
Abstract
Background:
Pressure ulcers rank as the third most costly disease to health care services. The prevalence in Iran for hospitalised patients is approximately 19%. This study aimed to compare the effects of Arnebia Euchroma ointment dressings with silver nanoparticle dressings on pressure ulcer healing in patients admitted to intensive care units (ICUs).
Methods:
A randomised controlled trial was conducted with patients with pressure ulcers admitted to ICUs. The patients were randomly assigned to either the intervention group, which received the Arnebia Euchroma ointment dressing (n = 30), or the control group, which received silver nanoparticle dressing (n = 30). Three assessments, including one pre-intervention, one during, and one after the intervention on day (1, 7, and 12), were conducted using the Pressure Ulcer Scale for Healing (PUSH) and Nonverbal Pain Scale (NVPS) to evaluate the healing progress and pain intensity levels over time.
Results:
The study results revealed that both the Arnebia Euchroma ointment and silver nanoparticles had positive effects on wound healing; there was no significant difference between the two treatments. The mean pain intensity decreased on the first, seventh, and twelfth days; and there was a significant difference between the two groups. Patients in the Arnebia Euchroma ointment group experienced lower pain intensity during and after dressing on the first, seventh, and twelfth days.
Conclusion:
Wound healing was expected in the silver nanoparticle group, whereas promising results were also observed in the Arnebia Euchroma ointment dressing group. Since the full effects of silver nanoparticles on humans and the environment are still unknown, the use of locally sourced herbal medicines such as Arnebia Euchroma can be considered as an alternative, or even in combination with silver nanoparticles.
Background
The skin, the body’s largest organ, plays a crucial role in protecting internal organs from environmental harm (Muhammed et al., 2020; Rashdan and El-Naggar, 2023). Pressure ulcers pose a significant global challenge for healthcare professionals (Mervis and Phillips, 2019). These ulcers are characterised by damage to the skin or underlying tissues, typically occurring on bony prominences due to prolonged pressure or friction caused by movement (Berman et al., 2021). Local ischaemia, a restriction in blood supply to any tissue, is the underlying cause of pressure ulcers. The body tissue experiences continuous pressure between surfaces such as beds or chairs, leading to reduced blood flow. This deprivation of oxygen and nutrients leads to the accumulation of metabolic waste products within cells, ultimately resulting in tissue death (Khakhkhar, 2020).
Pressure ulcer prevalence serves as an important and sensitive indicator for measuring the quality of nursing care worldwide (Abdi et al., 2018). In the United States, the annual incidence of pressure ulcers affects one to three million individuals (Haugen and Galura, 2019; Saghaleini et al., 2018) leading to over 60,000 deaths each year (Berman et al., 2021). Pressure ulcers, the third most costly condition following cancer and cardiovascular diseases, account for approximately 4% of the annual healthcare budget in Europe (Hajhosseini et al., 2020). In the United States, pressure ulcers costs $9.1 to $11.6 billion per year, with individual patient costs ranging from $20,900 to $151,700 per pressure ulcer (Agency for Healthcare Research and Quality, 2014). These costs continue to rise each year (Fashaei et al., 2024). Research conducted by Andrade et al. (2016) revealed that the overall cost of care for patients with pressure ulcers was approximately 22.5% higher than that for other patients (Andrade et al., 2016). A systematic review conducted by Karimian et al. (2016) showed that the prevalence of pressure ulcers in hospitalised patients in Iran was 19% and this prevalence tended to increase with age. The loss of the protective layer of the skin due to pressure ulcers increases the risk of infections, leading to prolonged hospitalisation, increased costs, and potential health complications for patients (Karimian et al., 2016).
Pain is a significant complication of pressure ulcers (Moore et al., 2019). The pain associated with these wounds is frequently described as constant and relentless. It is important to avoid friction-induced skin disorders and instead, use medications and specialised equipment for pain relief (Ham et al., 2016). Pain resulting from pressure ulcers can significantly affect an individual’s quality of life, disrupting daily activities, and the rehabilitation process. The intensity of this pain is not always correlated with the severity of the pressure ulcers (Jackson et al., 2017). All stages of pressure ulcers are associated with pain (McGinnis et al., 2014). Moreover, oral painkillers may not effectively alleviate pressure ulcer pain, leading to increased usage and potential side effects (Ferris et al., 2019). In a qualitative study by Jackson et al. (2017) involving 12 nonverbal patients with pressure ulcers, it was reported that these patients experienced significant challenges in expressing and communicating the intensity of their pain to their caregivers . Additionally, the act of dressing a wound itself can be a source of pain (Carrere et al., 2021).
An ideal dressing should be nontoxic, prevent bacterial infections, adhere well to the wound site, maintain a moist environment, possess high absorbency, allow air permeability and resemble the skin’s structure (Lee and Choi, 2024; Muhammed et al., 2020). The optimal temperature of the wound site should also be maintained, and pain should be minimised during dressing application and removal. However, dressings with these characteristics are often expensive (Etafa et al., 2018), and insurance companies in Iran typically do not cover their costs, making them inaccessible to many patients, particularly in regions with lower quality of life indices (Pouraskari et al., 2024; Sharif et al., 2018). One potential solution to this problem is the utilisation of locally available medicinal resources in Iran, which are affordable and easy to use (Safdari et al., 2021). Traditional societies are often characterised by their tendency to preserve indigenous customs and ancient cultural practices. In many countries, the use of herbal materials plays a crucial role in fulfilling basic healthcare needs. Africa and Asia, in particular, have a rich tradition of using herbal medicines (Kakooza-Mwesige, 2015).
Arnebia Euchroma, native to southeastern Iran, has been traditionally used for its ability to heal wounds and burns, reduce inflammation, and relieve pain. The root of Arnebia Euchroma contains beneficial compounds such as shikonin, naphthoquinone, and alkannin (Devi et al., 2021; Hoseini-Tahmasbi et al., 2013; Varaei et al., 2018), which have been identified for their antioxidant activity (Jain et al., 2021). These substances possess various properties, including wound healing, antifungal, antiviral, antimicrobial, anti-parasitic, and anti-inflammatory activities (Nasiri et al., 2016; Zhang et al., 2020; Zhu et al., 2022). The alkaloids found in plant root help reduce the levels of reactive oxygen species, such as malondialdehyde and carbonyl protein, which can lead to cell membrane dysfunction. This helps prevent oxidative stress, reduce inflammation, and aid in wound healing (Wang et al., 2020). Furthermore, the root of Arnebia Euchroma contains sterols, steroidal glycosides, and triterpenes; which have strong anti-inflammatory and analgesic properties without chemical toxic effects (Fan et al., 2013). Recent studies have investigated the effects of Arnebia Euchroma on the healing of second- or third-degree burn wounds, as well as its potential for relieving pain and inflammation in patients with osteoarthritis, rheumatoid arthritis, and post-haemorrhoidectomy pain (Rajabi and Saghafi, 2022; Varaei et al., 2018; Zhu et al., 2019).
Silver can exist in three different forms: ionic particles such as silver nanoparticles, organic compounds such as silver alginate, and inorganic compounds such as silver oxide (Khakhkhar, 2020). The use of nanoparticles allows for the slow and continuous release of silver, which not only enhances the effectiveness but also reduces the required dosage and potential complications associated with silver usage (Seyyedmir et al., 2011). These nanoparticles are particularly suitable for treating infections that are multi-drug resistant and do not respond to common treatments (Lee et al., 2019). Despite the clinical effectiveness of silver nanoparticles in accelerating wound healing and preventing infections, concerns have been raised regarding their potential long-term side effects on internal organs, such as accumulation in the liver and kidneys (Jia et al., 2020; Rafiei et al., 2020; Zhang et al., 2016, 2020). These limitations underscore the need for developing safer alternatives with comparable therapeutic effects. This study aimed to compare the effects of Arnebia Euchroma ointment and silver nanoparticle dressings on wound healing and pain severity in patients with a pressure ulcer.
Methods
Trial design
This clinical trial follows a two-centre, two-group, double-blind design, with two parallel groups receiving phase II and III drugs. The study protocol was developed based on the Standard Protocol Items Recommendations for Interventional Trials (SPIRIT)(Chan et al., 2013). It was conducted between September 2022 and May 2023 in two hospitals in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines (Merkow et al., 2021). We did not have placebo control group as research has shown that dressing only with traditional sterile gauze has less efficacy in comparison with the other dressing (Geng et al., 2023; Zhang et al., 2023), and it was not ethical to deprive the patients of a more effective dressing. So we decided to compare the efficacy of Arnebia Euchroma with silver nanoparticle dressings. Silver nanoparticle dressings have been used as a broad-spectrum antimicrobial agent, and their efficacy has been reported in many investigations (Burdușel et al., 2018; Pang et al., 2023).
Sampling and study setting
The research was conducted with patients with pressure ulcers hospitalised in the Intensive Care Unit (ICU) departments of two hospitals. The inclusion criteria were as follows: patients over 18 years old with Stages 2, 3 or 4 pressure ulcers, inability to communicate verbally (non-verbal patients were included in the study because they present unique challenges in pressure injury assessment and management), presence of pain in the wound site, albumin level above 3 mg/dL which indicates good levels of nutrition – important for wound healing; and no history of kidney, liver or autoimmune diseases – which could alter wound healing. The exclusion criteria included individuals with a history of allergy to Arnebia Euchroma, silver and artificial jewellery, as well as those who had previously removed or replaced the dressing before the interventio n. Additionally, patients who experienced kidney failure (GFR < 30 mL/min/1.73 m2) or liver failure (AST > 50 U/L or ALT > 55 U/L) during the intervention were excluded from the study.
Sample size
A sample size of 60 patients was determined via G Power Software V.3.1.9.4 (Psychonomic Society, Madison, WI, USA). The parameters used for the estimation were α = 0.05, power (1-β err prob) = 0.80, effect size = 0.95 and confidence level 0.95. Based on a previous study investigating the impact of nano-silver particles on ulcer healing in patients (Asgari et al., 2022), the chosen sample size was considered sufficient in terms of statistical power and effect size.
Randomisation and allocation
Participants were allocated to either the intervention or control groups via a convenience sampling method. Random sequence generation was utilised for randomisation. The random number table was selected for this purpose, generating a collection of numbers in a completely random manner, without any specific pattern or order. In this study, a random number table was used to assign participants to the intervention group (even numbers) or the control group (odd numbers). The numbers in the table were read from left to right.
In this study, allocation concealment was achieved through the central randomisation method. A random sequence was assigned to an individual in each centre, and sampling was simultaneously conducted at two centres. The researcher contacted each individual and asked them about participants’ random assignment to either the intervention or control group. Given the patients’ critical condition and inability to provide consent, informed consent was obtained from their families prior to the initiation of the study, with full assurance of confidentiality and ethical handling of all patient information.
Ethics
The study was registered with Clinical Trials.gov (Registration IRCT20220308054222N1) on 2022-08-02 and approved by the Research Ethics Committee for Human Subject Research at Zahedan University of Medical Sciences, Iran (IR.ZAUMS.REC.1401.140). Participation in this study was entirely voluntary, and a written informed consent was obtained before the commencement of the study from patients’ families. All patients’ families were aware of the study’s purpose, risks and potential benefits before providing written consent. Patients’ families had the right to withdraw their patients from the study any time without any repercussions, while still receiving the treatment as usual. The study was conducted with the participants’ rights and safety protected by adhering to local Iran laws, and all methods were carried out in accordance with relevant guidelines and regulations of the Declaration of Helsinki. Every participant received a unique identification number, which protected their anonymity. Confidentiality was also confirmed.
Outcomes
Primary outcomes
This study aimed to assess the effectiveness of Arnebia Euchroma ointment and silver nanoparticles in reducing pain intensity during and after dressing in patients with pressure ulcers. The Pressure Ulcer Scale for Healing (PUSH) was employed to measure the size of the bed sores on the first, seventh and twelfth days. The Nonverbal Pain Scale (NVPS) was used to assess pain intensity on the first, seventh, and twelfth days of the study. Measurements were taken before, during, and after dressing changes on the specified days.
Measurement tools (validity and reliability)
The data collection tool comprised three parts. The first part gathered demographic information, the second part evaluated wound healing status via the PUSH, and the last part assessed patients’ pain intensity via the NVPS.
The PUSH evaluated three aspects of the wound: surface area, exudate amount, and tissue type. These criteria were used to assess the state of wound healing quantitatively, with scores ranging from 0 to 17. The wound area was measured by multiplying the maximum length by the maximum width using a millimetre ruler with an accuracy of 1:1000. The minimum score for wound area was 0, the maximum score was 10. We assessed the absorbed exudate amount based on the volume absorbed by the double-layer gauze bandage. A score of 0 indicated dry gauze, a score of 1 represented absorption of <25%, a score of 2 indicated absorption between 25% and 75%, and a score of 3 indicated absorption of more than 75%. The tissue type was scored as follows: closed tissue received a score of 0, epithelial tissue received a score of 1, granulation tissue received a score of 2, slough received a score of 3, and necrotic tissue received a score of 4 (Vaziri et al., 2021). The PUSH, developed by the International Pressure Injury Advisory Panel, is a valid and reliable instrument, as confirmed by multiple studies (Gardner et al., 2005; Günes, 2009; Stotts et al., 2001). It is also recognised and utilised as a standard measure for assessing pressure ulcer healing in nursing report sheets of intensive care units across. In this research, the scientific reliability of the PUSH was assessed by two independent wound specialists who observed 15 patients with pressure ulcers simultaneously. Separate checklists were completed, resulting in an inter-rater agreement and a kappa coefficient of 0.9.
The NVPS was developed to evaluate pain in patients who are unable to verbally communicate their pain. It consists of physiological and behavioural measurements, including five dimensions: face, activity, guarding, physiological I (vital signs such as heart rate and blood pressure) and physiological II (skin colour and sweating). Each section is scored between 0 and 2 and total score changes between 0 and 10. In the interpretation of the scale, 0–2 show no pain, 3–6 show mild pain, and 7–10 show severe pain (Kaya and Erden, 2019). The scoring for the NVPS is as follows:
Face: No sign receives a score of 0, occasional grimace receives a score of 1, and frequent grimace receives a score of 2.
Activity: Lying down in a normal position receives a score of 0, cautious movements receive a score of 1, and restless or withdrawal activity receives a score of 2.
Guarding: Lying down without putting hands over area of body receives a score of 0, splinting areas of the body receives a score of 1, and rigid receives a score of 2.
Physiological I (vital signs): Stable vital signs receive a score of 0, a change < 20 receives a score of 1, and a change >20 receives a score of 2 (HR > 20/min or SBP > 20 mmHg above the baseline). The score for this dimension ranges from 0 to 2.
Physiology II (skin colour): Warm and normal receives a score of 0, reddened or dilated pupils receive a score of 1, and paleness receives a score of 2. Each dimension is scored on a scale of 0 to 2 (Kaya and Erden, 2019; Odhner et al., 2003; Tahmasbikouhpaie et al., 2018).
The non-verbal pain scale (NVPS), developed by Odhner (2003) assesses pain in patients who are unable to communicate verbally. This tool has undergone psychometric testing in Iran (Tahmasbikouhpaie et al., 2018). In the present study, we calculated Cronbach’s alpha for each dimension of the NVPS to ensure that the items within each dimension are internally consistent. The Cronbach’s alpha values for each dimension are as follows: (face: α = [0.77], activity: α = [0.78], guarding: α = [0.72], physiology I: α = [0.71], and physiology II: α = [0.72]).
Overall, the Cronbach’s alpha for the entire scale is 0.74.
Categorisation of pressure ulcers
Pressure ulcer definition and stages: The researchers followed the Revised National Pressure Ulcer Advisory Panel (NPUAP) Pressure Injury Staging System Guidelines (Edsberg et al., 2016), which include definitions for pressure injury stages.
Stage 1: Pressure injury: intact skin with a localised area of nonblanchable erythema
Definition: Intact skin with a localised area of nonblanchable erythema may appear differently in darkly pigmented skin.Presence of blanchable erythema or changes in sensation, temperature or firmness may precede visual changes. Colour changes do not include purple or maroon discolouration; these may indicate deep tissue pressure injury (DTPI).
Stage 2: Pressure injury: partial-thickness skin loss with exposed dermis
Definition: Partial-thickness loss of skin with exposed dermis may appear when the wound bed is viable, pink or red, moist, and may also present as an intact or ruptured serum-filled blister. Adipose (fat) tissue is not visible and deeper tissue is not visible. Granulation tissue, slough, and eschar are not present. These injuries commonly result from adverse microclimate,shear in the skin over the pelvis, and shear in the heel.
Stage 3: Pressure injury: full-thickness skin loss
Definition: Full-thickness skin loss, in which adipose (fat) tissue is visible in the ulcer and granulation tissue and epibole (rolled wound edges) is often present. Slough and/or eschar may be visible. The depth of tissue damage varies by anatomical location; areas of significant adiposity can develop deep wounds. Undermining and tunnelling may occur. Fascia, muscle, tendon, ligament, cartilage, or bone is not exposed. If slough or eschar obscures the extent of tissue loss, this is an unstageable pressure injury.
Stage 4: Pressure injury: full-thickness skin and tissue loss
Definition: Full-thickness skin and tissue loss with exposed or directly palpable fascia, muscle, tendon, ligament, cartilage or bone in the ulcer and slough and/or eschar may be visible. Epibole (rolled edges), undermining and/or tunnelling often occur. Depth varies by anatomical location. If slough or eschar obscures the extent of tissue loss, this is an unstageable pressure injury.
Deep tissue pressure injury: persistent nonblanchable deep red, maroon, or purple discolouration
Definition: Intact or nonintact skin with a localised area of persistent nonblanchable deep red, maroon, purple discolouration; or epidermal separation revealing a dark wound bed or blood-filled blister. Pain and temperature change often precede skin colour changes. Discolouration may appear differently in darkly pigmented skin. This injury results from intense and/or prolonged pressure and shear forces at the bone-muscle interface. The wound may evolve rapidly to reveal the actual extent of tissue injury, or may resolve without tissue loss. If necrotic tissue, subcutaneous tissue, granulation tissue, fascia, muscle, or other underlying structures are visible, this indicates a full-thickness pressure injury (unstageable, Stage 3 or Stage 4). DTPI is not recommended to describe vascular, traumatic, neuropathic, or dermatologic conditions.
Mucosal membrane pressure injury
Mucosal membrane pressure injuries are found on mucous membranes with a history of a medical device in use at the location of the injury. Mucosal tissues are especially vulnerable to pressure from medical devices such as oxygen tubing, endotracheal tubes, bite blocks, orogastric and nasogastric tubes, urinary catheters, and faecal containment devices (Camesi et al., 2023).
Data collection
The intervention group received an Arnebia Euchroma dressing every 48 hours for a total of 12 days. The area was cleansed with normal saline and sterile gauze. After cleansing the wound, a 2-mm layer of Arnebia Euchroma ointment was applied to cover the entire wound surface. The wound was then bandaged with sterile 10 × 10 gauze and adjusted according to the wound size. The dressing area was secured in place using hypoallergenic adhesive.
Before proceeding with the main intervention, a sensitivity test was conducted by applying a layer of ointment on the patient’s arm. After ensuring that no allergic reactions occurred, the main intervention was carried out after a 30-minute period. The active ingredient in this ointment is derived from the root of the Arnebia Euchroma, which is prepared as a gel using beeswax and olive oil (Darudarman Salafchegan Company,Tehran, Iran/New Derm/Bed sore ointment).
In the control group which received silver nanoparticle dressing, the wound was first cleansed with sterile gauze and normal saline. The silver nanoparticle dressing was then applied, ensuring that it covered the outer edge of the wound within a 1-cm radius. The dressing area was secured in place using hypoallergenic adhesive.
The dressing was monitored daily, and according to the manufacturer’s recommendation, the dressing was changed when the colour of the silver nanoparticle dressing changed from light green to white, which typically occurred every 72 hours. In this study, the silver nanoparticle dressing used was AgiCoat, produced by Emad Pharmaceutical Company (Isfahan, Iran), with sizes of 5 cm × 5 cm and 10 cm × 10 cm, and a silver concentration of 1.7 ppm/cm2. The dressing was changed according to the guidelines provided by the manufacturer (Asgari et al., 2022).
Data analysis
Data analysis was conducted via SPSS 26 (IBM Corporation, New York, USA). Descriptive statistics, including central tendency and dispersion for quantitative variables, and frequency and percentage for qualitative variables, were used. The normality of the variable was assessed via the Shapiro–Wilk test. Inferential statistics involved the application of tests including: the chi-square test, independent t-test, repeated measures ANOVA test, and Fisher’s exact test. A significance level of 0.05 was considered for all tests.
Results
The results showed no statistically significant differences in age, sex, marital status, pressure ulcer location, stage of ulcer, serum albumin level, Body Mass Index (BMI), diabetes status, and opium addiction between the groups (p > 0.05; Table 1). Although BMI, diabetes, and opium addiction were not part of the initial inclusion criteria, they were analysed in the results due to their potential impact on the study outcomes. These factors emerged as relevant variables during data analysis and were considered important for a comprehensive interpretation of the findings. For context regarding opium addiction, Iran has one of the highest per capita rates of opium addiction globally, with approximately 2.8% of its population aged 15 and above affected, and accounts for about 42% of the world’s total opium consumption (United Nations Office on Drugs and Crime 2023).
Characteristics of participants at baseline (N = 60).
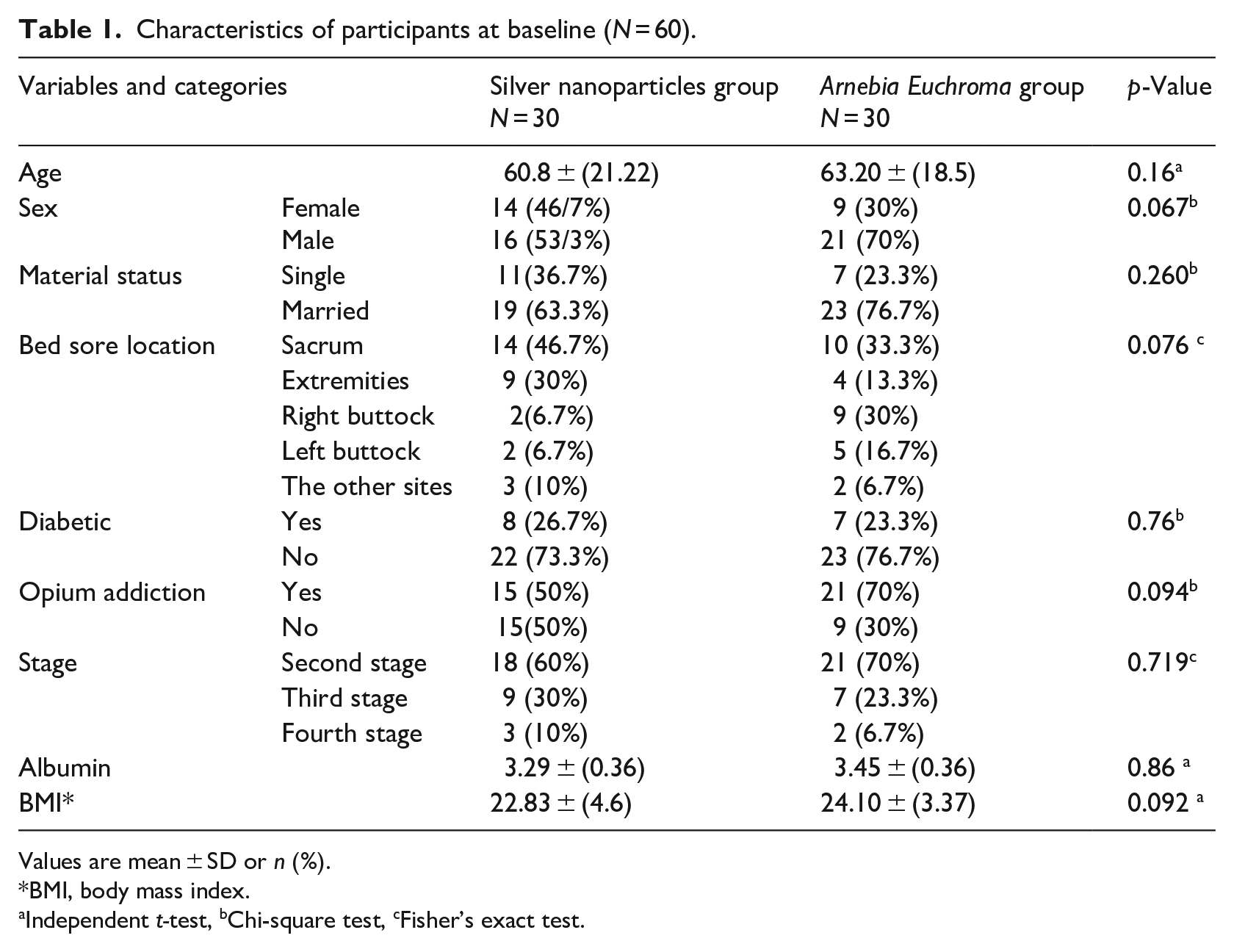
Values are mean ± SD or n (%).
BMI, body mass index.
Independent t-test, bChi-square test, cFisher’s exact test.
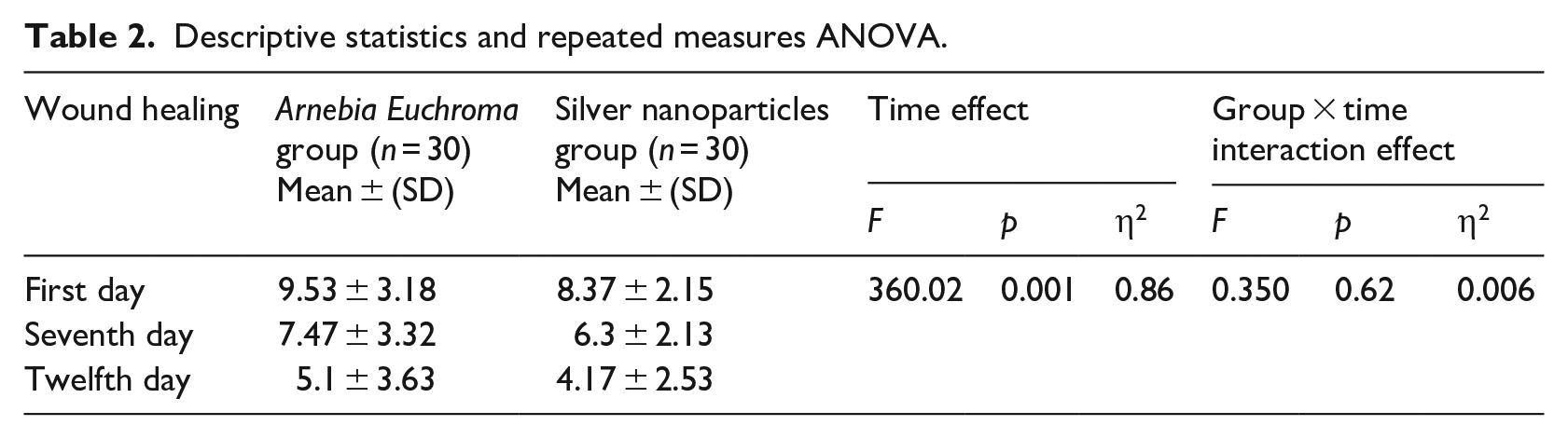
There was no significant difference in the mean wound size between the two groups before the intervention. Repeated measures analysis of variance showed that wound healing significantly improved in both groups over time (p = 0.001). The type of intervention did not have a statistically significant impact on the healing process over time (F = 0.350, η2 = 0.006, p = 0.62). Overall, the wound healing process was positive and similar in both dressing groups (Table 2).
Descriptive statistics and repeated measures ANOVA.
The results showed patients did not experience pain on the first day, before the intervention. However, there was a statistically significant difference in mean pain intensity before (T1), during (T2) and after the intervention (T3; F = 9.48, η2 = 0.14, p = 0.02). The Bonferroni test indicated that there was a significant difference in pain reduction between the groups during (p = 0.002) and after the intervention (p = 0.013). The highest mean pain intensity was recorded during dressing in both groups (Table 3).
Descriptive statistics, repeated measures ANOVA and pairwise comparisons.
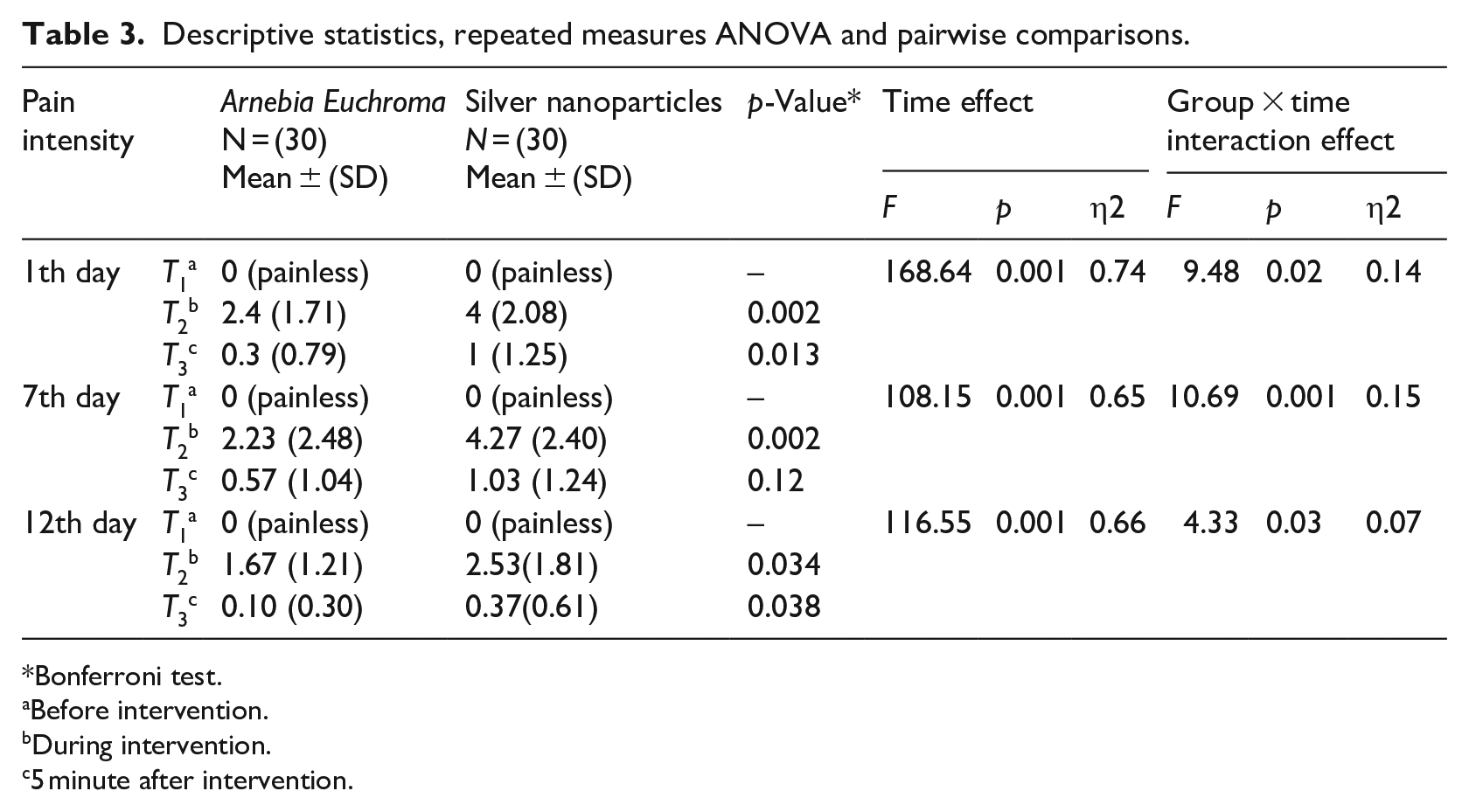
Bonferroni test.
Before intervention.
During intervention.
5 minute after intervention.
The results showed patients did not experience pain on the 7th day before the intervention. The highest mean pain intensity was recorded during dressing in both groups. There was a statistically significant difference in the mean pain intensity before (T1), during (T2) and after the intervention (T3; F = 10.69, η2 = 0.15, p = 0.001). The Bonferroni test showed a significant difference in pain reduction between the groups during intervention (p = 0.002); after the intervention, there were not a significant differences between two groups (p = 0.12). However, the mean pain intensity in the Arnebia Euchroma group was lower than the silver nanoparticles group (Table 3).
On the 12th day, the results showed patients did not experience pain before the intervention. The highest mean pain intensity was observed during dressing in both groups. There was a statistically significant difference in the mean pain intensity before (T1), during (T2) and after the intervention (T3; F = 4.33, η2 = 0.03, p = 0.07). According to the Bonferroni test, there was a significant difference in pain reduction between the groups during (p = 0.034) and after the intervention (p = 0.038). Patients in the Arnebia Euchroma group experienced lower mean pain intensity (Table 3).
The results indicated that the mean pain intensity of patients in both groups decreased over time (from the first day to the twelfth day). Patients in the Arnebia Euchroma group reported lower mean pain intensity during and after dressing on the first, seventh, and twelfth days.
Discussion
The study results revealed that both the Arnebia Euchroma ointment and silver nanoparticles had positive effects on wound healing. There was no significant difference between the two treatments. The mean pain intensity decreased on the first, seventh, and twelfth days, and there was a significant difference between the two groups. Patients in the Arnebia Euchroma ointment group experienced lower pain intensity during and after dressing on the first, seventh and twelfth days.
Both groups experienced positive wound healing outcomes. Although some studies have reported the prevalence of infection among patients with pressure ulcers to be higher than 50%, no signs of infection were observed in the patients in this study (Guest et al., 2018). In the group that used silver nanoparticles dressing, wound healing was observed, and no signs of infection were seen (e.g. purulent exudate, erythema, discolouration, or malodor). Silver nanoparticles have well-documented antimicrobial properties (Bruna et al., 2021), wounds treated with Arnebia Euchroma ointment also remained free from any clinical signs of infection, which may be related to its antibiotic and anti-inflammatory effects, consistent with findings from other studies (Aliasl et al., 2014; Wu et al., 2024;). For the purpose of this study, clinical signs of infection were assessed through clinical observation, and no microbiological assessment via wound culture was conducted. The healing effects of the Arnebia Euchroma, which are attributed to antioxidants such as alkaloids, help reduce factors that impede tissue repair such as malondialdehyde and carbonyl proteins. Additionally, it assists in reducing inflammation and promoting wound healing (Varaei et al., 2018).
Arnebia Euchroma has been shown to have antifungal, antibacterial, healing, and analgesic effects. For example, Mohammadi et al. (2022) compared clotrimazole vaginal ointment with Arnebia Euchroma ointment in 112 women with candida vulvovaginitis and reported improvements in vaginitis symptoms (discharge, pain, burning) in both groups, with no significant difference between them. However, the candida culture results significantly differed between the two groups. The clotrimazole group showed more negative cultures after the intervention. It seems therefore that Arnebia Euchroma significantly reduces fungal infections (Mohammadi et al., 2022). Arnebia Euchroma ointment has also been found to have effects on parasitic agents such as Leishmania major. A study by Sozangar et al. (2012) examined the in-vitro effects of Arnebia Euchroma and yarrow on Leishmania major. The study showed a significant decrease in the number of parasites during the intervention compared to yarrow (a plant used in herbal medicine for its anti-inflammatory, astringent, and wound-healing properties). This effect was observed across different concentrations of Arnebia Euchroma, indicating its significant impact on reducing parasitic infections (Sozangar et al., 2012). Nasiri et al. (2016) studied the effect of Arnebia Euchroma ointment in 45 patients with second-degree burns. The intervention group received Arnebia Euchroma ointment, whereas the control group was treated with silver sulfadiazine until the wound healed. The analysis of the first 15 days of the intervention showed that wounds treated with Arnebia Euchroma ointment significantly healed earlier than those treated with silver ointment. Patients also experienced less pain and burning when dressing with Arnebia Euchroma ointment. The researchers concluded that Arnebia Euchroma ointment had fewer side effects (Nasiri et al., 2016). Mizani et al. (2021) conducted a study on the impact of Arnebia Euchroma on joints, while Memarbashi (2021) examined the effects of Arnebia Euchroma ointment on pain and burning in patients undergoing haemorrhoidectomy (Memarbashi et al., 2021; Mizani et al., 2021). Both studies reported the analgesic properties of Arnebia Euchroma. Additionally, Soltanian et al. (2010) demonstrated the effectiveness of Arnebia Euchroma ointment in reducing pain in patients with osteoarthritis, which is consistent with the present study (Soltanian et al., 2010).
The analgesic and anti-irritant properties of Arnebia Euchroma ointment are likely attributed to the presence of anti-inflammatory and wound healing compounds in the plant. It is important to note that there is no evidence directly associating these compounds with pain receptors. Instead, the ointment accelerates wound healing, reduces inflammation and improves perfusion, resulting in decreased pain and burning sensation. Consequently, patients need less analgesia (Mizani et al., 2021). The anti-inflammatory properties of Arnebia Euchroma ointment can be attributed to its derivatives, shikonins and flavonoids (Liu et al., 2010; Siavash et al., 2016). Rafiei et al. (2020) reported that oral extracts of Arnebia Euchroma had positive and protective effects on platelet count, coagulation tests, and liver enzyme improvement in Wistar rats (Rafiei et al., 2020). By comparison, the toxic effects of high-dose silver nanoparticles and their long-term usage have become a health challenge and a concern for healthcare workers in recent years (Zhang et al., 2022). In a study by Zhang et al. (2016) on the absorption rate of silver nanoparticles, it was concluded that 30%–99% of silver nanoparticles accumulated in the liver instead of reaching the target organ, potentially leading to increased liver damage (Zhang et al., 2016). In a study conducted by Jia et al. (2020), it was found that silver nanoparticles >15 µg/mg resulted in an increase in the expression of carcinogens, adverse effects on type B lymphocytes and the development of leukaemia (Jia et al., 2020).
Strengths and Limitations
This study had a limited scope as patients were selected from only two hospitals. However randomisation enhanced rigor and power was achieved. Due to financial and time constraints, the duration of the intervention was restricted, and the long-term effects of the Arnebia Euchroma dressings on patients’ wounds were not investigated; nevertheless the two week window gave a good trend indication. Although no signs of infection were observed and the wounds gradually healed over time, microbiological examination through wound culture was not performed in this study so conclusive absence of infection cannot be claimed. However as microbial colonisation can occur without causing harm, visual signs and symptoms—reflecting the host’s inflammatory response—are generally a more reliable indicator of clinically significant infection than microbiology alone.
Conclusion
This study is one of the first to compare Arnebia Euchroma ointment and silver nanoparticles dressings in the treatment of pressure ulcers, focusing on pain reduction and wound healing. The results indicated an anticipated reduction in the mean wound size in the silver nanoparticles group and a promising reduction in the Arnebia Euchroma ointment group. The group using Arnebia Euchroma ointment dressing reported lower levels of pain compared to the silver nanoparticles dressing group. Since the full effects of silver nanoparticles on humans and the environment are still unknown, the use of herbal medicines such as Arnebia Euchroma can be considered as an alternative or even in combination with silver nanoparticles.
Recommendations
This study is one of the initial investigations into the effectiveness of Arnebia Euchroma ointment for pressure ulcer healing. This research suggests that dressing with Arnebia Euchroma ointment yields similar outcomes to dressing with silver nanoparticles. Given the limited knowledge regarding the effects of silver nanoparticles on humans and the environment, along with concerns raised by some researchers regarding its usage and environmental hazards (Ferdous and Nemmar, 2020) it is recommended to use herbal medicines such as Arnebia Euchroma in combination with silver nanoparticles. In this study, Arnebia Euchroma root ointment with a 10% concentration was used in combination with olive oil and beeswax. However, other studies have used different parts of the Arnebia Euchroma or alternative combinations such as goat or cow ghee/butter, with varying concentrations of Arnebia Euchroma extract (Nasiri et al., 2016). Further research is needed to determine the optimal concentration of the Arnebia Euchroma, identify the most suitable plant components and establish compatible substances for combining with Arnebia Euchroma extract.
Key points for policy, practice and/or research
Arnebia Euchroma extract is indicated as effective in the wound healing process for patients with pressure ulcers.
Arnebia Euchroma extract is indicated as effective in relieving pain in patients withpressure ulcers, by comparison to nano-silver dressings
Arnebia Euchroma extract is cheaper and more accessible than other dressings.
Further research for identifying the most effective concentrations of Arnebia Euchroma extract and alternative combinations is recommended.
Footnotes
Acknowledgements
We would like to express our gratitude to all the patients and their families who participated and helped us in this study. We would like to thank all the clinical personnel who contributed to this study.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.