
Abstract
Background
Improved survival rates for people with cystic fibrosis have led to increased rates of co-morbidity, of which diabetes is the most common. Cystic fibrosis related diabetes affects 19% of adolescents and up to 50% of adults, although little is known about their experiences of this co-morbidity.
Aims
To investigate the experiences of living with and managing cystic fibrosis related diabetes among adolescents and adults.
Methods
Systematic review and thematic analysis of qualitative evidence.
Results
Six studies, rated good quality, were included in the review and four main themes emerged from the data: knowledge and understanding; emotional and social impact; balancing both conditions; acceptance and adjustment. Although the main themes reflect adolescent and adult experiences, there were subtle variations in their sub-themes. Participants' overriding story was of journeying towards acceptance and integration of cystic fibrosis related diabetes into their lives. This included their unpreparedness for the likely onset of cystic fibrosis related diabetes and their struggles to balance the competing demands of living with and managing cystic fibrosis and diabetes.
Conclusions
The diagnosis of cystic fibrosis related diabetes and its incorporation into daily life is challenging for many people with cystic fibrosis. Review findings indicate opportunities for cystic fibrosis related diabetes interventions pre-diagnosis, at diagnosis, and during ongoing management, which need integrating into routine cystic fibrosis care.
Keywords
Introduction
Cystic Fibrosis (CF) is the most common life-limiting inherited disease in the Caucasian population. It is a complex multisystem disease characterised by abnormal transport of sodium and chloride, which results in thick viscous secretions in the lungs, gastrointestinal tract, liver, pancreas and reproductive tract, and elevated sodium concentrations in sweat (Elborn, 2016). Cystic fibrosis occurs in approximately one in every 2500 live births (Dodge et al., 2007) and currently affects 10,070 babies, children and young adults in the United Kingdom (UK) (Cystic Fibrosis Trust (CFT), 2020). In the 1930s when CF was first described, 70% of babies died within the first year of life (Andersen, 1938). The median predicted age of survival is now 47 years (CFT, 2018) and infants are expected to live to over 50 years of age (MacKenzie et al., 2014).
Improved survival has led to increased rates of co-morbidity with diabetes being the most common. The prevalence of cystic fibrosis related diabetes (CFRD) increases with age, affecting 2% of children, 19% of adolescents and 40–50% of adults (Moran et al., 2009). In the UK, 33.9% of the CF population who are older than 16 years have CFRD (CFT, 2020). The primary cause is insulin deficiency, however, few people with CF have completely ‘normal’ glucose tolerance and CFRD is viewed as part of a continuum of glucose tolerance abnormalities (Moran et al., 2010).
Mortality in people with CFRD remains significantly increased compared to those who have CF without CFRD (Lewis et al., 2015), and their clinical status is more compromised. This includes lower lung function (Koch et al., 2001), increased growth of respiratory pathogens with increased concentrations of airways surface liquid glucose (Garnett et al., 2013), more hospital admissions (Marshall et al., 2005) and a lower body mass index (BMI) (Koch et al., 2001).
Although CFRD shares some features of Type 1 and Type 2 diabetes mellitus (T1/2 DM), there are important pathophysiological differences that require a unique approach to diagnosis and management. United Kingdom and international clinical guidelines recommend annual screening because of the often insidious onset of the condition (CFT, 2004; Brunzell et al., 2015). A significant focus on managing nutritional status is recommended, often necessitating a high-energy diet that conflicts with T1/2 DM dietary advice, and insulin therapy that is tailored to individual requirements taking into account both the clinical and nutritional status. The importance of patient knowledge for self-management of CFRD is emphasised (CFT, 2004; Brunzell et al., 2015) and guidelines have been produced for children and adolescents for whom self-management can be a particular challenge (Moran et al., 2018).
The guidelines also recommend collaborative multidisciplinary team (MDT) approaches to care (CFT, 2004; Brunzell et al., 2015). Specialist cystic fibrosis teams typically include doctors, nurse specialists, dietitians, physiotherapists, psychologists and/or social workers. Nurse specialists are responsible for patient advocacy, clinical management, advice and support, education, research and management, including the co-ordination of some teams (CFT, 2001). However, CF care is also delivered by non-specialists in ward and community-based services including registered nurses with responsibilities for child or adult care (Reisinho and Gomes, 2016).
Common to the formulation of the guidelines has been the use of quantitative evidence hierarchies that range from randomised controlled trials to expert clinical opinion. The patient’s voice, including their experience of self-managing CFRD and the challenges they face are not present. Brunzell et al. (2015) have acknowledged that these remain unanswered questions.
Among adults with CF, ‘paradox of control’ and ‘living deaths’ describe their struggle with the treatments necessary to maintain stable health (Varilek and Isaacson, 2020). Cystic fibrosis is an unpredictable disease and day-to-day variability in health is observed (Knudsen et al., 2018). Among children and adolescents, loss of opportunities, isolation and disempowerment negatively affect their CF management (Jamieson et al., 2014). These difficulties are likely to be compounded by the onset of CFRD but are dependent upon individual disease management strategies, coping mechanisms and illness trajectories. A significant part of managing diabetes involves self-management; people with CFRD must make decisions about how to manage their life, CF and CFRD. Through the first author's clinical experience it was observed that not everyone with CF has the same relationship with CFRD and for some it was a major obstacle and far worse than CF. How CFRD impacted upon the lives of people with CFRD appeared to affect self-management skills. To date there has been no systematic appraisal of the experiences of individuals who live with the CFRD. Looking for understanding of why people experience CFRD in different ways, and what factors help them or inhibit them in their management and coping prompted this systematic review. This review therefore aims to answer the following research question: among adolescents and adults, what are their experiences of living with and managing CFRD?
Methods
The systematic review employed the thematic analysis methodology of Thomas and Harden (2008), which was originally devised to explore the need for interventions and their acceptability to patients. The review is reported in accordance with the ENTREQ statement (Tong et al., 2012: Enhanced transparency in reporting the synthesis of qualitative research).
Search strategy
Ovid Medline, CINAHL, EMBASE and PsychINFO databases were searched from their inception to July 2020. Search strategies were tailored to each database and the Ovid Medline strategy is available as supplementary material (Supplementary figure S1). Studies were included if they sampled adolescents 10 years of age and above or adults with CFRD, and used qualitative methods to explore the experiences of living with and managing CFRD. Studies were excluded if they primarily used quantitative methods or only concerned people with T1/2 DM.
Secondary search strategies looked for published and unpublished work via CF conference abstracts and proceedings in Pediatric Pulmonology and The Journal of Cystic Fibrosis, to reflect current clinical practice and research these were reviewed from 2006 onwards. The reference lists of potentially eligible reports and articles were also hand searched. The lead author screened all titles and abstracts against the inclusion/exclusion criteria, and this process was verified by all authors to ensure relevant papers were captured.
Data extraction and synthesis
Tabulation and thematic analysis techniques guided data extraction and synthesis. A data extraction template was used to capture key methodological detail for each study including the country of origin, research aim, participants, design and methods, and key thematic findings. Following Thomas and Harden (2008), study results were then read and reread, and free codes were assigned to descriptive themes relevant to the review’s aim. These codes were further interpreted to yield analytical themes and sub-themes. The constant comparison of descriptive and analytical themes across studies facilitated an inductive synthesis that represented a third order interpretation of the studies’ collective findings.
Data were extracted by the first author (SC) and verified by independent members of the research team (SW, AJ, JS) who also conducted preliminary descriptive and analytical coding. Coding was also undertaken by the first author (SC) and both sets of results were compared to generate a final synthesis of the data. Any additions, omissions or disagreements were agreed through discussion (SC, SW, AJ, JS). The results of these analytical methods are reported separately for adults and adolescents.
Quality appraisal
All studies were quality appraised using the Critical Appraisal Skills Programme (CASP) checklist for qualitative research (CASP, 2016). The checklist includes 10 questions, nine of which are rated as ‘yes’, ‘can’t tell’ or ‘no’, and pertain to a study’s research design and the methodology for data collection and analysis. The 10th question invites a qualitative response regarding the value of the research. Appraisals were conducted by the first author (SC) and verified by independent members of the research team (SW, AJ, JS).
Results
A total of 1829 records were returned from the search strategy after duplicates were removed (Figure 1). Following the screening of titles and abstracts, full text articles were retrieved if they met the review’s inclusion criteria or if there were any methodological uncertainties (n = 36). After careful review, six studies were included in the qualitative synthesis. PRISMA flow-chart.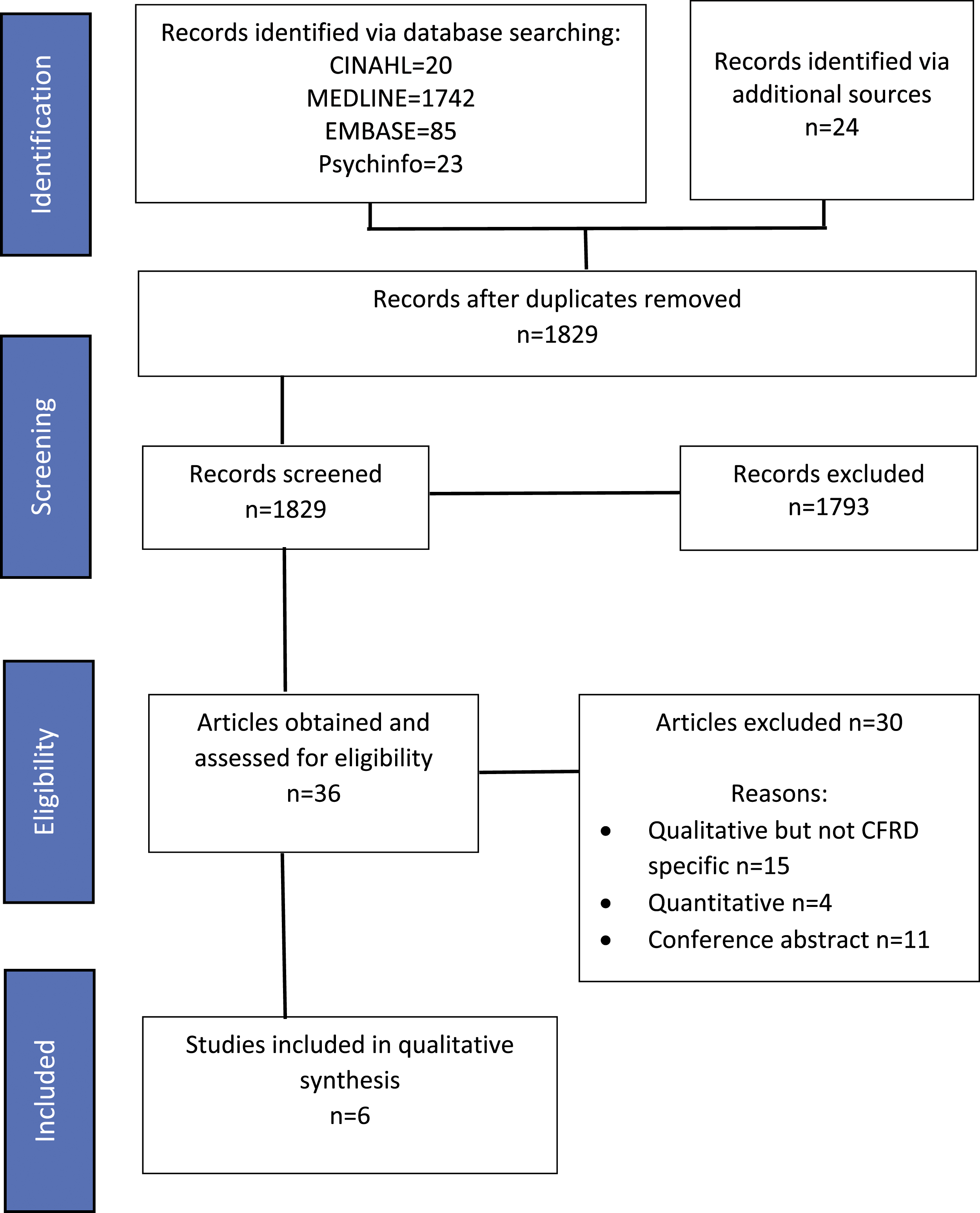
Study characteristics
Study characteristics.
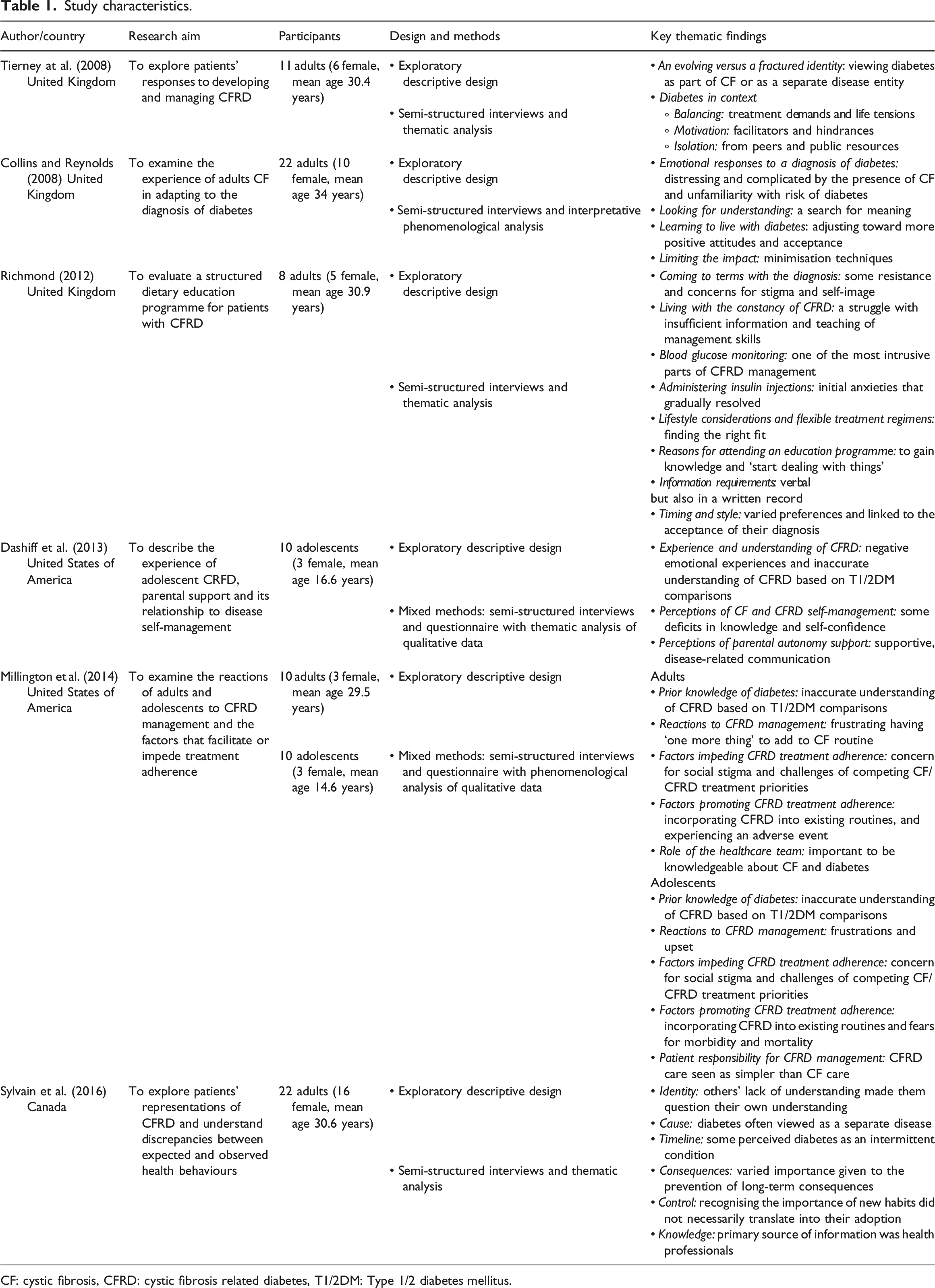
CF: cystic fibrosis, CFRD: cystic fibrosis related diabetes, T1/2DM: Type 1/2 diabetes mellitus.
Quality of studies
CASP qualitative appraisals.
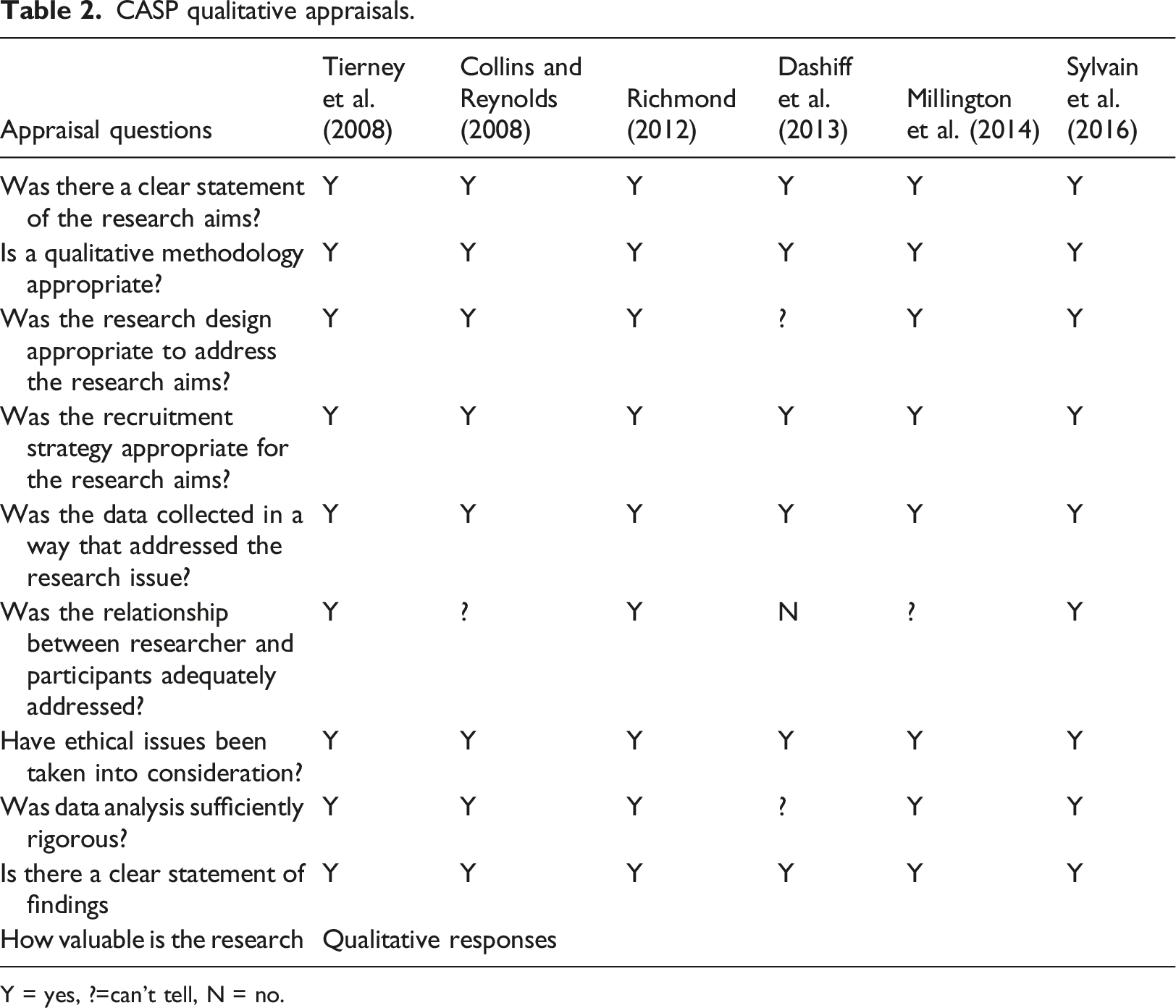
Y = yes, ?=can’t tell, N = no.
Thematic analysis results
Data were transformed into four main themes, each with a number of sub-themes (Figure 2). Although the main themes represented both adolescent and adult experiences, there were some variations in their sub-themes. Each theme is presented below together with illustrative quotes from the studies, annotated to indicate the study and type of data presented (text or a verbatim quote). Themes and sub-themes.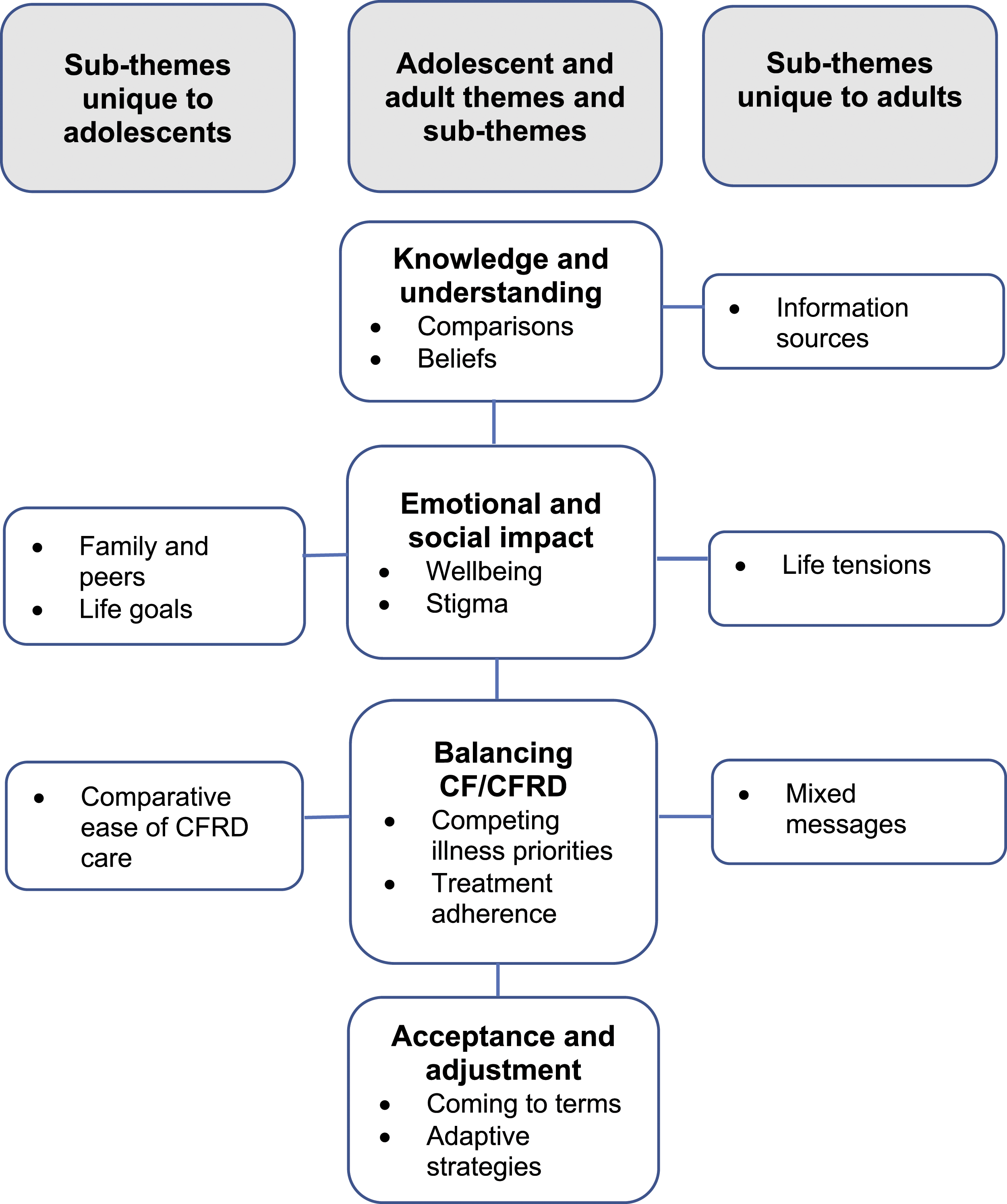
Knowledge and understanding
The lack of knowledge and understanding, with regards to the cause and management of CFRD, of people with CFRD and the people who help support them along with the realisations that CFRD is not the same as other types of diabetes is central to this theme. All studies heard from people with CF who lacked knowledge and understanding about CFRD, particularly its causes and management. Misunderstandings were reported among family and friends, and some healthcare professionals including general practitioners (GPs), particularly in relation to dietary advice. This was compounded by segregation policies to minimise the risk of cross-infection between individuals with CF, which prevented face-to-face peer support. Accurate information was sometimes hard to access and the misunderstandings of others could have a profound effect. A sense of despondency was clear in the narratives of some interviewees … when recalling how their condition was not understood properly by others, especially by certain members of the medical profession. (Tierney et al., 2008_text, pp. 242)
To make sense of CFRD, participants often made comparisons with people they knew who had T1 or T2DM, and with their personal experience of CF. In the first instance, this was problematic because of the pathophysiological differences between T1/2DM and CFRD. Comparisons with the life-limiting condition CF meant that CFRD was not always considered to be a significant concern. The possibility of diabetes complications was downgraded against the likelihood of succumbing to CF.
A lack of adequate information and the comparative appraisals that were made could lead to spurious perceptions of CFRD. Some participants viewed it as temporary and held inaccurate beliefs about its causation. Others oscillated between viewing it as a separate disease or as an evolution of CF. This ambivalence suggested a reluctance to integrate the two conditions with implications for the management and control of CFRD. As long as I see diabetes as a secondary condition, I can’t put the two together … it’s like they’re two different things even though they go with the same health problem. (Sylvain et al., 2016_quote, pp. 1134)
There were counter-examples of these challenges when participants received advice from their CF teams or specialist CFRD services. However, there was acknowledgement across the papers that information about CFRD and its likely occurrence needed to be available earlier in a person’s CF illness trajectory, and not just at the point of CFRD diagnosis. Annual CFRD screening was useful for patients to ‘warm them up’ to the possibility of CFRD. (Millington et al., 2014_text, pp. 105)
Although adolescents did not reference hard to reach or inaccurate information sources, their experiences mirrored those of adults. They sought understanding by comparing their condition with family or friends who had T1/2DM, resulting in inaccurate generalisations and a poor understanding of CFRD.
Emotional and social impact
This theme explores the emotional and social impact of CFRD from its diagnosis though to its influences upon everyday life. Being diagnosed with CFRD provoked mixed emotions and was more significant for some people. Many reported negative feelings, which included descriptions such as ‘shocking’, ‘hard’, ‘terrible’, ‘depressing’ and ‘agitating’. The negative impact could be protracted, even if the person had been diagnosed for several years. Conversely, a few participants felt relief when diagnosed because it provided an explanation for their symptoms. The value of routine annual CFRD screening was confirmed by some participants, whom it had helped to accept the diagnosis when it was made.
Fears of increased morbidity and mortality were expressed, although in terms of the overall impact on health CF was regarded as worse because it was considered life-limiting. The possibility of diabetes related complications was not of great concern for health with the likelihood of succumbing to CF first being greater. I know about the long-term consequences\x{2026} if the diabetes ever gets to the stage where it causes me those sort of problems I\x{2019}ll be dead chuffed because I\x{2019}ll still be here\x{2026} but I suspect the CF will get me first. (Tierney et al., 2008_text, pp. 240)
Concerns for the ‘constancy’ of CFRD were common. The illness did not ‘fade into the background’ in the same way that CF did, and its treatments could not be ‘hidden’ as they could for CF. Often, individuals had to manage aspects of their diabetes care in public, such as monitoring blood glucose levels and administering insulin, which impacted on their emotional and social health. Embarrassment was frequently expressed as was a concern for stigma. A deeply rooted consequence was that the development of CFRD made some people’s CF more visible. This disrupted ‘normal’ identity, interfered with a person’s lifestyle, and brought their feelings about CF to the foreground. I saw it as something that would hamper my lifestyle. Something that would …interfere. (Millington et al., 2014_quote, pp. 102) I think I was quite distraught…and found it really difficult to have that on top of (CF) …having to…deal with something else. It made me think about CF more. (Collins and Reynolds, 2008_quote, pp. 482)
The life tensions that participants felt as a result of their diagnosis were managed in a more cavalier way by some. They aimed to preserve their quality of life even if it meant engaging in activities that were not conducive to a compromised health status. For many patients, the priority was preserving their immediate quality of life, with the rigorous treatment of their diabetes coming second. (Sylvain et al., 2016_text, pp. 1138)
However, this was not always the case. Having life aspirations could enhance a person’s diabetes and CF care, and this seemed to be particularly true of adolescents, whose life goals often motivated increased self-care activities. In other respects, adolescents experienced the consequences of a CFRD diagnosis in much the same way as adults, including negative emotional responses such as feeling ‘upset’ and ‘distress’, and concerns for social stigma. An important difference was the influence of family and peers. (Adolescent) patients may struggle with completing treatment recommendations in the face of social pressures and the desire for autonomy … having their parents physically inject them was prohibitive to sharing CFRD responsibility. (Millington et al., 2014_text, pp. 105)
Balancing CF and CFRD
A prominent theme within this review, that significantly influenced the management of CFRD, concerned the need to strike a balance between CF and CFRD. Participants experienced competing treatment demands from both conditions, trying to balance respiratory treatment and therapies with nutritional management strategies and insulin and blood glucose monitoring, where most viewed CF as being the more important. Cystic fibrosis related diabetes was associated with an increased treatment burden that impacted all aspects of daily life, and the addition of ‘one more thing’ to be managed was particularly frustrating. Difficulties were also encountered when trying to balance diet and blood glucose levels, particularly when dietary advice was conflicting. Juggling conflicting dietary demands of cystic fibrosis and diabetes coupled with the lack of practical professional advice available was seen as one of the biggest challenges in adapting to diabetes. (Collins and Reynolds, 2008_text, pp. 478)
Fluctuations in treatment adherence were not uncommon. Forgetfulness, lack of time, poor knowledge and the avoidance of pain were reasons for not monitoring blood glucose levels. The aforementioned desire to preserve quality of life also meant that CF treatments were often prioritised. Though understandable, these fluctuations could establish a negative cycle of reinforcing behaviours. A lack of glycaemic control impacted negatively on weight, lung function and overall health, and when unwell with CF-related illnesses such as respiratory exacerbations, it became more difficult to control blood glucose levels. This was particularly noticeable when corticosteroids were prescribed as a CF treatment. For some participants, the development of diabetes marked the point at which their CF health began to deteriorate, whilst others became anxious that deterioration would occur.
How CF was viewed and managed by adults appeared to influence their thoughts, feelings and responses to diabetes. Cystic fibrosis related diabetes demanded more attention than CF, its management required more forward planning, and it was often relegated to second place. This was not so among adolescents who considered CFRD care to be easier than CF care, perhaps because the latter depended more on parental oversight. Although many (adolescent) patients were still working on becoming independent with CF treatments they were able to manage diabetes on their own. CFRD care was seen as simpler than CF management. (Millington et al., 2014_text, pp. 103)
Acceptance and adjustment
People with CFRD embark on a tentative journey of acceptance and adjustment from the point of diagnosis to incorporating CFRD into their lives. Although the deleterious effects of a CFRD diagnosis could be protracted, participants became more accepting of its implications and made necessary adjustments over time. Coming to terms involved a search for clarity and the resolution of uncertainties. Whilst acknowledging the shock of a diagnosis, participants’ unpreparedness for the likelihood of CFRD evolving as part of their condition, and the resulting struggle toward acceptance and integration that they described, provides salutary lessons for service providers. Healthcare professionals need to be aware that, despite participants’ status as ‘expert patients’, highly experienced in the management of CF, they were not equipped with knowledge and confidence for managing this second chronic illness. (Collins and Reynolds, 2008_text, pp. 483)
The adaptive strategies that participants described drew on their experiences of living with a chronic condition and its management. Existing lifestyle patterns, routines and coping mechanisms developed for CF were applied to their self-care of CFRD. For some, CFRD became a condition unique to people with CF, quite separate from their initial understandings based on T1/2DM and was integrated into their personal worlds, from where a better balance of disease management was achieved. Adolescent views echoed the attainment of adaptive strategies, but their pathways appeared simpler. Perhaps they were less encumbered by longer life histories and instead, experienced a world full of new beginnings. Their experience of CF helped them come to terms with a CFRD diagnosis, and they had become more responsible for the care of their CF because of CFRD. Integration was less challenging and acceptance more welcome. I’m not going to walk around with ulcers on my body or lose my feet or my fingers. That\x{2019}s not going to happen to me because there\x{2019}s too much that I have planned for myself. … (Millington et al., 2014, pp. 102) If you know that you have a good insulin regime going…there’s no real reason that you should be high at any point. (Millington et al., 2014, pp. 102)
Important to note that these adolescent responses were underpinned by vigilant and supportive parenting. Both studies that included adolescent samples emphasised the need for clinicians to support parents, especially at the point of CFRD diagnosis, to reduce their anxieties, provide information and promote their competence to integrate CFRD management into existing CF routines.
Discussion
This is the first qualitative synthesis of research evidence into the experiences of living with and managing CFRD. The story to emerge is of participants journeying towards acceptance and integration of CFRD, and their struggle to strike a balance with the competing treatment and management demands of CF. Their struggle is understandable given the onset of one potentially life limiting condition within the context of another. However, the evidence also points to factors that may hinder people’s understanding of CFRD and their progress towards acceptance and effective self-management.
Although CF is the most common life-limiting inherited disease in the Caucasian population, and CFRD the most common co-morbidity, all studies demonstrated that the relationship between these conditions was poorly understood by people with CF, their families, friends, and some healthcare professionals. This was particularly pertinent to dietary advice but there were also inaccuracies in perceptions of CFRD including its causation and separateness from CF, rather than understanding it to be part of the CF illness trajectory. Some participants were unprepared for this possibility and their reliance on comparisons with T1/2DM left them vulnerable to poor self-management strategies. How participants understood and perceived CFRD was therefore seen as a key determinant of their responses to the condition.
This highlights the importance of education delivered by non-specialist healthcare professionals who care for people with CF. This includes registered nurses who work with children or adults in hospital-based and community services, as well as GPs and other primary care staff. It also raises questions about the utility of existing diagnostic nomenclature ‘cystic fibrosis related diabetes’. ‘Related’ does not infer a direct causal relationship but an association of sorts, and one that was considered quite distant and separate from CF by some participants. This is not necessarily helpful and may have contributed to the unpreparedness of participants for the development of CFRD, and subsequent comparisons with T1/2DM to further their understanding. On reflection of these findings, we believe it is time to review this diagnostic nomenclature and to consider instead the term cystic fibrosis diabetes (CFD). This is commensurate with T1/2DM nomenclature but also makes clear its difference; CFD is neither, it is a separate type of diabetes that is caused by CF which requires its own specific management.
Adopting the name cystic fibrosis diabetes in clinical practice would encourage people with CF and their healthcare professionals to see the condition as a combined entity, and influence approaches to its care and management. The change may also raise awareness of the risk of CFRD much earlier in a person’s CF illness and facilitate its incorporation into annual screening of the condition. This provides opportunities to prepare people and to lessen the shock of diagnosis and other negative emotions. It also enables earlier promotion of management strategies that incorporate CFRD care into pre-existing CF routines, thereby enabling better negotiation of the balancing act that participants reported. Ultimately, because of the close links between nutritional status, lung function and diabetic control, managing CF and CFRD as one condition will influence survival.
These shifts in diagnostic language, assessment and management strategies appear particularly suited to adolescents. Life goals and aspirations motivated their diabetes self-care activities, and integration of the two conditions was often less challenging than it was for adults. Cystic fibrosis related diabetes screening and management approaches that mirror these potentials will reap medium and long-term health benefits.
Some of the findings from this review are similar to those of reviews into other co-morbid conditions that involve diabetes. Hierarchical ordering of co-morbidities and the prioritisation of care informed by personal values is commonly reported (Lim et al., 2017; Cheng et al., 2018). Cystic fibrosis was often viewed as the most important illness because it is life-limiting; however, the importance in optimising the management and support of people with CFRD needs addressing because the presence of CFRD is associated with increased morbidity and mortality (Lewis et al., 2015). This review’s findings also echo nursing guidance for CF care, specifically the profession’s need to understand different phases of the disease process, with its ability to offer phase-specific interventions that support adaptation to the health-disease process (CFT, 2001; Reisinho and Gomes, 2016). Our findings suggest there are intervention opportunities for nurses and allied health professionals at three stages in the CFRD phase: pre-diagnosis, at the point of diagnosis and ongoing management.
Some people with multi-morbid conditions reported being overwhelmed at times but many more appeared to be resilient and determined to persevere despite challenges (Liddy et al., 2014). In the CFRD populations within this review, there was not a sense of being overwhelmed, CFRD was seen as more of an inconvenience and nuisance. It led to disruptions in daily life. It challenged identity by bringing illness into the foreground because treatment needed to be conducted outside the home and could no longer be hidden. Experience developed while living with one chronic condition and familiarity with healthcare systems can help the management of subsequent illness (White et al., 2016). The majority of people with CF have attended hospital and clinics from a very early age. Through this they have developed knowledge of their condition, experience of managing complex treatment regimens and become familiar with healthcare systems. This would have facilitated the adjustment needed to accommodate CFRD into their lives.
Novel and important findings from this review are the unpreparedness of participants for the likely onset of CFRD, their search for hard-to-find information, inaccurate beliefs about its causation and nature and the struggle to balance the management of CF and diabetes. However, these are manageable challenges through partnerships in care that appreciate individuals’ unique illness experiences and offer person-centred services.
Study limitations
Although the overall quality of the included studies was rated as good, they were few in number, representing 73 adults and just 20 adolescents. The findings from this systematic review do not appear to have been affected by the different healthcare systems of the three countries represented within it. Although limiting the transferability of the review’s findings, this is an important indicator for the current breadth of research into this condition. The interpretative nature of the thematic analysis technique can lead to variability in findings depending upon a researcher’s stance. The dietetic professional background, training and experience of the first author may have coloured data interpretation. The use of a second coder and analyst from the nursing profession (SW, JS) allowed for wider consideration of the analysis process, which should have limited the effects of this possible bias.
Implications for practice and research
There are three stages in a person’s CF/CFRD illness transition where enhanced practice-based interventions would be beneficial.
Pre-CFRD diagnosis
Annual screenings and other contacts with specialist CF services provide opportunity to routinely educate people about CFRD, including the increased likelihood of its occurrence as people age, and to address any misconceptions about the condition. Emphasising causation and treatment differences between CFRD and T1/2DM at an early stage may head off the tendency for some people to use their knowledge of T1/2DM as a basis for managing CFRD once diagnosed.
At the point of diagnosis
Participants reported difficulties adjusting to their new health status and to their sense of self-identity, and for some, these difficulties were protracted. Services need to be sensitive to the psychosocial impact of the diagnosis and emotional support may be needed into the medium term.
Written, take-away information or online resources about CFRD and its management need to be made available at the point of diagnosis. Cystic fibrosis charities such as the CF Trust and CF Foundation have online discussion groups for peer support, which given the segregation practices used to avoid cross-infection between people with CF, may be helpful.
Ongoing management
Services need to support self-care knowledge and abilities, and encourage the integration of CFRD care into routine CF management. It should not be assumed that people will easily adjust to managing CFRD because they are already experts in their CF care. Active, ongoing problem-solving of any obstacles may be necessary. Parents also need support to adjust to the new health status of an adolescent, and encouragement to practise autonomy supporting behaviours by recognising and valuing their adolescent’s contributions to self-care.
The limited empirical research that was found into the most typical co-morbidity of the most common life-limiting inherited disease in the Caucasian population is of some concern. Further research is now needed to build on this work to refute or confirm its findings and to deepen our understanding of the experience of living with and managing CFRD. It would be particularly beneficial to explore the experiences of different groups of people with CFRD, this could include those who are newly diagnosed with CFRD or the groups where recruitment can be more challenging such as adolescents and young adults. This systematic review did not assess the impact of different stages of CF disease, it would be valuable to gain understanding of the CFRD management experiences at different stages of illness trajectories, for example, what are the additional challenges to living with and managing CFRD for people with end-stage CF, during transition to adult care, following a lung transplant or during pregnancy?
To improve CFRD management and knowledge and to optimise glycaemic control further research is also needed to support the development of appropriate CFRD self-management education programmes, this includes the exploration of CFRD self-management behaviours and identification of self-management requirements.
Since the completion of this systematic review the health and lives of people with CF have been dramatically transformed by the introduction of treatments designed to correct the underlying genetic defect. CF is caused by an impairment of the cystic fibrosis transmembrane conductance regulator (CFTR) protein; CFTR modulators target the defective CFTR protein. Cystic fibrosis transmembrane modulator therapy is regarded as one of the greatest advancements in CF but due to its infancy there is very little research knowledge, particularly qualitative work, about its impact upon patients’ experiences of their new reality such as their expectations for life and health, well-being, self-care needs and values. The impact of CFTR modulators on diabetes is also not fully established. With this enormously changed health context we need to identify changes in the experiences of living with and managing CFRD to understand what patients’ health and wellbeing needs are now.
Conclusion
This is an important review of an under-researched condition with findings that increase awareness of people’s experiences of CFRD, and identify potential areas for practice development. Nurses are at the forefront of care delivery to people with CF, both in specialist and non-specialist settings. Participants from studies included in this review called for better knowledge and integration of CFRD into CF services. Review findings indicate opportunities for CFRD interventions pre-diagnosis, at diagnosis, and during ongoing management. Nurses in partnership with their MDT colleagues might usefully draw on this work to review their existing practices.
• People with cystic fibrosis (CF) should be routinely screened for and educated about cystic fibrosis related diabetes (CFRD), including its causal link to CF and the treatment differences between CFRD and Type 1/2 diabetes mellitus. • People need support to develop CFRD self-care knowledge and abilities, and to integrate these into their CF management routines. • Nurses are at the forefront of specialist and non-specialist CF care and need to incorporate phase-specific CFRD interventions into their routine practices. • Services need to be sensitive to the psychological and social impact of a CFRD diagnosis and provide opportunity for people to discuss the emotional challenges they encounter • Cystic fibrosis diabetes (CFD) is a more accurate diagnostic term than CFRD and may foster better integration of the two conditions.Key points for policy, practice and/or research
Supplemental Material
Supplemental Material - The experience of living with and managing cystic fibrosis related diabetes: a qualitative review
Supplemental Material for The experience of living with and managing cystic fibrosis related diabetes: a qualitative review by Sarah Collins, Andrew Jones, Sue Woodward and Jackie Sturt in Journal of Research in Nursing
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article represents independent research arising from a Clinical Doctoral Research Fellowship. Sarah Collins, ICA-CDRF-2015-01-023 is supported by the National Institute for Health Research and Health Education England. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research, Health Education England, or the Department of Health.
Ethical approval
Ethical approval was not required for this systematic review.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.