This study presents the MSRP-Q, a newly developed instrument for assessing individual differences in stress responses. Stress-related assessment tools remain underdeveloped for individuals with intellectual disabilities (de Witte et al., 2021; Scott and Havercamp, 2018). The MSRP-Q has the potential to become a valuable diagnostic tool in this field. By mapping maladaptive stress response patterns, it may help identify stress-related problems and clarify behavioural indicators of prolonged or unhealthy exposure to stressors. This could support more accurate diagnostic decision-making. For example, using the MSRP-Q can raise awareness among direct support workers, enabling them to relate the behaviour of individuals with intellectual disabilities to contextual stressors. This allows them to respond in a more sensitive and responsive manner, which can support stress regulation (Doodeman et al., 2023). In addition, the instrument may contribute to the development of individualised risk profiles, indicating which individuals are more vulnerable to the negative effects of stress. Such insights could enable professionals to design preventive interventions or make environmental adjustments to more effectively reduce stressors. For example: describing an individual with an intellectual disability in terms of their maladaptive stress response patterns rather than their problematic behaviour may help focus attention on their specific support needs. These may include a need for recovery time, reduced exposure to chronic stressors, or targeted support for developing stress regulation skills.
Further research is needed to understand whether, and in what ways, maladaptive stress response patterns can be influenced by changes in the living environment or through therapeutic interventions.
At a scientific level, the MSRP-Q offers a new perspective by defining maladaptive stress response patterns as a transdiagnostic factor. This concept can be further explored in relation to other stress-related factors, such as coping strategies and biological markers, to gain a more complete insight into the functioning of stress systems in individuals with intellectual disabilities. Future studies should also examine whether maladaptive stress response patterns manifest similarly across countries, as the MSRP-Q items are grounded in observations from Dutch residential care settings, which may differ from those in other countries (Hatton et al., 2022).
This preliminary study offers promising indications that the MSRP-Q may be a valid and reliable instrument for identifying maladaptive stress response patterns in individuals with intellectual disabilities.
Footnotes
Acknowledgments
We would like to express our gratitude for support during the research to: Dr. Peter Vriesema, Zozijn, Dr. Vanessa Olivier-Pijpers, Ipse de Bruggen. Dr. Eline Roelofsen, Kennisplatform EVB plus.
Ethical approval
Ethical approval to conduct the study was obtained by the Ethics Committee (FETC) of the Faculty of Social and Behavioural Sciences of Utrecht University (EC- 22-0057).
Consent to participate
Participants, or their legal representatives where applicable, received written information about the study, including details on data handling. Informed consent was obtained from participants or their legal representatives. Informants who completed the questionnaire also received study information and provided informed consent.
Author Contribution
Matthijs Heijstek served as the principal investigator and was responsible for data collection, conducting the analyses, and drafting the manuscript. Lex Wijnroks supervised the study, contributed to the development of the research design, and provided critical feedback throughout the research process and the preparation of the manuscript. Agnes M. Willemen contributed to the development of the plan of analysis and supported the conduct and reporting of the statistical analyses. She also contributed to the review and revision of the manuscript. Marian J. Jongmans was responsible for the overall supervision of the research project and provided strategic guidance throughout the development of the study and the preparation of the manuscript. All authors contributed to the manuscript and approved the final version.
Funding
The first author was supported by Zozijn through dedicated research time to conduct this study at Utrecht University.
Declaration of conflicting interests
The authors declare no conflicts of interest.
Data Availability Statement
The data that support the findings of this study are not publicly available due to agreements with the client councils of the participating care organisations.
Appendix
Maladaptive Stress Response Pattern Questionnaire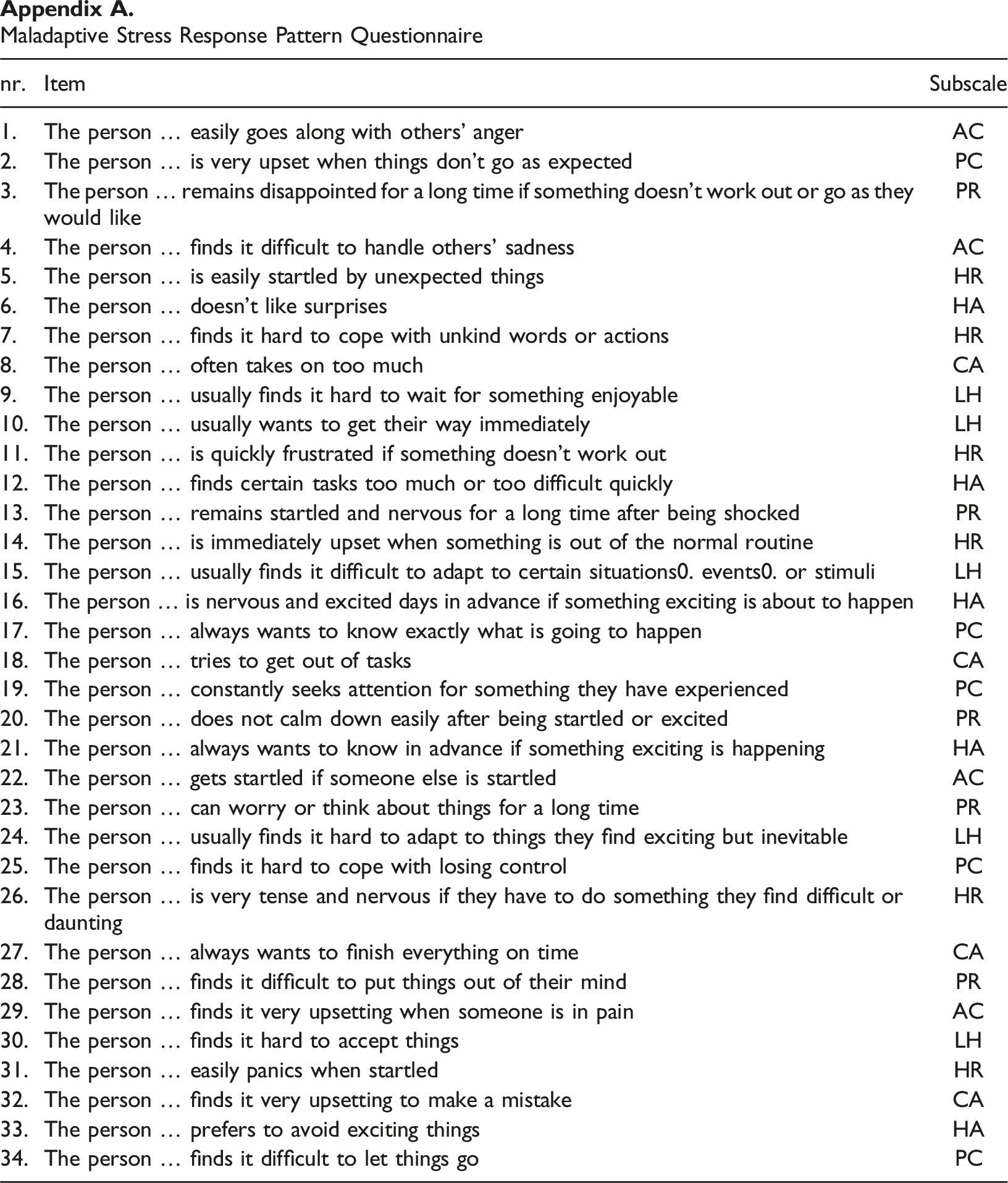
nr.
Item
Subscale
1.
The person … easily goes along with others’ anger
AC
2.
The person … is very upset when things don’t go as expected
PC
3.
The person … remains disappointed for a long time if something doesn’t work out or go as they would like
PR
4.
The person … finds it difficult to handle others’ sadness
AC
5.
The person … is easily startled by unexpected things
HR
6.
The person … doesn’t like surprises
HA
7.
The person … finds it hard to cope with unkind words or actions
HR
8.
The person … often takes on too much
CA
9.
The person … usually finds it hard to wait for something enjoyable
LH
10.
The person … usually wants to get their way immediately
LH
11.
The person … is quickly frustrated if something doesn’t work out
HR
12.
The person … finds certain tasks too much or too difficult quickly
HA
13.
The person … remains startled and nervous for a long time after being shocked
PR
14.
The person … is immediately upset when something is out of the normal routine
HR
15.
The person … usually finds it difficult to adapt to certain situations0. events0. or stimuli
LH
16.
The person … is nervous and excited days in advance if something exciting is about to happen
HA
17.
The person … always wants to know exactly what is going to happen
PC
18.
The person … tries to get out of tasks
CA
19.
The person … constantly seeks attention for something they have experienced
PC
20.
The person … does not calm down easily after being startled or excited
PR
21.
The person … always wants to know in advance if something exciting is happening
HA
22.
The person … gets startled if someone else is startled
AC
23.
The person … can worry or think about things for a long time
PR
24.
The person … usually finds it hard to adapt to things they find exciting but inevitable
LH
25.
The person … finds it hard to cope with losing control
PC
26.
The person … is very tense and nervous if they have to do something they find difficult or daunting
HR
27.
The person … always wants to finish everything on time
CA
28.
The person … finds it difficult to put things out of their mind
PR
29.
The person … finds it very upsetting when someone is in pain
AC
30.
The person … finds it hard to accept things
LH
31.
The person … easily panics when startled
HR
32.
The person … finds it very upsetting to make a mistake
CA
33.
The person … prefers to avoid exciting things
HA
34.
The person … finds it difficult to let things go
PC