
Abstract
Background
Advance Care Planning (ACP) communication is difficult to implement in hospital. Possibly this has to do with the fact that the concept is not well tuned to the needs of hospital professionals or that they experience implementation barriers in practice.
Aims
The aim of this study was to investigate what is valued in having ACP conversations by hospital professionals (physicians, nurses, psychologists and social workers) and what they experience as barriers and facilitating factors for having ACP conversations with patients.
Methods
A Delphi study consisting of two rounds with respectively 21 and 19 multidisciplinary experts from seven European countries was organised. Data were analysed using content analysis and descriptive statistics.
Results
Participants agreed that ACP is valued mostly because it is seen to improve transmural continuation of care, emotional processing of the loss of a patient, and serenity at the end of life. Reported barriers are patient characteristics blocking patient-centred communication and a lack of knowledge to have these conversations. An important facilitator is multidisciplinary cooperation.
Conclusions
There is consensus by experts from different settings and countries suggesting that these results can theoretically be applied to hospital settings in Europe. This study reveals that hospital professionals value ACP in hospital practice, but that they encounter several barriers to its implementation.
Introduction
In Europe, 22% of adults could benefit from palliative care at the end of life (Connor and Sepulveda Bermedo, 2014). The hospital is an important care setting for palliative patients, as many palliative patients reside (Cohen et al., 2008; Department of Health, 2008; Van den Block et al., 2007) and die (Broad et al., 2013; Cohen et al., 2008; Flory et al., 2004; Gomes et al., 2012a, 2012b; Howell et al., 2010; Loucka et al., 2014; Marcucci and Cabrera, 2015; Wilson et al., 2009; Yang et al., 2006) in hospital. At such times, palliative patients receive treatments (e.g. radiotherapy) and forms of care (e.g. oxygen, intensive care unit (ICU)) that are more invasive than in other settings (Strom et al., 2017). Studies have shown shortcomings in meeting the needs of palliative patients and relatives in the acute hospital setting (Barbera et al., 2008; Ferrand et al., 2008; Goodlin et al., 1998; Phua et al., 2011; Plonk and Arnold, 2005; Teno et al., 2004; Walling et al., 2010; Weber et al., 2012; Zhang et al., 2012). Two important shortcomings are inadequate communication (Al-Qurainy et al., 2009; Ferrand et al., 2008; Gagnon and Duggleby, 2014; Goodlin et al., 1998; Phua et al., 2011; Plonk and Arnold, 2005; Reyniers et al., 2014; Teno et al., 2004; Walling et al., 2010; Weber et al., 2012; Zhang et al., 2012) and a focus on unrealistic cure and life-prolongation in this setting instead of focusing on quality of life (Al-Qurainy et al., 2009; Gott et al., 2009; Reyniers et al., 2014).
Advance Care Planning (ACP) communication might contribute to overcoming these shortcomings in the hospital setting (Al-Qurainy et al., 2009; Anon, 2015a, 2015b; Brinkman-Stoppelenburg et al., 2014; Houben et al., 2014; and see http://www.goldstandardsframework.org.uk/acute-hospitals-training-programme and http://webarchive.nationalarchives.gov.uk/20160805122006/http://www.nhsiq.nhs.uk/improvement-programmes/long-term-conditions-and-integrated-care/end-of-life-care.aspx). A systematic review by Brinkman-Stoppelenburg et al. (2014) shows that complex ACP interventions that include patient-health professional communication were found to result in preference-concordant care, an increased frequency of out-of-hospital and out-of-ICU care, and an increased compliance with patients’ end-of-life wishes and satisfaction with care (Brinkman-Stoppelenburg et al., 2014).
However, attempts to embed ACP in routine hospital care using relatively simple patient-or health professional-focused interventions have had only limited impact (Lovell and Yates, 2014; The SUPPORT Principal Investigators, 1995). Since Street and Ottman’s State of the Science Review (2006) recommended that studies should address the factors that affect the implementation of ACP, few studies have been published in this regard (Ahluwalia et al., 2014). When looking at the implementation literature, there are two important strategies to improve implementation. One strategy for successful implementation of any health improvement intervention is to understand what is valued about the intervention (Baker et al., 2001; Greenhalgh et al., 2004). Another strategy is to understand what the obstacles and facilitating factors are in respect of implementation (Baker et al., 2010; Grol and Grimshaw, 2003; Pantoja et al., 2014).
The aim of our study was to give an overview of the shared opinions of experts in the field in Europe concerning what they think is experienced as valuable about having ACP conversations in hospital for hospital professionals, and what they think hospital professionals experience as obstacles and helpful factors when they have ACP conversations.
The research questions (RQs) were the following: RQ1: What do experts think is valuable in having ACP conversations in hospital? RQ2: What do experts think are obstacles and helping factors for having ACP conversations in hospital?
Methodology
Participant characteristics
Experts recruited from four disciplines considered to have ACP conversations in hospitals (nurses, physicians, psychologists and social workers) from seven different countries of the European Union (EU), were purposively sampled (Hasson et al., 2000) according to their expertise in working with palliative patients in the acute hospital setting. Inclusion criteria were (a) working with severely ill patients in hospital for at least 5 years; or (b) studying the topic scientifically and having worked with severely ill patients in hospital for at least 5 years; and (c) being a certified physician, nurse, psychologist or social worker. Exclusion criteria were (a) not having had clinical practice; (b) having only worked on a palliative care unit; or (c) not having worked with or studied palliative patients in hospital for more than 2 years.
Data collection and analysis
Data in this study were collected and analysed following the Delphi survey technique (Hasson et al. 2000). The Delphi survey technique is in essence a series of questionnaires that is sent out consecutively to the volunteering participants (Hasson et al., 2000). Our first questionnaire asked the participants to respond to open questions; the second was then built upon the responses to the first. Successive questionnaires give participants feedback on the collective responses of the group, providing the opportunity for individuals to modify their judgements in light of this newly shared information (Hasson et al., 2000). The process builds on the qualitative responses of individuals and measures the group’s responses quantitatively. The process ends when consensus is reached, or when sufficient information has been exchanged (Hasson et al., 2000). Our study consisted of two rounds; the first (R1) lasted 8 weeks, the second (R2) 6 weeks, and R1 and R2 were spaced 8 weeks apart.
Data collection R1
In preparation for the first round in which experts were to be consulted, a series of open-ended questions was formulated based on previous research results of our research group (Vanderhaeghen et al., 2018). This was an in-depth content analysis based on grounded theory from interviews from hospital physicians, nurses, psychologists and social workers, all working with severely ill patients.
Composition of the Delphi panel in R1 and R2.
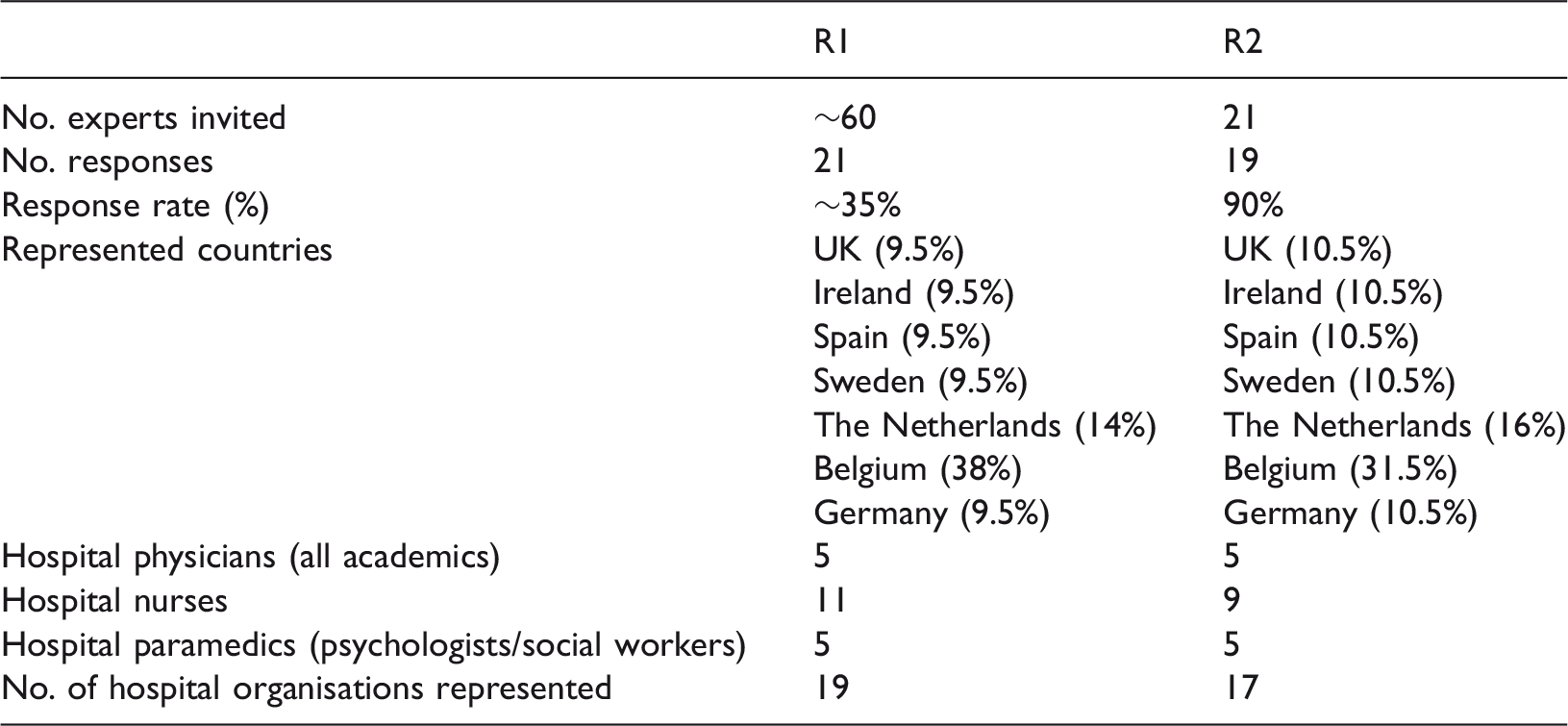
R1: Round 1; R2: Round 2.
Data analysis R1
The answers of the 21 participants were analysed using content analysis (Charmaz, 2006; Strauss and Corbin, 2015), supported thereby by software designed to analyse qualitative data (MAXQDA 11). The in-depth and sentence-by-sentence analysis resulted in eight important themes for RQ1.
Data collection R2
Aggregate scores and responses for 16 questions posed to the Delphi panel (n = 19) in R2.
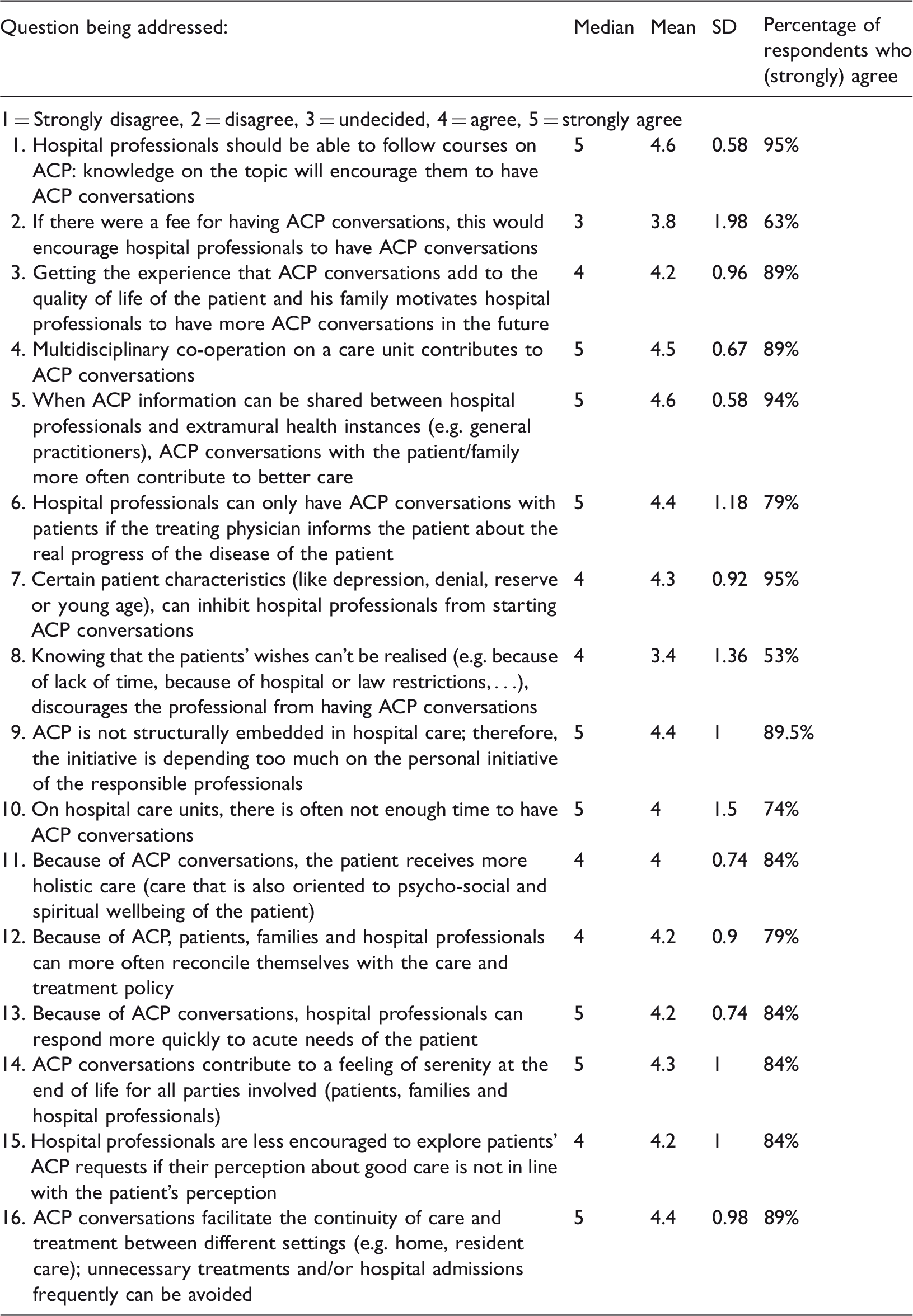
ACP: Advance Care Planning.
Data analysis R2
Of the 21 questionnaires distributed, 19 were sent back by email (90%). Table 1 shows important details concerning the characteristics of the panel of the second round. Before analysis of this questionnaire, the researcher (BV) checked whether participants made remarks concerning the formulation of any question. None were excluded, as all the respondents agreed with the given usage of the phrases. Descriptive statistics found that the distributions were mostly skewed, and a visual check confirmed that none were bimodal (two groups with a different opinion concerning a question). The median was chosen to represent the most typical value given by the panel for each item in R2 (range = 1–5). For every question a percentage of participants (strongly) agreeing was calculated, with a cut-off of 75% of participants (strongly) agreeing (marking 4 or 5). Next to these values, the mean and standard deviation (SD) were calculated for each statement.
Results
Results R1
First, the experts find ACP conversations in hospital valuable because they contribute to care that is holistic: when one explores values around care, this inevitably leads to care that is focused on the person as a whole. Second, ACP conversations are seen as valuable because they contribute to care that transcends the hospital walls; by looking at the future, care can be adapted to needs at home. Third, the experts agree that ACP contributes to knowledge on what to do when the patient is in crisis, because there is constant tuning to the needs of the patient. Professionals know better what the patient wants when he is unable to decide because of an emotional or physical crisis. Knowing what to do also helps to preserve serenity. According to the experts, there is a sense of control when a sudden, difficult situation occurs. In that way, emotional crises can be avoided for all parties involved. Furthermore, hospital professionals think ACP conversations help patients and families alike with the emotional processing of what is happening, because time for reflection is created. For RQ2, three important facilitators were mentioned by the experts. The first is continuous and accessible education concerning ACP. The second is multidisciplinary and extramural sharing of information; when necessary information can be shared with other disciplines, one can build on the ACP conversations from others. Third, the experience with ACP conversations (e.g. the experience that patients receive better care and are more satisfied with care) encourages professionals to have ACP conversations in other patient cases. Important obstacles are knowing that the ACP wishes will not be executed (e.g. concerning legal restrictions); patient characteristics like depression and denial (professionals are not convinced that ACP conversations are of benefit to these groups); not enough means (time, money, personnel) and barriers for attunement between the different parties, mostly because of fragmentation of care (e.g. transfers between care units).
Results R2
A clear consensus was found amongst the panelists for 12 out of 16 questions, with more than three-quarters of the experts agreeing with the stated questions, having a median and mean of ≥ 4 and SD ≤ 1, meaning that for those questions there were no answers that were strongly deviant from the scores that the majority of the group gave. For question 6 SD was >1, but >75% of respondents agreed and the mean and median were high. When looking at qualitative data, the most critical remarks speak in favour of having a physician who is open with the patient about the disease evolution: ‘If patients are fully informed, it is easier to talk openly.’ (translation from Dutch). For these reasons, we decided that sufficient consensus was found for this question.
Three questions (questions 2, 8 and 10), however, had an SD of >1, had rather low means and medians, and <75% of respondents agreed with the statement. The three least favoured statements were ‘If there were a fee for having ACP conversations, this would encourage hospital professionals to have ACP conversations’; ‘Knowing that the patients’ wishes can’t be realised (e.g. because of lack of time, because of hospital or law restrictions, …) discourages the professional to have ACP conversations’; and ‘On hospital care units, there is often not enough time to have ACP conversations’. Next to quantitative measures, qualitative data, which were gleaned from the remarks, also show that participants disagree. For example, for question 10, one participant feels the need to state that this is ‘absolutely true’. Conversely, someone else states that ‘There is felt to be no time; but there is … and much time is wasted for irrelevant things’. Given these outcomes, we decided to conclude that no consensus was reached for these statements.
Most consensus was found for questions 1, 5 and 7. Participants almost all agreed with the fact that hospital professionals should be able to follow courses on ACP, because knowledge on the topic would encourage them to have ACP conversations. They also agreed with the statement that when ACP information can be shared between hospital professionals and extramural health instances (e.g. general practitioners), ACP conversations with the patient/family more often contribute to better care. Furthermore, they believed that ACP conversations facilitate the continuity of care and treatment between different settings (e.g. home, residential care); because of ACP, unnecessary treatments and/or hospital admissions frequently can be avoided.
A total of 89% of panelists agreed with questions 3, 4, 9 and 16. An important perceived barrier is that ACP is not structurally embedded in hospital care. Therefore, the initiative is too dependent on the personal initiative of the responsible professionals.
Discussion
When answering RQ1, one could say that ACP seems of value for different reasons. First, ACP is seen to be an aid to easy continuation of transmural care throughout the disease process, which is seen to be of great benefit to patient care (questions 5 and 16). Second, ACP is seen to be of value because hospital professionals can respond more quickly to the acute needs of a patient. As reported in the qualitative survey of R1, knowing what to do in situations of crisis gives hospital professionals a feeling of control. This takes away tension and fear. With this in mind, it is not surprising that participants state that ACP contributes to serenity at the end of life for all parties involved (question 14, 84%). Another explanation is given in R1, where participants often mentioned the fact that they can accept the loss of a patient better emotionally when they have ACP conversations: they have more time for reflection about and the processing of the approaching death of a patient, which is seen as helpful.
When answering RQ2, an important result of this study is that there is strong consensus about the fact that certain patient characteristics have a discouraging effect on hospital professionals in respect of engaging in ACP conversations (question 7, 95% of participants agree). When we look into the detail of the qualitative data of R1 of the study, we notice that those characteristics appeal to professionals in two ways. Some patient characteristics (like age) appeal to their own ideas about good care. For example, when young patients ask for treatment to be stopped, this is perceived as not in line with their own convictions about what the ‘good’ decision is. Other patient characteristics like reserve, depression and denial appeal to the conviction that these patient populations are emotionally burdened by talking about existential themes. For this specific group, ACP is believed not to be useful in ameliorating the last part of life or preparing for a good death. These findings are in line with the results of a previous study by our research group (Vanderhaeghen et al., 2018) and with the findings of other studies that find that a subjective component (attitudes and convictions of professionals) influences ACP discussions and decision making, which inhibits patient-centred care (Bender et al., 2015; Visser et al., 2014a). This might lead to inequality in the ACP decision-making process, where patients receive their desired care and treatment more or less easily, depending on certain characteristics (Vanderhaeghen et al., 2018). With this in mind, another result worth discussing is the fact that 89.5% of experts (strongly) agree with the fact that ACP should be structurally embedded in care (question 9). When looking in detail at the qualitative responses of the study, certain experts think that when ACP questions are embedded in the daily routine, all patients are automatically included in an ACP trajectory. It is also mentioned as a way to be less dependent on communication between the treating physician and their patient: if it is considered normal that patients are addressed about their wishes for care and treatment, the decision to start an ACP process is less dependent on the treating physician. This view is supported by other studies as exemplified by a systematic review by Cooper et al. (2014). A limitation of this approach is that the convictions of professionals are not changed by being obliged to have these conversations; one cannot be forced to preserve an open attitude while exploring care and treatment wishes that are not in line with one’s own. Maybe raising awareness about personal blind spots and (subconscious) beliefs and wishes are more effective than the top-down installation of ACP in routine daily care.
Another important finding is that a lack of (continuous) training is seen as an important barrier: professionals report that hospital professionals do not have enough knowledge about ACP to conduct it in practice. This finding is in line with previous research (Alexander et al., 2006; Allen et al., 2015; Visser et al., 2014b).
Another interesting finding concerning the barriers for ACP conversations is the fact that some professionals think they have insufficient time for ACP conversations with patients, while others do not think that (question 10, <75% agree, SD 1.5). When looking in detail, nurses and physicians, especially, report the issue of time as an important inhibiting factor. Some suggest multidisciplinary cooperation as a means to cope with time pressure: social workers and psychologists often take up these conversations. In general, multidisciplinary cooperation is seen to be an important facilitating factor for ACP (79% of experts agree). This view is also supported by other studies (Trivedi, 2013; Visser et al., 2014b). While some would want to solve this by freeing budget for these conversations, this view is certainly not shared by most of the participants (question 2, 69% agree).
Conclusions
Studies show that ACP communication is difficult to implement in hospital (Lovell and Yates, 2014; The SUPPORT Principal Investigators, 1995). Possibly this has to do with the fact that the concept is not well tuned to the needs of hospital professionals or that they experience implementation barriers in practice. This two-round Delphi study, consisting of expert physicians, nurses, psychologists and social workers, shows that professionals value ACP because it is seen to ease the disease process in many ways: it contributes to transmural continuation of care, serenity, and emotional processing of the loss of a patient by hospital professionals. Reported barriers are certain patient characteristics blocking patient-centred communication about goals of care and treatment and a lack of knowledge (education) about these conversations. An important facilitator is multidisciplinary cooperation in a team where relevant information can be shared, and professionals can build upon previous patient communication with colleagues. Experts from different settings in different countries all agree upon these themes, suggesting that these results can theoretically be applied to hospital settings all over Europe. When measures are taken to ease the ACP process for hospital professionals, this knowledge can be taken into account.
We recommend that future research builds further on these insights, by quantifying the education needs, time constraints and other barriers and facilitators mentioned. This information could serve to determine priorities for hospital policy.
Key points for policy, practice and/or research
There is strong consensus between experts about the fact that certain patient characteristics have a discouraging effect on hospital professionals in respect of engaging in ACP conversations (e.g. patients of young age, patients in denial). These convictions might lead to inequality in the ACP decision-making process, where patients receive their desired treatments more or less easily depending on certain characteristics. When developing training, this knowledge should be taken into account. Experts strongly agree with the fact that ACP should be structurally embedded in care. Certain experts think that when ACP questions are embedded in the daily routine, all patients are automatically included in an ACP trajectory, which could be an interesting recommendation for policy makers. A limitation of this approach is that the convictions of professionals are not changed by obliging them to have these conversations; one cannot be forced to preserve an open attitude while exploring care and treatment wishes that are not in line with one’s own. Maybe raising awareness about personal blind spots and (subconscious) beliefs and wishes are more effective than the top-down installation of ACP in routine daily care. This study shows that accessible education, especially about communication skills, is seen to be very helpful for further adoption of ACP. An important facilitator is multidisciplinary team cooperation on care units. Head nurses should be aware of the fact that installing regular moments of gathering are seen to have a positive effect on ACP communication in the care unit. We recommend that subsequent research builds further on these insights, by quantifying the education needs, time constraints and other barriers and facilitators identified here. This information could serve to determine priorities for hospital policy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics statement
All participants received and signed an informed consent letter in which the purpose of the study was clearly stated. Ethics approval for the study was given by the Ethics Committee UZ Leuven (S58196 / B322201525224 / I / U).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.