
Abstract
The issue of wastage caused by missed appointments features prominently at a time when cost-saving measures become ever more important in the health care economy. Missed appointments are said to cost the NHS in the region of £600 million per annum. Various strategies are being tried and tested to ensure that people attend their appointments (or are in for domiciliary visits) including texting and phoning reminders. Clearly, attending for health care is generally in a person’s best interests. However, in the UK, if appointments are missed, then the usual outcome is a ‘three (or even two) strikes and you are out’ approach with a notification to the General Practitioner.
In this paper we will argue that the seemingly widespread ‘Did Not Attend’ (DNA) routine described above is not appropriate where children and young people are concerned. The issue here is that the child or young person ‘Was Not Brought’ (WNB) to their appointment, rather than the fact that they DNA. This is important, because not only is access to health care their fundamental right (United Nations Convention on the Rights of the Child, 1989: Article 24), but failure to attend for health care is recognised as a child protection issue within statutory definitions of neglect. Failings in presenting children for health care is also known to feature prominently in cases that have reached the threshold for Serious Case Reviews, and this paper summarises the evidence in this respect. We conclude the paper by suggesting that reconceptualising child and young person DNA as WNB will lead to positive interventions to safeguard and promote the welfare of children that go beyond the missed appointment to a move towards the child-centric practice described in recent key reviews.
Keywords
Introduction
This paper seeks to examine the evidence to support a reconceptualisation of ‘Did Not Attend’ (DNA) to ‘Was Not Brought’ (WNB) to encourage health professionals to take a proactive and child-centred stance in ensuring the well-being and safety of children and young people who miss appointments. We begin by briefly discussing the problem of missed appointments in the current health care climate of cost reductions and efficiency measures outlined in the public health white paper and NHS reforms (HM Government, 2010a). The paper examines the semantics of missed appointments and the terminology commonly used in child and family public health practice. We then move on to a brief review of children’s rights to health care and link this to the statutory definition of neglect. We also outline the policy imperative and the evidence from serious case and child death reviews that support a WNB stance, before concluding with some pointers for child and family public health practice.
Background
Nurses, midwives and health visitors will be aware that the issue of wastage caused by missed health appointments is featuring prominently at a time when cost-savings measures in public service provision come under scrutiny (HM Government, 2010a). Missed appointments are typically labelled as ‘Did Not Attend’ (DNA) in patients’ notes. Whilst we acknowledge that health care is delivered in a variety of settings, including the home, published information on DNA is usually linked to data for ‘no shows’ to hospital outpatient appointments (e.g., BBC News, 2011). The figures are stark. According to an article from Dr Foster, Health and the National Health Service (NHS) Information Centre, missed outpatient appointments cost hospitals £600 m per annum; with reported higher rates of non-attendance by young adults 1 and those in the most deprived socio-economic groups (Dr Foster, 2009). The Dr Foster article suggests that missed appointments may be a marker of the quality of the interface between primary and secondary care and the author adds that inappropriate referrals may also feature as an explanation. However, they also report patients’ explanations including forgetfulness, fear, anxiety and a misunderstanding of the system. The article additionally makes reference to initiatives to address DNA rates, including the use of SMS messages and e-mail, with notable success reported within one paediatric outpatient service, and a finding that many patients will attend if a second appointment is offered (Dr Foster, 2009). However, readers will be aware that where patients DNA a further appointment, the usual practice within the UK NHS is to withdraw them from the waiting list and send a letter to the general practitioner (GP) accordingly.
We suggest that the routine decision of health professionals not to offer an additional appointment without a re-referral is a reasonable step to take where consenting adults are concerned (vulnerable adults and those whose unmet health needs impact on their ability to parent, e.g. adult mental health, learning disability or substance misusers, should have more robust follow-up). However, the position for children and young people is arguably not as straightforward; as Roe (2010) has previously maintained, it is the case that the child is ‘not brought’ rather than that they DNA. As we will note, a failure to present a child for health care is reflected in statutory definitions of child neglect. For a minority of children this failure can be the harbinger of serious maltreatment.
This article thus seeks to expose the evidence to support a reconceptualisation of DNA to ‘Was Not Brought’ (WNB) to encourage health professionals to take a proactive and child-centred stance in ensuring the well-being and safety of children and young people who miss appointments. We begin by examining the terminology used in child and family public health practice, followed by a brief review of children’s rights to health care and link this to the statutory definition of neglect. We then outline the policy imperative and the evidence from serious case and child death reviews that we believe support a WNB stance.
The semantics
The concepts of DNA and sometimes Failed to Attend (FTA) are used to refer to patients or clients who do not attend an appointment without cancelling it first. The use of these terms and acronyms is well established in health care practice. Many health providers have DNA guidelines; some being integrated with ‘No Access Visit’ (NAV) and family disengagement policies. In child and family public health practice, the term NAV – not available at home to be seen for a pre-arranged appointment – is also used widely. Hughes (2009: 57) has described how the following situations may be described as no access:
There is no one at home for an opportunistic drop in visit. There is no one at home for a visit which was made by appointment with the family. There is someone at home but they don’t open the door. The door is opened but you are not invited in.
Local DNA policies and guidance have been widely introduced in NHS organisations since publication of the UK National Service Framework for Children, Young People and Maternity Services (DfES and DH, 2004: 10) which stated: Children or young people failing to attend clinic appointments following referral from their general practitioner or other professional may trigger concern, given that they are reliant on their parent or carer to take them to the appointment. Failure to attend can be an indicator of a family’s vulnerability, potentially placing the child’s welfare in jeopardy. It can equally be an indicator that services are difficult for families to access or considered inappropriate, and need reviewing.
This UK wide policy document went on to emphasise the need for systems to be in place to identify children or young people who do not attend an appointment following a referral for specialist care, so that the referrer is aware they have not attended and can take any follow-up action considered appropriate to ensure that the child’s needs are being met (which may include a home visit or telephone contact to find out, for example, whether the appointment is no longer necessary). (DfES and DH, 2004: 10)
The child’s right to health care
The United Nations Convention on the Rights of the Child (1989) outlines a series of protective and welfare rights (‘Articles’) for children and young people (defined as those under the age of 18 years). An understanding of the importance of the children's rights agenda is fundamental to good safeguarding practice (Powell, 2007; Reading et al, 2008). Importantly, the Convention is recognised as a ‘major driver’ (Munro, 2011) in promoting the welfare of children and ensuring their survival, best interests and achievements into adulthood. Article 24 concerns child health and the reduction of child mortality, and in doing so, recognises the right of the child to the enjoyment of the ‘highest attainable’ standard of health and health care services. Crucially it also promotes the role of the state in ensuring that, ‘no child is deprived of his or her right of access to such health care services.’
Whilst this means that governments must ensure the provision of high quality health services to meet the needs of children and young people, it also places the onus on parents (or those with parental responsibility) to ensure that such services are accessed. Where children are not brought to their appointments, the state also has a duty to ensure timely intervention to address such failures and protect the child’s health and wellbeing. Nurses, midwives and health visitors are a key part of the child and family public health workforce who have unparalleled opportunities to make a major contribution to safeguarding and child protection (Appleton and Clemerson-Trew, 2007; Appleton, 2011; Powell, 2011). The seemingly routine activity of following up children who fit the category of WNB for health care could be one way in which these professionals can demonstrate proactive safeguarding that may, in turn, provide a vital means of rescue for a child.
Safeguarding children policy
The duties and responsibilities of all those working with children, young people and their families to safeguard and promote the welfare of children are outlined in statutory guidance Working Together to Safeguard Children: a guide to inter-agency working to safeguard and promote the welfare of children (HM Government, 2010b)
2
. Safeguarding and promoting the welfare of children is defined in the guidance as:
protecting children from maltreatment; preventing impairment of children’s health or development; ensuring that they are growing up in circumstances consistent with the provision of safe and effective care; and undertaking that role so as to enable those children to have optimum life chances and to enter adulthood successfully (HM Government, 2010b: 34).
This broad description of safeguarding encompasses not only protection but a wider and more positive emphasis on prevention and ensuring children and young people’s well-being and safety. The adoption of a WNB stance undoubtedly fits within this definition of safeguarding. However, whilst the guidance provides a broad definition of safeguarding, it is to all intents and purposes concerned with actions that need to be taken to protect children and young people who are at risk of, or suffering, maltreatment. Working Together (HM Government, 2010b) defines child protection as: a part of safeguarding and promoting welfare. This refers to the activity that is undertaken to protect specific children who are suffering, or are likely to suffer, significant harm. Effective child protection is essential as part of wider work to safeguard and promote the welfare of children. However, all agencies and individuals should aim to proactively safeguard and promote the welfare of children so that the need for action to protect children from harm is reduced. (HM Government, 2010b: 35)
The guidance categorises child maltreatment as being physical, emotional or sexual abuse or neglect, although in reality children who are being maltreated are frequently suffering from more than one type of harm.
Neglect, which is currently the most frequently used category that relates to children who become subject to a child protection plan, may involve a parent failing to:
provide adequate food, clothing and shelter (including exclusion from home or abandonment); protect a child from physical and emotional harm or danger; ensure adequate supervision (including the use of inadequate care-givers); or ensure access to appropriate medical care or treatment.
HM Government (2010b: 39) emphasis added
This latter point was highlighted in National Institute for Health and Clinical Excellence (NICE) guidance published in 2009 on When to suspect child maltreatment which recommended that health professionals ‘consider neglect if parents or carers repeatedly fail to attend essential follow-up appointments that are necessary for their child’s health and well-being.’ This guidance also reminds health care professionals to consider child maltreatment, ‘if there is an unusual pattern of presentation to and contact with health care providers, or there are frequent presentations or reports of injuries’ (NICE, 2009: 20) and if a child or young person has poor school attendance that has no justification on health or other grounds.
However, we would urge caution in concluding that a failure to present a child for health care automatically brings families into the statutory child protection arena; there may be valid reasons for the failure to attend (other than where a parent has a good rationale for cancelling or rearranging the appointment). Indeed families may never receive appointments, as letters go astray or, as Cohn (2010) notes, they change their address. Kennedy (2010) also found some evidence that appointments were missed through poor communication and at no fault of the parent. He also noted that children with multiple health needs or disability were unreasonably expected to attend multiple appointments at diverse locations, sometimes on consecutive days. Clearly health services need to take a joined-up approach and co-ordinate such provision. However, the importance of NHS service providers following up ‘no shows’ in children’s health care is recognised by health regulators who have firmly linked this issue with good safeguarding children practice (Care Quality Commission (CQC), 2009). As with many policy documents in the child protection field, the CQC review of safeguarding children practice in the NHS followed a child protection tragedy. And, whilst recognising that fatal or serious maltreatment represents only a very small minority of cases (‘the tip of the iceberg’), it is to this literature that we now turn as it cogently illustrates evidence for a WNB approach and the links between failures to access health care and the child protection arena.
Evidence from serious case reviews
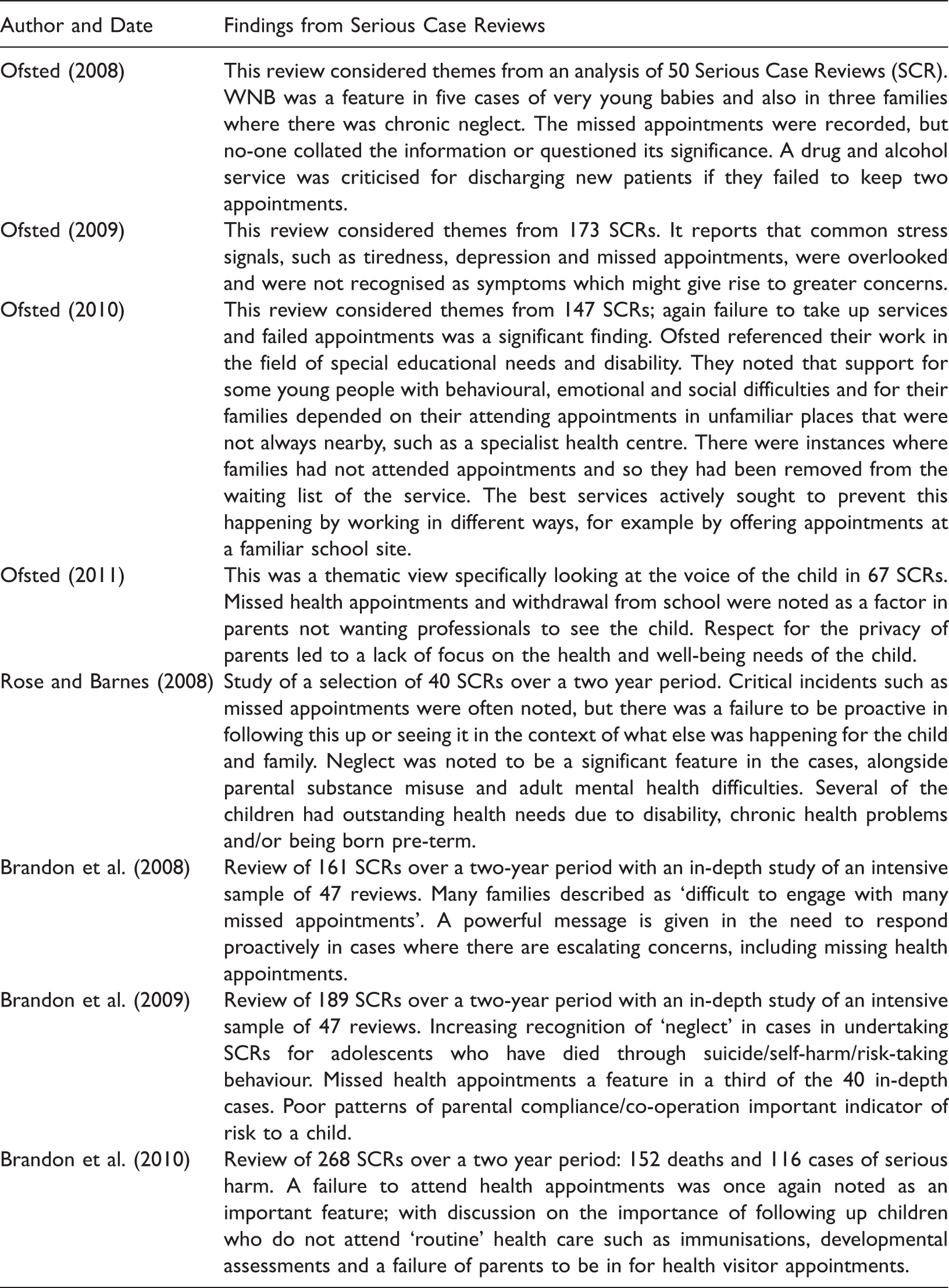
There are a number of publications that have sought to analyse common themes from child maltreatment cases that are at the severe end of the spectrum, i.e. those concerning serious and fatal child maltreatment. These publications have consistently highlighted the issue of children missing appointments (and/or mothers’ poor attendance for ante-natal care) as a notable feature in the case. The seminal work of Reder et al. (1993) is a useful starting point; here the authors sought to analyse the major child death inquiries (n=35) of the preceding 20 years and to set their findings in a social context. They describe a notion of ‘closure’ that at first was generally intermittent but in retrospect became terminal in the lead up to the fatal event: This was a striking phenomenon, noted in over half of the thirty-five cases, in which the family attempted to tighten the boundary around themselves so that they reduced their contact with the external world and few people were able to meet or speak to them. For example, their curtains were always drawn, the children stopped playing outside and no longer attended school or nursery. The parents failed appointments with professionals, the children were not taken to scheduled visits to health clinics and social workers and health visitors could not obtain entry to the home when they called. (Reder et al., 1993: 99)
Findings in relation to missed health appointments
It is worth noting too that DNA has featured in public Child Death Inquiry reports, for example, Jasmine Beckford’s ‘non-attendance’ at nursery school for 10 months was a feature of the case before her death on 5 July 1984 (London Borough of Brent, 1985).
Child death review processes
Further evidence of the importance of following up children and young people who fail to attend for health care is provided by the literature surrounding statutory child death review processes, whereby deaths of all children are routinely reviewed by a multi-agency panel. Such processes became a requirement for Local Safeguarding Children Boards in England in 2008 and are being adopted elsewhere in the UK. These standardised processes draw on the experiences and learning from other countries (most notably the United States, e.g. Webster et al. (2003)). Early findings from UK based studies of those piloting the process reinforce the importance of following up those children who are ‘WNB’.
Pearson (2008) who reports on panels’ analysis of 126 child deaths noted situations in which children who were not taken for health appointments subsequently died and recommended that health services should proactively follow-up non-attendees. In a study of early starter panels, Sidebotham et al. (2008) reported on the case of a two-year old child with epilepsy who died from multi-organ failure against a background of missed appointments.
Discussion
NHS providers are increasingly cost conscious and concerned about the wastage associated with missed health care appointments and the potential savings that can be made by addressing this problem. Initiatives aimed at preventing missed appointments include automated calls to patients, email and SMS reminders. However, in the UK, if appointments are missed, the usual outcome is a ‘three (or even two) strikes and you are out’ approach with a notification to the General Practitioner. In this paper we have presented evidence that the seemingly widespread DNA routine described above is inappropriate where children and young people are concerned, as they are mainly reliant on their parents and carers to bring them to appointments. The issue is that the child or young person ‘Was Not Brought’ to their appointment, rather than the fact that they DNA. This is important, because not only is access to health care children’s fundamental right (United Nations Convention on the Rights of the Child, 1989: Article 24), but failure to attend for health care is recognised as a child protection issue within statutory definitions of neglect.
We have argued that there is evidence from Serious Case Reviews and child death inquiry reports, albeit representing a very small number of cases, that failings to present children for health care, as well as withdrawal from school and no access visits feature prominently. However, further care needs to be applied when examining this evidence. As we have already discussed, DNA rates are not available for children under the age of 15 years, so we do not know the base rates for missed appointments and cannot therefore determine whether missed appointments occur more frequently in families where there are concerns about maltreatment.
From practice, we have extensive anecdotal evidence that failures to access health care are a common feature for those children who reach the threshold for child protection inquiries and that addressing such deficits feature highly within statutory child protection plans. However, finding empirical evidence to support this (other than in relation to serious case reviews) proved challenging, with one exception. Watson and Forshaw (2002) reporting on the findings of a retrospective audit of all paediatric outpatients appointments at one hospital, found that over a six month period of 2183 appointments, 685 were missed, and a third (157) of the non-attendees were known to social services. They report that of these 157 patients, ‘38 were listed on the child protection index, of whom eight were on the current child protection register’ (Watson and Forshaw, 2002: 739). Again, caution in interpreting these figures is required, as being known to children’s social care services is not a good enough proxy for maltreatment. The statistic will also include disabled children and these, of course, have a more than average number of appointments and so more scope for missing one. However, we also need to recognise that this additional complexity is compounded by the increased risk of this population of children suffering maltreatment (Murray and Osborne, 2009).
So what are the obstacles to paying more attention to children’s missed health care appointments?
Arguably if it became a requirement of the NHS Operating Framework for comprehensive data to be kept by NHS organisations about children’s missed health care appointments, then it would be possible to raise it as an organisational priority. There would also be a baseline from which to measure children’s missed appointments and thereby greater opportunities for considering the statistical evidence for links with statutory definitions of maltreatment. Until this data is recorded nationally, children will not be afforded an equal status with adults; a factor that challenges the United Kingdom’s compliance with the UN Convention on the Rights of the Child (1989) and adds to the concerns of many of us working in the safeguarding and child protection field that children, and their particular needs for welfare and protection, can be somewhat ‘invisible’.
We suggest that by reconceptualising child and young person DNA to WNB will lead to positive interventions to safeguard and promote the welfare of children that go beyond the missed appointment to a move towards the child-centric practice described in recent key reviews (Munro, 2011). As Roe (2010: 1052) has described ‘stating that a child was not brought to an appointment will remind individuals of the child’s vulnerability. Health professionals are likely to be more proactive in following up children who WNB than those who DNA.’ We agree firmly with Roe’s (2010) view. Child and family public health nurses working in primary and secondary care are in a key position to take forward a WNB strategy.
So how can WNB practice be developed for children and young people?
A wealth of recent policy emphasises the importance of early intervention work for promoting children’s health, development and well-being (Field, 2010; Allen, 2011; DH, 2011), as well as the need for good joined up working between services. The Healthy Child Programme (HCP) is the core health service for promoting, protecting and improving children and young people’s health and well-being (DH, 2009). Health visitors as leaders and deliverers of the HCP are well-placed to implement the WNB policy and if copied in to WNB correspondence, to follow up children who fit the category of WNB for health care.
We believe that all health care professionals must adopt the child-centric focus advocated by Munro (2011) following her independent review of child protection. Roe (2010: 1052) has recommended that existing policies and databases should be retitled WNB instead of DNA and that ‘WNB rates should be the measure used’. Such policies should outline for staff the steps to be taken in WNB and NAV cases. Roe (2010) also stresses the need for health care professionals to determine the reason why a child or young person was not taken to an appointment, considering this primarily from the child’s perspective, but also taking into consideration any parental difficulties.
Properly addressing the issue of WNB requires a shift in thinking, which needs to move beyond the development of local polices and guidelines, to positive action in practice. A very important task is to assess the reason for the WNB and to consider its significance from the child’s perspective. This means assessing the child or young person’s needs, their possible vulnerability and the risk to their health and well-being. If a child is not brought to an appointment there are important questions to consider:
why has this child not been brought for their appointment? what are this child’s needs? what is the risk to the child’s health and well-being? what information do we already have about this child? (You may need to liaise with the person who referred the child or other professionals who have knowledge about the child and their family.) is this the first or a repeated WNB? is there a Common Assessment Framework (CAF)/lead professional? is the child known to children’s social care services? is the child subject to a child protection plan? are there any parental difficulties that are impacting on the ability to meet the needs of the child? what am I going to do about it and what action should I now take?
It is clear from the evidence presented in this paper that children are more likely to be vulnerable if they are not brought to health care appointments, so follow-up is always required. As well as liaising with the referrer there may also be a need to communicate with other services to seek further information about the child and family. It is important to document the WNB, and make a record of action taken and outcomes. Child and family public health nurses should liaise with their manager or safeguarding/child protection lead if they have concerns about a child or young person’s health or well-being.
Conclusion
This paper has reviewed relevant health policy and attempted to systematically present the available evidence on children and young people’s missed health care appointments. The paper reveals a growing body of evidence, largely from Serious Case Reviews, that missed appointments, along with school withdrawals, and lack of follow up, is often a feature of serious or fatal cases of child maltreatment. We have argued for a reconceptualisation of DNA to ‘Was Not Brought’ (WNB) to encourage health professionals to take a proactive and child-centred stance in ensuring the safety and well-being of children and young people who miss appointments. We have concluded with some practical steps to support the development of practice in the area of WNB, which should assist Child and Family Public Health Nurses in delivering care to children and young people who are not brought to health care appointments.
Key points
Health care professionals should reconceptualise DNA ‘Did not Attend' to WNB ‘Was not Brought' for children's missed appointments.
Children have a fundamental right to health care.
Children are more likely to be vulnerable if they are not brought to health care appointments.
Health care professionals must assess the reason for the WNB and consider its significance from the child's perspective.
Document WNB and make a record of action taken and outcome.