
Abstract
Coping with breathlessness is a complex and multidimensional challenge for people with chronic obstructive pulmonary disease (COPD) and involves interacting physiological, cognitive, affective, and psychosocial dimensions. The aim of this study was to explore how people with moderate to most severe COPD predominantly cope with breathlessness during daily living. We chose a multi-modal grounded theory design that holds the opportunity to combine qualitative and quantitative data to capture and explain the multidimensional coping behaviour among people with COPD. The participants’ main concern in coping with breathlessness appeared to be an endless striving to economise on resources in an effort to preserve their integrity. In this integrity-preserving process, four predominant coping types emerged and were labelled: ‘Overrater’, ‘Challenger’, ‘Underrater’, and ‘Leveller’. Each coping type comprised distinctive physiological, cognitive, affective and psychosocial features constituting coping-type-specific indicators.
In theory, four predominant coping types with distinct physiological, cognitive, affective and psychosocial properties are observed among people with COPD. The four coping types seem to constitute a coping trajectory. This hypothesis should be further tested in a longitudinal study.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) has a profound impact on the lives of people coping with it, and the incidence of COPD is increasing worldwide (WHO, 2008). COPD is characterised by a progressive reduction of pulmonary function affecting functional capacity and daily living quality (Ito and Barnes, 2009). Breathing difficulties are the most disturbing and distressing symptom of COPD (GOLD, 2010). ‘Breathlessness’ and ‘dyspnoea’ are terms commonly used to describe breathing difficulties (West and Popkess-Vawter, 1994). While ‘dyspnoea’ designates laboured breathing observable to another person, ‘breathlessness’ specifies the subjective feeling of laboured breathing with or without dyspnoea and/or abnormal pulmonary function (West and Popkess-Vawter, 1994).
Coping with breathlessness comprises interacting physiological, cognitive, affective, and psychosocial dimensions (Nici et al., 2006). Despite a growing body of knowledge regarding how people with COPD cope with breathlessness, it is still unknown whether these interacting dimensions shape particular coping types. In this paper, we will present a grounded theory that captures the multidimensionality of how people with COPD predominantly cope with breathlessness during daily living.
Background
Breathlessness is a hallmark symptom of COPD (GOLD, 2010). People suffering from COPD develop a variety of strategies to cope with breathlessness, which both negatively and positively influence their breathing abilities and accomplishment of daily living activities during hospital stay (Lomborg and Kirkevold, 2005; Lomborg et al., 2005) and at home (Nici et al., 2006).
Low self-efficacy, anxiety, depression, hypoxia, hypercapnia, hypoxia-induced cognitive decline, skeletal dysfunction, weight loss or obesity and other concomitant diseases each compromise patients’ breathing abilities and functional level in daily living (American Thoracic Society/European Respiratory Society, 1999; Davis et al., 2006; Kobayashi et al., 1996; Masuda et al. 2001; Nonoyama et al., 2007). Consequently, coping with breathlessness may constitute a complex process involving physiological, cognitive, affective and psychosocial dimensions (Nici et al., 2006).
The short-term effect of pulmonary rehabilitation appears to be significant in relation to dyspnoea, fatigue, emotions and patients’ control over COPD (Lacasse et al., 2006). However, the long-term effect, measured on outcomes as health-related quality of life and readmission frequency, seems less so (Bratås et al., 2011; Nici et al., 2006). Given that the type of coping seems to influence health-related quality of life (Hesselink et al., 2004) and survival rate (ZuWallack, 2007) in patients with COPD, coping problems may contribute to the burden of advanced respiratory disease (Nici et al., 2010). Elucidating possible interrelations between predominant coping types and verbal and nonverbal behaviour, thoughts, feelings, and impaired physical condition may reveal indicators of coping preferences. Coping-type-specific indicators can form the basis for identifying individual coping patterns and thereby facilitate individualising pulmonary advice to address symptom control and quality of life.
Aim
The aim of this study was to explore how people with moderate to most severe COPD predominantly cope with breathlessness during daily living. The study focused on conceptualising (and thereby explaining) a variety of behavioural and physiological processes involved in coping with breathing difficulties. This paper reports the first part of a larger study, in which we investigated other behavioural and physiological coping-type-specific indicators.
Methods
Design
Classic grounded theory (GT) was chosen as the overall design (Glaser, 1978, 2001, 2004; Glaser and Strauss, 1967) and the study relies on a realist epistemology (Lomborg and Kirkevold, 2003). A multi-modal approach was chosen (Jørgensen et al., 2012) holding multiple modes of data collection and analysis processes with the intension of capturing physiological, cognitive, affective and psychosocial dimensions of coping behaviours.
This multi-modal approach is in line with classic GT, which holds the opportunity to combine qualitative and quantitative data to generate theory grounded in data from the empirical area under study (Glaser, 2008). The study followed Glaser’s advice in generating a theory with the ability to explain patterns of behaviour (Glaser, 1978). Data were collected at the hospital and in the participants’ homes after discharge.
Participants
Patient details including predominant coping type (N = 12)
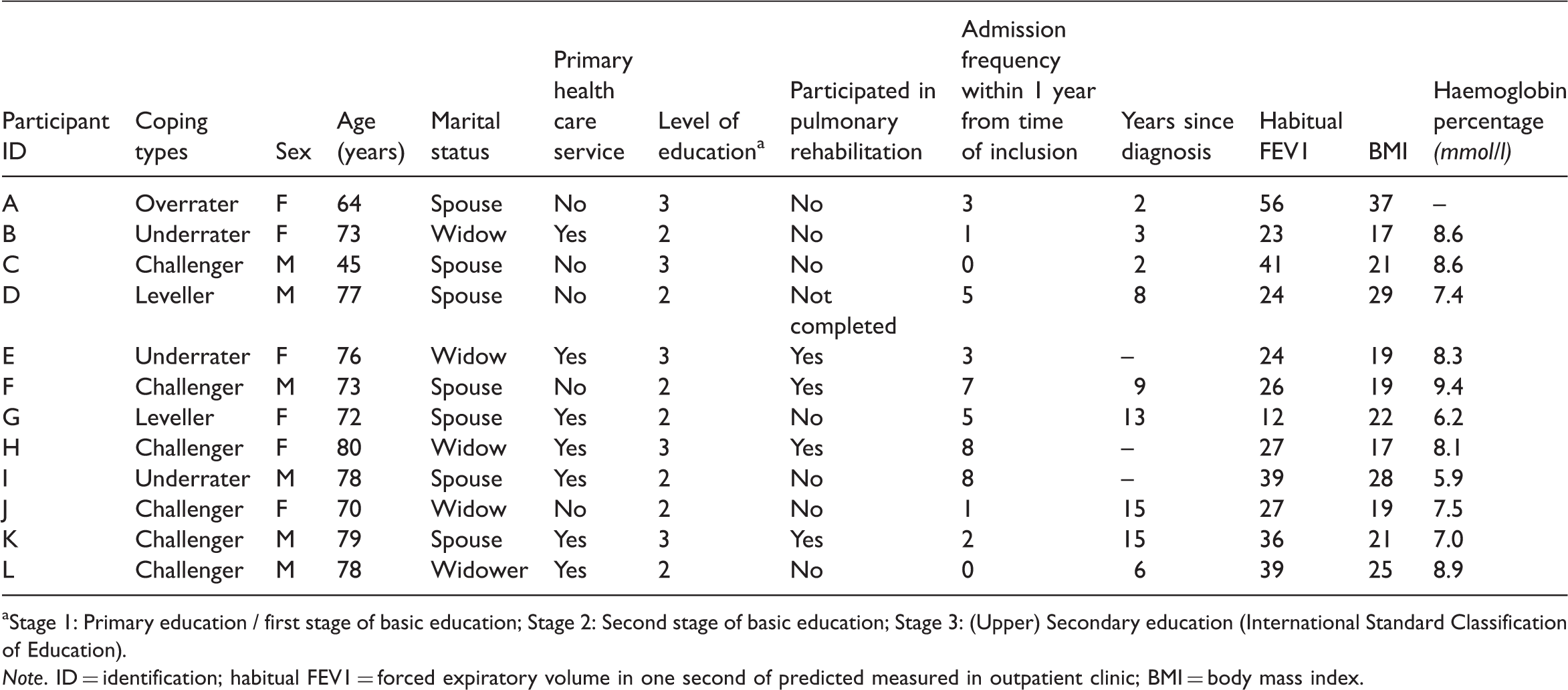
Stage 1: Primary education / first stage of basic education; Stage 2: Second stage of basic education; Stage 3: (Upper) Secondary education (International Standard Classification of Education).
Note. ID = identification; habitual FEV1 = forced expiratory volume in one second of predicted measured in outpatient clinic; BMI = body mass index.
Study participants’ comorbidities
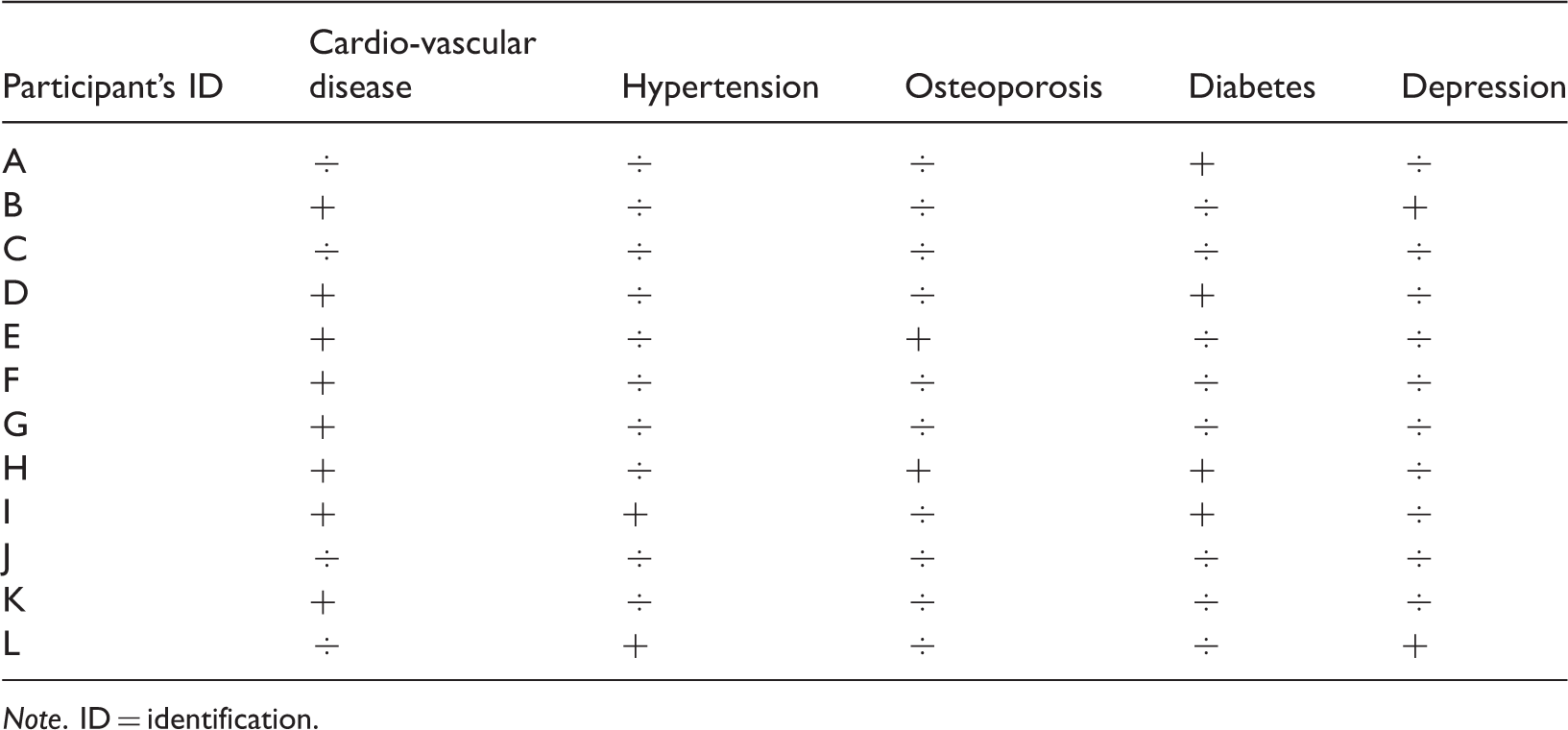
Note. ID = identification.
Data collection
Investigating the complex process of coping with breathlessness in the participants’ daily living called for both creative and innovative thought when choosing methods of data collection that would sufficiently match the multidimensionality of coping. Because of the ambition of integrating physiological, cognitive, affective, and psychosocial variables into the evolving grounded theory, we prioritised gathering comprehensive data related to each participant rather than including a larger number of participants. Based on common knowledge about COPD this study partly collected a pre-planned data set (Figure 1), which was the source for additional data.
Flow chart for the preplanned data collection process during PBC on a day-to-day basis. Note. PBC = personal body care; MBS = The modified Borg scale; FEV1 = forced expiratory volume in one second of predicted; SaO2 = oxygen saturation.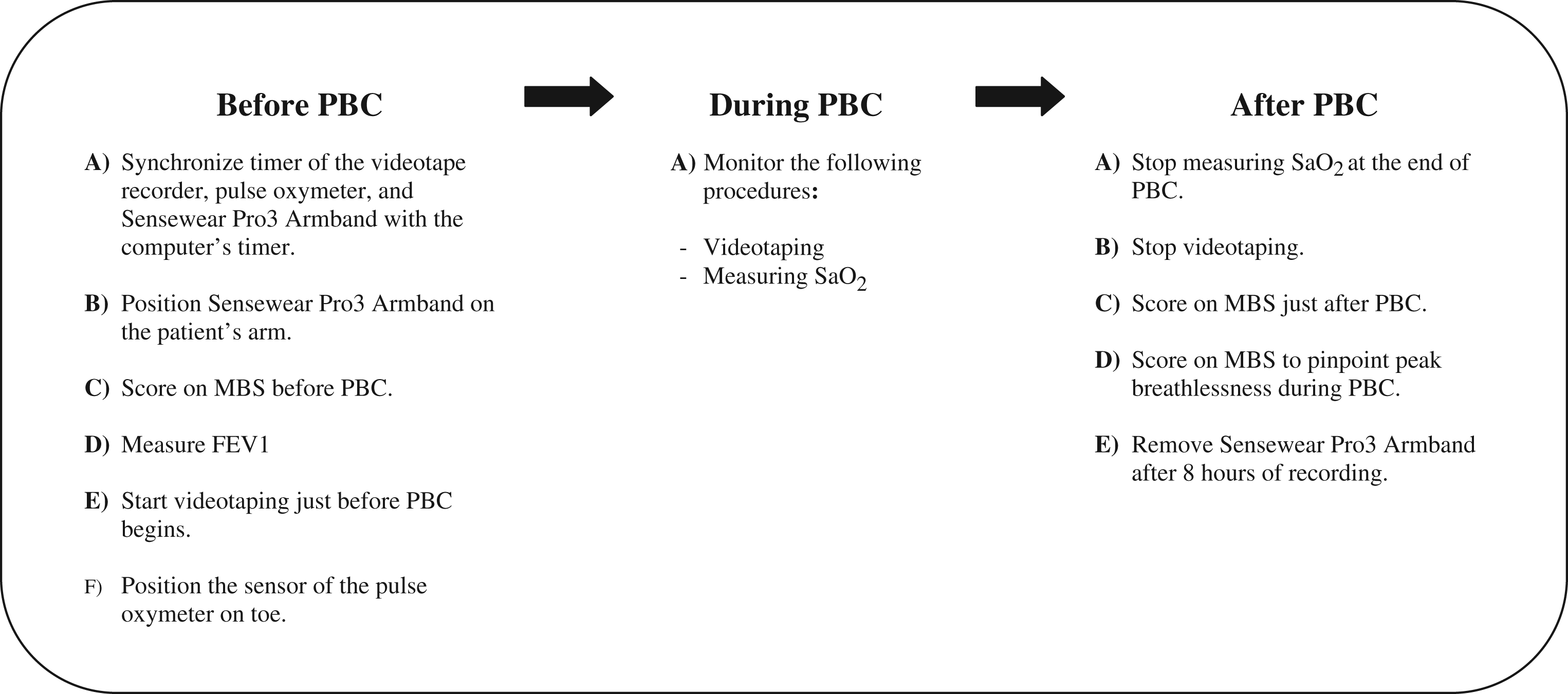
The aim was to secure data that could capture the multidimensionality of coping. The pre-planned data were collected before, during and after personal body care (PBC). The theoretical sampling procedure guided the analysis of the pre-planned data, as well as the inclusion of new data. Figure 2 illustrates the chronology of collecting and analysing the total database during the three-phased joint data, code and analysis procedure.
Chronology of data collection and analysis processes. Note. MBS = modified Borg scale; FEV1 = forced expiratory volume in one second of predicted; SaO2 = oxygen saturation; MET = metabolic equivalent; RR = respiratory rate.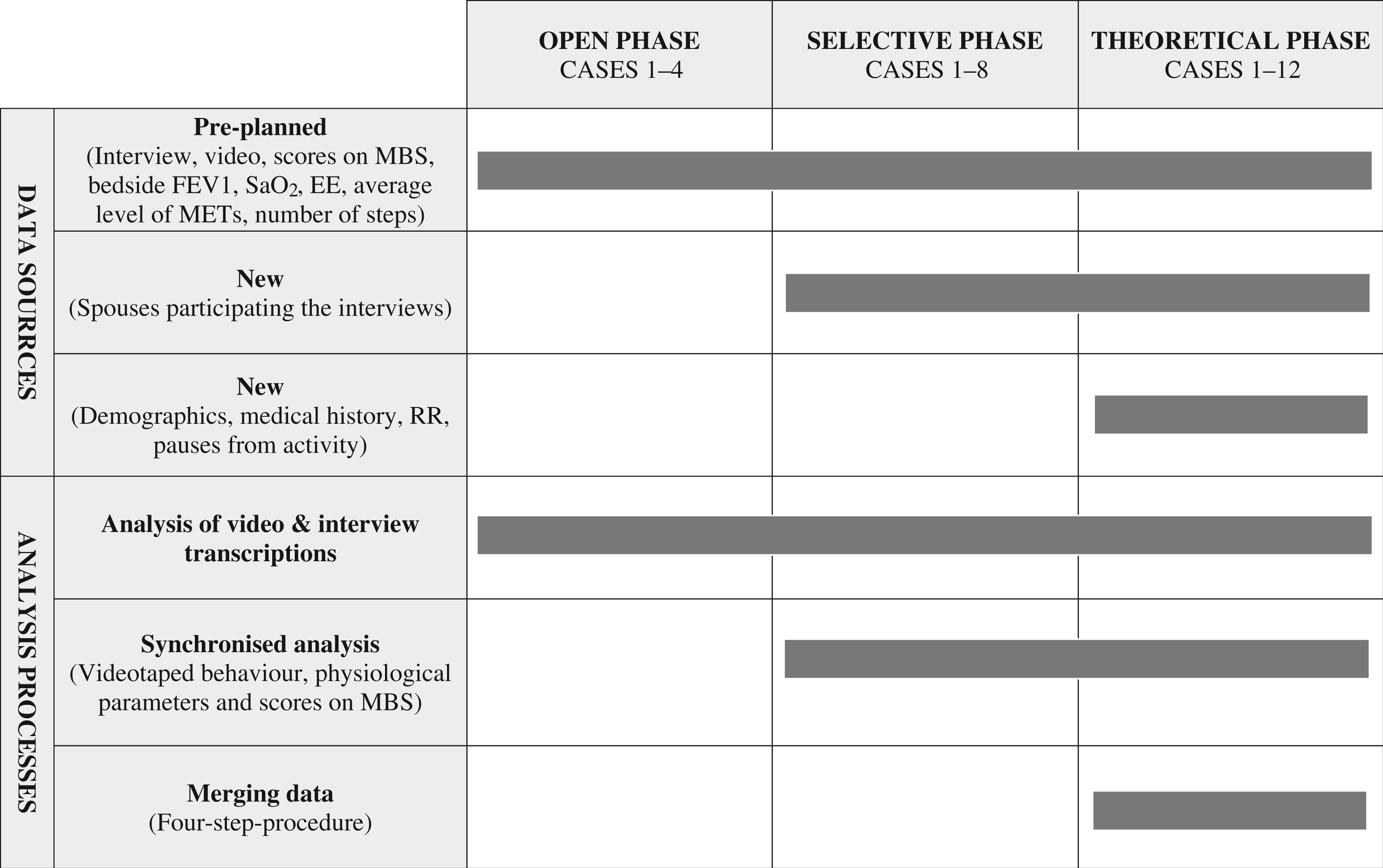
Data collection and analysis guided the theoretical sampling phase. For example, the coping behaviour of the first included participant with moderate COPD persistently deviated from the behaviour of the following five included participants with severe or very severe COPD. Several possible reasons for this deviation were looked for in the data. In the ensuing data collection and analysis process, this heterogeneity led us to obtain an equal distribution of male and female participants with differing degrees of COPD. Additionally, data revealed that spouses constituted a significant extra-personal and interpersonal resource, playing a vital role in how participants handled a life influenced by breathlessness. Therefore, spouses were invited to participate in the following interviews with the intention of enriching our understanding of the participants’ coping strategies. These discoveries on equal terms with other preliminary findings resulted in an ongoing alteration of guides for interview, video observation, and selection of video sequences. Additionally, theoretical memos (notes about the data, concepts and conceptualisation process) played a vital role in generating and articulating the theory (Glaser, 1978). Writing memos paced the process of generating the theory; forced us to verify categories; avoided us to draw premature conclusions; stored ideas and made them sortable. In the theoretical phase, memos became the primary source for saturating the categories and their interrelationship.
Video-based narratives
People with COPD may have communicative difficulties due to hypoxia-induced cognitive decline, weakened memory, and reduced linguistic skills (Incalzi et al., 1998; Meek et al., 2001; Michaels and Meek, 2004; Schwartzstein, 1998). To accommodate this impediment towards generating fruitful interview data, video and interview were combined in the ‘video-based narrative’ (VN) method (Jørgensen, 2007). VN consisted of videotaping each individual participant during PBC and subsequently interviewing the participant on the basis of video sequences and an interview guide. This procedure was conducted during hospitalisation and at the participants’ home 2–3 weeks after admission to investigate how context may affect coping. PBC was initially chosen as an example of a troublesome daily activity, as this activity often escalates breathlessness and threatens the integrity of people with COPD (Leidy and Hasse, 1999; Lomborg and Kirkevold, 2005; Lomborg et al., 2005; Nici et al., 2006)
According to the video literature (Davidoff et al., 1998; Horwitz et al., 2003; Mihai et al., 2007), people viewing themselves stimulate their memory and narration. Therefore, using video for self-observation is pivotal in VN, and it was used to stimulate the participants’ memory supporting their narration regarding what it is like to live with chronic breathing difficulties. Striving to avoid any violation of the participants’ integrity, a covenant was developed: (1) exact rules were devised for video recording (e.g. the recording of personal intimate hygiene was not allowed); (2) participants were offered the opportunity to abstain from participation at any time without any appraisal; and (3) additional permission from the participants was required for the video recordings to be used in other settings in the future.
Physiological recordings and intensity of breathlessness
Video recordings of the participants during PBC sessions were combined with measurements of SaO2 displaying the participants’ oxygen capacity during the process of coping with loss of breath.
The modified Borg scale (MBS) (Kendrick et al., 2000) was used to capture the subjective experience of breathlessness intensity. The participants ranked the intensity of breathlessness using the MBS before and after PBC sessions, as well as retrospectively to describe their peak experience of breathlessness during the performance of PBC. Bedside forced expiratory volume in one second of predicted (FEV1) was measured just before PBC and after scheduled morning dose of bronchodilators.
People with COPD often emphasise their reduced level of activity as a hallmark of managing life with COPD (Leidy and Hasse, 1999). Additionally, the level of activity in daily living seems to be related to their way of coping with COPD (Katz et al., 2005). To investigate possible interactions between level of activity and predominant types of coping with breathlessness, the participants wore a validated multi-sensor armband (SenseWear®, PRO3 armband; BodyMedia, Inc., Pittsburgh, PA, USA) (Patel et al., 2007; Watz et al., 2008) positioned on the upper right arm for 2–3 days. The armband estimated the intensity of physical activity, expressed in metabolic equivalents (METs) expressing an average person’s metabolic rate. A unit of metabolic equivalent, or MET, is a ratio comparing a person’s metabolic rate while seated at rest to their metabolic rate while performing some task (Ainsworth et al., 1993).
Physical activity was measured for 8 h per day for at least two consecutive days, both during hospital stay and at home. Accommodating differences in measuring time among the participants, all armband measurements were calculated as a mean average per hour. For technical and safety reasons, the armband was removed for bathing or showering.
Like VN the physiological recordings and scores on the MBS were pre-planned while the following methods were included along with the analysis as they, in accordance with GT (Glaser, 1978), were found to be relevant and thereby ‘earned their way’ into the study.
Demographics and medical histories
Comorbidities and age seemed to partly explain a deviant coping behaviour in two of the participants. Consequently, demographics and medical histories were included in order to explore possible indicators of coping types (see Tables 1 and 2).
Data collection was delimited in relation to recording video, measuring the numerous physiological parameters and scores, and transcribing interviews and videos, as these procedures produced no additional understanding of the core categories and subcategories. The number of data collection sessions per participant is illustrated in Figure 3.
Number of data collection sessions per participant.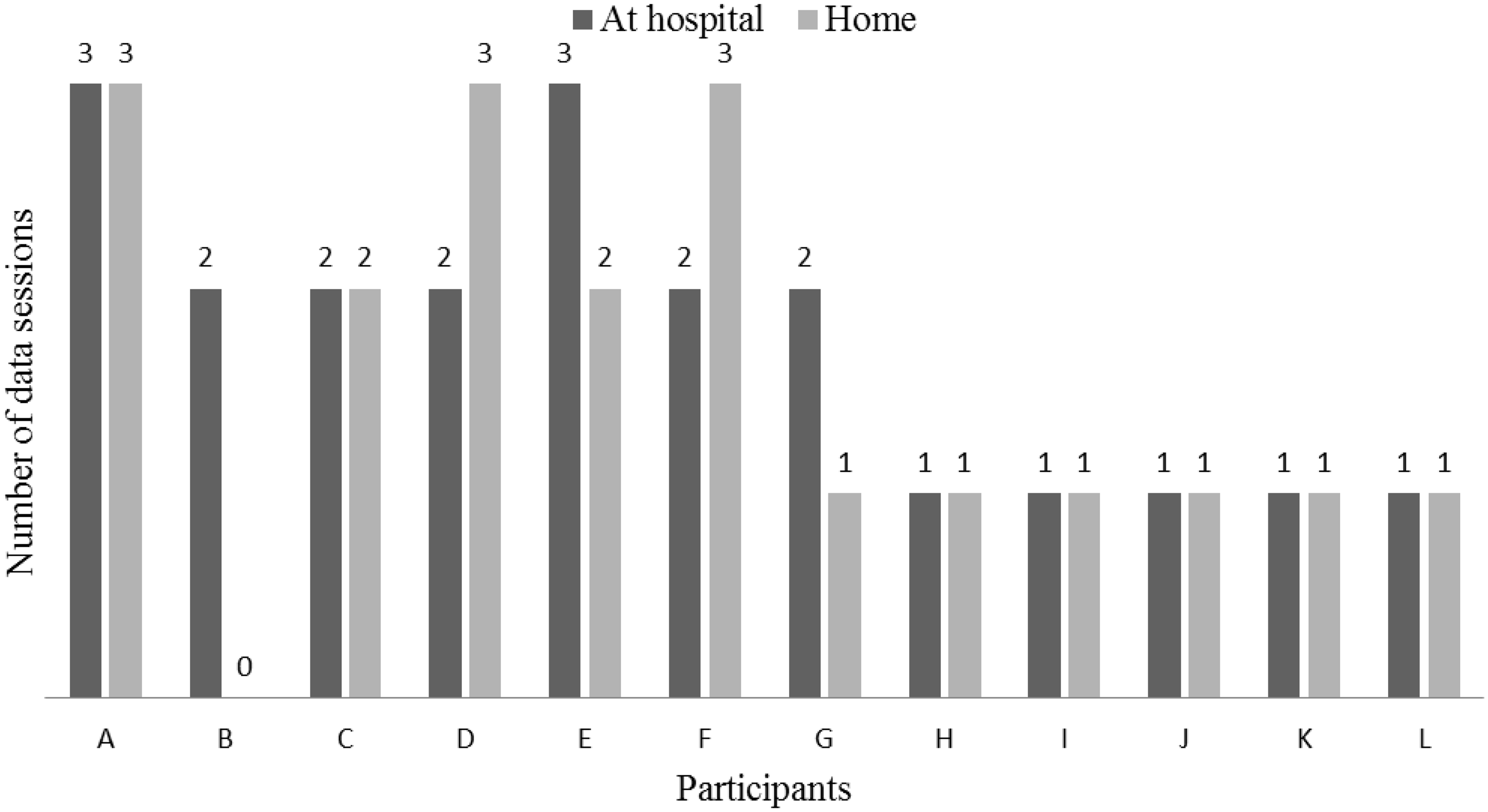
In total, our final database contains 50 variables with physiological, cognitive, affective and social information about each participant. The theory was based on data from 24 interviews, 40 video recordings, 32 video transcriptions, 40 sets of measurements of physiological parameters, 40 sets of MBS scores and 12 sets of demographics and medical histories. The generated theory was based on data collected both during hospital stay and at the participants’ homes as the analysis revealed that the main concern in coping with breathlessness and predominant coping type characteristics did not differ noticeably between the two different contexts.
Ethical considerations
The Danish Data Protection Agency gave permission to conduct the project (J. No. 2008-41-2266). According to the Scientific Committee for the County of Aarhus, the Biomedical Research Ethics Committee System Act does not apply to this project. With reference to The Helsinki Declaration (World Medical Association Declaration of Helsinki, 2000), all participants were informed both verbally and in writing about participation in the study.
Data analysis
Exemplifications on three different types of comparisons in the constant comparative process
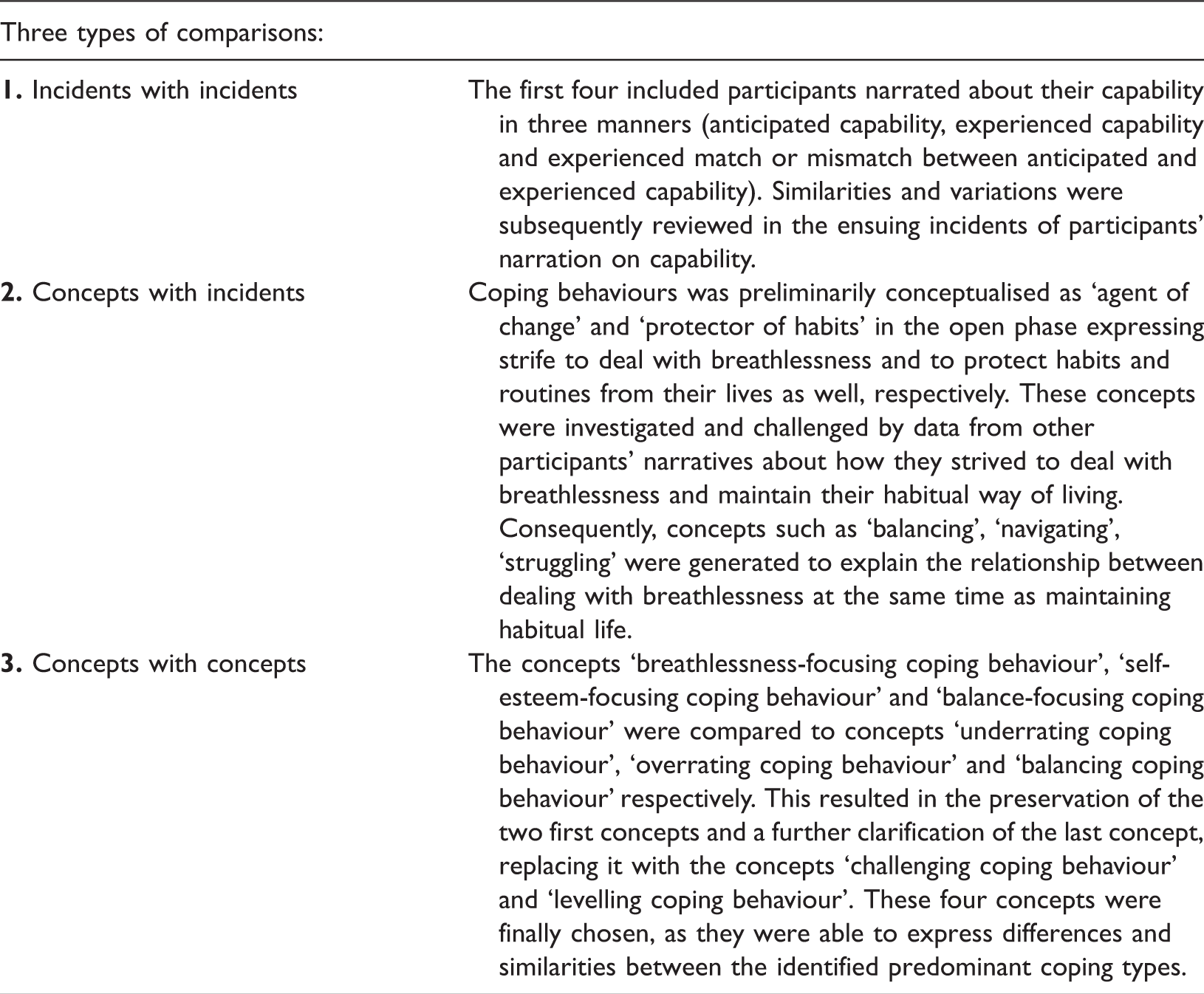
The joint data, code and analysis process produced three kinds of subordinated analysis processes embraced in the constant comparison procedures: (1) analysis of video and interview transcriptions focusing on identifying and conceptualising the possible interplay of participants’ thoughts, feelings, and nonverbal behaviour in coping; (2) synchronised analysis of videotaped behaviour, physical parameters and scores using a time table; and (3) finally, merging data (Figure 4). The process of merging data consisted of four chronological steps: (a) participants were classified according to the four identified, yet preliminary coping types; (b) preliminary coping type classifications of the participants and possible coping type indicators were incorporated into an Excel spread sheet; (c) by letting one indicator at a time determine the classification of the reaming coping type indicators, interesting indicator patterns among the preliminary coping types were generated, enhancing our understanding of the coping types; (d) statistical analysis were conducted by pooling observations on possible coping type indicators that were observed during the synchronised analysis.
Chronology of the merging data procedure.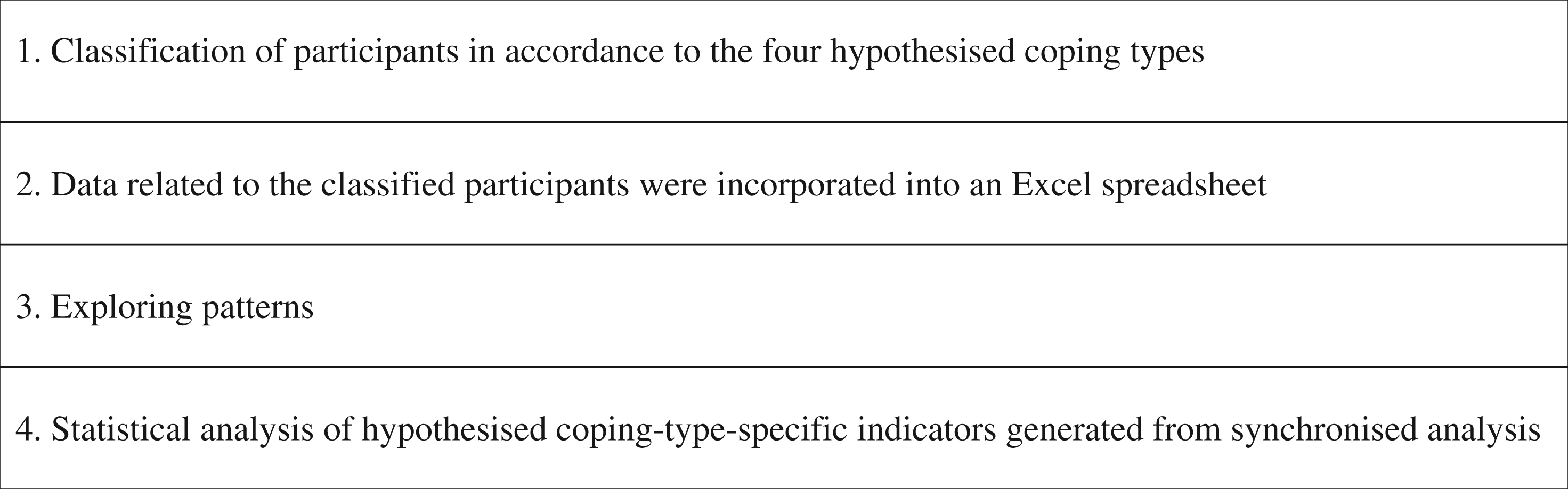
In retrospect, it became obvious that the core category (main concern) and subcategories (coping types) were based first and foremost on interviews and video recordings, while the measurements, medical histories and the statistical analysis of hypothesised coping-type-specific indicators observed in the videos saturated the core category, and also generated additional subcategories.
Results
Coping type specific indicators
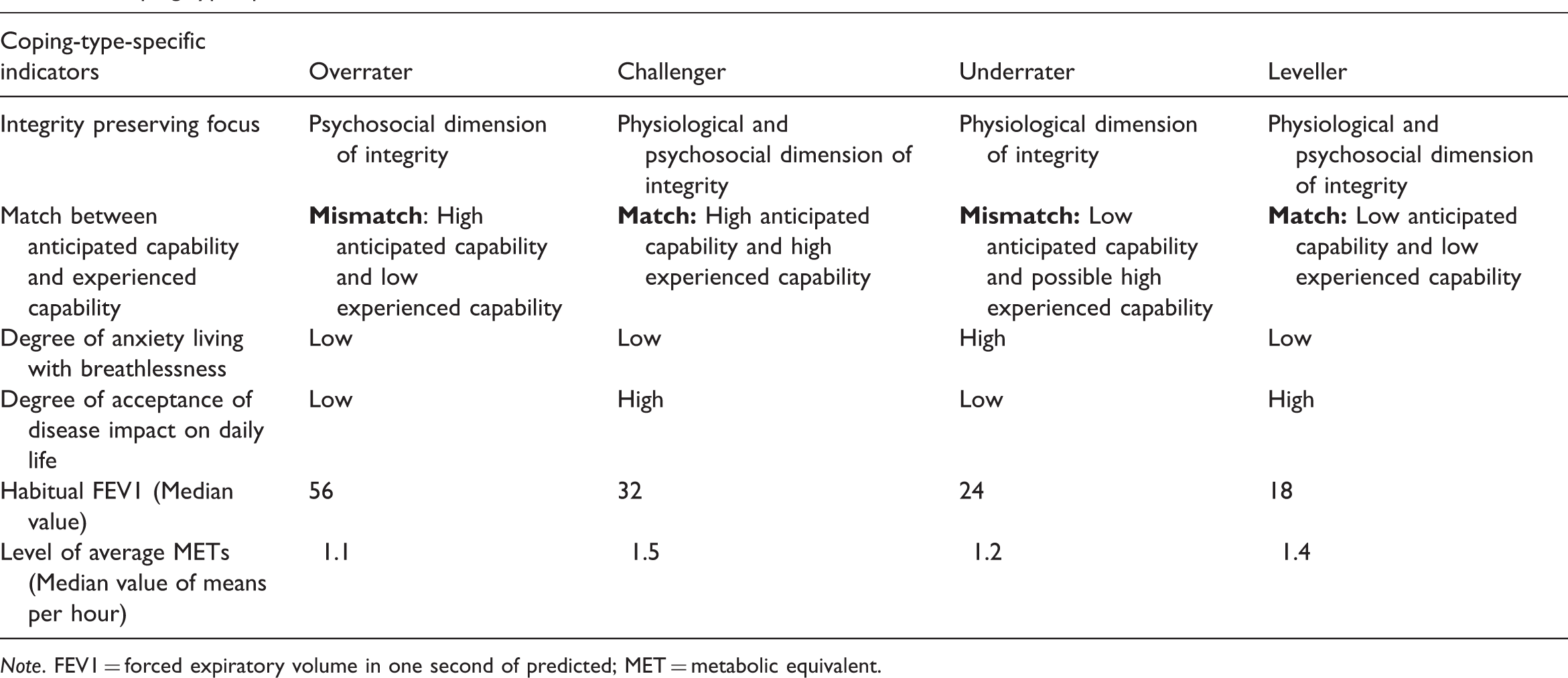
Note. FEV1 = forced expiratory volume in one second of predicted; MET = metabolic equivalent.
How the other included physiological and behavioural data (bedside FEV1, scores on the modified Borg Scale, SaO2, respiratory rate, type and frequency of pauses from activity) may be able to function as coping-type-specific indicators is presented elsewhere.
Four types of coping with breathlessness during daily living
Among the study participants, we identified four types of coping behaviour with breathlessness, and labelled them ‘the overrater’, ‘the challenger’, ‘the underrater’ and ‘the leveller’. ‘Economising integrity preservation’ was the main purpose of coping. As illustrated in Figure 5, coping with breathlessness appeared to be a circular process comprising a cascade of cognitive, affective and behavioural actions.
The process of coping with breathlessness during daily living.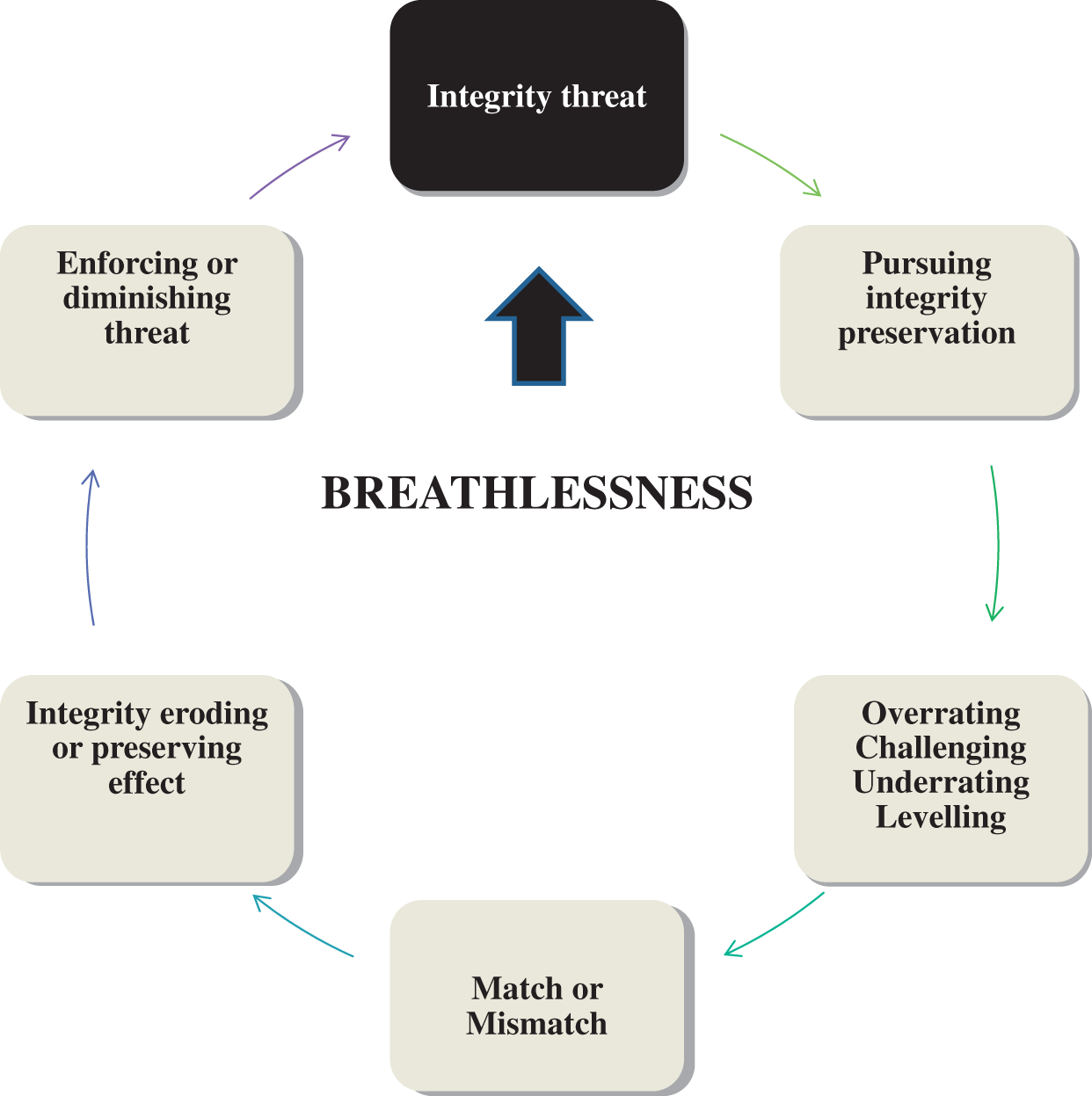
Across the four coping types, the participants experienced that breathlessness was threatening to the physical and psychosocial dimensions of their integrity. They feared asphyxiation and loss of worth as social human beings. Consequently, participants focused on preserving either both the physical and psychosocial dimensions, or only the dimension perceived to be most at risk of being violated by breathlessness. The participant’s choice of preservation focus depended on coping type.
In trying to preserve their integrity, the participants economised with their resources in multiple ways. For the participants, economising meant to administer resources in an efficient and suitable manner. The criteria for the efficiency and appropriateness of the economisation were coping-type-specific and depended on the focus of each patient’s integrity preservation. Across the four coping types, six predominant and interacting strategies for economising resources emerged (Figure 6).
Economising strategies used by the four coping types.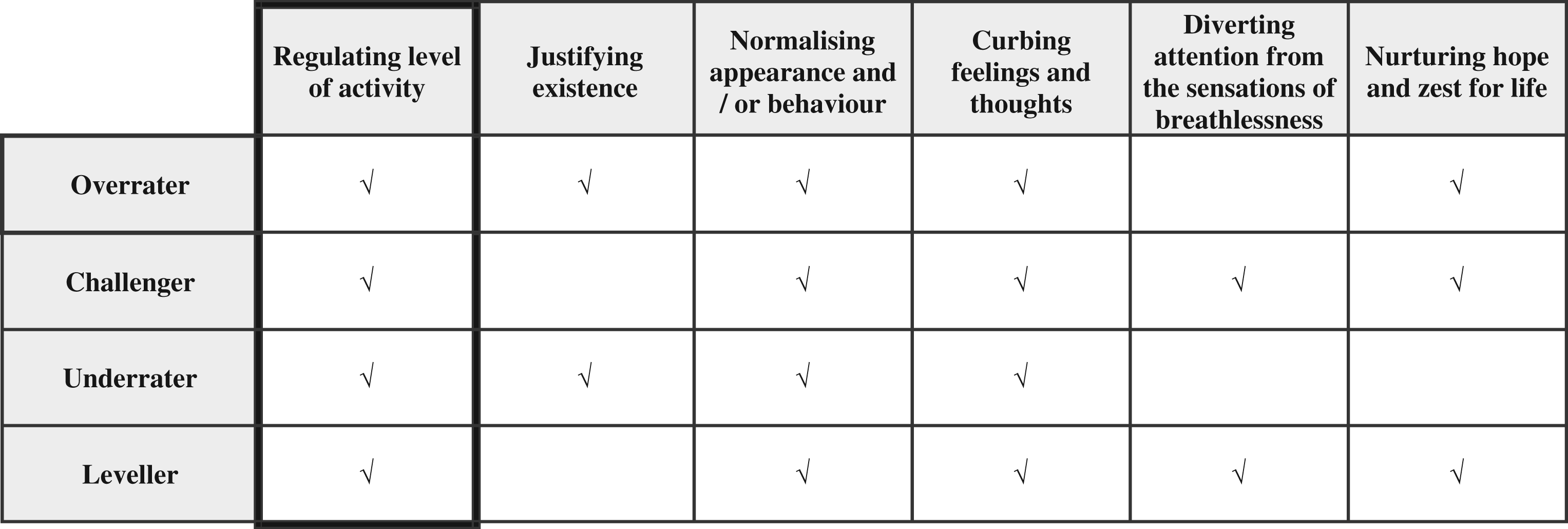
Each coping type seemed to favour some of the strategies. However, the regulation of activity level appeared to be the basic economising feature, urging participants to avoid breathlessness-related stress, anxiety, and physical and psychosocial defeat. All participants narrated their capability in three ways: (1) their expectations regarding level of capability; (2) their experienced capability; and (3) the experienced match or mismatch between the anticipated and experienced capability. Thus, participant A with overrating coping behaviour stated: ‘I plan the day as if I am well (anticipated capability), but I rarely manage to go through it (experienced capability) … this is annoying and stresses me (experienced match or mismatch) … ’ Participants regulated their activity level either by overrating, challenging, underrating, or levelling their anticipated capability. These four manners of regulation partly constituted the four coping types. When overrating or underrating their capability, the participants were unilaterally focused on either the psychosocial or physical dimensions of integrity, neglecting the other dimensions. As shown in Figure 7, this unilateral focus created a mismatch between the participants’ anticipated capability and experienced capability, resulting in integrity-eroding behaviour.
Match or mismatch between anticipated capability and experienced capability.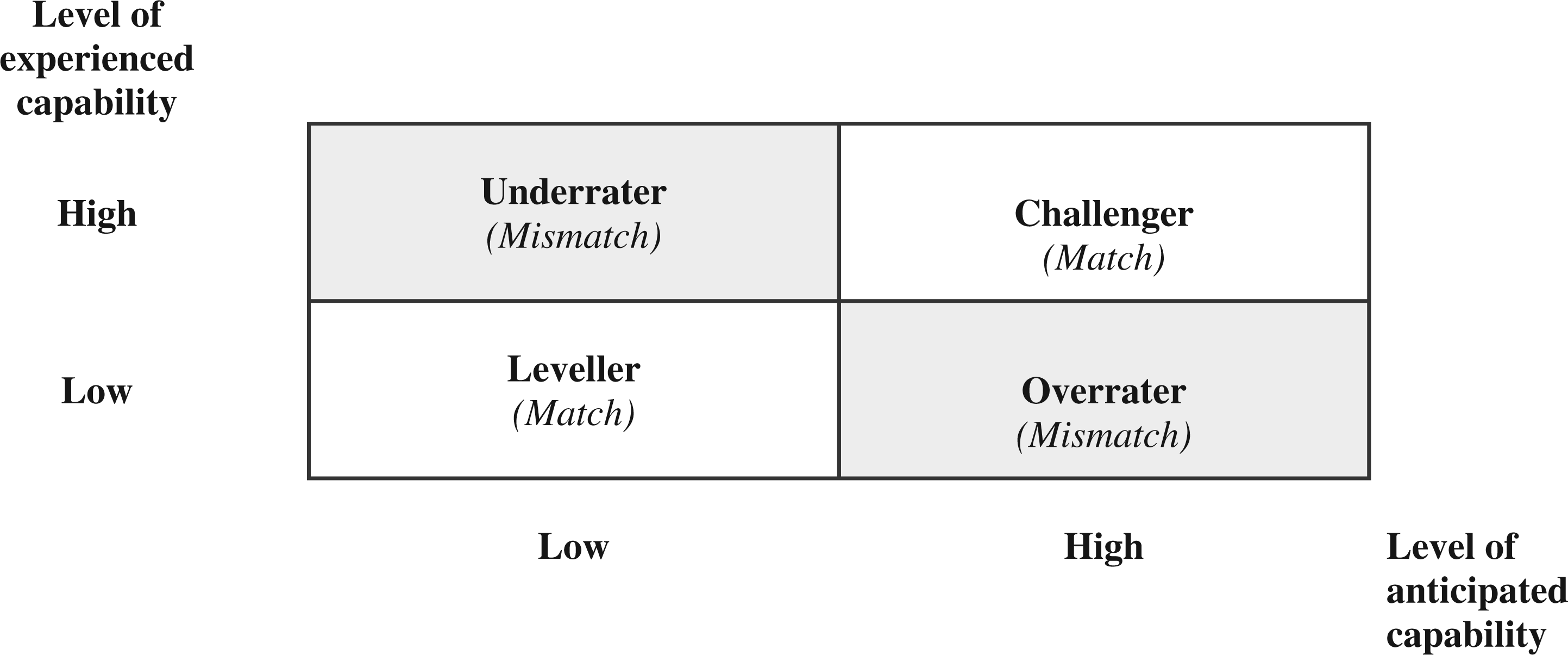
Conversely, participants who consciously challenged and levelled their capability were continuously attuned to their anticipated capability, which resulted in an integrity-preserving behaviour creating a between anticipated capability and experienced capability. These integrity-eroding or integrity-preserving behaviours respectively enforced or diminished the participants’ experience of threat caused by breathlessness.
Three cardinals of difference appeared among the coping types: (1) how the participants perceived the impact of breathlessness on their integrity; (2) how the participants met this threat while striving to preserve their integrity; and (3) the consequences of the preservation of integrity. These cardinal differences will provide structure in the following elaboration of the four coping types.
Overrater
‘The Overrater’ behaviour appeared in only one participant who focused on preserving psychosocial integrity, and consequently overestimated the physical capability required to sustain a level of daily life activities as a healthy person. Moderate COPD appeared in this coping type, indicating that the physical awareness of breathlessness was minor and breathlessness was therefore less life-threatening (Table 3). This participant for instance experienced a minimum of breathlessness during PBC. Therefore, maintaining their self-image as capable of living an active life as a normal and healthy person appeared to be the main purpose, which manifested as making effort to preserve normal habits, routines and procedures. In this way, overrater behaviour would predominantly focus on preserving psychosocial integrity, first and foremost by regulating the level of activity at the same time as curbing feelings and thoughts.
This economising process was accomplished to avoid the stressful experience of not being capable. Participant A stated: ‘It stresses me not to do what I have planned for the day … and stress makes me breathless so I try to calm down …’. Nevertheless, the strong effort to fulfill the role of managing a normal life seemed to be the most obstructive factor against fulfilling this effort. Planning and starting the day anticipating to have the strength of a healthy person appeared to result in failed completion of the plan, damaging the participants’ self-image as a capable individual. As illustrated in Table 3, the average level of METs among ‘overraters’ appeared to be the lowest among the coping types, with a median value of 1.1, suggesting that the neglect of actual physical capacity may reduce the level of activity obtained by a patient with COPD. This neglect manifested itself in a mismatch between anticipated capability and experienced capability, termed ‘mismatching capability’ (Figure 7). Overrating seemed to create a rebound effect that eroded physical and psychosocial integrity, as the patient’s expectation of being capable was rarely accomplished and the physical condition was strained instead. This coping type contained a strong normative characteristic, expressed as ‘I must be able to’.
Challenger
‘The Challenger’ focused on keeping a balanced preservation of both physical and psychosocial integrity. A distinct feature of this coping type was a consciousness of how breathlessness made an impact on daily living and (attuned to reduced physical conditioning) how to accommodate wishes for accomplishing important activities. The impact of breathlessness did not result in a fear of escalating breathlessness or loss of self-esteem. On the contrary, this coping type exuded confidence regarding how to manage life with breathlessness. Despite a common experience of not being able to control the occurrence of breathlessness, ‘The Challenger’ would control to what extent breathlessness was allowed to control life. Participant H stated: ‘I cannot control breathlessness but I can control how much breathlessness controls my life’. This coping type continuously challenged physical limits substantiated in the pulmonary benefits of exercising as well the as benefits of self-esteem as a capable person. Participant L stated: ‘Even though it makes me breathlessness … and I have to rest … I will sprinkle my garden … it’s important to me … and it’s exercise’. ‘The Challenger’ refused to accept incapability in relation to accomplishing daily living activities of especially high importance. Severe COPD and highest average level of METs were observed in participants who employed this coping type (Table 3). Figure 7 illustrates the match between challengers’ anticipated capability and experienced capability, in which they preserved a self-image as both a competent patient with COPD and a healthy person still taking part in selected life activities. This finding may explain why this coping type did not employ the economising strategy of ‘justifying existence’, as shown in Figure 6. Preservation of integrity succeeded through a balanced focus on preserving both physical and psychosocial integrity. In contrast to participants who employed overrating behaviours, participants who employed challenging behaviours created a reinforcing effect on the pursuit for the preservation of integrity. Challenging created a ‘matching capability’, expressed as ‘I am and will be able to’ (Figure 7).
Underrater
‘The Underrater’ focused on preserving physical integrity, risking the underestimation of capability to avoid both the fear of suffocation and suffocation itself. Breathlessness was experienced by participants with this coping type as an uncontrollable and potentially life-threatening experience. To avoiding the risk of suffocation, ‘The Underrater’ would focus on avoiding breathlessness first and foremost by reducing the level of activity. Participant B stated: ‘It is so nice that my helper know I can’t do anything … if my breathlessness gets worse I panic … so it’s nice that they know I can’t do a thing’. The second-lowest median value FEV1 and the lowest average level of METs were observed in participants who employed this coping type. Except for one participant with severe COPD (participant I), the participants who employed this coping type had a degree of COPD severity placed at the lower end of the ‘very severe COPD’ classification. The one participant with severe COPD (participant I) also had the highest degree of co-morbidity, suffering from diabetes, core pulmonary disease, and anaemia (Table 1).
Unilateral focus on preserving physical integrity resulted in a conspicuous struggle, compromising natural attempts to preserve social roles. This compromising coping type created a need for justifying existence (Figure 6) through explaining deselection of daily life activities of high importance. Participant E stated: ‘… there are a lot of things that I won’t give up … but I see the writing on the wall … saying I have to’. Furthermore, the unilateral focus on physical integrity may reduce functional capacity over time, creating a rebound effect. This rebound effect results in a downward spiral, as reducing activity level may decrease physical conditioning, and thereby increase the patient’s risk of experiencing breathlessness during activities. In this way, courage in attaining important daily life activities may be eroded. Therefore, striving to preserve integrity could create a vicious cycle of integrity-eroding behaviour, as neither physical nor psychosocial integrity was preserved. This coping type contained the experience of ‘I dare not be capable’ expressing a low level of anticipated capability in relation to experienced capability, thereby creating a possible ‘mismatching incapability’ (Figure 7).
Leveller
‘The Leveller’ had a balanced focus on preserving both physical and psychosocial integrity in daily living. This coping type would secure enough strength to get through the day by conserving energy. Although ‘The Leveller’ and ‘The Challenger’ behaviours each featured a balanced focus, ‘The Leveller’ had a higher level of acceptance regarding a low level of capability. Participant G stated: ‘ … this is how it is … you can’t do the things you used to do … you must learn to accept that …’. ‘… it’s just … the day must go by as good as possible … don’t you think … that’s the way it is’. Unlike the other three coping types, this coping type was based on acceptance of breathlessness and its impact on life. In general, participants who employed this coping type regarded breathlessness as controllable in relation to avoiding escalating breathlessness, and consciously refused to fight against being sick. This coping type emerged in participants with the lowest median value of FEV1 (18) and very severe COPD. On the contrary, participants with levelling behaviour showed a higher level of activity (average level of METs: 1.4) than participants with overrating or underrating behaviour, suggesting that a lack of fear and a high degree of acceptance of limited physical capacity may have resulted in a more levelled economising strategy. This economising behaviour may secure a higher level of activity throughout the day. ‘The Leveller’ contained an awareness of economising their strength, using the whole spectrum of economising strategies. Like ‘The Challenger’, ‘The Leveller’ did not predominantly apply the strategy ‘justifying existence’. This conscious awareness of accepting physical limits and not dreading breathlessness created a match between anticipated capability and experienced capability, expressed as ‘I know and accept I am not able to’, thereby reinforcing the process of integrity preservation.
Discussion
This study generated a theory on four predominant types of coping with breathlessness holding physiological, cognitive, affective and psychosocial features. Comparing research findings on coping is difficult to accomplish due to the heterogeneity of coping research (Skinner et al., 2003). However, to the best of our knowledge no studies have identified similar four coping types among people with COPD comprising physiological, cognitive and affective coping-type-specific indicators.
Comparing central elements of the theory with current coping literature enhance, though, the understanding and explanation of the identified coping behaviour. Thus, coping with breathlessness during daily living appears to be a complex and demanding task with existential importance for people with COPD. This finding is consistent with Morse (1997)’s and Charmaz (1983)’s studies highlighting that living with a chronic disease means struggling to preserve integrity. Balancing between living with the disease and maintaining a self-image as a capable human being is evidently a main concern in chronically ill people (Boyles et al., 2011; Charmaz, 1995; Cicutto et al., 2004). Additionally, our theory supports that people with COPD use a variety of economising strategies in coping with breathlessness as regulating activity level (Leidy et al., 1999; Lomborg et al., 2005; Siela, 2000), justifying existence (Boyles, 2011; Lomborg et al., 2005), normalising appearance and behaviour, curbing feelings and thougths (Boyles, 2011; Lomborg et al., 2005), diverting attention from the sensations of breathlessness (Peuter et al., 2004), and nurturing hope and zest for life (Persson and Rydén, 2006). It is noteworthy that these economising strategies are positive and constructive in their capacity of being means of preserving the participants’ integrity.
Lung hyperinflation is a progressive condition and a distinctive physiological feature of breathing problems among people with COPD. This condition contributes to the intensity and sensation of breathlessness (O’Donnell, 2006). Breathlessness consists of qualitatively different sensations with fluctuating intensity occurring as a result of an interaction between physiological, psychological and socio-cultural factors (American Thoracic Society, 1999; Nici et al., 2006; GOLD, 2010). This complexity may support the finding that COPD is a heterogeneous disease that mirror variability among people with COPD when it comes to correlations between disease severity (FEV1), degree of breathlessness and exercise tolerance (Agusti et al., 2010; GOLD, 2010; O’Donnell, 2006). However, by categorising the study participants in accordance with their predominant and multidimensional coping behaviour, instead of their FEV1, coping-type-specific variances in FEV1 and level of activity appeared. Among participants with ‘Overrater’ or ‘Underrater’ coping behaviour, the unilateral focus on either the psychosocial or physical dimension of their integrity may be due to their stages of COPD, as breathlessness may be less of a problem for people with COPD stage II compared to people with COPD stage III and IV (Garcia-Aymerich et al., 2011).
The rebound effect found in the wake of the ‘Underrater’ coping type is a well-known phenomenon in sedentary lifestyle, as the low level of activity deconditions the body and further aggravates both breathlessness and capability (Clark et al., 2009; Garcia-Aymerich et al., 2006). However, whether coping type shapes the manner of activity regulation or vice versa may be a ‘chicken or egg’ discussion. Physical inactivity is both a cause and an effect of declining physical function in the elderly (Belza et al., 2001). Several studies indicate factors that influence activity level, including anxiety and depression (Clark et al., 2009), past exercise habits (Soicher, 2009), marital status (Cohen et al., 2006), level of self-efficacy, gender (Siela, 2000), comorbidities of systemic inflammation and left cardiac dysfunction (Watz et al., 2009), diabetes (Garcia-Aymerich et al., 2006), and supplemental oxygen (Nonoyama et al., 2007).
Similarities seem to exist between our concept ‘anticipated capability’ and Bandura’s concept ‘self-efficacy’ (Bandura, 1977). People’s beliefs in their efficacy play an important promote role in health (Bandura, 1995; Wood and Bandura, 1989) and in coping with a life with breathlessness (Nici et al., 2006). Self-efficacy expresses the person’s trust in his ability to handle a situation. The higher self-efficacy a person holds the better he performs (Bandura, 1995). This may explain why people with ‘Challenger’ and ‘Leveller’ coping behaviour appear to have the highest activity level and a general sense of being able to go through with activities of most importance to them. But our theory also implies that a high anticipated capability does not necessarily result in a high experienced capability or performance as seen in the ‘Overrater’ coping behaviour. On the contrary, an anticipated capability insufficiently attuned to experienced capability may result in a low activity level and damaged self-esteem.
Lazarus found that coping is a constantly changing effort to manage internal and/or external demands constituting two general coping strategies: ‘Problem-focused coping’ expressing an active effort of solving the problem causing stress and ‘Emotion-focused coping’ aiming to reduce the negative emotions caused by stress (Lazarus and Folkman, 1984). These coping characteristics also appear in the four coping types, as people with ‘Overrater’ and ‘Underrater’ coping behaviour predominantly focus on preserving their psychosocial and physical integrity, respectively, partly by reducing feelings of not being capable and feelings of fear of suffocation. On the contrary, people with ‘Challenger’ and ‘Leveller’ coping behaviour resort to predominantly focus on solving the problem causing stress by meeting their needs as a pulmonary ill person at the same time as maintaining specific activities improving their self-esteem as a social human being.
The study participants constitute a homogeneous group as they comprise a selected population of people with moderate to very severe COPD who have previously been hospitalised due to exacerbation of COPD. The study participants may consequently share physiological and behavioural characteristics which, on the other hand, may differ from characteristics on non-hospitalised people with similar degree of lung decline. Our theory proposes that habitual FEV1 has the ability to discriminate predominant types of coping with breathlessness among previously admitted persons with COPD. As FEV1 is expected to decline over time due to aging and COPD (Pitta et al., 2005), the association between FEV1 and the identified four coping types suggests predominant coping behaviour to change over time constituting a coping trajectory among previously admitted people with moderate to very severe COPD. Thus, a ‘time dimension’ seems embedded in the multidimensionality of coping with breathlessness indicating that people with COPD follow a coping trajectory going from overrating to challenging to underrating to levelling coping behaviour. Since people with challenging and levelling coping behaviour seem to adapt to a reduced capability at the same time as they withhold a life style that preserve their self-esteem, pulmonary advise may support people with overrating and underrating coping behaviour to strive for integrity-preserving behaviour as challenging or levelling coping behaviour, respectively. This hypothesis on a coping trajectory based on a cross sectional exploration must of course be further tested in a longitudinal study exploring coping trajectories and mechanisms involved.
This study’s use of the labels ‘overrater’ and ‘underrater’ coping behaviour (contrary to the more favourable labels as ‘challenger’ and ‘leveller’ coping behaviour) poses ethical contentions, as it indicates a deficit in coping behaviour among people with COPD. The health care professionals’ use of concepts and pre-understanding, derived from theories and predefined labels, can influence the identity, capability and coping behaviour of chronically ill people (Telford et al., 2006). A thorough explanation of the purpose of these labels is therefore necessary and must be communicated to health care professionals and people with COPD before applying the labels in pulmonary rehabilitation.
Assessing the quality of a grounded theory must take into account four criteria. The theory should fit the data; work to explain, predict and interpret the empirical area under study; be relevant meaning that the theory must focus on a core concern or process that emerges in a substantive area; and should be modifiable with contextual changes (Glaser, 1978; Glaser and Strauss, 1967; Lomborg and Kirkevold, 2003). Our hypothesis on the four coping types works to explain different degrees of success in coping with breathlessness in daily living, which we assert is a relevant contribution to practical rehabilitation interventions. The coping types mirror a Western culture and a society that strongly encourage self-care. One can, therefore, imagine a need for theoretical modification along with cultural changes. Interpreted from a realist epistemological position (Lomborg and Kirkevold, 2003), fit might have been compromised due to the reliability of data derived from measuring instruments. Therefore, measuring time and the participants’ intermittent use of rollator may impede the reliability of the measured average level of METs (Hill et al., 2010; Watz et al., 2009). However, the reliability of this study’s finding on a relation between FEV1 and activity level are supported by Watz et al.’s study observing a sedentary activity level among participants with stage II–IV COPD.
Conclusion
In theory, four predominant types of coping with breathlessness during daily living appear among previously hospitalised people with COPD. The theory suggests several coping-type-specific indicators. The four coping types seem to constitute a coping trajectory.
Key points
Four predominant types of coping with breathlessness were identified among people with COPD comprising physiological, cognitive, affective and psycho-social characteristics. The four coping types seem to constitute a coping trajectory following lung declination due to aging and COPD. Identification of individual types of coping with breathlessness among people with COPD can support immediate and specific rehabilitation intervention based on individual needs for counselling on how to live with breathlessness. The hypothesis of a coping trajectory must be further tested in a longitudinal study. If a coping trajectory is proved to be valid, this knowledge should be a central element in education and support of people with COPD to modify coping behaviour and achieve either a challenging or levelling coping behaviour.
Footnotes
Conflict of interest statement
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.