
Abstract
Background
Owing to the loss of autonomy associated with aging, home-dwelling older people often need the support of family and friends, particularly of a family caregiver whose demanding role can have negative health consequences. The empirical literature reports that some caregivers are resilient and continue to grow and develop, whereas others have difficulty coping with the role and suffer psychological distress.
Aims
The aim of this study was to examine the contribution of personal and contextual factors to the resilience of female family caregivers of home-dwelling functionally or cognitively impaired older people in Lebanon.
Methods
A predictive correlational design was used. The study was conducted with a cohort of 140 female primary family caregivers cohabiting with an older person aged 65 years or over. Data were collected through home-based structured interviews.
Results
Four factors were shown to be significantly associated with caregiver resilience: problem-focused coping strategies, emotion-focused coping strategies, sense of self-efficacy and caregiver meaning of caregiving.
Conclusion
The study offers potential priorities for nursing interventions aimed at promoting caregiver resilience. The results enable the creation of the foundations of a transferable contextual theory of resilience among female family caregivers in Lebanon.
Keywords
Introduction
In the Western world, numerous studies have been conducted on the family caregivers of home-dwelling older people. The majority of these caregivers are women (Torres Tailfer, 2010). The studies have brought to light the difficulties that caregivers face and the precariousness of their state of physical and mental health (Mannion, 2008; Timothy and Ginger, 2008). Other works have shown, however, that caregiving for an older person at times offers the caregiver opportunities for self-development, as well as challenges that can elicit satisfaction and gratification (Machamer et al., 2002).
In Lebanon, very few studies have been carried out on family caregivers, despite the fact that caregiving by the family for a home-dwelling physically or cognitively impaired older person is more and more frequent and constitutes, as it does in European and North American countries, a chronic stress situation. An 18-month longitudinal study conducted in Lebanon (Séoud et al., 2006) on 152 female family caregivers indicated nevertheless that, although the majority of women caregivers complained of a deterioration in their state of health, nearly half saw their state of health stabilise or improve. These women caregivers seemed to adapt to the sources of chronic stress that they faced, despite the deterioration of their older relative’s condition and the increasingly demanding care that they had to deliver.
People who manage to adapt to experiences of continuous stress are considered to be resilient (Gaugler et al., 2007). Various disciplines have examined the concept of resilience, which is defined as the capacity to succeed, live and develop positively and in a socially acceptable manner despite stress or adversity that normally carries a severe risk for negative outcomes (Vanistendael, 1998). Studies have demonstrated the impact of resilience on health, and described resilience as a potential factor in the maintenance (Hardy et al., 2004) and improvement of wellbeing (Bonano et al., 2007; Hegney et al., 2007) and health (Tusaie et al., 2007).
The concept of resilience brings new considerations to the theoretical approach often used in the study of caregiving, particularly in the United States, that is, the stress and coping model. According to this model, all caregivers faced with significant stress generally react by seeking ways to manage it (Lazarus and Folkman, 1984). The concept of resilience goes beyond stress management in that resilient people learn from situations and feel more empowered to meet challenges. In fact, what seems to distinguish resilience from coping is that the latter arises in response to a specific stress situation and, unlike resilience, does not imply a life project beyond the event (Manciaux, 2001).
Resilience seems to entail a constellation of personal and contextual factors (Ahern, 2006; Tusaie and Dyer, 2004). Numerous European and North American studies have examined the contribution of these factors above all among children, adolescents, adults and older people (Bonano et al., 2007; Friborg et al., 2005; Steinhardt and Dolbier, 2008; Tusaie et al., 2007). Despite the fact that taking care of a home-dwelling older person is considered a chronic stress situation, little is known about the resilience of family caregivers and these associated factors.
Background
In light of the theoretical and empirical literature reviewed, certain personal and contextual factors seemed to warrant consideration as potential predictors of individual resilience among female family caregivers in Lebanon. Knowledge of their impact would allow the planning of nursing interventions to foster the resilience associated with family caregiver health and wellbeing. In this regard, in the empirical studies of resilience carried out to date, Ataie et al. (2008) and Jonker and Greeff (2009) have observed a significant association between resilience and family relations as a contextual factor. Moreover, although social support from family and friends has been one of the contextual factors most widely investigated for its potential contribution to the phenomenon of resilience (Hegney et al., 2007; Hildon et al., 2008; Steinhardt and Dolbier, 2008; Ungar et al., 2007) this factor has never been considered as a predictor of resilience among family caregivers of older people outside of the American context. Any study of resilience in the Lebanese context could not overlook this variable, given that support is an integral part of daily life and household ritual. Such support is provided in particular by members of the extended family, friends, and neighbours who are considered to be friends and, at times, part of the family.
Regarding more specifically cultural beliefs, as far as we are aware, no study carried out on family caregivers has ever documented the potential link between resilience and the meaning of caregiving. In the Lebanese context, taking care of an aging relative springs from the intergenerational transmission of learning. Female family caregivers take care of older people in order to conform to social norms, but the meaning they ascribe to caregiving and its contribution as a factor of resilience remain to be determined.
As for the relevant personal factors to consider in the study of resilience, although some have been taken into account in certain American studies (Ataie et al., 2008; Wilks, 2006), they have not been examined in any other context. It is essential, therefore, to gain a better understanding of these before planning any nursing interventions aimed at fostering the resilience of this target group in Lebanon. More specifically, two of these factors, namely the use of coping strategies such as humour, relaxation, positive thinking, and social activities to deal with stress and sense of self-efficacy, deserved consideration on account of the fact that they could be the focus of learning throughout one’s life and could be modified through intervention. In a few qualitative studies, these factors were considered by respondents to be personal factors of resilience (Cameron and Brownie, 2010; Harris, 2008; Hildon et al., 2008; Jonker and Greeff, 2009; Ross et al., 2003; Tusaie et al., 2007); the results of these studies, however, have been mixed.
In addition, sense of self-efficacy, which is considered a personal resource, has been the focus of growing attention in studies of family caregivers of older people (Gignac and Gottlieb, 1996; Zeiss et al., 1999). These studies have revealed an association between caregiver perceived personal efficacy and resilience. However, here too, results have not been conclusive (Hardy et al., 2004) and further research has been recommended on this variable’s contribution to the phenomenon of resilience (Gaugler et al., 2007).
In summary, to our knowledge, no study had ever been conducted on Lebanese female family caregivers with a view to determining the factors that might influence individual resilience. A better understanding of the contribution of personal and contextual factors could offer nurses the knowledge required to intervene in the aim of promoting resilience in the face of adversity and thus improving the health of the caregiver (Ahern, 2006).
In light of the above, we undertook a study to examine the contribution of personal factors, including coping strategies and self-efficacy, and of contextual factors, including family relations, perceived social support from friends, and the meaning of caregiving, to resilience among female family caregivers of a home-dwelling functionally or cognitively impaired older relative in Lebanon.
Materials and methods
Design
A predictive correlational design was used to examine the association between resilience and, respectively, personal and contextual factors. The literature reviewed enabled the identification of a hypothetical empirical model of predictors of resilience among female family caregivers. More specifically, two sets of hypotheses were put forward. The first concerned the contribution of personal and contextual factors to resilience. The second regarded the effect of certain sociodemographic and clinical variables likely, according to the literature, to influence resilience and, therefore, worthy of consideration as control variables in the model. More specifically, these included age (Bonano et al., 2007; Wilks, 2006) and educational level (Bonano et al., 2007; Gaugler et al., 2007) of the female family caregivers, and level of functional impairment and frequency of behaviour problems of the cared-for older person (Gaugler et al., 2007; Rogerson and Emes, 2008). Indeed, previous studies have documented a positive relationship between age and resilience (Bonano et al., 2007). However, concerning the association between the level of education and resilience, published results are somewhat contradictory (Bonano et al., 2007; Gaugler et al., 2007). Moreover, it seems that health deterioration and behaviour problems of the older parent, both sources of chronic stress for the caregiver, show a negative relationship with resilience (Gaugler et al., 2007).
Figure 1 illustrates this hypothetical model and the direction of the hypothetical relationships.
Hypothetical empirical model of predictors of individual resilience.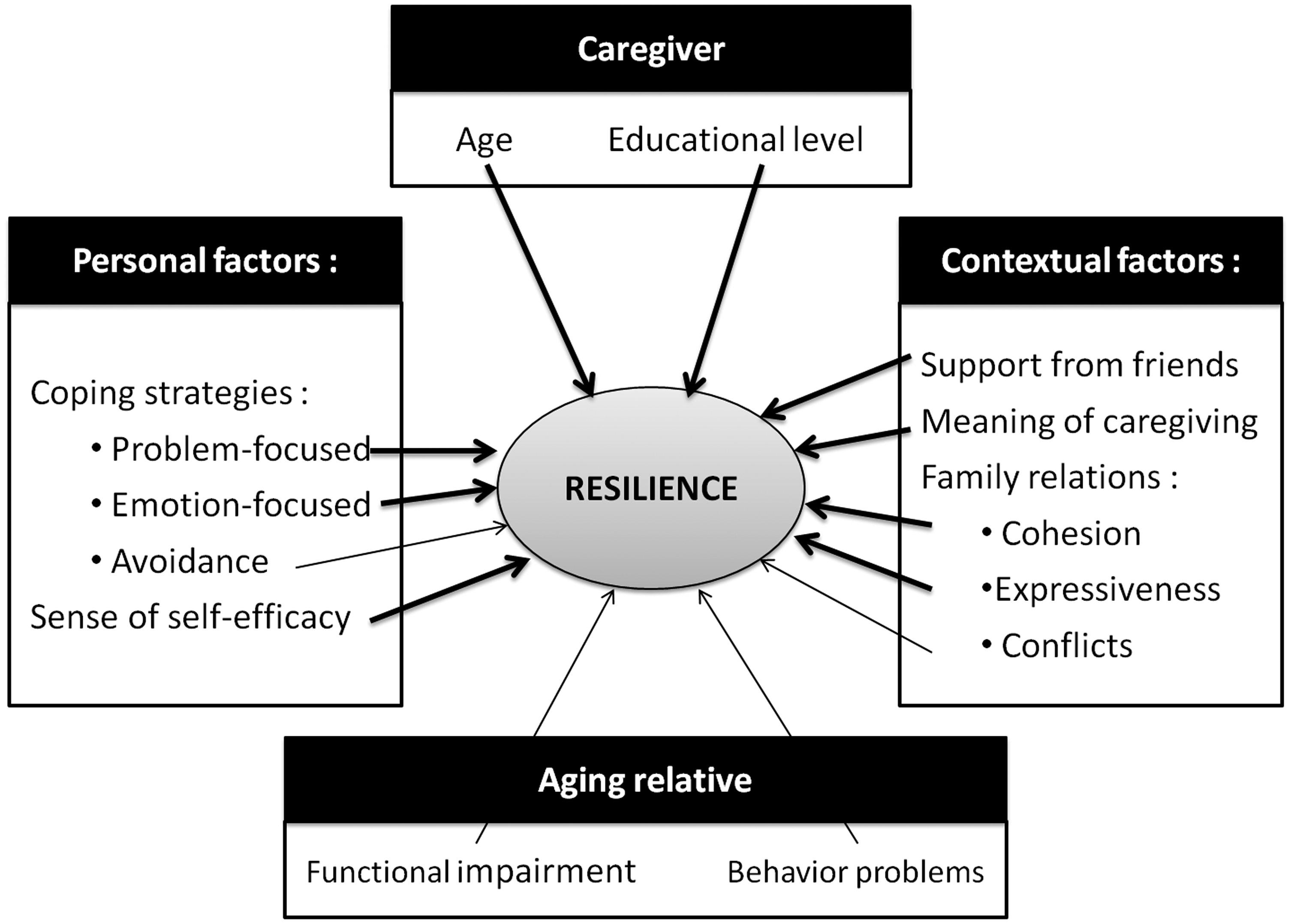
Sample
Statistical power analysis (Laurencelle, 2007) was used to determine sample size. In this regard, it was estimated that for statistical power of 0.80, a significance level of 0.05 and a moderate effect size (0.15) on caregiver resilience, a sample of 140 female family caregivers was needed. These caregivers were recruited following a convenience procedure and a snowball strategy. To be part of the sample, the women caregivers had to be Lebanese, 18 years old or over, fluent in Arabic, the primary woman caregiver for at least six months – that is, the person who provided the most support, help and care to a functionally or cognitively impaired relative 65 years old or over – and cohabiting with the older person at home. Taking care of more than one older person and manifesting cognitive impairment limiting the ability to complete the questionnaire were exclusion criteria. In all, 165 women caregivers were recruited, of which 25 were excluded from the study for not meeting the inclusion criteria.
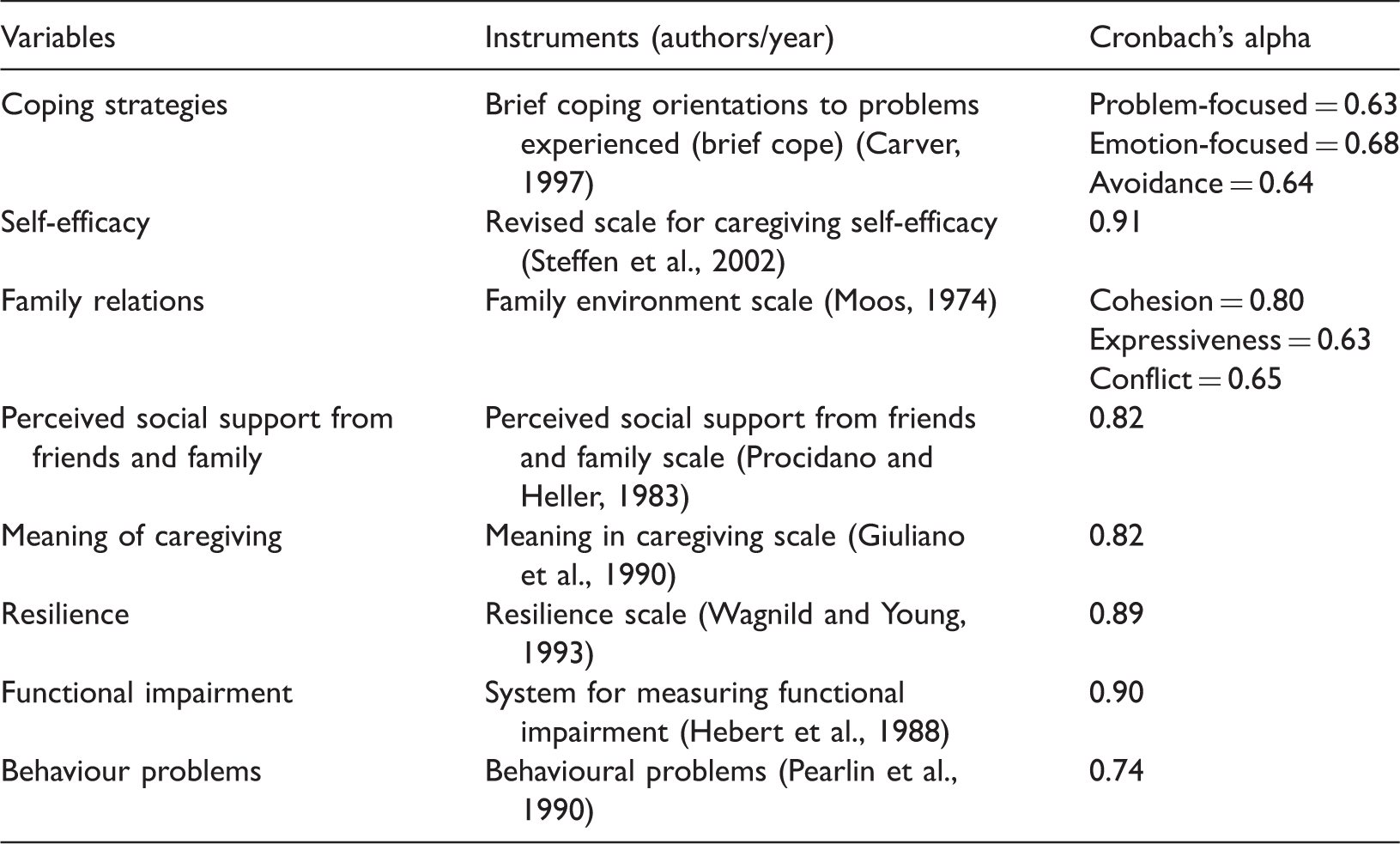
Instruments of measure
Instruments for measuring the study variables.
Procedure
After receiving approval from the Ethics Review Board (no. 11-038-CERSS-P), the researchers carried out the pilot on five female family caregivers and conducted the interviews thereafter. These interviews took place at the homes of the female family caregivers in a room away from the cared-for relative and lasted on average 45 minutes. They were conducted by female interviewers who were trained in using the interview guide and administering standardised questionnaires, and who were supervised by the principal investigator.
Statistical analysis
SPSS version 19 was used for data entry and statistical analysis. A descriptive analysis was used to examine the sociodemographic characteristics of caregivers and their relatives, and to measure all variables. To identify the predictors of resilience, hierarchical regression analyses were performed.
Results
Sociodemographic and descriptive characteristics of the women caregivers and their cared-for relatives
Sociodemographic characteristics of the female family caregivers (N = 140).
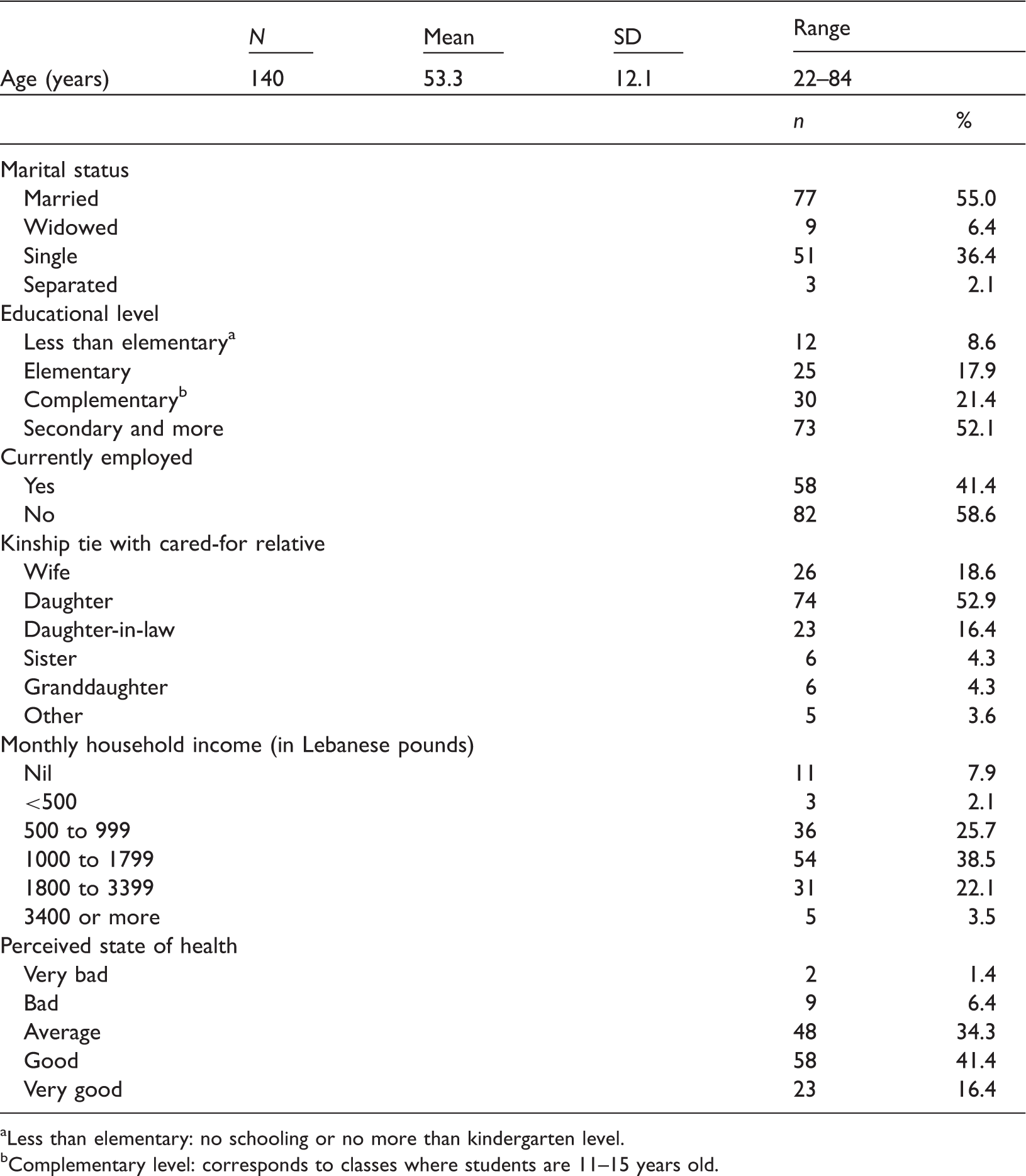
Less than elementary: no schooling or no more than kindergarten level.
Complementary level: corresponds to classes where students are 11–15 years old.
Regarding the older people receiving care, they were for the most part women and widowed. They had a mean age of 81 years. Their state of health was perceived by the female family caregivers as mostly bad (40%) or average (26.4%).
Descriptive results regarding control, personal and contextual variables
Descriptive statistics on principal variables under study.
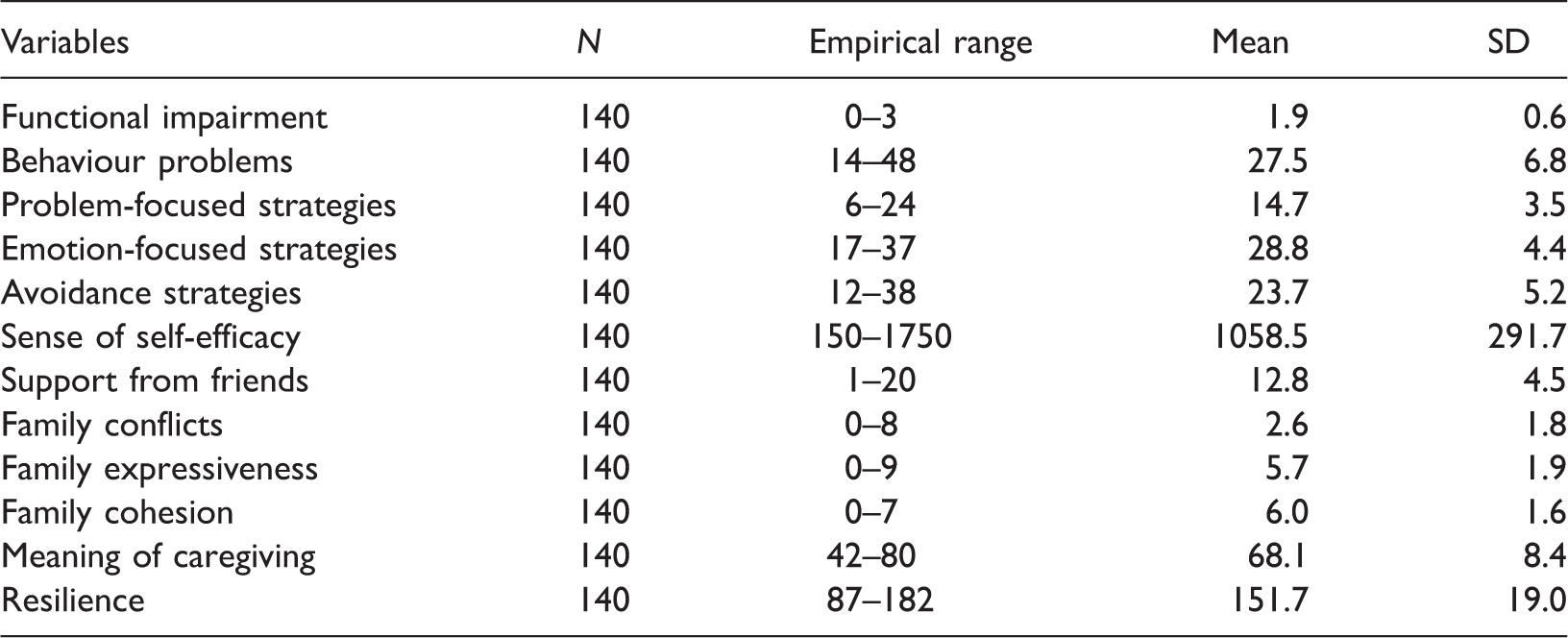
The female family caregivers made greater use of emotion-focused and avoidance coping strategies than of problem-focused strategies, and ascribed a positive meaning to caregiving. They also reported a moderate to moderately high level of sense of self-efficacy in taking care of their aging relative. Moreover, the caregivers perceived good support from friends and reported few family conflicts.
Regarding the cared-for relatives, most needed partial or total help with activities of daily living and instrumental activities of daily living and presented few behaviour problems.
Predictors of resilience
Hierarchical regression analysis of predictors on resilience (N = 140).
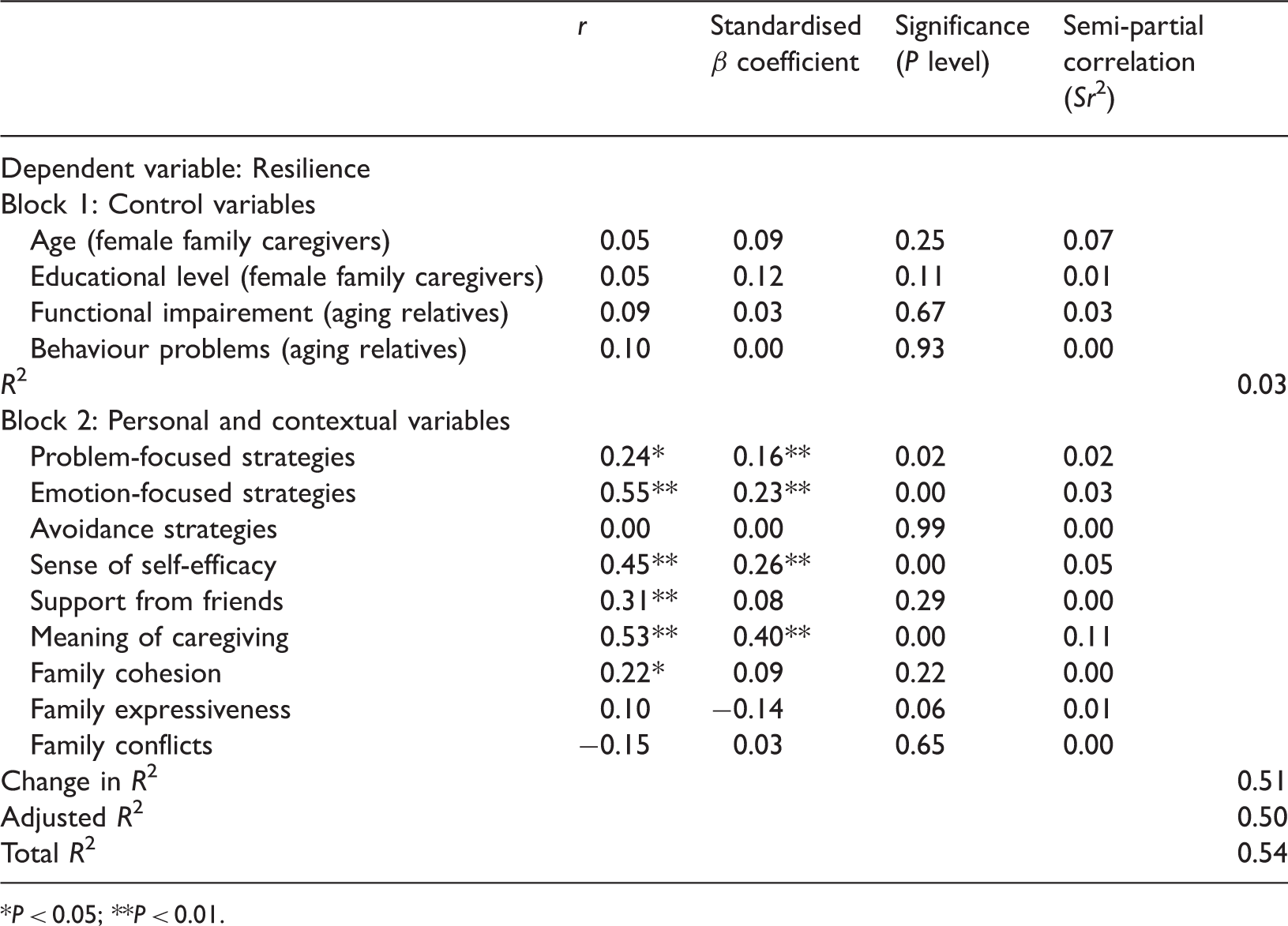
P < 0.05;.
**P < 0.01.
Meaning ascribed to caregiving was the factor that most explained the variance in resilience, followed by sense of self-efficacy. Two types of coping strategies, namely problem-focused strategies and emotion-focused strategies, also made a significant contribution in this regard. Accordingly, the higher the degree of self-efficacy perceived by women caregivers and the more they ascribed meaning to caregiving, the higher their level of resilience. Also, the more women caregivers used problem- and emotion-focused strategies, the higher their resilience level. As for the control variables, none proved significantly related to resilience.
Discussion
The aim of our study was to examine the contribution of personal factors, namely the use of coping strategies and self-efficacy, and of contextual factors, namely family relations, perceived social support and meaning of caregiving, to resilience among female family caregivers of a home-dwelling functionally or cognitively impaired aging relative in Lebanon. The choice of these variables was informed, on the one hand, by the results and limits of the literature reviewed and, on the other hand, by the fact that these variables were consistent with Lebanese culture, sensitive to societal beliefs and habits, and amenable to change via a nursing intervention.
The results of the study confirm the association between some of the variables in our empirical model and resilience, but show no association for other variables. Indeed, the positive association between the use of problem-focused coping strategies and the use of emotion-focused coping strategies, respectively, and resilience among female family caregivers was confirmed. Although the descriptive results of our study indicate that female family caregivers use emotion-focused strategies much more than problem-focused strategies, both types proved to be associated with resilience among women caregivers. The fact that the female family caregivers in our study resorted more often to emotion-focused strategies might be related to the beliefs of Lebanese people, for whom faith is a source of peace of mind and a means of spiritual renewal that provides a sense of strength (El Kahi et al., 2003). Moreover, religious principles and social norms constitute in Lebanon the bases of family solidarity and mutual help (Mourad, 2008). These last two factors, however, were not explored in this study for two reasons. On the one hand, religion and social norms have not been sufficiently documented in the literature as being linked to resilience; on the other, they represent in Lebanon highly sensitive subjects of discussion if not topics of potential conflict and discord.
The positive association between a strong sense of self-efficacy and resilience among female family caregivers was also confirmed. Indeed, a strong belief in one’s self-efficacy confers confidence in one’s abilities, which in turn diminishes stress and contributes to wellbeing (Bandura, 1997). Accordingly, the stronger one’s sense of self-efficacy, the higher the objectives that one sets for oneself and the stronger the commitment to one's achievement (Bandura, 1982, 1997). This could, in part, explain resilience.
Where the contextual factors are concerned, only one positive association emerged with caregiver resilience and it was with the meaning of caregiving. This is in line with the study by Ross et al. (2003), in which one of the characteristics of resilient people was having a philosophy of life related to the meaning of caregiving. Furthermore, ascribing meaning to events constitutes one of the pillars of resilience (Vanistendael, 2001). This perspective converges with the idea to the effect that when one manages to find meaning, one acquires the ability to deal with suffering and to transcend it (Frankl, 1984). Indeed, over one’s lifetime, everyone desires stability despite the fact that one is exposed to change. In order to regain stability, one seeks to ascribe meaning to this change (Baumeister and Vohs, 2002), a meaning strongly tied to one’s culture and beliefs (Wong and Wong, 2012). However, the fact that the factors considered in this study accounted for only 54% of the variance in caregiver resilience indicates that the model could be further refined with the addition of other potentially more explanatory factors.
Our study, however, presents certain limitations. Owing to the fact that ours was a convenience sample, the significant results obtained cannot be generalised to all female family caregivers of a home-dwelling aging relative in Lebanon. Moreover, the results showed that more than two-thirds of the female family caregivers in the sample had a moderately high to high level of resilience. Social desirability might have played a role in these results, especially as, in general, the female family caregivers knew the interviewers. Despite the fact that the items of the questionnaire were examined to make sure that they were not overly sensitive to social desirability, we recommend in future studies the inclusion of a social desirability scale in the battery of instruments used, such as the one developed by Crowne and Marlowe (1960).
Another limitation concerns our choice of instruments of measure. In the absence of Lebanese norms and tools, North American instruments were selected and translated into Arabic. Although we complied with the back-translation method (Haccoun, 1987), some items might have been less well understood than others by the female family caregivers, raising questions about the cultural adaptation of the instruments. This could explain in part the poor internal consistency obtained in our study for certain instruments of measure, which could have influenced the validity of the results concerning these variables.
Despite these limitations, our study enabled the creation of the foundations of a contextual theory of resilience among female family caregivers of a home-dwelling older person in Lebanon. The results also identify priorities for nursing practice, particularly regarding the planning of interventions for female family caregivers aimed at promoting their resilience and, in turn, their health. Identifying, mobilising, valorising and, if needed, developing the strengths and resources of the family and the environment (Ionescu, 2011) are at the heart of nursing intervention. The four significant predictors of resilience to emerge from the study are elements that could be developed through psycho-educational nursing interventions. For example, nurses could support family caregivers in seeking solutions for dealing with the effects of the caregiving situation through reinforcement of coping strategies already used, or learning of new problem – or emotion-focused coping strategies. In this regard, knowing that a sense of self-efficacy – a key predictor of resilience – is considered the chief prerequisite for behavioural change, it is by helping caregivers acquire or reinforce this quality that nurses could bring them to manage their older relatives with greater confidence and thus become more resilient. Finally, nurses could also strengthen the meaning that family caregivers ascribe to caregiving by helping caregivers interpret or perceive caregiving and its scope in a different light. This, too, could help caregivers achieve greater resilience.
At a time when the population is aging and female family caregivers are being called upon to play an increasingly large role in taking care of aging relatives, the knowledge generated by this study is of high social relevance. Indeed, the four factors identified as predictors of resilience, namely problem-focused coping, emotion-focused coping, the meaning of caregiving and self-efficacy, are factors that could constitute the plot of an innovative nursing intervention focused on the strengths and growth potential of caregivers.
Key points for policy, practice and/or research
Research: foundations for a potentially transferable contextual theory of resilience among women family caregivers of a home-dwelling elderly person in the Lebanese context. Practice: leads for nursing interventions aimed at promoting resilience by modifying or strengthening the contributing factors identified. Policy: support policy for family caregivers.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this paper.
Funding
The authors received no financial support for the research, authorship and/or publication of this paper.
Acknowledgements
This study was supported by the Research Council of Saint Joseph University, Lebanon.