
Abstract
Background
Coronary artery disease is a major cause of morbidity and mortality with high readmission rates. Hospital readmissions for coronary artery disease contribute to rising healthcare costs and are a marker of quality of care. Despite this, prior studies have found that readmission rates vary widely.
Aims
This study aims to determine the impact of social support, depression, comorbidities, symptom severity, quality of life and readmission among coronary artery disease patients in Thailand.
Methods
A total of 321 coronary artery disease patients from tertiary care hospitals across all regions of Thailand were recruited for this study. Data were analysed using multiple regression analysis.
Results
The coefficient for social support (beta = −0.22) was found to be significant (p < 0.05), whereas comorbidity, symptom severity, depression and quality of life were not significant. Thus, social support was found to be the most significant predictive factor for readmission.
Conclusions
Accordingly, when designing effective nursing interventions, nurses should promote social support interventions for coronary artery disease patients to improve the quality of care, decrease readmission rates and improve patients' quality of life.
Introduction
Coronary artery disease (CAD) is a chronic medical with high morbidity and mortality rates (Pelle et al., 2008; Sethares and Elliott, 2004; Volz et al., 2011). This group of patients tends to be readmitted to hospital due to recurrence of the condition (Gheorghiade et al., 2013; Ryan et al., 2014; Desai et al., 2009). Thus, the readmission rate is recognised as a marker of quality of care (QOC) and poses a significant financial burden on rising healthcare costs (Coffey et al., 2012; Hasan et al., 2009; Lundback et al., 2017; Sud et al., 2017; Dharmarajan, 2016). Although readmission is a marker of QOC, prior studies have found that readmission rates vary between 15% and 30%, within 30–60-day post-discharge period and between 25% and 50% within 6 months after the first hospitalisation, increasing to 80% within 1 year. This accounts for approximately 70% of the healthcare costs of CAD patients in the United States (US) (Giamouzis et al., 2011; Dharmarajan, 2016; Dordunoo et al., 2017). Various reasons are given for readmission, such as other medical problems, non-adherence to health recommendations (e.g., medication adherence, diet, fluid restriction or emotional factors), mental health factors (e.g., pain, anxiety, depression, substance abuse or cognitive disorders), environment and inadequate discharge planning (Annema et al., 2009; Desai et al., 2009; Coffey et al., 2012; Hasan et al., 2009; Eastwood et al., 2017; Jencks et al., 2009). Thus, readmission remains an important issue in health systems that indicates hospital-level quality and efficiency of care. Frequent readmission after discharge is increasingly recognized as a marker of inpatient QOC and is a significant contributor to rising healthcare costs (Desai et al., 2009; Dharmarajan, 2016; Hasan et al., 2009; Jencks et al., 2009). The role of nurses in the care of CAD patients includes providing routine 24-hour care, contributing to the discharge process and assisting patients and their families in making lifestyle adjustments. It is essential to consider the patient as part of a family structure so family needs can be assessed and met through individual or group sessions using appropriate resources. Thus, a study of the factors predicting readmission is needed for patients in this group.
Review of the literature
In Thailand, readmission has been documented as a QOC marker in CAD. However, previous studies examining readmission have focused on a single disease or condition (Jenghua and Jedsadayanmata, 2011; Kiatchoosakun et al., 2012). For example, research has been conducted on the readmission of heart failure (HF) patients. One study examined the rate and predictors of early readmission (within 30 days of discharge) among Thai HF patients by reviewing the electronic medical database. It found the early readmission rate for HF patients was 14.1%, when the length of stay in hospital was more than 5 days. In CAD patients it found that a history of diabetes mellitus, renal failure and digoxin were all factors associated with readmission. The most common cause of readmission was angina pectoris and chronic renal failure (Jenghua and Jedsadayanmata, 2011; Kiatchoosakun et al., 2012).
In addition, several interventions have been conducted to reduce the readmission rates of CAD patients such as fluid restriction intervention, discharge planning, advice and counselling intervention and medication regimen intervention, amongst others (Annema et al., 2009; Ryan et al., 2014; Jenghua and Jedsadayanmata, 2011). However, the readmission rate in CAD patients remains high. Moreover, most studies on readmission have been conducted in the US, but the factors related to readmission among CAD patients may vary across cultures and populations. In Thailand, the limited research conducted on the factors related to readmission has tended to confirm those in the US. However, because Thai cultural characteristics are different from the US, it is reasonable to suspect that research findings might differ too, such as comorbidities, symptom severity, depression, social support and living behaviour, which are all known to be factors related to readmission (Annema et al., 2009; Coffey et al., 2012; Hasan et al., 2009; Jencks et al., 2009).
In healthcare, quality has been defined as ‘the degree to which the health service increases the likelihood of desired health outcomes and are consistent with current professional knowledge’. There are three components of a quality care model (Duffy, 2009: 28). The first is the structure, which refers to the context or condition in which care is provided. Factors in this component are the institutional resources, provider credentials and patient characteristics. This study focuses on the patient characteristics because we wished to emphasise the manipulated factors related to patients. The second component is the process, which refers to the actions carried out for the patient, including both the technical and interpersonal aspects of care. The third component is the outcomes, which are the consequences of the healthcare process. Again, this study focuses on CAD patient characteristics because we aimed to manipulate the factors related to the patients before developing a process to improve the outcome. Thus, the following factors have been documented related to readmission among CAD patients: social support, depression, comorbidities, symptom severity and quality of life (QOL) (Annema et al., 2009; Betihavas et al., 2012; Carel, 2004).
The relationship among variables can be explained as follows: (a) social support significantly improved QOL and was linked to a decrease in readmission in CAD patients (Bennett et al., 2011; Volz et al., 2011); (b) patients had greater depressive symptoms, reflecting the high rate of readmission (Betihavas et al., 2012; Pelle et al., 2008); (c) symptom severity was consistently related to readmission, with a higher severity of symptoms related to high readmission (Carel, 2004; Giamouzis et al., 2011); (d) comorbidity had the greatest association with readmission and is a precipitant for patients' early readmission (Coffey et al., 2012; Hasan et al., 2009); and (d) CAD is a chronic condition and has an unstable course of illness with unpredictable exacerbations and progression of symptoms, resulting in poor QOL and is linked to frequency of readmission (O'Loughlin et al., 2010; Sethares and Elliott, 2004). Thus, the study aims to determine the impact of social support, depression, comorbidities, symptom severity, QOL and readmission.
Methods
Design
This cross-sectional study aimed to determine the impact of social support, depression, comorbidities, symptom severity and QOL on readmission among CAD patients in Thailand.
Readmission, which refers to the number of CAD patients with repeated hospitalisation within 12 months of discharge from index hospitalisation, which was collected from their medical record. Comorbidity, which refers to the presence of one or more additional conditions co-occurring with CAD in the patient and was determined from medical records. Symptom severity, which was measured using the Canadian Cardiovascular Society Classification for classifying angina, where Class IV – unable to do any activities with or without angina at rest; Class III – have symptoms with daily living activities, and so experience moderate limitation; Class II – experiencing angina only during vigorous physical activity and so a slight limitation; and Class I – only experiencing angina during strenuous or prolonged physical activity (Sangareddi et al., 2004). Multidimensional Scale of Perceived Social Support (Zimet et al., 1988). This instrument was developed for those undergoing a diagnostic coronary angiography. The 12-item scale was designed to assess three aspects of perceived social support (from friends, family and significant others). Participants were asked to respond to 12 items on a Likert scale from 1 (disagree very strongly) to 7 (agree very strongly), with a total score ranging from 12–84. A higher score represents a higher level of social support. A score between 12 and 36 would be a low level of social support, from 37–60 would be mild social support and from 61–84 would be a higher level of social support. This had a high internal reliability (Cronbach's alpha = 0.89) (Phromsornt et al., 2019). Cardiac Depression Scale (CDS) (Hare and Davis, 1996; Oldridge, 1997). The CDS is a 26-item self-rating scale used specifically for medical cardiac patients in Australia. It consists of two dimensions: Dimension 1 (sleep, uncertainty, mood, hopelessness and inactivity) and Dimension 2 (anhedonia and cognition). The CDS has been validated in adult cardiac inpatients and had satisfactory concurrent validity with the Beck Depression Inventory. The CDS has a high internal consistency (Cronbach's alpha = 0.91) and test-retest reliability coefficient of 0.94 in the Chinese version (Wang et al., 2008). Participants were asked to respond to 26 items on a Likert scale from 1 (strongly disagree) to 7 (strongly agree), with a total score ranging from 26–182. A high score represents a high level of depression. The score less than 90 is defined as no depression, score range from 90–100 is defined as mild to moderate depression, and score more than 100 is defined as strong depression. The Cronbach's alpha coefficient of Thai version was 0.82 (Polsook and Aungsuroch, 2019). Quality of Life Index-Cardiac version IV which was developed to measure QOL in terms of cardiovascular patients' satisfaction with life. This was translated into Thai by Saengsiri (2003) and comprised 70 items in two parts. The first part (35 items) measured the patient's satisfaction with various aspects of life, whereas the second measured the importance of those aspects. This tool covered the four domains of (a) health and functioning, (b) social and economic, (c) psychological /spiritual and (d) family. Answers were based on a Likert scale ranging from 0–5, with a final score range from 0–30. A lower score indicates a poor QOL (score 1–10). A score 11–20 is defined as a low QOL and score between 21 and 30 is defined as a high QOL. The internal consistency the Thai version using Cronbach's alpha was 0.91.
The benefits and risks of the intervention and the protection of human rights were presented in non-technical terms to the patient and their consent to participate in the study was obtained. All subjects agreed to participate and signed an informed consent form after being given a written description and further verbal information about the research project. Participants were asked to complete questionnaires. During data collection, participants were able to leave the study at any time.
Results
Characteristics of the participants
Demographic characteristics of the CAD patients of this study (n = 321).
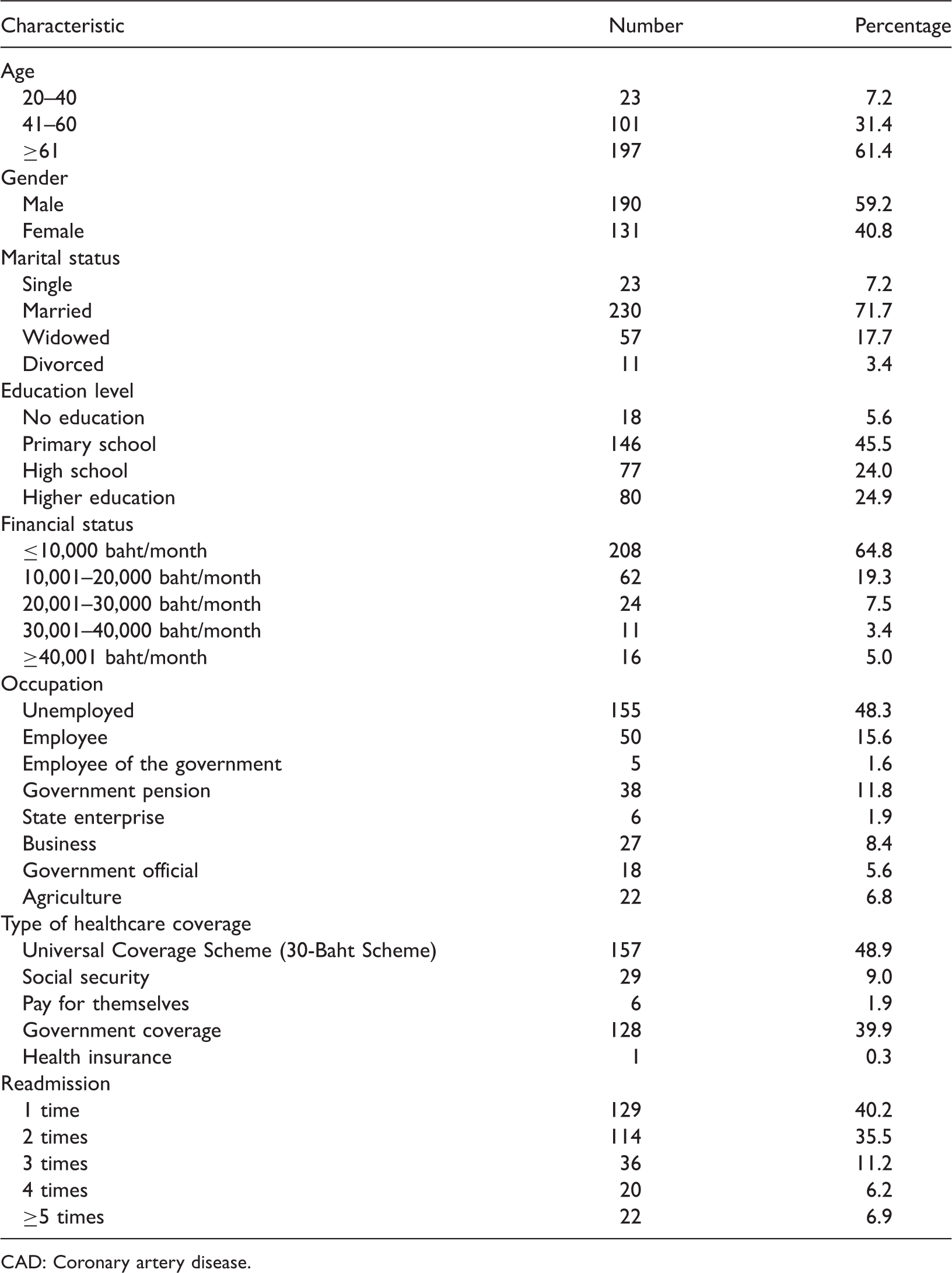
CAD: Coronary artery disease.
Description of predictive variables
Most participants had a high level of social support (60.4%) and slightly more than half were not depressed (51.7%). Nearly one-quarter of participants had no comorbidity (24.0%), followed by two (16.5%) and four comorbidities (12.7%). For symptom severity, one-third of the participants were Class II (35.7%), followed by Class III (28.9%), Class I (18.6%) and Class IV (16.9%). The majority of participants had a high QOL (76.9%).
Predictors of readmission
ANOVA.
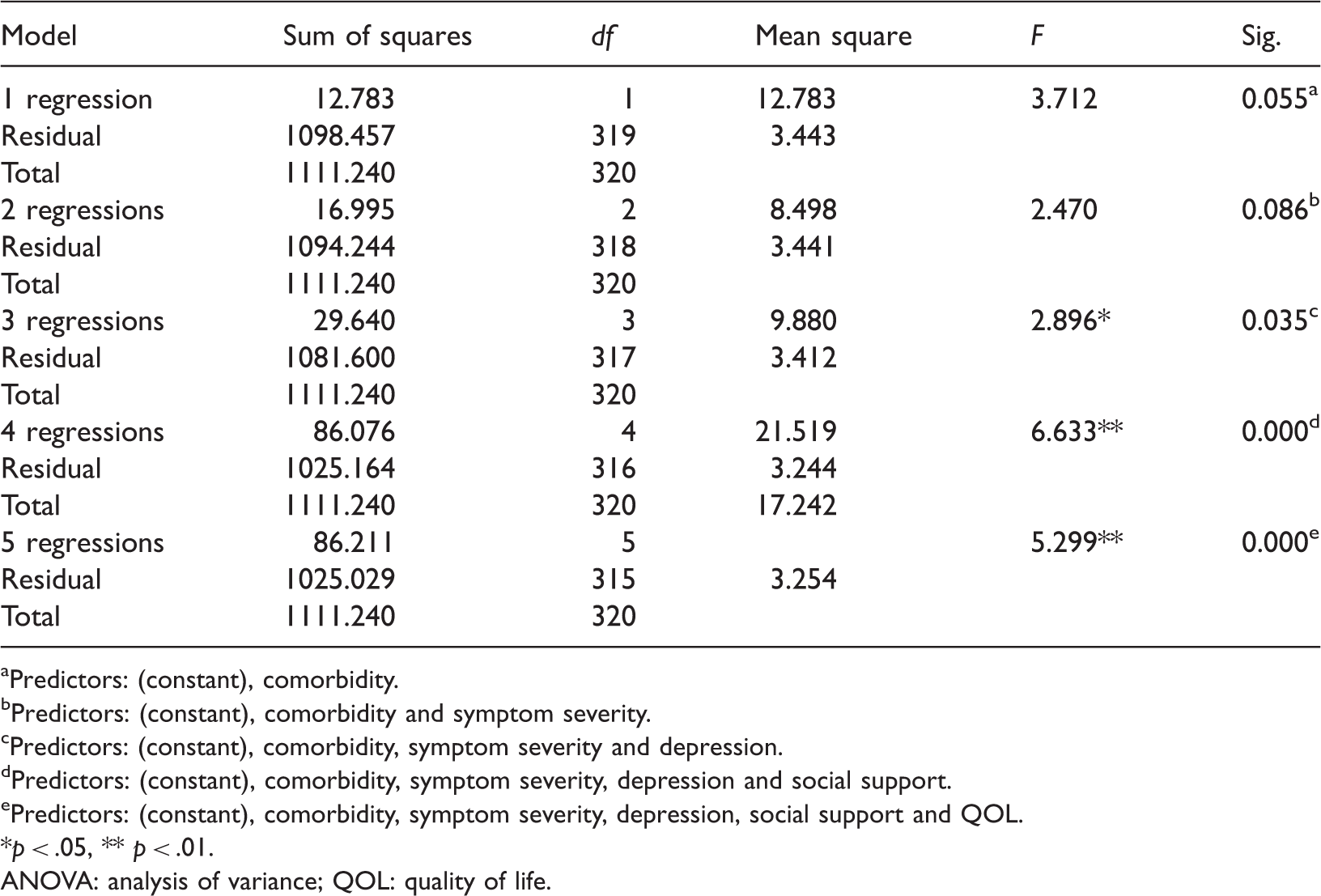
Predictors: (constant), comorbidity.
Predictors: (constant), comorbidity and symptom severity.
Predictors: (constant), comorbidity, symptom severity and depression.
Predictors: (constant), comorbidity, symptom severity, depression and social support.
Predictors: (constant), comorbidity, symptom severity, depression, social support and QOL.
*p < .05, ** p < .01. ANOVA: analysis of variance; QOL: quality of life.
Regression coefficients.
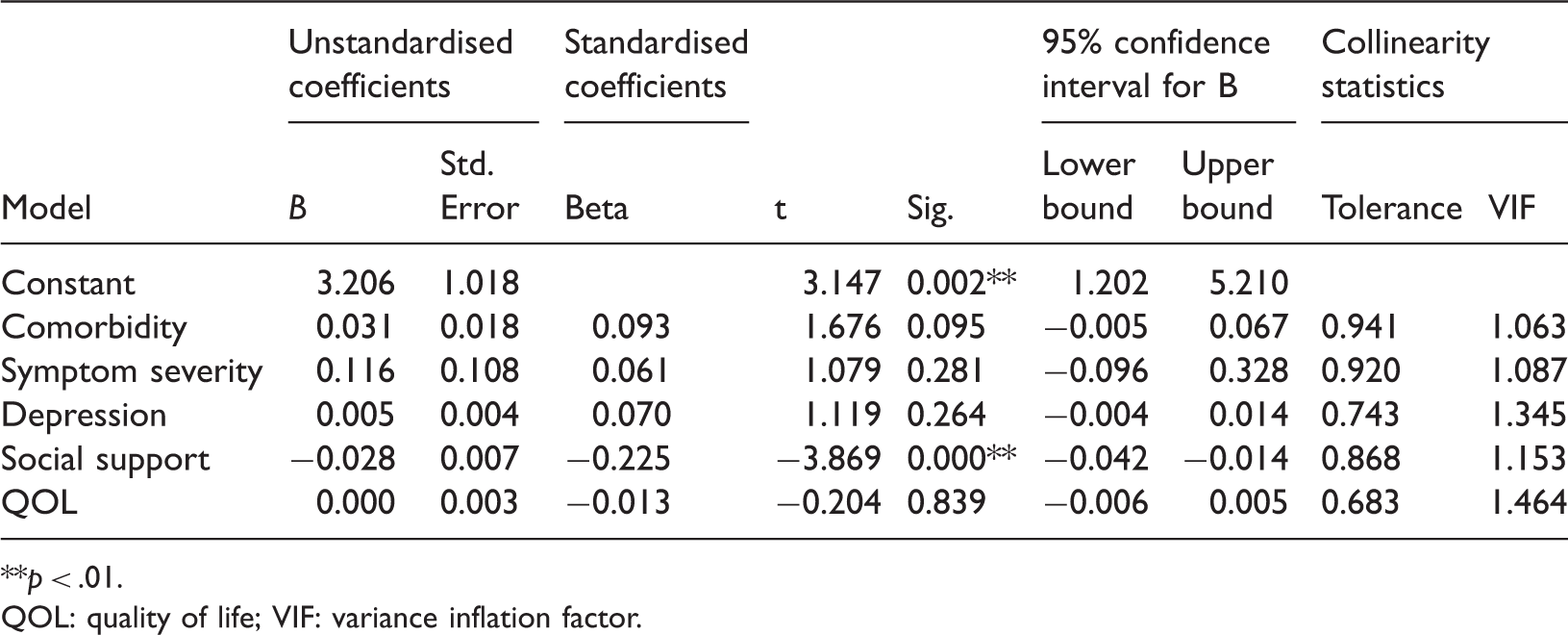
**p < .01.
QOL: quality of life; VIF: variance inflation factor.
Model summary.
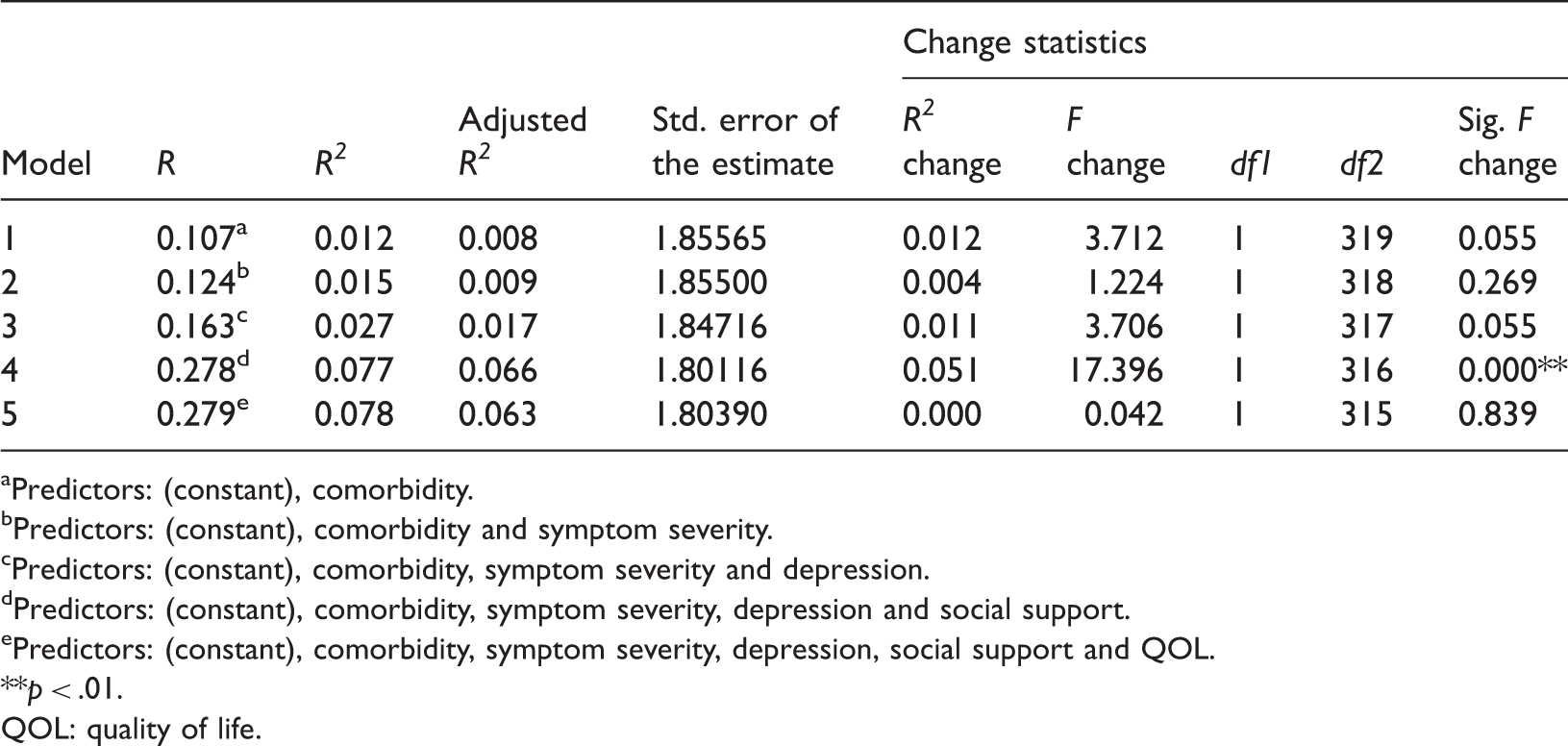
Predictors: (constant), comorbidity.
Predictors: (constant), comorbidity and symptom severity.
Predictors: (constant), comorbidity, symptom severity and depression.
Predictors: (constant), comorbidity, symptom severity, depression and social support.
Predictors: (constant), comorbidity, symptom severity, depression, social support and QOL.
**p < .01.
QOL: quality of life.
Discussion
According to the findings of this study, the five factors of comorbidity, symptom severity, depression, social support and QOL explained 7.8% of the variance (p < 0.05) in readmission among CAD patients. However, only social support was found to be significant at the p < 0.05 level and was negatively correlated with readmission because most participants were married (71.7%), so had someone to take care them, resulting in lower readmission rates. Additionally, in Thailand people usually have a close extended family and most participants lived with family members, thus it is possible family members participated in the care and support of these patients (Polsook et al., 2013; Polsook et al., 2016). This result concurs with other studies that show social support is negatively correlated with readmission. For example, social support has been shown to be related to decreased readmission and mortality rates among CAD patients (Lu et al., 2016; Tang et al., 2018) and CAD patients with a high level of social support had lower readmission rates, whereas adult chronic CAD patients with a lack of social support had an increased risk of readmission (Bennett et al., 2011; Tang et al., 2018).
The other four variables of this study (comorbidity, symptom severity, depression and QOL) were not significant. Comorbidity did not predict readmission because nearly one-third of the participants in this study reported no comorbidity (24.0%), which meant participants did not have the complexity of other health conditions. Thus, readmission is at a lower rate in this study. This result is similar to other studies, where more comorbidities had a positive correlation with readmission. For example, more comorbidities were found to be a significant predictor of readmission (Hasan et al., 2009) and had the greatest association with readmission (Coffey et al., 2012) or early readmission in CAD patients (Gheorghiade et al., 2013; Betihavas et al., 2012; Kwok et al., 2018). Additionally, more comorbidities were shown to reflect poor health and the burden associated with an increasing readmission (Benbassat and Taragin, 2000; Kansagara et al., 2011). For symptom severity, more than one-third of participants (35.8%) were Class II: a slight limitation of physical activity but comfortable at rest. Ordinary physical activity results in fatigue, palpitation and dyspnoea (shortness of breath), so they do not have severe clinical symptoms (Sangareddi et al., 2004). Thus, the participants can participate in any activity without severe clinical symptoms. This finding supports previous studies showing symptom severity was consistently related to readmission and a higher severity of symptoms was related to a higher rate of readmission (Giamouzis et al., 2011; Carel, 2004).
In our study most participants did not exhibit depressive symptoms (51.7%) because they had a high level of social support, no comorbidity and could participate in activities without severe clinical symptoms. So, the participants had lower readmission rates. This result is supported by other studies, where no depressive symptoms or a lower level of depression symptoms were associated with lower readmission rates (Pelle et al., 2008). Additionally, post-myocardial infarction, no depression and increased adoption of secondary prevention measures led to a decrease in hospital admission, where depression was related to readmission (Myers et al., 2012). Moreover, depressive symptoms were demonstrated to have an adverse effect on readmission (Volz et al., 2011; Dhital et al., 2018), where CAD patients who developed severe depressive symptoms tended to have an increased chance of hospital readmission and a lower QOL.
The majority of participants had a high QOL. As shown by the researchers mentioned above, high social support meant patients had a spouse or family member helping them, so they had lower readmission rates. The results of this study contrast with a previous study, where a low QOL predicted readmission. Indeed, QOL is recognised as a significant predictor of readmission for CAD patients (Dhital et al., 2018; Heo et al., 2009; O'Loughlin et al., 2010), where CAD patients who experience physical and emotional symptoms that result in a poor QOL are linked to a higher frequency of readmission (Kim et al., 2019; Sethares and Elliott, 2004; O'Loughlin et al., 2010). Likewise, CAD was found to be a chronic condition with an unstable course and unpredictable exacerbations and progression of symptoms, which resulted in a poor QOL and was linked to an increased frequency of readmission (Kim et al., 2019; Sethares and Elliott, 2004; O'Loughlin et al., 2010).
The limitations of this study include that the data were based on self-reports, which could have caused overestimated or underestimated values. Based on these findings, a longitudinal study should be conducted to assess the changes in these variables and readmission in CAD patients to provide a more causal explanation regarding readmission in CAD patients and its predictors.
Conclusion and implications for practice
Social support was found to be a significant predictive factor for readmission. Based on the findings of the study, social support should be promoted to enhance the ongoing care of CAD patients. Although depression is not associated with hospital readmission in this study, the mediating effects of anxiety and depression contributing to the QOL of patients with CAD are well established (Lee et al., 2014). It would be beneficial for all CAD patients to be screened for depression so proper intervention can be provided to avoid hospital readmission. This information about the results of this study will help nurse as a health care team to solve hospital readmission among CAD patients. This was a cross-sectional study, but future studies are needed with an experimental/quasi-experimental design with intervention and control groups that promote social support. This would then show if this variable was real and effective in decreasing readmission in this group to improve QOC and decrease readmission rates and healthcare costs, while improving the patient's QOL.
Footnotes
Key points for policy,practice and/or research
Social support was found to be a significant predictive factor for readmission. Nurses should promote social support to enhance care of CAD patients. Nurses, as part of a multidisciplinary team, should screen for depression in CAD patients for the early detection of depression symptoms. This information about the results of this study will help nurses in the health care team to solve hospital readmission among CAD patient. More studies are needed with an experimental/quasi-experimental design with intervention and control groups that promote social support intervention. For an effective decrease in readmission in this group, policy makers should promote social support to improve QOC and decrease readmission rates and healthcare costs while improving the patient's QOL.
Acknowledgements
The authors thank the participants for their time and effort. Additionally, the authors would like to thank the targeted hospitals for facilitating for data collection process.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approvals
This study was approved by the ethics committee of the tertiary care hospitals from all regions of Thailand prior to data collection. Those IRBs included the Ethics Committee of Hatyai hospital (approval 85), the Ethics Clearance Committee on Human Right Related to Research Involving Human Subjects Faculty of Medicine Ramathibodi Hospital, Mahidol University (2558/716), Research Ethics Committee Faculty of Medicine Chiang Mai University (2558-03518), IRB of the Faculty of Medicine, Chulalongkorn University (074/59) and the Khon Kaen University Ethics Committee for Human Research (00001189).
Funding
The author(s) disclose receipt of the following financial support for the research, and/or publication of this article: This work was supported by the Ratchadaphiseksomphot Endowment Fund, Chulalongkorn University (grant CU-GR_60_38_36_03).