
Abstract
Introduction:
During the COVID-19 pandemic, nursing personnel presented a higher prevalence of fear of contagion, anxiety symptoms, depression, and burnout syndrome. However, the variables associated with these conditions in Mexico are unknown.
Objective:
To determine the clinical, sociodemographic, and psychological variables associated with fear of contracting COVID-19 and burnout syndrome in nursing personnel.
Methods:
The study was a cross-sectional correlational study. It included 423 Mexican nursing professionals, working in public and private institutions, of different specialties aged 18–61 years (M = 36 years), the sampling was non-probabilistic by convenience. The instruments used were: COVID-19 fear scale, Maslach Burnout Inventory, Generalized Anxiety Disorder Scale-7 and Patient Health Questionnaire-9. Multinomial logistic regression models were used to analyse the results.
Results:
The factors associated with fear of contagion were anxiety symptoms (Odds Ratio [OR]: 7.806, p < 0.05), caring for patients with COVID-19 (OR: 5.460, p < 0.05, 0.001) and mild emotional exhaustion (OR: 5.181, p < 0.05). The syndrome dimensions were: depressive symptoms (OR: 12.062; 7.667, p < 0.05), fear of contagion (OR: 4.978; 4.913; 4.921; 4.921, p < 0.01), marital status (OR: 3.404; 3.219, p < 0.05) and young age (OR: 1.064; 1.084, p < 0.05).
Conclusions:
The factors associated with fear of contagion and burnout syndrome found were having clinical psychological symptoms, as well as being young, being single, being married and being in the health system caring for patients with COVID-19.
Introduction
By July 2021, the COVID-19 pandemic had generated a global prevalence of 183,198,019 confirmed cases, with a total of 3,971,687 deaths (Johns Hopkins Coronavirus Resource Center, 2021; Pan American Health Organization, 2020). One of the population groups most affected by infection since the first wave was health personnel, at least 570,000 cases of COVID-19 had been reported in this group worldwide (International Council of Nurses, 2020). While in Mexico, 2,531,229 positive cases and 233,425 deaths had been registered, with nurses being the most affected group with the highest number of infections with 92,924 (39.7%) cases and 700 deaths (Lozano-Vargas, 2020; Secretary of Health, 2021).
These figures, together with the short time to treat patients due to the critical condition in which they arrive, scarce human and material resources, and the longer time spent in the care rooms providing care, cause nursing staff to be at risk for fear of contagion, symptoms of anxiety, depression, burnout syndrome, concern for the family, conflicting interpersonal relationships with partners or family, isolation, work overload, less rest time, high level of demands and long working hours (Cai et al., 2020; Greenberg et al., 2020; Silva-Gomes and Silva-Gomes, 2020). Among the conditions, fear of contagion and burnout syndrome stand out, since they have greatly impacted the health of the nursing team (Cruz et al., 2021).
Fear of contagion refers to the underlying concern about acquiring an illness with a possible fatal outcome (Hawryluck et al., 2004; Person et al., 2004). Prevalence within nursing staff has been shown to range from 43% to 95% (Hu et al., 2020; Salazar de Pablo et al., 2020). It has been reported as the second most prevalent in nursing staff, as in the study by Liu et al. (2020), where it was found that all staff in charge of treating patients diagnosed with COVID-19 are afraid of contagion and have even chosen to live in isolation from their families, in order to avoid contagion.
Regarding burnout syndrome, this is a psychological syndrome in response to chronic stressors that develops in those subjects who work with people in any type of activity, characterised by the feeling of emotional exhaustion (EF), depersonalisation and reduced personal fulfilment (PR) (Maslach et al., 2001). Burnout damages the quality of life of the professional, as well as the quality of his or her healthcare work, since it can cause dysfunctional behaviours, such as, errors in medication doses application, delays in treatment, communication failures, and absenteeism; which in turn, makes it extremely difficult for health personnel to perform their work (Calle Hermina, 2020; Culquicondor, 2020).
Burnout, even before the pandemic, was present in various workers of the nursing group, since in Mexico at least 15–50% of the personnel suffered from this syndrome (Medina, 2017). In addition to the prevalence, it is known that during the pandemic, the estimated prevalence for Mexican nursing professionals has been estimated to be between 15% and 43% (Álvarez et al., 2021; Juárez-García, 2020).
While its overall prevalence during the pandemic has been estimated to be between 30% and 60%, as in the study by Hu et al. (2020), in which 60% of a sample of 2014 nurses were found to have moderate-high levels of EF, 42% reported high levels of depersonalisation (DE) and 60% suffered from low PR. Matsuo et al. (2020) identified that 46% of a sample of 126 nurses suffered from this syndrome.
Few studies have mentioned the relationship between psychological conditions such as anxiety or depression with the presence of fear of contagion and burnout syndrome during the COVID-19 pandemic. Especially, when talking about burnout, this variable has been linked to a greater extent with psychosocial and personal aspects such as age, sex, marital status, work climate, position held, working hours, and conflictive or limited interpersonal relationships (Giusti et al., 2020; Maslach et al., 2001; Saquero et al., 2018).
Finally, it should be noted that most of the research documenting the psychological impact on the nursing team comes from countries such as China, Italy, and Spain, since they are the countries that were most affected by the pandemic at the beginning. However, it is still necessary to know how the health crisis has impacted Mexico and Latin America, where the prevalence of the effects is beginning to be documented (Pappa et al., 2020). For this reason, the present study had the following objectives: explore if there are differences in the prevalence of psychological affectations between nursing personnel who requested leave and personnel who were working, and to determine the factors associated with fear of contagion and burnout syndrome in nursing personnel during the COVID-19 pandemic in the months of March to August 2020.
Methods
This was a cross-sectional correlational study, which included 423 nursing professionals of both sexes working in public and private hospitals in Mexico. The sample was obtained by availability. It was obtained electronically from March 2020 to August 2020. Each participant agreed to participate in the present study by signing the online informed research consent form. Nursing professionals from Mexico who worked in COVID-19 centres, general public or private health centres were included, as well as those who had cared for patients with COVID-19. Only those participants who were nursing trainees in training were excluded. Finally, questionnaires showing noncommittal responses were eliminated.
Instruments
Sociodemographic and background form
A questionnaire was designed, which inquired about sociodemographic data that could be related to burnout syndrome and fear of contagion, such as: sex, age, number of children, marital status, place of work, health status, feeling discriminated against and work situation. In addition, it contained clinical data: health status, suffering from a chronic degenerative disease, having cared for patients with COVID-19, isolation within the home due to the disease and having been previously infected with COVID-19 at some point.
Fear of COVID-19 scale
Developed by Kwasi et al. (2020), it is a self-administered unifactorial scale made up of seven statements that are scored according to the degree of agreement that the person gives to the statements. The minimum possible score for each question is one, and the maximum is five. The total score is calculated by adding the scores of all the questions, having a minimum total of 7 and a maximum total score of 35, with the maximum being an indicator of high or high fear, while the low score indicates presence of minimal fear. It has an internal consistency of α = 0.82 and a reliability of internal conscience (ICC) = 0.72, while in the version for Mexican population validated by Galindo (2020), the internal consistency was α = 0.82 and a reliability of ICC = 0.88.
Maslach burnout inventory
Developed by Maslach et al. (1997), it consists of 22 questions, which are grouped into three dimensions: EF, depersonalisation, and PR. The items inquire about the frequency with which certain feelings related to the syndrome are experienced, and are scored from 0 to 6, obtaining a specific score for each of the dimensions that can be interpreted under the following cut-off points: EF: 18 low, 19–26 medium and 27 high, Depersonalisation: 5 low, 6–9 medium and 10 high, and PR: 33 low, 34- 39 moderate and 40 high. In Mexican population conducted by Meda et al. (2008), the internal consistencies of the subscales were: α = 0.86 (CE), α = 0.82 (RP) and α = 0.53 (DE), besides explaining 47% of the variance.
Generalized anxiety disorder scale
Developed by Spitzer et al. (2006), self-administered unifactorial scale made up of seven items that evaluates anxiety symptoms in Likert format from 0 to 3 points, obtaining scores between 0 and 21 points. The score obtained is interpreted according to the cut-off points: 0–4 minimal, 5–9 mild, 10–14 moderate and 15–21 severe. It has a unidimensional structure that explains 63% of the variance and an overall Cronbach’s alpha of 0.92. In the Mexican version validated by Mendoza et al. (2020), for the general population, the overall Cronbach’s alpha was 0.87 and 57.75% of the variance.
Patient health questionnaire
Developed by Kroenke et al. (2001), it is a nine-item self-administered unifactorial scale that assesses symptoms of depression, which has also been used in nursing professionals (Camargo et al., 2022). The items are scored from 0 to 30 and a maximum score of 27 points and a minimum of 0 points is obtained. The score obtained is classified according to the cut-off points of the scale, which are: 0–4 minimum, 5–9 mild, 10–14 moderate, 15–19 moderately severe and 20–27 severe. It has an overall Cronbach’s alpha of 0.89. In the Mexican version validated by Mendoza et al. (2020), for the general population, the overall Cronbach’s alpha was 0.85 and explains 47% of the variance.
Statistical analysis
Statistical analyses were performed in SPSS software version 21 (Document number: 213045). A central tendency analysis (mean and frequency distribution) was used to identify the prevalence of the psychological variables. The Mann Whitney U test for independent samples was also chosen. In addition, a Pearson correlation analysis was performed between the clinical and sociodemographic psychological variables. Only the psychological, clinical, and sociodemographic variables in which statistically significant correlations were identified were included in the multinomial logistic regression analysis for each of the variables ‘fear of contagion and burnout’, in which a statistical significance level of p < 0.05 was used.
Results
Description of the sample
The sample of this study was composed of 423 participants, of whom 368 were women and 64 men, from different states of the Mexican Republic: 90 from Mexico City, 180 from the State of Mexico and 153 resided in different states. Of these, 262 had children and the largest percentage worked in public institutions (See Table 1).
Sociodemographic description of the sample (n = 423).
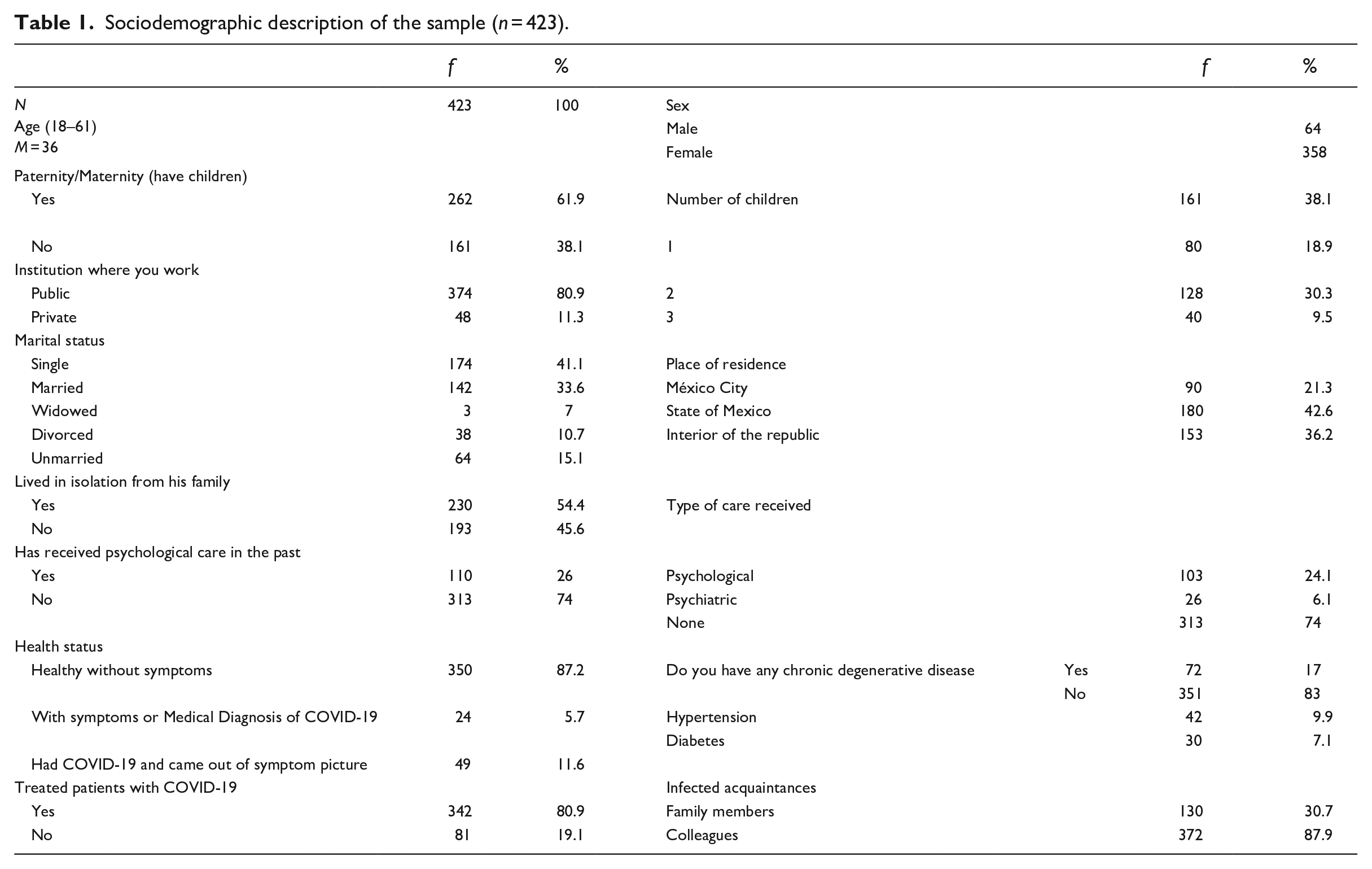
In this sample it can be observed that 54.4% isolated themselves to avoid infecting their families. Regarding clinical characteristics, 5.7% reported having symptoms or medical diagnosis of COVID-19 and 11.6% reported having been infected and leaving the symptom picture. 30.7% reported knowing of family members who had been infected and 87.9% reported knowing partners. Finally, it can be observed that 80.9% attended patients diagnosed with COVID-19 (see Table 1).
Prevalence of psychological effects
In the sample, 20.3%, presented a severe level of fear of contagion. Regarding the presence of burnout syndrome, in the dimension of EF, 20.8% were at a high level, for depersonalisation, 20.8% presented this dimension at high levels, and 26% at a low PR level. For the presence of anxiety symptoms, 10.6% were found to present severe symptoms. Finally, for symptoms of depression, 5.4% were found to have severe symptoms. Significant differences, associated to work leaves, were only found in the presence of anxiety symptoms where the scores of the personnel who requested leave (Mdn = 7, Range = 21) were higher than those of the personnel who were working (Mdn = 5, SD = 21) U = 12,615, p = 0.048.
Factors associated with fear of contagion
A model explaining between 36.2% and 38.7% of the variance was obtained, which proved to be significantly reliable x2 = 190.211 (gl = 60, p = 0.001) (see Table 2). In the model it was found that having cared for patients with COVID-19, having mild emotional fatigue, as well as having anxiety symptoms at some clinical level (minimal, mild, moderate and severe) were significant associated factors of fear of contagion (see Table 2).
Parameter estimates for the fear of contagion by COVID-19 model.
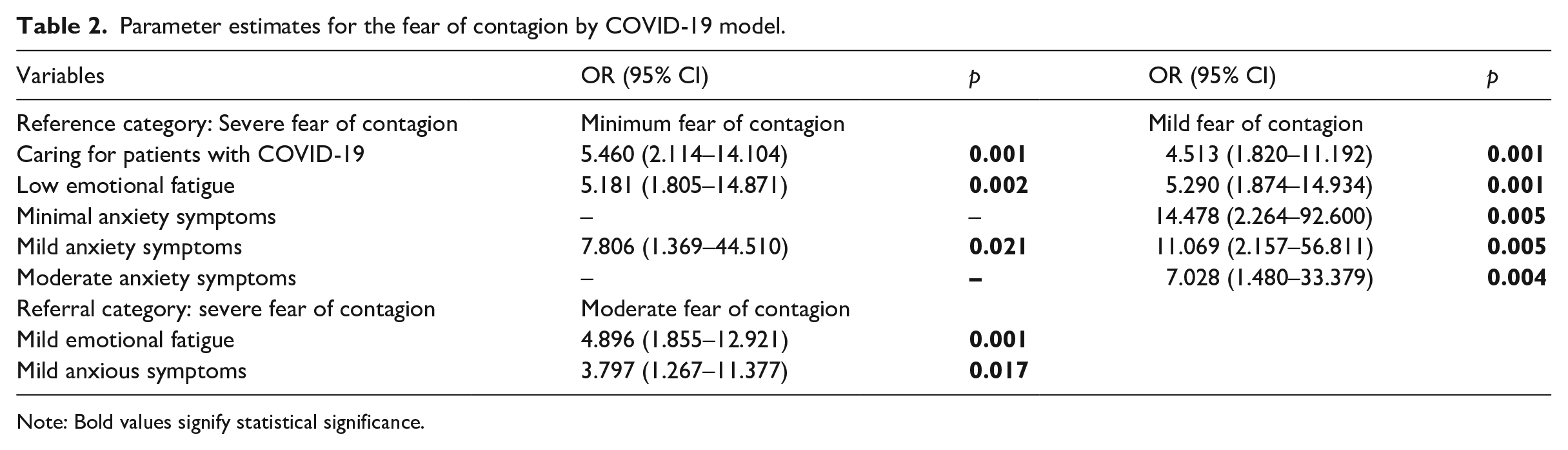
Note: Bold values signify statistical significance.
Factors associated with the dimensions of burnout syndrome
The model for EF explained 42.8% (Cox and Snell) and 48.9% (Naguelkerke) of the variance and proved to be reliable x2 = 236.374 (gl = 50, p = 0.001). Young age, being married or single, having minimal depressive symptoms and suffering from fear of contagion at some level, were positively associated with the presence of EF (see Table 3).
Parameter estimates for the emotional fatigue model.
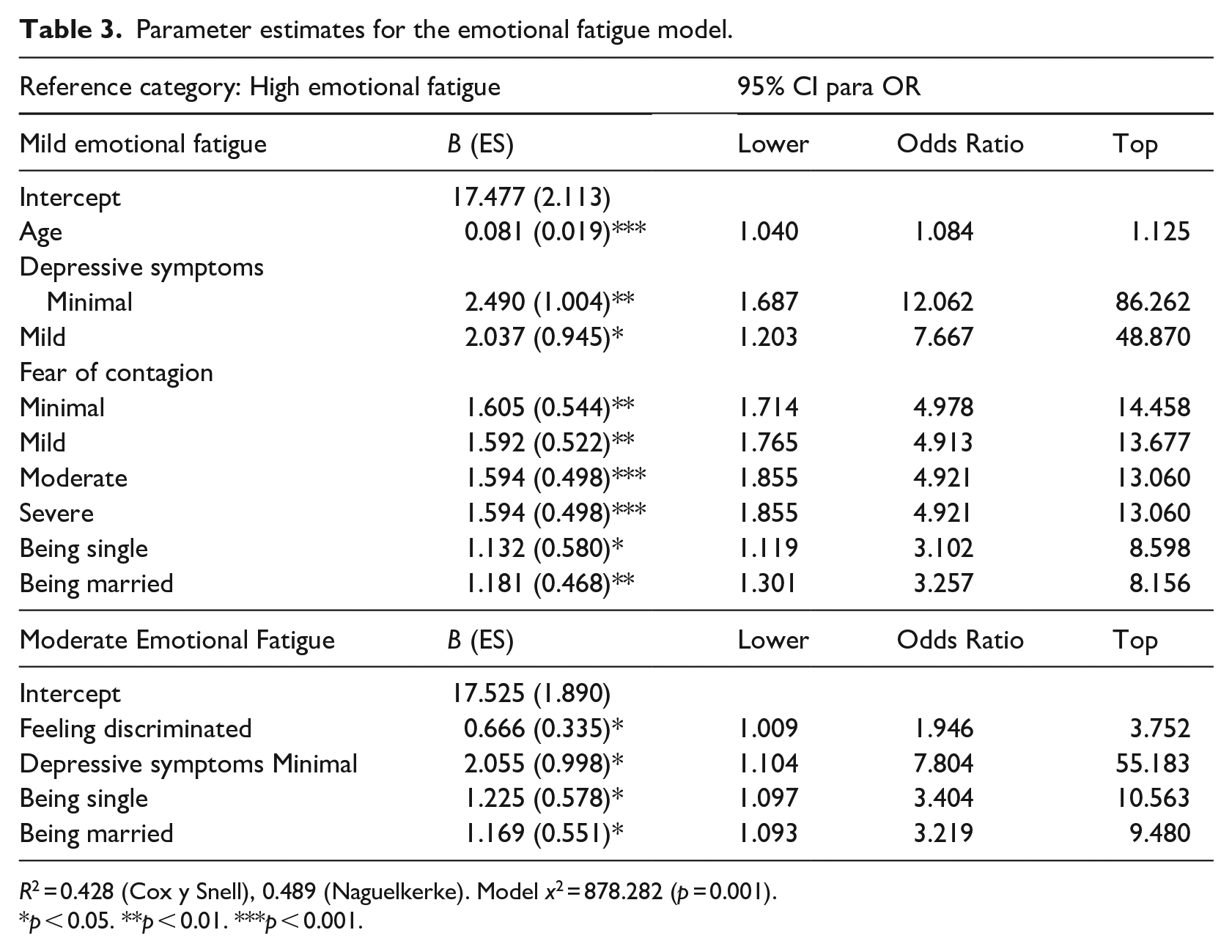
R2 = 0.428 (Cox y Snell), 0.489 (Naguelkerke). Model x2 = 878.282 (p = 0.001).
p < 0.05. **p < 0.01. ***p < 0.001.
As for the depersonalisation model, the model that was significantly reliable x2 = 122.319 (gl = 52 p = 0.001). The presence of mild anxiety symptoms was associated with a lower probability of suffering depersonalisation in any of its levels. While young age, presenting minimal and mild depressive symptoms were positively associated with susceptibility to the presence of depersonalisation symptoms at any of their levels (see Table 4).
Parameter estimates for the cynicism model.
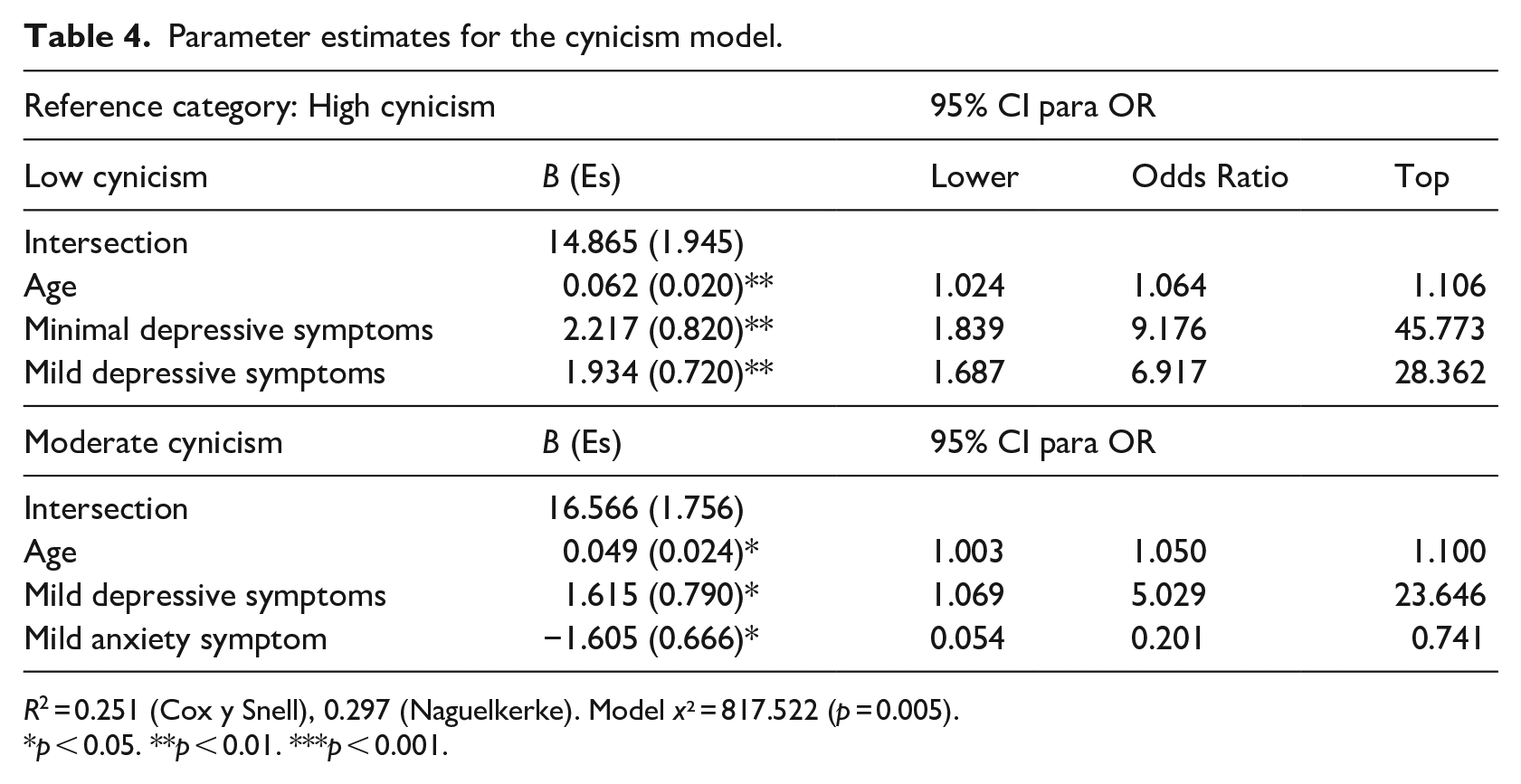
R2 = 0.251 (Cox y Snell), 0.297 (Naguelkerke). Model x² = 817.522 (p = 0.005).
p < 0.05. **p < 0.01. ***p < 0.001.
Finally, the model of low self-actualisation was significantly reliable x2 = 128.738 (gl = 52 p = 0.001). In this model, sociodemographic and psychological predictors were found. It should be clarified that in this model negative relationships are associated with the presence of low self-fulfilment; it was observed that young age, minimal depressive symptoms, minimal fear of contagion and having children were positively associated with low self-fulfilment (see Table 5).
Parameter estimates for the low self-efficacy.
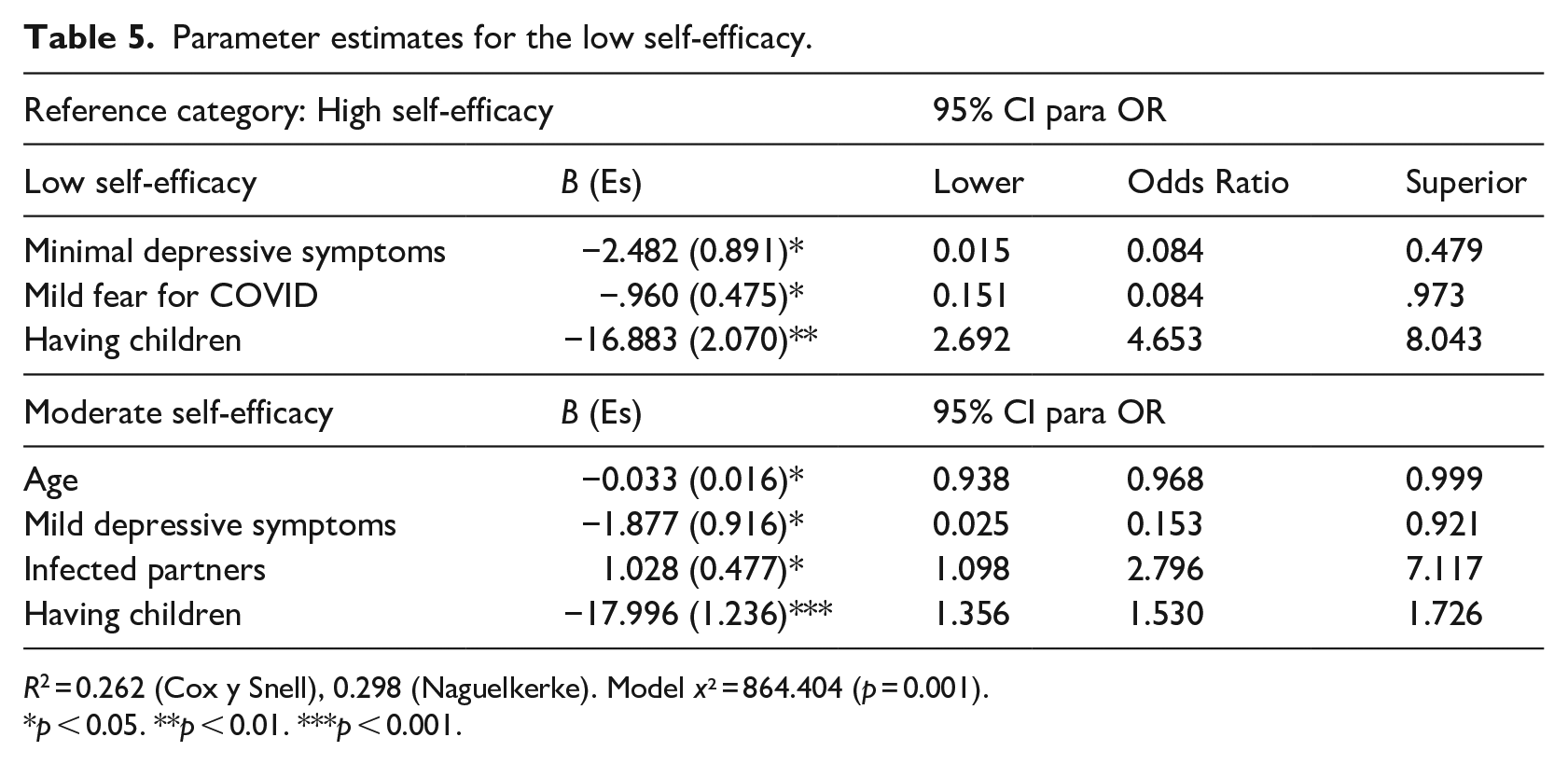
R2 = 0.262 (Cox y Snell), 0.298 (Naguelkerke). Model x² = 864.404 (p = 0.001).
p < 0.05. **p < 0.01. ***p < 0.001.
Discussion
Variables associated with the dimensions of burnout syndrome and fear of contagion were found. The factors significantly associated with the presence of the dimensions of burnout syndrome were: young age, having children, being single or married and feeling discriminated against had a greater association with the quality of life of nurses by increasing emotional fatigue and depersonalisation. The variables associated with fear of contagion were providing care to patients with COVID-19, symptoms of health-related anxiety, and suffering from emotional fatigue.
Regarding the variables associated with fear of contagion, these are consistent with the results observed in research in Asian and European countries. Where it had been reported that being part of the team in charge of providing care to people diagnosed with this disease, suffering symptoms of health anxiety as well as suffering emotional fatigue at some level, were variables that were positively related to the presence of fear of contagion (Hu et al., 2020; Jackson et al., 2020; Liu et al., 2020; Mertens et al., 2020). This would be an important point to generate psychosocial support with the aim of preventing fear from making it impossible for personnel to participate in interventions, since misinformation or even excessive information can lead to people being terrified of contracting the disease. Similarly, it will be important to integrate stress reducing techniques such as diaphragmatic breathing, mindfulness, progressive relaxation, guided imagination within the care programmes for the management of emotional dysregulation, as well as for the related symptoms (Fuentes and Zúniga, 2021).
Regarding the variables associated with burnout syndrome, the results coincide with those observed in other studies conducted during the pandemic, where there was a relationship of sociodemographic factors with the presence of the syndrome within the nursing staff, which may be due to the fact that being young with less experience in their work, is related to more stress and self-criticism (Calle Hermina, 2020; Hu et al, 2020). Further, studies have shown that stress and lack of social support due to feeling discriminated against, as well as, poor interpersonal relationships with partners, friends or family, are a risk factor for developing burnout (Palacios and Paz, 2021; Silva-Gomes and Silva-Gomes, 2020).
In addition, it will be important to implement interventions focused on helping people who are at greater risk, such as young nurses with children who are single or married, since these were at higher risk in comparison with being divorced or widowed. As for the group of single staff with a child, stress may increase because of childcare concerns and childcare cost/expenses, making them more prone to burnout. It will be important to implement interventions where they are provided with strategies and coping with stress, relaxation techniques and support with pragmatic and financial needs (Manzano, 2020). While for those who are married, the quality of the relationship, support in childrearing activities, and presence of domestic violence might also be factors of influence, which has been mentioned to have increased during this pandemic, due to social isolation (Huarcaya-Victoria and Calle-Gonzáles, 2020).
Similarly, other studies conducted with nursing professionals have identified the relationship of burnout syndrome with depression and fear of contagion (Giusti et al., 2020), which can be explained by being exposed to risk situations such as being infected and situations of work overload which are situations that generate stress and emotions linked to emotional fatigue and depersonalisation (Hu et al., 2020; Huarcaya-Victoria and Calle-Gonzáles, 2020; Nishimura et al., 2019). In addition to implementing social support techniques aimed at people who became isolated or had to be quarantined, as well as for allowing adequate mourning in situations where a family member or beloved companion died, which will decreased such conditions (Palacios and Paz, 2021).
Since it is a health crisis with a great demand and risk for health, people are more likely to develop mental disorders during or even after the pandemic. These changes in mental health will in turn have repercussions on the number of personnel who will be able to provide care to patients who require it, since this pandemic will bring with it an increase in mental illnesses and related symptoms such as anxiety, depression and post-traumatic stress (Palacios and Roman, 2021).
It should be noted that, although burnout syndrome was associated with depressive symptoms, fear and anxiety symptoms, these associations were only present in minimal and mild symptomatology. Some research reports that the relationship with higher levels of symptomatology indicates comorbidity of disorders rather than a risk factor (Orellana and Orellana, 2020). Therefore, having comorbid disorder can cause absenteeism and incapacity to work in healthcare (Calle Hermina, 2020).
Finally, although there were variables associated with fear of contagion and burnout syndrome, the proposed models are not fully compatible; this may be similar to the previous experience that Asian countries had with other infectious diseases (MERS and SARS), which had promoted learning about the implication and how to manage epidemiological crises and epidemics (Lavell et al., 2020).
The pandemic was unparalleled and was a novel experience in Latin America. Because of this, the media initially promoted erroneous and contradictory information about what the pandemic was about. pandemic. Therefore, the social representation of the pandemic may generate an influence and predict fear of contagion and burnout syndrome.
Limitations and future perspectives
Among the limitations of this study is that the area of care in which the nurses worked was not identified, which may influence the scores and related factors, since work areas such as emergency or intensive care are areas of great chronic stress, even before the pandemic. Similarly, there was no psychiatric interview to identify personnel who had a prior diagnosis of any of the psychological conditions. In addition, the sample was collected during the early stages of the pandemic (from March 2020 to August 2020), so it is possible that the levels of burnout related to the pandemic were just beginning, and a baseline was not used to determine whether there was already a prevalence of this condition in the sample before the study. Longitudinal studies were needed to understand the evolving nature of these conditions. Regarding future perspectives, it is hoped that other research can use these data to generate interventions focused on reducing the impact of the associated variables to prevent nursing personnel from having serious mental health problems in the future. In addition, prospective longitudinal studies are suggested to strengthen the internal validity of the findings of this study.
Conclusions
The situation faced by the nursing teams may have repercussions on their mental health, presenting symptoms, while the COVID-19 pandemic is still having an impact in that they might worsen over time, which will cause these personnel to be prone to develop various mental health problems.
Therefore, it is important to identify the risk factors of nursing professionals, in order to determine their impact on the development of mental illness in Mexican nurses, who are working in a country where the number of infections has been high and the amount of material resources has been scarce, which can generate greater workload, worry, and therefore greater stress (Secretaria de Salud, 2021).
In addition, these risk factors identification may strengthen public mental health programmes, as well as, contribute to improve health policies that will help determine which professionals require greater support by risk stratification and risk for developing a mental disorder or clinically significant psychological symptoms that limit their functional activity. This will prevent a loss of human resources by intervening specifically with at-risk personnel.
Key points for policy, practice and/or research
Determining the correlates of fear of contagion and burnout syndrome makes it possible to generate a triage that helps to identify nursing personnel who are at risk of developing any of these affectations as part of the quality indicators in the Mexican health system.
The correlates of fear of contagion and burnout syndrome reported in this study can form part of the variables to be evaluated during the assessment of the mental health status of health professionals.
Likewise, knowledge about the risk factors can be taken into account for the development of psychological interventions aimed at addressing the needs of the personnel.
The clinical and sociodemographic factors found in this study can serve health institutions and provide tools that help professionals to take other preventive measures, such as rotations of service areas so that professionals can have less exposure to the risk of contagion.
Footnotes
Availablity of data materials
The data sets generated during and/or analysed during this study are available through the corresponding author, or upon request.
Consent to participate and publish
Informed consent was obtained from all participants included in this study. Consent was submitted online using google forms; only participants who signed the consent form agreeing to participate were included. Participants signed the online informed consent regarding the publication of their data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors did not receive support from any organization for the work presented, in the preparation of this manuscript, conduct of this study. RCM is supported by the MSKCC core grant P30 CA008748.
Ethical approval
Approval was obtained from the ethics committee of the National Autonomous University of Mexico. The procedures used in this study conform to the principles of the Declaration of Helsinki.