
Abstract
Aim
This paper reports a study that explored the experience of people living with chronic illness among a group of Irish patients.
Background
Chronic conditions affect the lives of millions of people around the world. Understanding their experience and how they cope with chronic illness can help nurses develop appropriate plans for their patients. To date no study on the experience of chronic illness in Ireland was found.
Design
A qualitative descriptive design using focus group interviews was used in this study.
Method
Two focus group interviews with a convenient sample of 19 people with chronic illness were carried out and data collection took place in 2008.
Findings/results
Although the participants’ chronic conditions were varied, a number of common themes were evident from their narratives. These were: ‘a sense of loss’, ‘feelings of anger and frustration’, ‘uncertainty and stress’ and ‘adapting to a new life’. Financial loss and the fragmented nature of health care for people with chronic illness were particularly felt by this group of Irish participants.
Conclusion
It was clear that chronic illness affected their physical, psychological and social lives. They identified a number of personal losses, but felt strongly that they had to continue to make changes in their lives as they struggled to adapt to a new life. The contribution of partners and family members were crucial in this process of adaptation. Service providers need to assess the extent to which their services meet the needs of people with chronic illness in an integrated way.
Introduction
In developed countries, as many as 25% of 65–69 year olds and 50% of 80–84 year olds are affected by two or more chronic health conditions simultaneously (World Health Organisation, 2008). Chronic conditions are described as long-term conditions with an uncertain course, often leading to negative consequences such as physical suffering, psychological problems, reduced quality of life, reduced ability to work, family difficulties and sometimes to disability (Lundman and Jansson, 2007).
Chronic conditions according to the World Health Organisation (2002) cover a broad category of what could appear on the surface as disparate health concerns. However, persistent communicable (e.g. HIV/AIDS) and non-communicable diseases (e.g. cardiovascular disease, cancer and diabetes), certain mental disorders (e.g. depression and schizophrenia) and on-going impairments in structure (e.g. amputations, blindness, and joint disorders) are all chronic conditions.
Meeting the needs of people with chronic illness require insight into how they make sense of, cope and live with their condition. If health care professionals can understand the process that facilitates people to move towards coping with their chronic conditions, it can make a substantial contribution to enhance their chronic condition self care management and their lives.
Literature review
Research on experiences of living with long-term conditions has shifted from an outsider perspective to the experience from the perspective of the person with the disease or condition (Thorne and Paterson, 2000). A review of the literature revealed many qualitative studies on the experience of people with specific chronic conditions such as diabetes (Watts et al., 2010) asthma (Rudestam et al., 2004), heart disease (Peterson et al., 2010) or cancer (McCaughan and McKenna, 2007), although there are a growing number of studies looking at the experience of chronic illness generally (Kralik, 2002).
Whitemore and Dixon (2008) found that the emotional aspects of living with chronic conditions present daily challenges for the sufferer and their relatives. They also reported that living with chronic conditions led to feelings of sadness, depression, anxiety, anger, frustration and fear.
People who experience significant injury or illness often go through a process of grieving for their losses and making sense of them before they can make adjustments (Wilde, 2003). The theme of ‘loss’ was reported by Lundman and Jansson (2007). The participants described loss as a partial or total impairment of physical and/ or mental functions and strength, as well as changes in appearance and posture. These changes caused impediments in functions such as balance, bending over, using the hands and stamina. These losses led to modifications of previously ingrained habits, such as daily routines, eating habits and socialising. While each chronic condition has problems specific to the type of condition, there may be common challenges and needs across chronic conditions. People living with chronic conditions need to adapt their lives and make changes to overcome these challenges. Commonalities include recognising symptoms and taking appropriate actions, using medications effectively, managing complex self-management regimens, making difficult lifestyle adjustments and developing strategies to deal with the psychological consequences of the condition (Strauss et al., 1984; Wagner et al., 2001).
Whitemore and Dixon (2008) found that the process of adapting to life with chronic conditions was complex and multifactorial. Numerous factors including treatment side effects, a progressive or uncertain condition trajectory, co-morbidity, bad days, financial hardships and interpersonal/environmental challenges contributed to a disruption or difficulty in the process of adapting to life with a chronic condition. Days of adjusting, inner peace and positive self-worth were intermixed with days of struggling, frustration and isolation for many participants. Participants were faced with ongoing emotional, physical and spiritual challenges that required attention.
In a qualitative study, Kralik (2002) identified the process ‘extraordinariness’ and ‘ordinariness’ as central to adjusting to a life with chronic conditions. Extraordinariness was a phase of turmoil and distress while the ‘ordinary’ phase involves incorporating chronic condition into their lives. Transitions in chronic condition experience involve movement from extraordinariness to ordinariness and sometimes back again and were found to be processes that are nonlinear, sometimes cyclical and potentially recurring throughout a woman’s life and distress.
Different socio-economic conditions, health systems and social support in different countries may affect the experience of chronic illness. To date no study on the experience of chronic illness in Ireland was found. This study explored the experiences of people with varying chronic conditions in order to find how their experiences compare with those of people elsewhere.
Methodology
Aim
The aim of this study was to explore the experience of people living with chronic illness among a group of Irish patients.
Design
A qualitative descriptive design, as described by Sandelowski (2000) was used in this study.
Participants
The target population was adults with chronic illness (as diagnosed by a doctor) and able to take part in the study. Those with severe mental impairment (as assessed by their clinical manager) were excluded. Participants were recruited from a local community health service, whose manager provided a list of willing participants to the researcher (1st author). Twenty-four willing participants were contacted by telephone and 19 agreed to take part, after the study was explained to them. The participants’ age ranged between 18 and 70 and their conditions varied from Parkinson’s disease, multiple sclerosis, rheumatoid arthritis, chronic pain syndrome to cancer.
Method of data collection
Focus groups were selected mainly because they are effective in getting people to share their experiences, as the aim was to explore commonalities and differences between their accounts of their conditions. The interactive nature of focus groups was attractive as it was anticipated the perceptions of some would be endorsed or negated by others, thereby producing a fertile debate on the topic of chronic illness.
Two focus groups were conducted with 10 (seven women and three men) and 9 (seven women and two men) respectively, and lasted approximately 90 min each. The first 15 min were used for introductions and for facilitating them to settle as a group. The researcher (1st author) initiated the discussion, asked questions, elicited responses and encouraged conversations. A general question about what the experience meant for them and how it has affected their lives was used as an introduction to the focus group interviews. Participants were encouraged to talk freely about their experiences. The facilitator’s role was to ask for clarifications, examples and explanations. The interviews were tape-recorded, with permission from participants. Data were collected in 2008.
Ethical considerations
Ethical approval was granted by the appropriate Regional Ethical Committee. Signed, informed consent was obtained from each participant before taking part in the study.
Data analysis
Data analysis followed the steps described by Braun and Clarke (2006), which consisted of: familiarising oneself with your data, searching for themes, reviewing themes, defining and naming themes and producing the report. The transcripts of the two focus groups were read and re-read by the first author. The process of coding the data involved systematically working through the data giving equal and full attention to each data item. The researcher created groups of data extracts by cutting extracts from the transcribed data, and sorting them into bundles. The extracts were then coded for what the researcher considered was being said or referred to by the participant. After all the data were initially coded and collated, the analysis involved considering how different codes combined to form overarching themes.
To enhance the credibility of the findings (Lincoln and Guba, 1985), reflective diaries were kept by the first author and the content was discussed with two other team members. Through discussions, personal biases in terms of beliefs, attitudes and perceptions were thus brought into the open. The other two researchers also sampled some transcripts. Differences in interpretations were resolved through discussion. The final version of the findings represents the consensus reached by the three researchers.
Results
Participants talked freely about their experiences. It was clear that, while their conditions and situations were varied, a number of common themes were evident from their narratives. These were:
a sense of loss; feelings of anger and frustration; uncertainty and stress and adapting to a ‘new life’.
Themes and sub-themes.
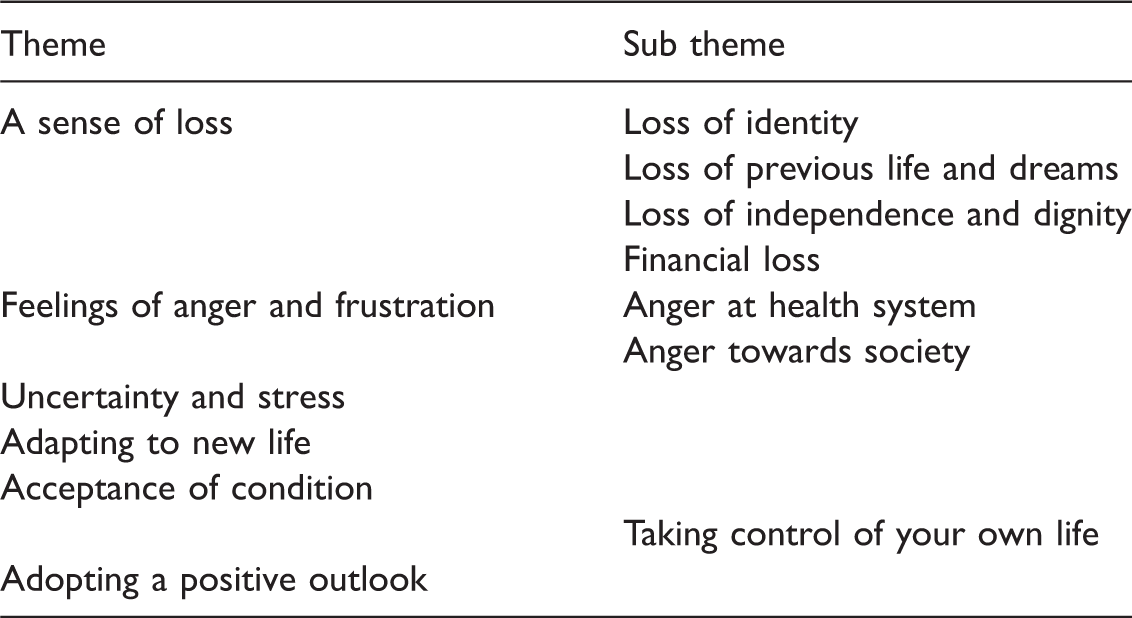
A sense of loss
Most of the participants experienced loss in varying forms throughout the time that they have lived with chronic conditions. The sub themes were ‘loss of identity’, ‘loss of previous life and dreams’, ‘loss of independence and dignity’ and financial loss.
Loss of identity
Several of the participants shared their experience of losing their sense of identity after being diagnosed with chronic conditions. They believed that because of their condition, people saw their condition or disability first and the person next. All of a sudden I’m a patient, I’m a woman with named condition, do you know what I mean? I felt that I didn’t want to be identified like that. And they actually sit down and talk to you man to man, it’s not like you’re just another patient and you know when you sit down that he’s looking at you and eye contact and he’s asking you like how did you get on today or what was your situation.
Loss of previous life and dreams
Many of the participants felt that they had ‘lost’ their previous lives and that the life they lived now was different to the one they had experienced before developing their present condition. This was experienced as difficult and involved learning new ways of achieving normal everyday activities. The loss of their previous lives brought with it feelings of sadness accompanied by loss of confidence and dignity. This sense of sadness at the loss emerged strongly from many participants: I can’t do a lot of the little ordinary things anymore that I used to be able to do. I’ve been going to hospitals for the past 26 years. I have a condition which means I cannot do what I once loved, and I did everything horseriding, swimming, hockey everything. But now I’m at the ripe old age of 37. I’m hoping to get my health right and I have
Loss of independence and dignity
Chronic condition can sometimes be accompanied with loss of musculo-skeletal functions, which can lead to loss of independence in different ways. This loss of independence resulted in loss of dignity. Unfortunately I’m actually at a stage that I actually can’t do the things that I used to be able to do, so my husband has to do a lot of things. You go in raw, just imagine yourself with no esteem … you’re depending on medical people to tell you the best things for you, as I said you’re skinless, headless and you don’t know where to turn.
Financial loss
Several of the participants found that living with chronic conditions had a financial impact on their lives. This loss of finance was brought about by having to pay for private tests and treatment because many participants felt that they simply could not wait until they were called for public appointments (Free State care). As the following narratives demonstrate, this placed considerable strain on individuals: I realised that the only way I was going to get seen quickly was to pay privately … … So then this year I actually nearly collapsed with pain … and I just said to my husband I can’t do this, so we’re going to have pay … I was throwing money out the window. When I went out the door I was no better than I went in.
Feelings of anger and frustration
Many of the participants experienced feeling angry at certain stages throughout their conditions. This anger was predominately directed at the health system, towards society and towards themselves.
Anger at the health system
Participants held varied and diverse views towards the health system. Many of these views were negative. Some participants felt that they had to wait for a long time to receive any treatment: I was all the time begging them can I have any exercises … I just felt I was at home wasting away, no exercises, no physio, no nothing, in severe pain, … they said they’d call me and I’m still waiting and that’s years ago. Well, I waited seven months to be diagnosed with cancer and because of the delay it’s terminal now. Whereas, if I would have been seen right away, it wouldn’t have spread to other organs.
This system of fragmented treatment resulted in some participants not knowing whom to turn to when they needed help.
Most of the participants wanted a community-based support service that could offer a means of sharing their experiences, having somebody local who they could talk to about their condition, the possibility of making friends and also vital medical treatment and advice. It’s just to have something away from the hospital … It’s a community-based thing to kind of wean you off the hospital. Like after we’ve dealt with the hospital and rather than just cutting you off, it is going to have a kind of a stepping-stone.
Anger towards society
Several participants felt anger towards certain attitudes they experienced from society. They felt that some people labelled them, which they hated. One woman felt that some people blamed her for the condition. Several chronic conditions are linked to lifestyle choices such as heart disease and because of this people sometimes feel that the person with chronic conditions has done something or not eaten healthy during their lives to develop the condition: Right ya, if I trust in angels and if I had juiced my fruit and eat my broccoli this whole hippy dippy new age stuff, so if you have [named condition] it’s because you’ve brought it on yourself. But when I look back I think for God’s sake what were you thinking, why didn’t
Uncertainty and stress
Having a long-term condition was perceived as having a significant impact on their lives. Not knowing how the condition would affect the participants and their families, now and in the future, caused uncertainty. The condition itself was a source of stress, including worries about getting worse, suffering a recurrence, side effects of medication and contracting additional conditions. Not knowing whether it would be possible to continue working and manage the home without help contributed to the stress. Not knowing how the disease would affect the participants and their families caused considerable stress. Several participants discussed the condition as stressful: But there’s also an awful lot of stress going on, you have your knee or whatever, or whatever your one thing is, so there’s a huge amount of stress going on around that and having somebody to talk it through and work all the things around it out help you is really important.
Adapting to a ‘new life’
The long process of accepting life with a long-term condition entailed confronting the self, personal actions and others. Getting on with life meant incorporating the changes brought about by the condition. The narratives communicated a reality in which the participants tried to compose a new picture of themselves and their life worlds. Adapting to a new life involved the ‘‘acceptance of the condition’, ‘taking control of own life’ and ‘adopting a positive outlook on life with chronic illness’.
Acceptance of condition
A life with chronic conditions had taught them to recognise and value what they had, and had made clear to them what was important in life. Most of the participants appeared to have accepted their condition; for several people this acceptance took a long time and was a difficult process. Their daily struggles are reflected below: I actually really, really feel that I’m working with this condition, some days not so well and some days I’m getting there. This is an unknown quantity, I can’t see tomorrow what will happen, I might have a huge flare up or whatever, but I seem to be going through a very stable time because several of my friends have remarked and I hardly noticed it myself, oh you’ve a spring in your step. I seem to be coping better and I’d say ‘yes I am’. I didn’t go in expecting a miracle and anybody who does; they may as well leave now if you expect miracles.
Taking control of your own life
It was very important for the participants that they had control over their own lives. This included values such as independence, self-responsibility and self-control. Living with chronic conditions had taught them to recognise and value what they had and what was important in life. But the participants wanted to overcome these difficulties and take control of their life. One participant explained how she had to work hard to learn and adapt to a new way of life but now she considered that she had claimed back some control: And I had to work really hard to have to learn a new way of life, a new way of existence. I mean to look at me you wouldn’t even know that there is anything wrong, I can’t do a lot of the normal things anymore that I used to be able to do, but I can do other things; I have control now. I’ve got much more control and much, much better Instead of taking something like 25 bloody tablets a day I’m down to about 14 or 12. I’ve actually cut down considerably but I come off slowly … I’ve come down and down and I will get down further. I think one of the very important things that [Named service] has done for me is to help me live with the pain in a more acceptable manner and not to let the pain run me, I’m running the pain.
Adopting a positive outlook on life with chronic illness
An overwhelmingly positive attitude towards the present and the future was described. The narratives were summed up with the words, ‘Ah there’s more people worse off than me’.
The participants demonstrated an overwhelming determination to survive and get on with living their lives. They appeared to have placed a high priority on living as best they could and getting the most out of life. They appreciated the importance and support of partners and family. One participant shared her wish to simply be there for her family: But that I would be able to keep going, I have a nine year old daughter, I would like to be as good as I can mentally as well as physically to rear her and to have a good life with my husband. … a struggle and trying to fight this condition and trying to find a new way of existing, a new way of working to keep myself going. So I was limited, my husband was very supportive, he was very good, and he would do a lot of cooking and do a lot of cleaning and that. I suppose in some ways I would like to be as independent as possible … because I used to love it even though I’m heavy I loved walking, walking the beach, walk in the forest and you’d miss that.
Discussion
Discussion of findings
These findings, and those from previous studies, show that living with chronic illness has a significant impact on people’s lives. The 4-stage process, developed by Kralik (2002; familiar life, the ending, in limbo and becoming ordinary), were all present in the findings of this study. They all had a different life (before diagnosis) with which they were familiar with. They recognised that as this life changed, they experienced a number of losses. This stage was characterised by disruption, uncertainty, anger and frustration. The transitory period in which they tried to find their way, and make sense of their illness and their changed life, was particularly difficult. Eventually, most adapted to their new life (which changed constantly as the illness ran its course), but not totally without some of the reactions and emotions present in the earlier stages.
Although most of the findings have been reported before (Lundman and Jansson, 2007; Whitemore and Dixon, 2008
Financial loss is not generally studied from patients’ perspectives; the focus is mostly on the economic cost of chronic illness for governments. Strauss et al. (1984) showed that chronic conditions can be expensive for an individual. This depends, of course, on the country’s health system and the extent to which individuals or the State pays for health and social care services. In countries such as Ireland, where there is both public and private provision, often people opt for paying for private care when they are dissatisfied with public services.
Participants were also frustrated with the lack of comprehensive health services and the fragmented nature of health care for people with chronic illness. Mullaney (2007) pointed out that the current models of care in Ireland do not meet the care needs of those with long-term conditions. This is not a problem for Ireland only. The World Health Organisation (2002) highlights the fact that primary health care is oriented towards acute problems. Government Irish Government policies (Department of Health and Children, 2008) refer to chronic conditions as the ‘burden’ of chronic illness. This has negative connotations and it is no wonder that these participants felt anger and frustration as they tried to ‘navigate’ their way through a health service not tailored to meet their need, and at great financial costs to themselves.
Limitations of the study
This study was limited in that it involved patients from one service only. While much in their experiences are similar to those of people elsewhere, it is not known whether their perceptions of services and the care they received would reflect the experiences of most people with chronic conditions in Ireland. A further limitation of the study is that with the small sample used it is difficult to generalise the findings to all Irish people with chronic conditions. A larger study is required for a more comprehensive investigation of some of the issues raised in this study. For example, we need to know more about the economic cost of chronic conditions for individuals, and whether some people who have less access to health services because they cannot afford to pay for them have a lower quality of life than those who can pay.
Implications for practice
The complex needs of those suffering with chronic conditions need to be addressed. The experiences of loss, anger, isolation, the significant impact on the person and those around them and the eventual acceptance of the condition need to be recognised by those offering a service to people with chronic conditions. Comprehensive psychological treatment, continuity of care and a person-centred service in the community for people living with chronic conditions should be provided where this is not the case. To avoid the fragmentation of services, service providers need to assess the extent to which their services meet the needs of patients and clients in an integrated way based on close teamwork between multi-disciplinary health professionals and direct access to services based in the community.
The study found that many people living with chronic conditions felt angry towards the health system, with society and towards themselves. Health care professionals should be aware of these feelings of anger and be supportive in addressing them. By listening to people and believing them, feelings of anger and frustration could be prevented or minimised. Above all they want to preserve their dignity and to be treated with respect.
The experience of isolation that was found in this study needs to be addressed, therefore social groups or clubs should be facilitated by organisations for people living with chronic conditions to help them socialise and support each other and their families. Individuals living with chronic conditions have a need to share their stories.
Further research is required on the experiences of people living with long-term conditions in other geographical areas, perhaps with a larger sample and if possible a more balanced gender mix.
Conclusions
The experience of chronic illness in adult patients was characterised by a strong sense of loss in many aspects of their lives. Despite facing a number of physical, psychological, social and financial obstacles, they showed a strong desire and willingness to come to terms with their predicament and to take back control over their own lives. It was also clear that support from family, partner and friends as well as from health professionals was crucial in helping them to make changes to their lives as they struggle to adapt to a new life.
It is important for health professionals to gain insight into people’s lives, from the perspectives of those who live with such conditions, in order to deliver care appropriate care.
Key points for policy, practice and/or research
It was clear that chronic illness affected people’s physical, psychological and social lives. They identified a number of personal losses, but felt strongly that they had to continue to make changes in their lives as they struggled to adapt to a new life. The contribution of partners and family members was crucial in this process of adaptation. Comprehensive psychological treatment, continuity of care and a person-centred service in the community for people with chronic illness should be provided, where this is not the case. To avoid the fragmentation of services, service providers need to assess the extent to which their services meet the need of patients in an integrated way. By listening to people, feelings of anger and frustration could be prevented or minimised.
Footnotes
Declaration of conflicting interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.