
Abstract
This paper developed from discussions about the possible implementation and trial of an Australian maternal and early childhood sustained home visiting programme (MECSH), into a United Kingdom (UK) context. There are many similarities in services in the two countries, but some differences. To summarise and illustrate the complex and interconnected way that early years and preventive health services are specified, a diagram was developed, which provides a framework for this paper. The paper describes a health visiting service that encompasses universal, indicated and selective forms of prevention, with some embedded evidence-based programmes, forming part of a proactive and preventive service that is, itself, embedded within a wider resource system. Policy-driven terms derived from the English Health Visitor Implementation Plan have been used, but translated into the generic language of prevention (universal, indicated and selective), as a basis for future research. The place for different types of practitioner and needs of families with different levels of personal capacity or resource are also considered.
Increased understanding about how social determinants affect the whole population across a gradient has drawn attention to the need for more universal prevention, to tackle health inequalities. The components of successful early intervention programmes are well established, but more information is needed to support universal preventive services, which are delivered in a way that is proportionate to need. This paper, including the diagram that summarises its contents, is presented to stimulate discussion as well as guide future research and service development.
Keywords
Background
This paper developed from research discussions concerning the possible implementation and trial, in England, of a recently developed ‘maternal and early childhood sustained home visiting’ (MECSH) programme from Sydney, Australia (Kemp et al., 2011). Early childhood services in the two countries are similar in many respects, but there are some key differences.
Health visitors provide a broad-based child and family public health service, traditionally described as generic, proactive and universal (Council for the Education and Training of Health Visitors, 1977). Recently, political autonomy and devolution across the United Kingdom (UK) has been associated with increasing differences in the way health visiting is provided in each of the constituent four countries (Hoskins, 2009). This paper is about England, where there was a 20% fall in the number of health visitors employed between 2000 and 2010, from 10,046 to 8,125 full time equivalents (NHS Information Centre for Health and Social Care, 2011), being approximately 1 health visitor per 7,500 population, or 1 per 85 new births per year. The reduced workforce has inevitably affected the way that staff are deployed, including an increase in ‘skill mix’ staff working in teams led by health visitors, and use of local community provision, like Sure Start Children’s Centres and various early years services, which have increased in areas of deprivation (Audit Commission, 2010).
In Australia in the same period, child and family health services shifted from a clinic-based service to provision of at least one home-based postnatal visit followed by home and/or clinic-based visits, in recognition that more vulnerable families were not using well-baby clinics and more proactive engagement with families was needed. There was a 30% decrease in the number of child and family health nurses from 6,823 in 2003 to 4,686 in 2008 (Australian Institute of Health and Welfare 2005, 2010), despite the birth rate increasing by 16% in that time.
Two important concerns in both Australia and England are the perceived need to ensure a sound evidence base for practice and the focus on health inequalities. A third area, which is not the main focus of this paper, concerns how best to raise the skills of the existing workforce. However, an emerging area of discussion, which this paper aims to stimulate, concerns the relative emphasis placed on either implementing discrete programmes or developing services, as alternative mechanisms for achieving progress towards these goals. The term ‘programme’ is synonymous with an agenda, plan or schedule, and is particularly associated with the evidence-based practice movement. The phrase ‘manualised programme’ is sometimes used to emphasise the prior planning and prescription of activities, or the term ‘curriculum’ may describe embedded work packages, particularly in health education programmes. It is used here to mean manualised clinical approaches that specify a detailed and systemised set of intervention methods and activities used to address the needs of a specified target population. Such programmes will usually have been subject to rigorous testing through research trials.
Reference to ‘service’, on the other hand, infers provision or benefit. Dictionary definitions explain that a service is work done for somebody else, which may involve a helpful action or providing something for community. In particular, health services, as used in this paper, are organisational components funded to provide a range of health care functions to a defined population. The functions undertaken by a service will reflect the needs of the population to which it is targeted, which may be defined by a combination of characteristics such as age, condition and geography. Service descriptions encompass the entire infrastructure as well as the component parts, which may incorporate delivery of one or more programmes, care pathways or packages. Services are, therefore, broader but less specific than programmes; programmes may be one part of a service.
The debate raised in this paper is not about whether both programmes and services are necessary, which is widely agreed, but reflects some divergent views about whether they should be separate or joint activities, and whether or how one approach should lead or replace the other, as illustrated by different approaches adopted in England and Australia.
In England, there have been three distinct initiatives. First, a preventive programme for families with significant and potentially complex needs (Nurse Family Partnership, Olds, 2006) has been implemented under the title ‘Family Nurse Partnership (FNP)’, and there is increasing emphasis on identifying similarly robust programmes across the early years (Allen, 2011). In a second, separate development, government promises to increase the number of health visitors have been accompanied by clearer descriptions about how the universal health visiting service should be developed (Department of Health, 2011a, b). These two initiatives are intended to be complementary, and the ‘Healthy Child Programme’ (Department of Health, 2009) provides national guidance about how the different elements are supposed to fit together. However, these initiatives were implemented at different times, and are funded and managed differently. There is a substantial national package of support for the FNP, which has been implemented as a distinct project and programme, separate from the universal health visiting service and Healthy Child Programme, which are both locally funded and controlled.
The Nurse Family Partnership (Olds, 2006) has also been implemented as a distinct project for some sections of the population in Australia. There have also been new programmes of maternal and early childhood sustained home visiting (e.g. MECSH in New South Wales and Family Home Visiting in South Australia). In contrast to the English situation, these programmes were developed with a specific commitment to enabling development of the universal service delivered by child and family health nurses, as a single, integrated endeavour (Kemp and Harris, 2011).
Throughout the developed world, numerous programmes, funding streams and professional levels, interact in complex ways. This creates a need for greater clarity about how the different elements and options fit together, in order to promote effective ways of working or evaluating the impact of services and programmes on equity. This paper is presented in four parts, which aim to unravel and explain some of that complexity, both to stimulate discussion and provide a framework for future service planning and research.
First, the paper will explain how health inequalities follow a gradient across the whole population, and why early childhood provision is so important for equity. Second, it will explain the value and importance of universal provision across the whole population and why this is needed, in addition to selective prevention programmes that target families with specific risk factors, or programmes directed at populations or communities with concentrations of at-risk families. Third, it will explain the concepts of universal and indicated prevention, before finally exploring where and how professional skills are best directed in complex service settings. The diagram shown in Figure 1 was developed to help explain and conceptualise the different levels of prevention and need, and various forms of service response across a range of provision, and it will be referred to throughout the paper.
Matching programmes and services to family resource/capacity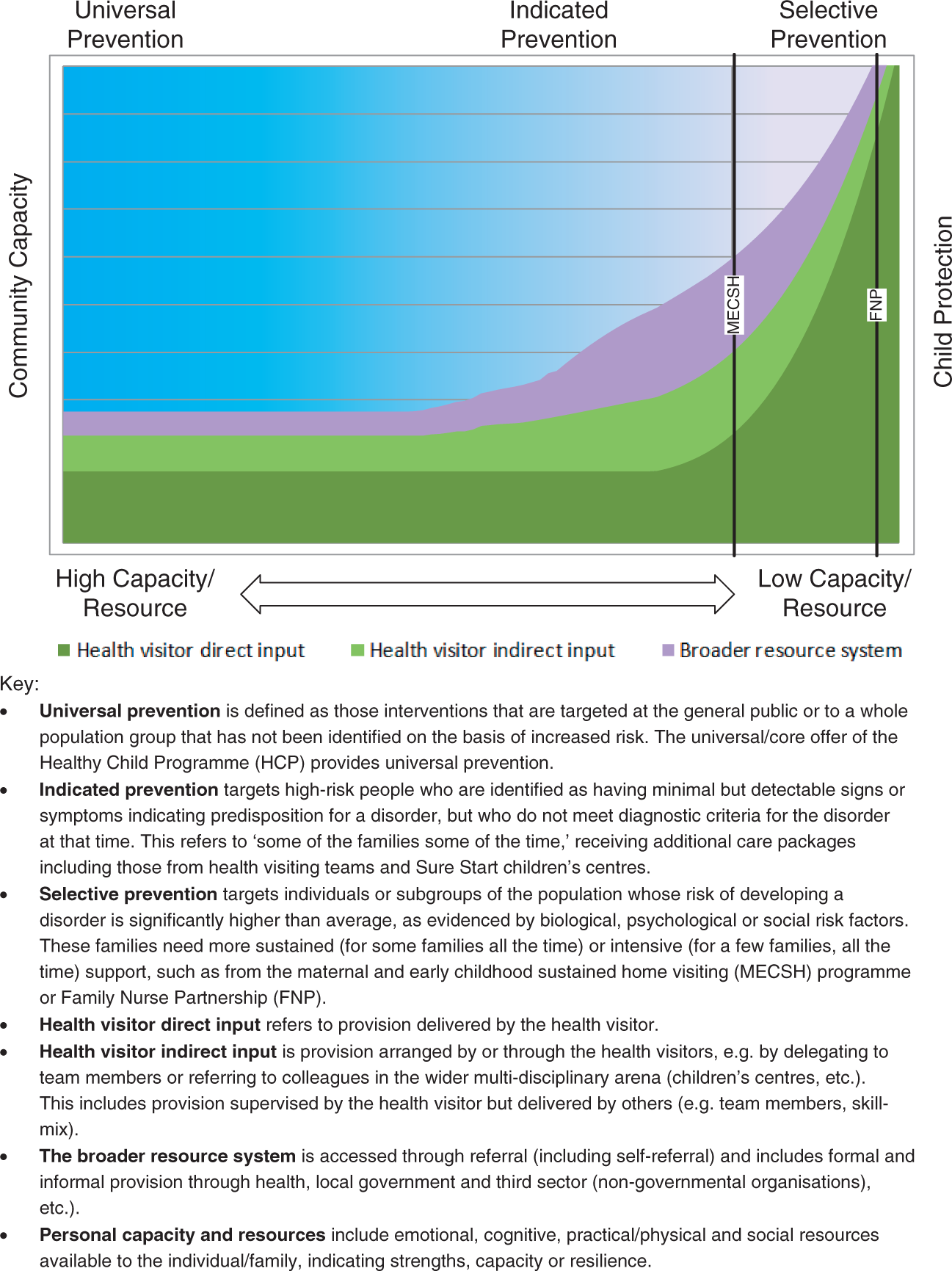
Health inequalities
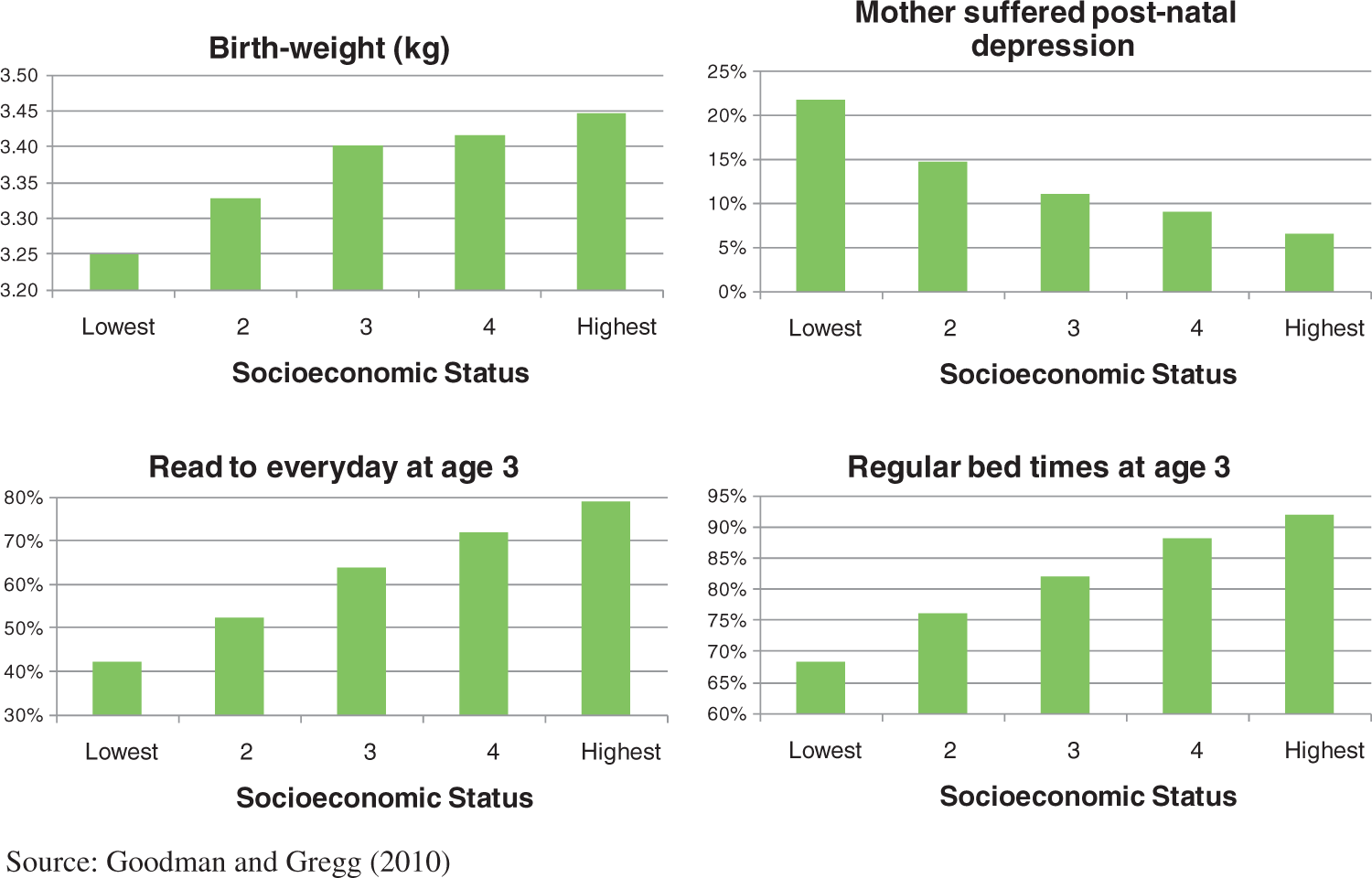
Evidence presented to the World Health Organization’s (WHO’s) Commission on the Social Determinants of Health (CSDH, 2008) showed how health inequalities, both within and between countries, affect the way people live, their consequent chance of illness, and their risk of premature death. England and Australia are both resource-rich countries, but children’s life chances are still significantly affected by their social situation at birth. It is particularly clear in these better-off parts of the world that health inequalities affect the whole social gradient, from the worst off to the best off. The Strategic Review into Health Inequalities in England (Marmot, 2010) identified examples to illustrate this gradient. Figure 2 shows deaths that would be avoided among infants born in England and Wales in 2005–6, if they all had the same chance of survival as those in the highest quintile (Oakley et al., 2009). Infants in the worst off 20% are most likely to be affected, but the gradient runs from bottom to top. The gradient is equally clear in factors affecting child development, shown in Figure 3, like birth weight, maternal post-natal depression, child being read to every day, and having regular bedtimes (Goodman and Gregg, 2010). The differences are most stark between the top and the bottom, but they run through the whole population, so that each socioeconomic step, up or down, affects the child’s life chances. Focusing only on the very worst-off will not achieve the major change in health inequalities that is needed.
Avoidable infant deaths. Estimated number of infant deaths that would be avoided if all quintiles had the same level of mortality as the least deprived, 2005–6 Factors affecting child development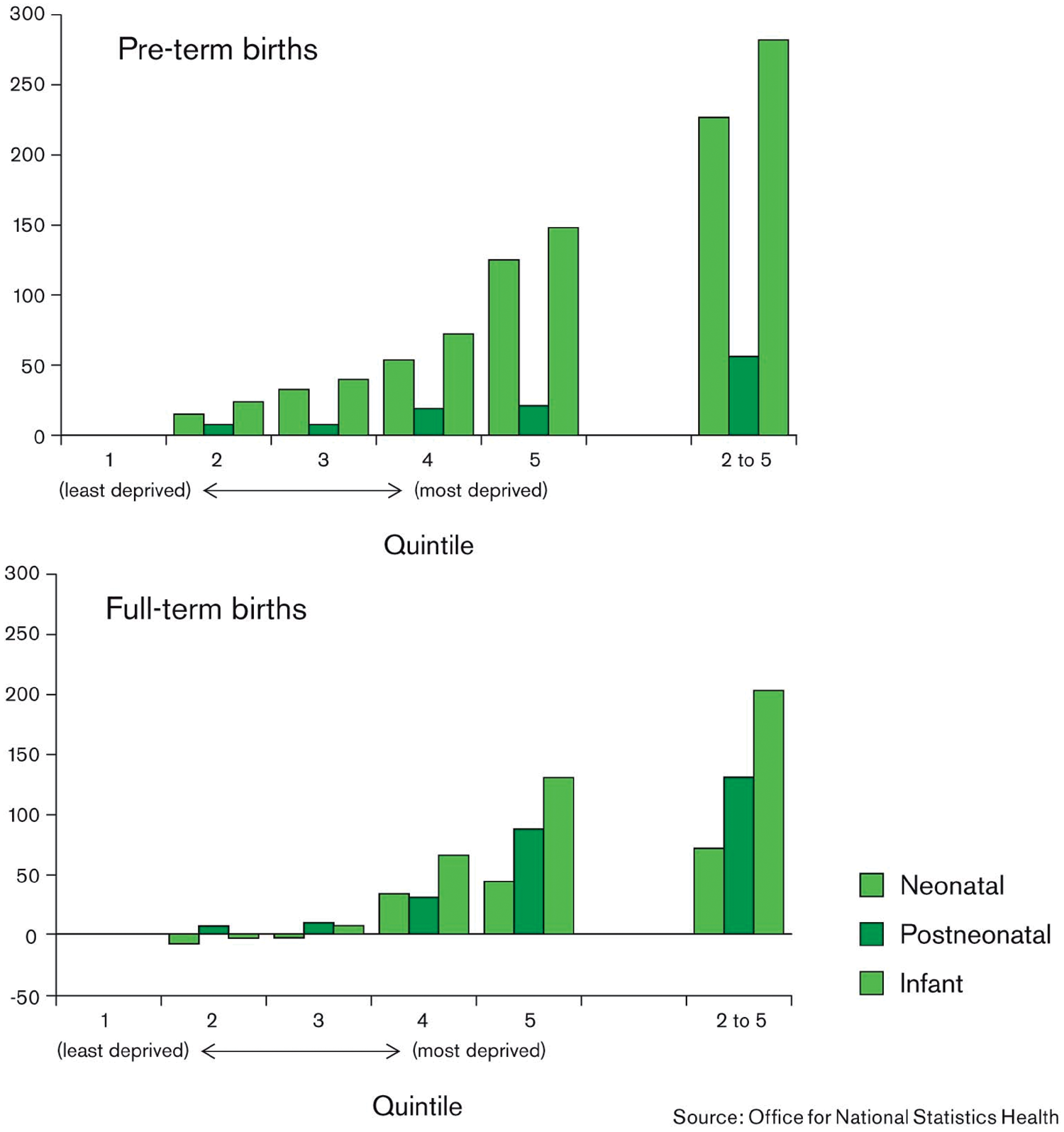
Figures 2 and 3 highlight a range of tangible issues and risk factors, which are important for needs assessment and for targeting, but their negative focus can distract from people’s individual strengths and the many resources upon which families can call. These resources are less clearly mapped, poorly defined, and measured far less often than problems, but they may also follow a gradient, as indicated by shading in Figure 1, which places families with the highest capacity at one end of a continuum, and those with the lowest at the other. In practice, the immediate and long-term impact of risk or resilience factors, as well as their interaction, are complex and difficult to predict. Factors intrinsic to the child and in their immediate environment, particularly their parents or carers, are likely to have the most significant affect on child outcomes. The sum impact of significant social risk factors may be ameliorated by child characteristics and the care and nurture they receive from their parents and carers. Further, practice that builds on people’s strengths is demonstrably more effective than approaches that emphasise problems, risks and the expertise of professionals (Macleod and Nelson, 2000; Davis and Day, 2010).
The interplay of resources and risks operates across communities as well as families, including the wider political scene that is so influential in terms of the social determinants of health, and across the life course. At each stage in life, the cumulative effect of those differences will be added to advantage or disadvantage from earlier years, so Marmot (2010) recommends taking a life course approach to addressing health inequalities. He draws on economic and scientific evidence to support his view that the early years should be both a starting point and the highest priority for action. Accumulated knowledge about the components needed for programme effectiveness (Harvard University Center on the Developing Child, 2007) has led to the current prevailing emphasis on selective prevention.
Selective prevention
Programmes designed for selective prevention target individuals or subgroups of the population whose risk of developing a disorder is significantly higher than average, as evidenced by biological, psychological or social risk factors (Gordon, 1983; WHO, 2004). FNP is an exemplar for selective prevention in the field of early childhood and parenting. It is an intensive home visiting programme that targets socially disadvantaged, first-time mothers and has been shown through a series of research trials to have consistently positive effects on a range of child and family outcomes (Olds, 2006). It has been implemented in England since 2007, in response to evidence that children born into the most significantly disadvantaged families are also most likely to experience multiple problems by the time they are 15 years old (HM Government, 2006). The FNP has the potential to break this cycle of disadvantage, and economic evidence shows the heavy initial investment would be far outweighed by later anticipated savings. However, there is lack of consensus or clarity about how generic services should be organised, so this paper explains some potential challenges associated with an uninformed expansion of elements of the FNP, or any other evidence based selective programme.
First, there is a tendency towards what might be called ‘mission creep’, that is, variations that develop despite recognition that fidelity to the programme is essential. Fixsen et al. (2005, page 35) warn against ‘the paradox of non-evidence-based implementation of evidence-based programs’ and the temptation to inappropriately adapt programmes in ways that potentially eliminate features that made it effective in the first place (Hemmelgarn et al., 2005). For example, a programme that is clearly effective for one group (in the case of FNP, single, first-time teenage mothers who present early in pregnancy) cannot be expected to work with other groups, such as older or multiparous mothers, those in better off situations, or with different needs, perhaps arising from mental health problems or substance misuse. Health visitors serve a large universal population base, who do not fit neatly into highly specified, narrow inclusion criteria, so a different approach is needed (Fixsen et al., 2005; Hohmann and Shear, 2002).
A medical analogy may help to explain why some adaptations are a violation of the programme. Diagnoses differ in type as well as severity: pneumonia is not a ‘bad cold’, so would not be treated as such. Someone with a cold would not be treated with a dilute form of the antibiotics used for pneumonia, nor would they work for influenza. The spread of infections is prevented through immunisation, not by treating with dilute medications designed to treat the disease. Clear distinctions apply across social and child developmental needs, which also differ in type as well as intensity, and all require specific responses tailored to their particular situation, just as different prescriptions are needed to treat or prevent different illnesses. So, an early childhood programme designed for one target population should be used only for that group. If different delivery methods, approaches or target groups are deemed important, they need testing through research, as with any other new programme.
The diversity and spread of need is the second challenge for specific, selective prevention programmes, which each have a particular focus or target group in mind. The FNP has proven effectiveness for an important but small proportion (possibly 2%, as shown in Figure 1) of the wider population of mothers and infants. However, whilst it hits this one significant target, it misses many others. A review of psychosocial risk factors identified antenatally in South West Sydney (Matthey et al., 2004) showed a high prevalence of potential problems (24.4% have had a recent major stressor, 19.3% have a mental health issue of concern, 5.2% experience family violence, 12.7% were at risk of depression). Overall, however, 40% of mothers had one or more risks for depression or poor coping postnatally. Providing a selective programme designed to help with any single one of these issues would be good for the affected mothers and children, but it would not shift the population curve for all families with vulnerabilities, nor change the whole picture of health inequalities for children.
Population paradox
Furthermore, health needs are distributed throughout the population, not just in selected groups. The majority of ‘cases’ are likely to be found outside the selected groups or areas, because of the greater numbers in the general population (Rose, 2008). This is sometimes known as the ‘population paradox’, which can be illustrated using an analysis carried out by the British Government’s Social Exclusion Task Force.
The Task Force identified seven key ‘family disadvantage indicators’ from the ‘Families at Risk’ review and mapped their distribution among children followed through the Millenium Cohort Study (Social Exclusion Task Force, 2007) (Figure 4). They noted that adverse child outcomes increased in line with an increasing number of indicators in a family. Indeed, the presence of just one or two of the factors at birth was associated with later adverse outcomes. They mapped the indicators to areas of disadvantage according to the (then current) Index of Multiple Deprivation (IMD) (Communities and Local Government, 2004), showing the anticipated gradient. Families with more than three or more than five indicators are concentrated in the worst-off areas, whilst those with none appear far more frequently at the better-off end (Figure 4a).
Population Paradox illustrated using number of children living with ‘family disadvantage indicators’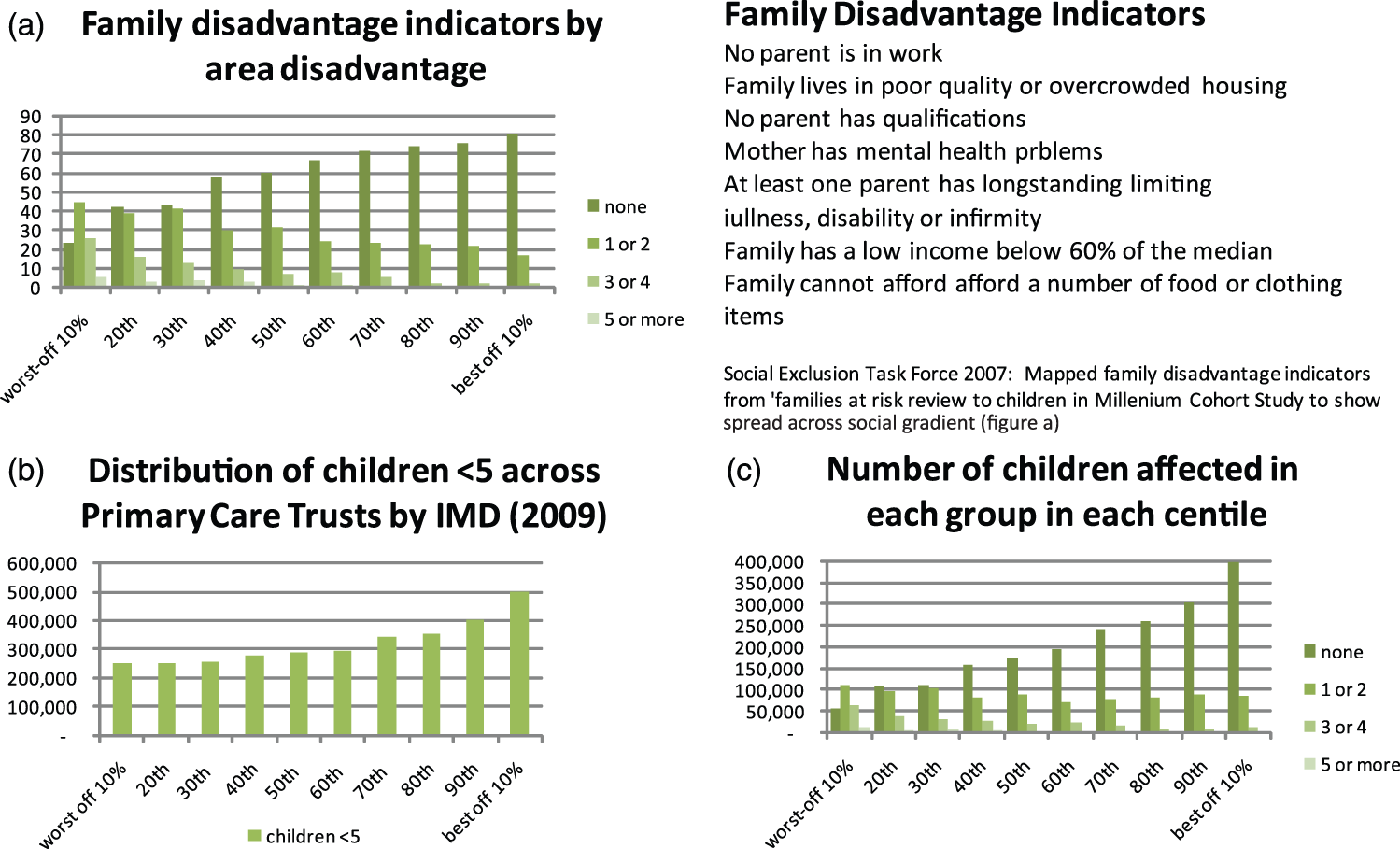
Mapping where pre-school children live produces a gradient going in the opposite direction, since far more children live in areas of relative affluence (Figure 4b). These figures are illustrative rather than exact, because the figures were derived from Primary Care Trusts (PCTs), which cover populations of 150,000–500,000 and encompass wide areas each including relative wealth and poverty. Even so, the figures give an idea of what happens when the data from Figure 4a are presented using headcount numbers rather than percentages, as in Figure 4c. This shows that, although many children living with family disadvantage indicators are concentrated in the most deprived 10% of areas, the actual number there is far exceeded by children living in the remaining 90% of areas.
Despite the approximate nature of such figures, they clearly illustrate the point that focusing exclusively on the extreme end of the gradient will only reach a small proportion of those in need, so health inequities will remain. Similar patterns of distribution occur, regardless of the actual nature of need or problem. Rose (2008) uses serum cholesterol levels and risk of heart disease to show that ‘a large number of people at small risk may give rise to more cases of disease than a small number of people at high risk, and such groups make up a relatively small proportion of the population’ (Rose 2008, page 59). To shift the curve of health inequalities and reduce overall prevalence, it is necessary to influence the whole population rather than focusing only on the areas or groups where there is the highest concentration.
Programmes and services
To achieve the desired reduction in health inequalities across the population, Marmot (2010, page 22) calls for a ‘second revolution in the early years:’ to increase the proportion of overall expenditure allocated for this age group, and to focus attention proportionately across the social gradient to ensure effective support to all new parents. This means grappling with how services are best delivered, which includes selective programmes, but encompasses a broader remit, including universal and indicated prevention, as indicated in Figure 1.
The MECSH programme, which was trialled in a deprived suburb of Sydney, aims to ‘shift the curve’ by targeting the worst-off 20%, including multiparous women, not just first-time mothers. As shown in Figure 1, this brings a sustained home visiting programme to a far larger and more heterogeneous group than that targeted by the Olds (2006) nurse–family partnership programme, and results of the initial trial were equally impressive (Kemp et al., 2011). MECSH was designed to capitalise on what is known about successful home visiting programmes (Macleod and Nelson, 2000; Harvard University Centre for the Developing Child, 2007), allowing sufficient intensity and duration (from pregnancy until the child is 2 years old), and focusing on parent and child. To encompass the range of needs encountered, it is broad based and multi-faceted, and also aims to exploit and integrate with any resources available in the wider community (Kemp and Harris, 2011). As well as home visiting, the programme includes group activities for MECSH families, and encourages engagement with and referral to other services, assisting and facilitating the transition of families as their involvement in the MECSH programme comes to an end. Also, MECSH was explicitly designed to support and develop the existing, generic service, making use of the highly skilled child and family health nurses, who are all trained in strengths-based practice using the ‘Family Partnership Model’ (FPM) (Davis and Day, 2010).
Health visitor direct input
Planning a universal preventive service (rather than a programme, or defined package of care) raises questions about who should deliver and receive it, what should be provided and how to conceptualise its purpose. There is a large literature about ‘universal health care’, which concentrates on social health protection, finance and insurance, drawing attention to the need for full financial support for health services. The World Health Assembly defined universal coverage as ‘access to key promotive, preventive, curative and rehabilitative health interventions for all at an affordable cost, thereby achieving equity in access’ (WHO 2005, para. 2). The universal health visiting service is supposed to provide promotive and preventive health interventions for all expectant mothers and those with pre-school children, following government guidance outlined in the ‘Healthy Child Programme’ (Department of Health, 2009).
Much of this universal provision requires ‘health visitor direct input’, as shown in Figure 1, because a high level of skill, such as that expected from a qualified health visitor, is needed to deliver it. This workforce needs to be equipped with models of practice, programme content and systems of implementation, as well as the necessary skills and ability to manage a largely undifferentiated caseload, to carry out a full health needs assessment of the infant, child and whole family, and the means to mobilise other forms of help or support. Where families have a high personal capacity or resource, the qualified health visitor is needed for one of two reasons. First, there may be a particular issue such as an acute breast-feeding problem, or behavioural or feeding advice, which will often be assessed and dealt with in a single contact – described as providing for ‘some families, some of the time’ (Department of Health, 2011b). Second, in some cases, contacts are so infrequent over the period of the child’s pre-school years that a full assessment is required at each meeting. This layer of direct health visitor input provides coverage of the whole population, which enables delivery of universal promotive and preventive services to all, with a greater frequency of contact where the need is higher (in individual families) or more prevalent (in the area/caseload).
Universal prevention
‘Universal prevention’ is defined as those interventions that are targeted at the general public or to a whole population group which has not been identified on the basis of increased risk (Gordon, 1983; WHO, 2004). The new service vision for health visiting, shown in Figure 5, emphasises universality, describing four levels of provision starting from the assumption that ‘all families need’ universal prevention (Department of Health, 2011b). Taking the proportionate stance recommended by Marmot (2010) allows for more or different offers to be made to families experiencing various types or greater intensities of need, which are considered further below.
New Service Vision: Need for support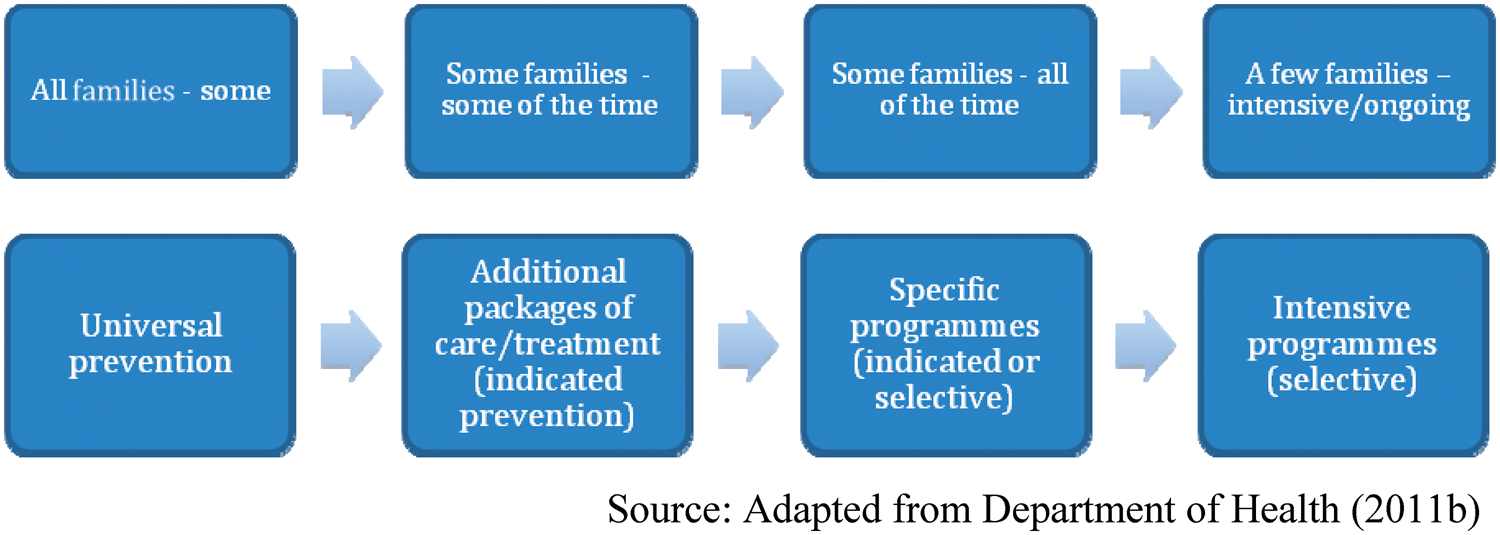
There is limited evidence about the effectiveness of universal prevention (Elkan et al., 2000), because trials tend to focus on the higher effect sizes for target populations obtained through selective or indicated programmes, or to lack a purposeful intervention. Wiggins et al. (2005) carried out a randomised controlled trial of a universal intervention, although it was delivered in an area of deprivation. The health visitors, who were to carry out monthly home visits to all new mothers in the area, were trained not to raise topics themselves (although they could respond to queries raised by the mothers), but to focus on social support. They found no evidence of changes to primary outcomes such as maternal smoking, depression or child injury, but the intervention group mothers experienced less anxious parenting and made better use of available services. A cluster randomised controlled trial in Northern Ireland, where health visitors increased the frequency of visits to all new mothers in the first eight weeks of an infants’ life, also found limited evidence of benefit, although satisfaction with the service was improved and emergency room attendance reduced (Christie and Bunting, 2011).
Macleod and Nelson’s (2000) meta-analysis, which included both promotion of family wellness and prevention of child maltreatment, showed better results from proactive, broad-based and multi-faceted universal and selective programmes, but stressed that they needed to occur over a minimum of 6–12 months, to anticipate any benefit. They suggest that changes in attitudes towards parenting, positive parent–child interaction, and a secure and stimulating home environment are necessary precursors to the prevention of child maltreatment, so the apparently limited benefits described in the two trials above may, nevertheless, be providing a sound basis for later improvement.
Clearer benefits are shown where activities are more specific, as in the large PONDER cluster randomised trial. This showed that women with raised Edinburgh post-natal depression scores (EPDS) fared significantly better than the ‘care as usual group’ if they received the intervention from health visitors trained to identify depressive symptoms, develop therapeutic relationships and provide psychological approaches to managing depression (Morrell et al., 2009). A further analysis of the data showed that women who scored below the EPDS threshold score of 12 (i.e., with no sign of depression) at 6 weeks after childbirth, were statistically less likely to score above that threshold at 6 months after childbirth, if their health visitor had undergone this training, than if they were in the ‘care as usual’ clusters (Brugha et al., 2011). In the treatment trial, 31 (11.4%) of 271 EPDS-positive women benefited from intervention, whereas in the prevention analysis of EPDS-negative women, 46 (3.1%) of 1,474 women benefited. This not only shows effective universal prevention, but also provides another illustration of the ‘population paradox’ described above.
Indicated prevention
The PONDER trial illustrates the importance of health visitors being able to access the whole population, so as to identify depressed women early, and offer them effective treatment both for their own sake and before their infants are affected. Similarly, access to timely and appropriate health care is needed for the very wide range of possible difficulties, developmental delays or diseases experienced by young children. This is in line with the idea that universal health care involves access to curative and rehabilitative are, as well as promotive and preventive care (WHO, 2005).
However, this conceptualisation has given rise to the notion that the ‘universal health visiting service’ is primarily concerned with case-finding and enabling those who need it to access appropriate help and support, rather than majoring on proactive, universal prevention. Similarly, it has been said that both public health nursing (Ciliska et al., 1996) and health visiting (Elkan et al., 2000) are mechanisms for delivering programmes, rather than being interventions in themselves. This perspective assumes that any preventive impact comes from the early intervention programmes, rather than from the professionals; and from timely recruitment to a therapeutic regime, rather than from proactive or primary prevention. Whilst this is important, it is not universal prevention; it is indicated prevention, which targets high-risk people who are identified as having minimal but detectable signs or symptoms indicating predisposition for disorder, but who do not meet diagnostic criteria for disorder at that time (Gordon, 1983; WHO, 2004).
Families with infants and young children often need support in the form of indicated prevention, which may be described as ‘packages’ or ‘programmes’ of care, or as a need for ‘extra health visiting’, at all the different points on the continuum. The ‘service vision’ for health visiting (Department of Health, 2011b) identified some straightforward descriptors of service levels, which map usefully onto the formal definitions of prevention types, as shown in Figure 5, starting with ‘all families need some’. Whilst it may be assumed that these levels also map across the population, as shown in Figure 1, a need for support with a short-term, specific issue (‘some families, some of the time’) occurs regardless of levels of deprivation: examples include breast-feeding or child behaviour problems, or immediate medical needs. Children with complex disabilities or enduring medical needs, likewise, cross all social groups (‘some families all of the time’), whereas vulnerable families who manage pretty well, as long as they have some ongoing support, tend to cluster in the deprived end of the population, with their needs rising in intensity as deprivation increases (‘a few families, all of the time’). The distinction between ‘some’ and ‘few’ is not specified, but ‘few’ signifies a smaller number than ‘some’.
Health visitor indirect input
The health visitor is not only responsible for direct provision of a service to an undifferentiated caseload of families, but also for leading a team that helps deliver appropriate, evidence-based support once a need has been identified. This is shown occurring across the spectrum of the population in Figure 1, as ‘indirect health visitor provision’. This provision is facilitated, but not delivered directly by the health visitor. The line showing indirect health visitor provision has a bulge in the curve, positioned where the population has a lower capacity and fewer resources to call upon, as it is assumed such families are more likely to need this additional, specific support; this needs to be taken into account when teams are set up. However, at the most deprived end of the population, families need intensive support from more highly qualified staff, so the curve tapers off as there should be a greater resource allowed for ‘health visitor direct input’. Indirect health visitor input may occur in three main forms, which are not always clearly understood or distinguished: delegation, referral and collaboration (Carr and Pearson, 2005).
First, delegation is when someone trained in that activity can be asked by the health visitor to deliver a specific, circumscribed package of care. Community nursery nurses are paraprofessionals with particular training in child development and behaviour, so they might be asked to provide specific support to help sort out an infant’s sleep patterns or to deliver baby massage classes to a group of parents. These, and other team members, are employed in teams managed by the health visitor, who remains accountable for any activities they carry out. Such ‘skill mix’ activities can safely be delegated when there is a degree of predictability, in that the required activity is known, the person carrying it out is known to have relevant skills, and parameters can be drawn about when the worker is to report back to the health visitor, who remains accountable for this delegated provision.
Second, a range of additional services is available to families, particularly in the more deprived areas. These might be run in children’s centres managed by local government, health sector or non-governmental organisations in the voluntary sector, which will often have been set up with joint or pooled funding, so that all parents can access them. Here, the role of the health visitor is through collaboration, which involves both helping to develop and maintain these services, and to signpost parents and support their attendance. The more vulnerable parents often need help to attend groups or activities, which may feel very strange and threatening initially. Some parents might feel able to access the service without reference to the health visitor, but the category of ‘indirect health visitor provision’ is still valid where there has been professional involvement in establishing and running the service, through the medium of the ‘lead health visitor’ and ‘Sure Start health visitor’ (Department of Health, 2011b). The lines of accountability for professionals are different here, and more complex, because staff are employed by different agencies, each with their own managers. Arrangements often have to be spelled out when the services are developed (Killoran Ross et al., 2005).
Third, where specialist provision is needed, this might be facilitated by referral from a health visitor to, for example, a speech and language therapist, child psychologist or community dietician. Sometimes, such services are open to self-referral, but they may be accessible only by referral from another primary care professional. Health visitors need to be acceptable as referrers to the specialist, so the reputation of their profession is important. They also need skills to both ‘work up the referral’ so that it is acceptable to the parent being referred, and to understand which service would be most appropriate under the circumstances (Chalmers and Luker, 1989).
The last layer of service provision to be described within Figure 1 is the broader, general resource system, which is funded by a mixture of government, charitable and private sources, and accessed through a range of different, usually locally defined, criteria. This may overlap somewhat with provision accessed only through the health visitor (‘indirect health visitor provision’), because parents with higher levels of personal capacity may well access groups and services that accept self-referral themselves. Where they have sufficient financial means, they might also use private or paid-for provision, which is less accessible to those at the more vulnerable end of the population. This level is important, particularly when considering transfer of evidence-based programmes between, or even within, countries, because of the extent of variation.
Conclusion
There is clear evidence of the need for additional, or higher professional education to deliver specific selective prevention programmes, such as FNP or MECSH. However, there is also a need for highly skilled professionals, like health visitors or qualified child and family health nurses, to deliver universal prevention across an undifferentiated caseload. Concurrently, these professionals can assess whether there is need for a circumscribed or specific package of care, which might be delivered by a less highly qualified (and so, less expensive) person, such as a community nursery nurse or an early years worker, perhaps with training to deliver parenting support, or help with infants’ sleep, feeding or behaviour problems. Such workers need support and supervision, and a team leader who is accountable for the delegated services they deliver. There is added complexity if funding sources or different employment sectors are involved – such as health services, non-governmental organisations, social and early years services – but in all case, lines of accountability need to be clear to staff and to the families receiving the services.
The framework for this paper was presented in Figure 1, which aims to summarise and illustrate the place for different types of practitioner in a health visiting service that encompasses universal, indicated and selective forms of prevention, with some embedded evidence based programmes forming part of a whole, proactive and preventive service. This was developed to support discussions about implementing a programme (MECSH) developed in Australia into the English system. Policy-driven terms derived from the English Health Visitor Implementation Plan have been used, but translated into the generic language of prevention first proposed by Gordon (1983) but now adopted internationally (WHO, 2004), as a basis for future research.
Overall, the figure conceptualises the range of need across the social spectrum, showing how a universal service with embedded programmes can operate to tackle health inequalities, with input increasing proportionately as needs become more marked, and changing in type to match population health across the gradient. It takes account of the valuable contributions made by skill-mix team members and by colleagues working in the wider early years and children’s services and other governmental and non-governmental sectors. It is hoped this framework will both stimulate discussion and help guide future research in this field, to discover which arrangements are safe and effective, and which are not.
Footnotes
Funding
We appreciate the Australian Primary Health Care Research Institute (APHCRI) 2010 Travelling Fellowship, which funded Dr Kemp’s visit to England and made discussions to develop this paper possible.
Conflict of Interest statement
None declared.