
Abstract
Background:
Research is essential for evidence-based nursing practice. However, in low- and middle-income countries like Nigeria, clinical nurses face multiple barriers to engaging in research, emphasis on research-informed care, and recognition of the need for culturally specific nursing research.
Objective:
This study examined factors influencing clinical nurses’ research involvement in Nigerian practice settings, guided by Bandura’s Social Cognitive Theory.
Methods:
A qualitative Interpretive Phenomenological Analysis (IPA) approach was used. Data were gathered via in-depth semi-structured interviews with 28 clinical nurses at a Nigerian tertiary hospital. Thematic analysis was informed by Social Cognitive Theory.
Results:
Three major themes were identified: (1) lack of cultural recognition and structural barriers, including systemic constraints and weak organisational leadership; (2) profession-related barriers, such as low research confidence, perceived irrelevance to clinical work, and motivation tied to academic demands and (3) practice-related barriers, involving peer influence, a weak nursing research culture, and shift work challenges. These factors impact nurses’ attitudes, motivation, and ability to participate in research.
Conclusion:
Clinical nurses’ research participation is hindered by structural, personal, and organisational barriers. Enhancing institutional support, research training, mentorship, and accommodating work environments can improve engagement. Building research self-efficacy and fostering a culture that rewards research may further sustain involvement.
Keywords
Introduction
Evidence-based practice (EBP) is built on research, and a robust body of literature affirms its indispensable role in guiding high-quality care (Grys, 2022; Lu, 2023). In recent years, the integration of research into clinical nursing practice has garnered increasing attention as a pivotal strategy for enhancing patient care, advancing professional standards and fostering EBP (Hwang et al., 2024). Nurse scientists are recognised as influential contributors to the advancement of practice through their capacity to generate and apply scientific knowledge (Birkhoff et al., 2020). Consequently, clinical nurses are increasingly encouraged to transition from passive consumers of research to active participants in the production of scholarly evidence.
Clinical nurses’ involvement in research is not merely an academic exercise, it plays a critical role in improving patient care, enhancing safety, and advancing the profession. When nurses participate in research or drive the research agenda based on nursing knowledge and observations, they help generate evidence grounded in real-world clinical practice, which informs evidence-based care, leads to better patient outcomes, and drives innovation in care delivery (Brunt and Morris, 2025; Hwang et al., 2024). A strong ‘nursing research culture’ within hospitals has been linked to improved organisational adaptability, stronger nurse performance, and a readiness to implement new practices (Balay-Odao et al., 2024; Jensen et al., 2023). In contrast, when nurses remain uninvolved in research, care may rely on outdated practices reducing the ability to respond to emerging problems or optimise care processes and limiting opportunities for continuous improvement or context-specific innovation (Albin and Perry, 2016; Nursing Education Staff, 2024). Without active nurse-led research, healthcare organisations lose valuable frontline insight that could highlight patient needs, inefficiencies, or risks that might otherwise be overlooked (Nursing Education Staff, 2024).
Nursing research plays a central role in advancing holistic, person-centred care by informing health promotion, patient education through ongoing follow-up, therapeutic relationships, enhanced communication, and collaborative partnerships across the care continuum (Appiah et al., 2025; Li, 2025; Melariri et al., 2022). Nurse-led health promotion research supports a wide range of activities, including preventive health assessments, cancer screening, participation in hospital-based wellness initiatives, and care across survivorship and end-of-life trajectories (Chen et al., 2023; Osei et al., 2025). In addition to shaping clinical practice, nursing inquiry contributes to the development of nursing knowledge, learning and curriculum frameworks that strengthen professional capacity, and practice readiness (Choperena et al., 2025). By centring patients’ lived experiences, cultural contexts and self-management capacities, nursing research enhances relational care processes, fostering respect, empathy, and improved quality of care (Mizumoto et al., 2023). Active engagement of clinical nurses in research generates practice-based evidence that strengthens patient education, supports shared decision-making, and promotes culturally responsive and equitable healthcare, particularly in low- and middle-income settings where locally grounded nursing evidence is critical (Appiah et al., 2023; Sebire et al., 2025).
In Nigeria, the imperative for nurse-led research is heightened by pressing workforce and population health challenges. These include persistent nurse migration, poor working conditions, staffing shortages, high clinical workloads, and limited access to research training and professional development (Ajala et al., 2025; Enebeli et al., 2024; Oyedokun et al., 2025). Concurrently, Nigeria faces a substantial burden of communicable and non-communicable diseases, ongoing maternal and child health challenges, and increasing demands for chronic and palliative care, all of which place nurses at the forefront of patient care delivery (Odunyemi et al., 2023). Despite this central role, nurses’ engagement in research remains limited, resulting in gaps in locally generated nursing evidence needed to inform contextually relevant practice and policy (Akingbade et al., 2023). Strengthening nursing-focused research is therefore critical to addressing national health priorities, improving care quality, and advancing equitable, culturally responsive healthcare across Nigeria (Adesola et al., 2024).
Despite this global movement, nurses in low- and middle-income countries (LMICs) such as Nigeria often encounter formidable challenges in engaging with research. A large-scale study conducted across 27 African countries identified critical barriers to nursing research, including the absence of dedicated research teams (47.7%), unreliable internet access (32.6%), lack of skilled research personnel (31.8%), and insufficient team commitment (23.8%) (Conradie et al., 2018). Unreliable internet access restricts nurses’ ability to access up-to-date research information, participate in online training and collaborate with peers, limiting their engagement in research activities (Ahmad et al., 2018). Insufficient team commitment refers to the lack of shared motivation and active support from colleagues and leadership, which diminishes the encouragement and collaboration necessary for nurses to participate confidently and consistently in research (Meneses-La-Riva et al., 2025). Similarly, findings from a Namibian study revealed institutional barriers such as inadequate theoretical preparation, organisational barriers including high workload and limited resources, and personal constraints such as lack of insight into the relevance of research (Hoebes and Ashipala, 2023). In Nigeria, specific impediments include a challenging clinical environment such as staff shortages, high workloads, insufficient clinical supervision, inadequate research training, minimal opportunities for continuing education, lack of institutional support, and a persistent theory–practice gap (Akingbade et al., 2023; Enebeli et al., 2024).
Within Nigeria’s healthcare landscape marked by a high disease burden and resource constraints the need for clinical nurses to contribute to research is both urgent and strategic (Angell et al., 2022). Understanding the underlying mechanisms that influence their engagement in research activities requires a theoretical framework capable of capturing the interplay between individual cognition, social dynamics and environmental influences. In this regard, Bandura’s Socio-Cognitive Theory (SCT) offers a comprehensive and context-sensitive lens for exploring the factors shaping research participation among clinical nurses.
SCT posits that human behaviour is the result of a dynamic, reciprocal interaction between personal factors, organisational, behavioural patterns, and environmental influences (Bandura and National Institute of Mental Health, 1986). By applying SCT, this study aims to move beyond surface-level structural barriers and instead interrogate the internal cognitive processes and contextual social factors that underpin nurses’ research engagement. Although existing scholarship has predominantly focused on institutional and educational barriers, there remains a critical need to explore how clinical nurses in Nigeria perceive and navigate the complex cognitive, social, and environmental factors that shape their research participation. Thus, this study aims to explore the barriers and facilitators influencing clinical nurses’ involvement in research, using a socio-cognitive lens to examine their lived experiences.
Methodology
Research design
A qualitative research approach, specifically Interpretive Phenomenological Analysis (IPA), was employed to explore the underlying factors influencing clinical nurses’ engagement in research within practice settings. IPA, as described by Smith and Osborn (2015), focused on understanding how individuals make sense of their lived experiences within their personal and professional contexts. This approach was well suited to the study’s aim because nurses’ decisions to engage or not engage in research are shaped by subjective beliefs, interpretations, and contextual influences that cannot be captured through quantitative methods alone. By allowing participants to articulate how they perceive, experience, and assign meaning to research within their clinical environment, IPA provided a nuanced understanding of the cognitive, motivational, and contextual mechanisms influencing their involvement. IPA facilitates this by focusing on participants’ lived experiences and meaning-making through in-depth analysis (Smith and Osborn, 2015). This methodological choice therefore aligns directly with the study’s goal of uncovering deeply rooted barriers and facilitators that shape research behaviour among clinical nurses. Given the recognised gap in theoretical understanding regarding nurses’ participation in research (Boström and Wise, 1994), Bandura and National Institute of Mental Health’s (1986) SCT was adopted as a guiding framework to support the interpretation of findings. This theory which posits that human behaviour results from dynamic interactions between personal, behavioural, and environmental factors provided a useful lens for examining how self-efficacy, organisational support, and past experiences influence nurses’ research behaviour. Although the study employed deductive reasoning in line with IPA methodology, the theoretical framework offered a structured foundation for connecting emerging themes to established concepts.
Study setting
The study was conducted at Delta State University Teaching Hospital (DELSUTH), Oghara, a 180-bed tertiary healthcare facility in southern Nigeria established to provide advanced medical services, specialist referral care, and clinical training for health professionals. DELSUTH hosts a wide range of clinical departments including medical, surgical, obstetrics and gynaecology, paediatrics, accident and emergency, intensive care, dialysis, and orthopaedics, which require a correspondingly diverse nursing workforce (Delta State University Teaching Hospital. n.d.a; Delta State University Teaching Hospital, n.d.b). Although the exact number of nurses and their cadre distribution are not publicly reported, job postings and institutional descriptions indicate that the hospital employs nurses across multiple qualification levels, including diploma-trained nurses, Bachelor of Nursing Science (BNSc) graduates, and specialist or postgraduate-trained nurses, as well as roles ranging from Nursing Officer to Chief Nursing Officer. These roles carry different clinical, supervisory, and professional development responsibilities, which are known to influence research engagement.
Target population and eligibility criteria
This study targeted registered clinical nurses providing direct patient care at DELSUTH in southern Nigeria. The inclusion criteria for nurses who took part in this study were as follows: (1) registered clinical nurses practising in the selected healthcare facility in Nigeria; (2) have at least 1 year of post-qualification clinical experience, to ensure they have had adequate exposure to clinical practice and potential research-related opportunities or barriers; (3) engaged in direct patient care (i.e., not in full-time academic, administrative or policymaking roles), and (4) have at least some awareness or exposure to clinical research, whether through observation, participation, or educational settings. The criteria for exclusion were: (1) student nurses, interns or individuals still undergoing formal nursing training; (2) was enrolled in a full-time academic degree programme (e.g. BSc, MSc or PhD) during the period of the study, as this may introduce bias due to structured exposure to research beyond the clinical setting, and (3) was involved in an ongoing disciplinary or professional restriction that limited their involvement in clinical practice.
Sampling techniques and study participants
Participants were recruited through purposive sampling using a maximum variation approach to capture diverse perspectives across nursing roles, departments, years of experience, gender and educational backgrounds. This ensured the inclusion of nurses with differing roles and exposures relevant to research engagement. Data collection took place between August and September 2023.
Data collection procedure
A semi-structured interview guide was collaboratively developed by all authors following a thorough review of relevant literature to ensure alignment with the study objectives. The authors are experienced nurses, each with over 3 years of clinical experience involving patient engagement, rapport building, history taking, and conducting interviews. Among them, two hold doctoral degrees in nursing research, whereas three others are currently enrolled in doctoral nursing research programmes. All have previously employed similar qualitative methods and research designs, contributing to the refinement and validation of the interview guide.
The interview guide explored factors influencing nurses’ participation in research through a series of major questions and targeted probes. Participants were first asked, ‘What factors influence your participation in nursing research?’ with probes addressing funding or monetary incentives, personal and external motivation, and available support. To understand the broader environment, nurses were asked to describe the research culture or general attitude towards research in their unit or department, with probes focusing on training experiences, the perceived relevance of research, post-research experiences, teaching effectiveness, encountered challenges, cultural support, and flexibility related to shift schedules. Lastly, the guide explored social influences with the question, ‘How have the research attitudes and behaviours of your peers or mentors influenced your engagement with nursing research?’ Probes here included peer support, role modelling, observed challenges, and team involvement. This structured approach ensured a comprehensive understanding of individual, cultural, and organisational factors shaping nursing research engagement.
Prior to the commencement of data collection, the interview guide underwent pilot testing to ensure its relevance, clarity and alignment with the study objectives. The guide was piloted with two clinical nurses who met the inclusion criteria but were not included in the main study. This process allowed the research team to evaluate the content and flow of the questions. Feedback from the pilot participants informed minor revisions, particularly in rephrasing some items to enhance clarity.
Interested nurses were approached individually by E.F. at the selected hospital through word-of-mouth communication and the distribution of study posters. Interviews were scheduled at mutually convenient times and conducted either in a quiet location within the hospital or at participants’ homes, based on their preference. All interviews were conducted privately in nurses’ rooms during break periods or after shifts, with only the researcher and participant present, as per the participants’ preference. To minimise coercion, participants were informed that their involvement was entirely voluntary, they could withdraw or end the interview at any time without consequences, and no incentives for partaking in this study or direct benefits would be provided before giving consent. Of the 37 nurses who initially consented, 5 of them later withdrew due to scheduling conflicts. Interviews continued until data saturation was achieved, that is, the point at which no new themes or relevant information were emerging from subsequent interviews. Data saturation was first observed at the 24th interview, after which four additional interviews were conducted to confirm and validate saturation, bringing the final number of completed interviews to 28. As no new ideas or concepts emerged after the 24th interview and responses remained consistent through the 28th, the researchers contacted the two remaining participants who had agreed to participate to thank them for their willingness and to explain that data collection had concluded. This decision to end data collection was mutually agreed upon by the first four authors. All participants who were interviewed completed the process and remained fully engaged throughout.
Data were collected through these 28 in-depth, face-to-face interviews with clinical nurses from various qualifications, roles and departments, allowing for diverse perspectives across professional roles and practice settings. All interviews were conducted in English by the lead researcher, E.F., between August and September 2023. English was chosen as the interview language since all participating nurses are proficient in it, as it is both the medium of instruction in their training and a common language spoken among nurses. Prior to initiating the interviews, the researcher introduced herself to each participant, clearly outlining her role and explaining the purpose of the study. This introduction was conducted in a warm and respectful manner to build rapport and foster a comfortable environment for open dialogue.
Ethical consideration
The study was conducted in compliance with the ethical principles of the Declaration of Helsinki. Ethical approval for the study was obtained from the relevant institutional ethics review board. All participants received detailed information about the study’s purpose, procedures and their rights, including the right to withdraw at any time without penalty. Written informed consent was obtained prior to participation. Confidentiality and anonymity were ensured by de-identifying all data, and interview recordings and transcripts were securely stored and accessible only to the research team. Ethical approval was obtained from the Health Research Ethics Committee, DELSUTH, Oghara, Delta State, Nigeria (Reference No. HRE/PAN/2023/031/0564). Written and verbal informed consents were obtained from all participants prior to their participation.
Methodological rigour
Trustworthiness was ensured using Guba and Lincoln’s four criteria (Guba and Lincoln, 1994). Credibility was enhanced through 2 months of engagement with participants, pilot testing and refining the interview guide, the use of field notes to capture contextual nuances and verification of data saturation with additional interviews to confirm the stability of emerging findings. Transferability was supported by providing thick descriptions of the study setting, participant characteristics and sampling processes, allowing readers to determine applicability to similar clinical contexts. Dependability was strengthened through systematic and transparent analytic procedures, including detailed documentation of coding decisions, use of ATLAS.ti for data organisation and regular peer debriefing to ensure consistency (Friese, 2012). Confirmability was upheld through reflexive practices such as regular self-reflection journals by the lead researcher to acknowledge and manage potential biases, and ongoing peer debriefing sessions among all the researchers to challenge interpretations. Moreover, confirmability was ensured through maintenance of an audit trail, and clear differentiation between participant accounts and researcher interpretations, ensuring that the findings remained grounded in the data rather than researcher bias.
This qualitative study was reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines (Tong et al., 2007).
Data analysis
Data analysis was conducted following the IPA framework, complemented by a deductive approach using Bandura’s SCT as a guiding lens. The process involved several iterative steps consistent with IPA principles (Smith and Fieldsend, 2021; Willis and Harvey, 2025).
Reading and re-reading: The first three researchers immersed themselves deeply in each interview transcript, repeatedly reading to develop a comprehensive understanding of participants’ lived experiences and perspectives.
Initial noting: After familiarisation, all transcripts were imported into ATLAS.ti software for open coding. During this phase, detailed notes were taken, focusing on descriptive observations, linguistic features, and conceptual reflections to capture preliminary insights and nuanced meanings within the data. Different coloured labels were applied to segments of text, each accompanied by brief annotations summarising key ideas. This visual coding system helped organise and distinguish emerging concepts, facilitating clearer identification and tracking of themes. Multiple team meetings were held during this process to ensure removal of redundancies and refine the coding framework.
Developing emergent themes: Building on the initial notes, related ideas were clustered together to form emergent themes within each case. These themes reflected meaningful patterns grounded in participants’ narratives, providing a rich, case-specific understanding.
Searching for connections across themes: Within each case, emergent themes were examined for relationships and grouped into coherent clusters. Special attention was paid to how these themes connected to the SCT framework and the individual’s narrative context.
Moving to the next case: This process was repeated for each participant’s transcript, maintaining sensitivity to unique individual experiences while remaining open to shared patterns.
Looking for patterns across cases (cross-case analysis): Finally, the researchers conducted a cross-case analysis to identify convergent and divergent themes across all participants, enabling a comprehensive understanding of the data.
During theme generation, SCT’s constructs of environmental conditions, behavioural influences, and personal factors were used as an a priori framework to organise and interpret the data. Environmental conditions captured structural, organisational, and cultural factors; behavioural influences encompassed motivations and social learning and personal factors addressed self-efficacy and beliefs about research. An SCT-based initial codebook facilitated deductive content analysis alongside the inductive IPA process, ensuring both theoretical coherence and rich, grounded insights. Regular team discussions enhanced rigour and credibility through consensus-building. This combined method allowed a nuanced exploration of how contextual environments, individual perceptions, and social behaviours collectively shape clinical nurses’ engagement in research. The analysis yielded three overarching themes, under which seven distinct subthemes were identified illustrated in Table 1.
Themes and subthemes.
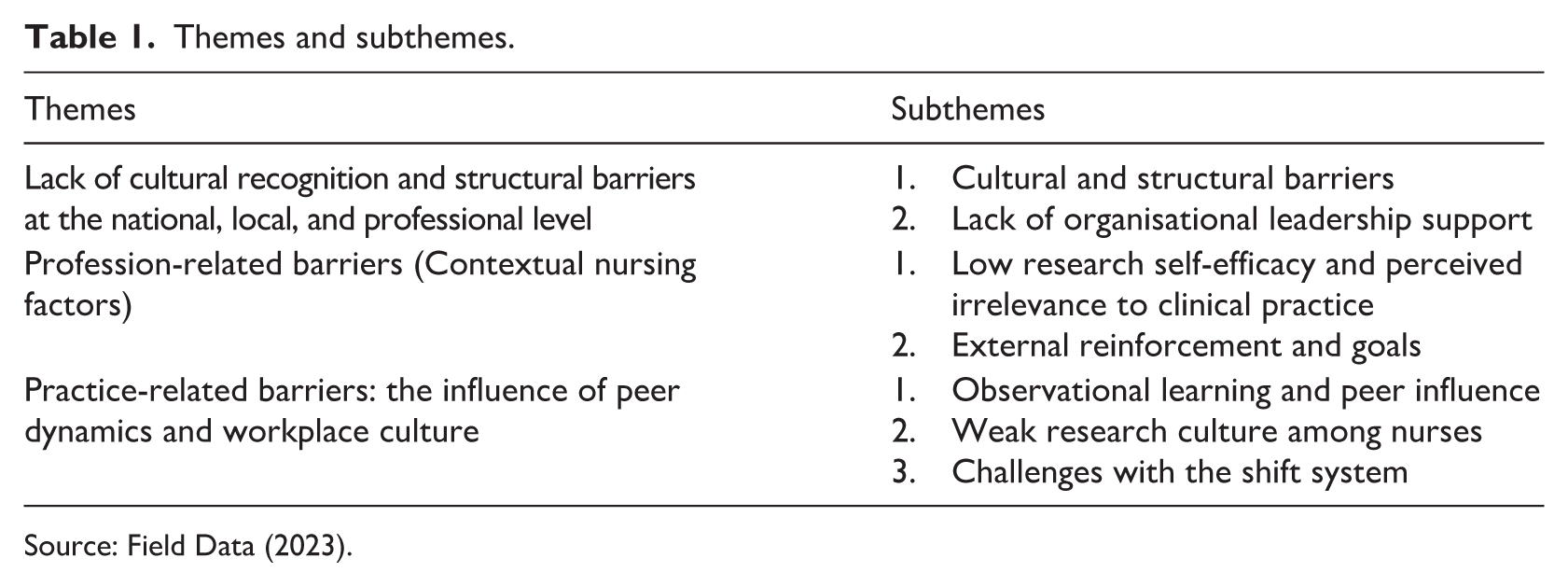
Source: Field Data (2023).
Results
This study involved 20 nurses from a tertiary hospital in Nigeria. Most participants were aged 31 to 40 years (57.1%), and females comprised 60.7% of the sample. The majority held a bachelor’s degree (82.1%) and had received prior research training (89.2%). Further information on professional ranks, salary ranges, years of experience, marital status, and departmental assignments is provided in Table 2.
Sociodemographic characteristics of participants.
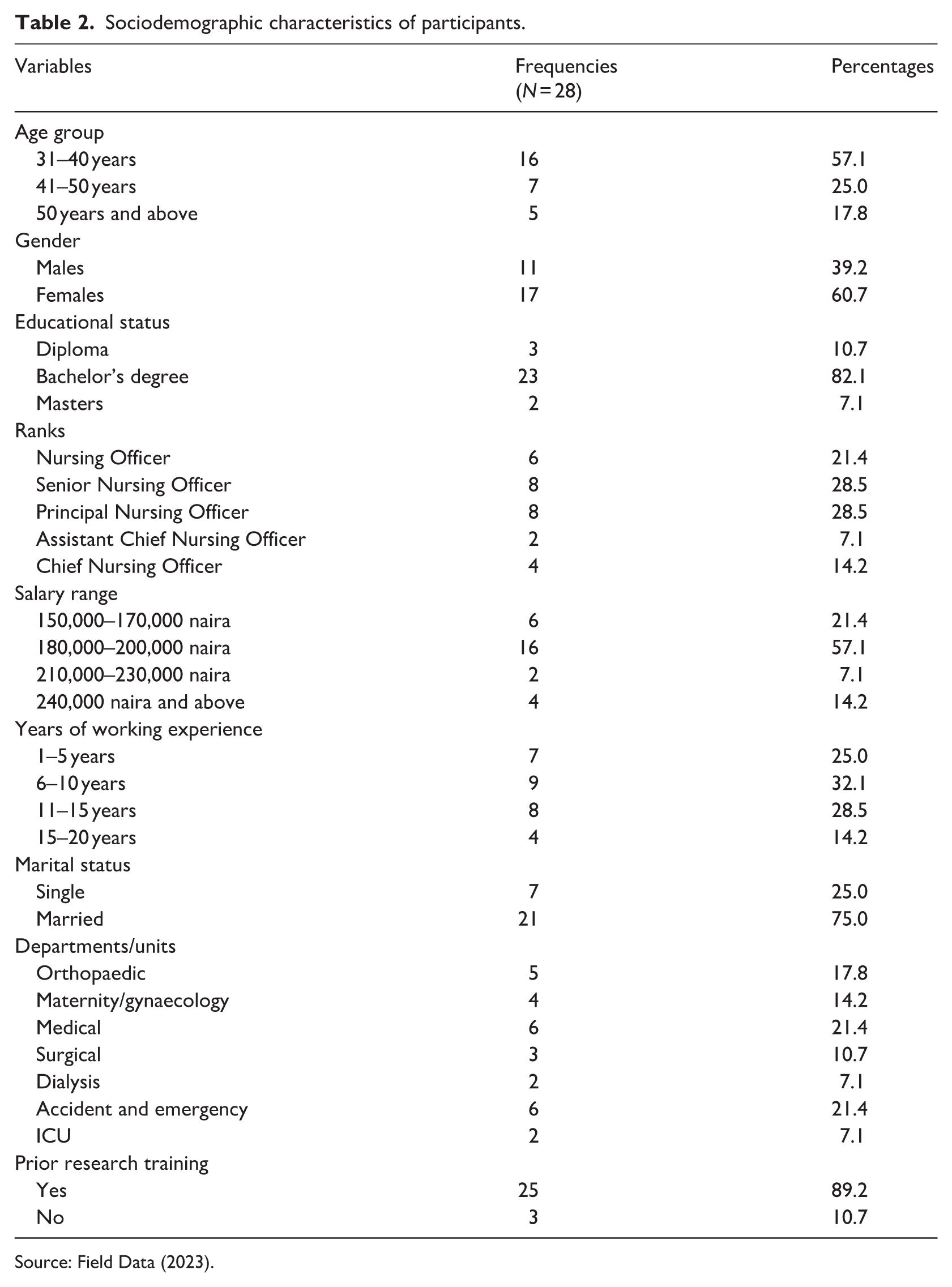
Source: Field Data (2023).
Theme 1: Lack of cultural recognition and structural barriers at the national, local, and professional level (organisational level)
This theme highlights entrenched cultural and structural challenges that limit clinical nurses’ engagement in research across national, local, and professional contexts. The undervaluation of nursing research is reinforced by organisational barriers, including inadequate funding, limited institutional support, and lack of protected time or resources. Within this theme, barriers to nurses’ research involvement include cultural and structural constraints as well as insufficient organisational leadership support.
Subtheme 1: Cultural and structural barriers
Participants’ narratives revealed how the longstanding prioritisation of medically driven research contributes to structural disinvestment in nursing-specific research. This cultural marginalisation translates into limited funding opportunities for nurses and reinforces inequities in resource allocation. Coupled with low remuneration, these structural constraints make self-funding research unrealistic, even for nurses who are highly motivated to engage in research.
There is no financial sponsoring that can encourage nurses to participate in research. In my case, for example, I am a nursing officer receiving close to 150,000 naira ($100) monthly, and this money is not sufficient to even care for my family as a single mum with two kids. So even though I am very much interested in carrying out research, I can’t do so because my hospital does not fund research and I also do not have money. Like I previously stated, research is money-intensive and there is no one interested in funding nursing research in Nigeria as far as I know. Unlike the medical doctors that get a lot of funding, we as nurses do not have the same opportunity so you don’t expect me to spend the little I have to fend for myself on research.
Some participants highlighted that overcoming cultural barriers requires a shift in attitudes and greater recognition of the value of nursing-specific research for improving patient outcomes. They emphasised that this change must be supported by policy-level interventions, with government leadership playing a crucial role in providing the necessary funding and structural support. As one participant noted: Nurses play a vital role in the health care system; we are the backbone. So, I believe those in authority should take responsibility by funding nursing research. Without that kind of support, it becomes hard for us to participate, no matter how interested or capable we are.
Subtheme 2: Lack of organisational leadership support
Participants reported that limited leadership support and lack of organisational prioritisation of research discouraged nurses’ involvement. The absence of encouragement, mentorship and lack of leadership support contributed to a weak research culture, reinforcing perceptions that research falls outside nurses’ professional roles and sustaining low participation as narrated by the participants below.
There’s no real encouragement from leadership when it comes to research. It’s not prioritised, so we just focus on our routine tasks. Over time, that lack of support makes everyone think research isn’t even part of our role. When the environment doesn’t promote research, people stop seeing the point. Then nobody talks about it, nobody mentors, and it just becomes a cycle, no support, no participation and no growth. Because research is neither encouraged nor emphasised among nurses, we tend to be hesitant when asked to participate in studies, we give all kind of excuses just to refuse participation.
Theme 2: Profession-related barriers (contextual nursing factors)
Building on the structural and organisational barriers, this theme focuses on profession-related and contextual nursing factors that shape nurses’ engagement with research. Participants’ narratives suggest that the marginalisation of nursing research within healthcare organisations is reinforced during professional training. Research is often framed as a project-based academic requirement rather than a core component of nursing practice, a perception that is further reinforced by what nurses observe in clinical settings where research is rarely modelled, encouraged, or integrated into routine care.
Subtheme 1: Low research self-efficacy and perceived irrelevance to clinical practice
This subtheme builds on the organisational culture and leadership gaps identify to present how these systemic influences shape nurses’ professional self-perceptions and beliefs about research. Nurses in this study therefore internalised the message that research is primarily an academic endeavour rather than an integral part of clinical nursing. This theme is a narrative of the nurses’ low confidence in their research abilities and scepticism about its practical value, ultimately diminishing their motivation to engage in research activities within clinical settings.
I’ve never really seen myself as someone who can do research. It feels like something meant for academics, not for someone like me working on the ward. To be honest, I don’t feel confident enough. Even during school, I struggled with understanding the basics, so I’ve always felt research is beyond my ability.
Additionally, some seasoned and older nurses remain sceptical about the practical value of research, perceiving it as less relevant to their current clinical duties and often leaving the responsibility for EBP to younger staff.
I’m not even sure what the benefit is. We’re already overworked, and I don’t see how research will help me care for patients better in this setting. Moreover, at this my age, I cannot be interested in research because I will soon be retiring from the nursing profession; so let the youngsters make the difference with research.
Many nurses described feeling disconnected from research, perceiving their daily work as driven by routine and past training rather than current evidence.
We don’t really see the impact of research in our daily work. Most of the time, what we do is based on routine and what we were taught years ago. So, it’s hard to understand why we should spend our little free time doing research when nothing changes in the hospital. (
Subtheme 2: External reinforcement and goals
As per the findings of this study, nurses’ engagement in research is often externally driven, motivated more by academic requirements than by personal or professional interest. Participants verbalised that research was viewed as a means to fulfil degree obligations which suggested that environmental demands such as mandatory research projects in training may trigger short-term participation without fostering long-term commitment or intrinsic motivation to sustained research engagement in practice.
Research done in the undergraduate programmes are done out of necessity which is to obtain degree in nursing not to meet or address a particular need. Hence, after two years of graduating some do not even remember their topic. We weren’t really taught to value research beyond school. It felt more like a hurdle to cross than something to continue doing in practice.
Many participants recalled that research during their training was often viewed as a mandatory task with limited emphasis on its practical application, direction, or support for wider dissemination beyond academic requirements.
In school, research was more of a formality like one more assignment we had to submit to finish our degree; you know our research work is usually only printed and kept in school and are not disseminated for others to access and utilise it.
Participants attributed many of their research challenges to inadequate teaching during their training, highlighting a lack of skilled instruction, poor integration of research into the curriculum, and limited guidance on applying or disseminating research findings.
The lecturer who taught us research in school didn’t seem to understand it himself. He often contradicted himself during lessons, which made research feel ambiguous and unnecessarily difficult. I managed to get through it for the sake of my degree, but honestly, I don’t feel confident or equipped to do research now, even though I know it’s something nurses are supposed to be good at.
Theme 3: Practice-related barriers: the influence of peer dynamics and workplace culture
This theme builds on the profession-related barriers rooted in education and professional socialisation to explore how the clinical practice environment and peer dynamics further shape nurses’ engagement with research. Nurses’ attitudes and behaviours around research are heavily influenced by the norms they observe among colleagues and the prevailing research culture or lack thereof in their workplaces.
Subtheme 1: Observational learning and peer influence
Nurses’ engagement in research is often influenced by the behaviours they observe in peers and mentors. Positive role models can boost confidence and motivation, while seeing others struggle or avoid research may create doubt and discourage participation. This peer effect plays a critical role in shaping nurses’ attitudes and willingness to engage in research activities.
During my undergraduate research, I struggled because the nurses around me people I considered friends wouldn’t even help me by filling out my questionnaires. They gave excuses or avoided me entirely. That experience made research feel isolating and discouraging. It left me with a negative impression that has stuck with me ever since.
Another participant expressed scepticism rooted in observing how research is often treated in practice: I think research is a waste of time because even when it’s done, it’s never implemented. Seeing how others dismiss it or ignore its outcomes makes me feel there’s no real point in engaging in it.
Subtheme 2: Weak research culture among nurses
Weak research culture among nurses was another factor that was mentioned by many of the participants to serve as a barrier to clinical nurses’ involvement. It was mentioned that research was not an activity that was inculcated amongst nurses but was always done for the purpose of attaining some form of benefit such as promotion for nurses in academia and award of nursing degree for nursing students.
Here in Nigeria, I would like to say that that research culture is not among nurses at all; unlike in other countries where you see nurses leading big studies, here you don’t see such. So is like there are no research predecessors to inculcate the act within nurses. I always witnessed seminars on nursing practice but not research. Research as part of nursing practice is not common in most facilities that I know of and in this facility, I have never seen nurses come together to conduct research. Most of the research in Nigeria are done by Nursing lecturers and or students.
Others noted that nurses within academic sector conducted research because it was a necessity for professional development not necessarily because it was a culture: Even nurses in academia, most of them conduct researches so that they can rise to the professor level and not because it is a part and parcel of them.
Subtheme 3: Challenges with the shift system
Several participants expressed that the nature of their clinical schedules left little to no flexibility for additional professional pursuits. The intensity and rigidity of the shift system were perceived as discouraging, ultimately reducing the likelihood of research involvement despite personal interest or perceived capability.
We work a three-shift system, but it’s poorly structured you might do a morning shift today, then afternoon tomorrow, and morning again before finally getting a day off. With that kind of schedule, you’re too exhausted to even think clearly, let alone carry out research. The shift schedule is so scattered that it’s difficult to have any form of planned life simply because you’re a nurse; so, conducting research becomes even more unrealistic.
Discussions
This study reveals that entrenched cultural and structural barriers profoundly limit clinical nurses’ involvement in research within Nigerian healthcare settings. The longstanding prioritisation of medically driven research marginalises nursing-specific inquiry, resulting in scarce funding, inadequate institutional support, and lack of protected time or resources for nurses. Despite strong personal motivation, many nurses face insurmountable financial obstacles due to low salaries and the unrealistic expectation of self-funding research, effectively excluding them from contributing to knowledge generation. Due to this, the participants emphasised the critical need for government and leadership intervention to provide dedicated funding and foster an enabling environment that values nursing research. These findings mirror those of Kyei et al. (2023) and Koirala et al. (2024), highlighting common systemic challenges in LMICs particularly sub-Saharan Africa where nurses face high workloads, low pay and limited professional development. Such conditions not only hinder self-funding but also perpetuate a culture where research is undervalued or viewed as inaccessible. Addressing these barriers calls for urgent institutional and governmental investment in nursing research through accessible funding and better compensation to strengthen EBP and improve patient care outcomes.
Similarly, lack of visible support and advocacy from organisational leadership significantly undermines nurses’ engagement in research activities. When leaders fail to prioritise research or provide mentorship, it signals to nursing staff that research is not a valued or expected component of their professional responsibilities. This absence of institutional backing contributes to a culture where research is marginalised, resulting in low motivation among nurses to participate in studies or pursue scholarly inquiry. Such an environment fosters disengagement and perpetuates a cycle where research remains peripheral to everyday nursing practice. These findings highlight the crucial role of leadership in cultivating a research-positive culture, as strong leadership involvement is key to integrating research into practice and advancing professional growth (Horning and Taylor-Pearson, 2024; Hung et al., 2023). Moreover, engaging in nursing research can enhance evidence-based leadership, which in turn improves nurse performance, organisational effectiveness, and patient outcomes (Välimäki et al., 2024).
Findings revealed profession-related barriers rooted in nursing education and clinical practice that limit nurses’ research engagement. Research is often seen as an academic task rather than a core nursing function, a perception formed early in training and reinforced by clinical environments where research is rarely modelled or encouraged. This disconnect fosters low research self-efficacy and doubts about its relevance to daily care. Experienced nurses often view research as peripheral, deferring EBP responsibilities to younger staff, highlighting a generational divide. Routine clinical work and the lack of visible research impact further discourage scholarly involvement. These results underscore the need to better integrate research into nursing education and practice to build confidence and demonstrate its practical benefits (Leiviska et al., 2025). Addressing these barriers is vital to developing a nursing workforce that values and actively engages in evidence-based care, improving outcomes and advancing the profession (Mohamed et al., 2024). Additionally, organisational support and interprofessional collaboration are essential to fostering this change (Olanrewaju et al., 2021).
The study further revealed that nurses’ research engagement is often driven by academic requirements rather than intrinsic motivation, leading to short-term involvement without sustained practice. Early training frames research as a mandatory task with little focus on practical use or dissemination, reducing its perceived relevance. Inadequate teaching, lack of mentorship, and poor curriculum integration undermine nurses’ confidence and interest in research. These barriers call for educational reforms that embed research as a core nursing competency, supported by skilled instruction and application guidance. Strengthening these areas can boost research self-efficacy, encourage ongoing engagement and enhance EBP (Al-Omari et al., 2024). Prior studies also note that personal interest and time constraints affect nurses’ research participation (Alotaibi, 2023; Balay-Odao et al., 2024). This study suggest the importance of teaching research as meaningful and practice-oriented rather than merely a graduation requirement and calls for a coordinated approach that aligns university training with clinical roles to support ongoing research engagement in practice.
The current study highlights the significant impact of peer modelling on nurses’ engagement in research. It revealed that nurses observed a lack of research interest and skills among colleagues, which negatively affected their own motivation. Concerns about being unable to recruit fellow nurses for research and seeing little implementation of research findings further diminished their interest and participation. This peer effect emphasises the importance of cultivating a supportive research culture where active participation is visible and encouraged (Sebire et al., 2025). The findings suggest that nursing stakeholders must foster environments where positive research experiences are the norm, helping to dismantle psychological barriers and strengthen the research culture among clinical nurses. Supporting this, Dagne and Tebeje (2021) found that negative experiences, especially a lack of institutional support, led nurses and midwives to intentionally avoid applying research in practice. Therefore, advancing nursing practice and reinforcing the profession’s evidence base requires strategies that enhance research exposure through supportive, mentor-guided experiences in clinical settings.
The study found that shift systems were a significant barrier to nurses’ research involvement. Participants noted that unpredictable and irregular shift schedules left them with little time for research activities, disrupting their ability to establish consistent routines and hindering professional development. This aligns with Ejebu et al. (2021), which, while not focused on research, highlighted how poorly structured shifts negatively affect nurses’ health, job performance and patient care. These findings underscore how shift systems can undermine not only clinical performance but also nurses’ ability to engage in research, a crucial aspect of professional growth. Therefore, it is essential for nurse managers and healthcare administrators to re-evaluate and adjust shift systems to allow nurses time and stability to pursue research.
Implications for practice, research, policy, and education
Based on the findings, the following implications are recommended:
Health and social care policy must provide dedicated research funding, resources, and supportive frameworks to enable evidence-informed nursing practice.
Nursing education and professional development should embed practical, confidence-building research skills and emphasise how research drives safer, higher-quality care.
Health systems and nurse managers should foster mentorship networks, create peer-led research opportunities, and celebrate clinical research achievements.
Workforce policy and nurse management should allow flexible scheduling and protected research time to integrate inquiry into daily practice.
Future research should test mentorship models, funding schemes, and shift redesign to build a sustainable research culture in LMICs and inform equitable health and social care policies.
Strengths and limitations
A major strength of this study lies in its use of IPA, which provided deep insights into the lived experiences and perceptions of clinical nurses, capturing the nuanced interplay of personal, environmental and behavioural influences. The application of Bandura’s SCT added theoretical rigour and guided the interpretation of complex themes. However, the study is limited by its focus on a single tertiary hospital; hence, findings may not be applicable to other regions or healthcare settings in Nigeria.
Conclusion
This study revealed that clinical nurses in Nigeria face interconnected socio-economic, personal, and organisational barriers that limit their engagement in research. Financial constraints and lack of institutional support, coupled with low research self-efficacy, limited confidence and unclear perceptions of research relevance, reduce nurses’ motivation to participate. Additionally, a weak research culture, absence of role models, and demanding shift schedules further hinder their involvement. Interpreted through Bandura’s SCT, these findings demonstrate how environmental conditions, personal beliefs, and behavioural patterns interact to reinforce low research participation. Addressing these barriers through improved institutional support, confidence-building opportunities and a more enabling research culture is essential for strengthening research engagement among clinical nurses in low-resource settings.
Key points for policy, practice, and/or research
Clinical nurses’ engagement in research in Nigeria is constrained by interconnected structural, professional and practice-level barriers, including limited funding, weak leadership support, low research self-efficacy and unsupportive workplace cultures.These barriers interact to shape nurses’ motivation, confidence and capacity to participate in research beyond mandatory academic requirements.Addressing these challenges requires coordinated action across policy, education and clinical practice to normalise research as a core nursing role.Creating protected time, mentorship opportunities and visible leadership commitment to nursing research is critical to sustaining engagement and strengthening evidence-based care especially in low-resource settings.
Footnotes
Acknowledgements
The authors sincerely thank the nurses who participated in this study and the researchers whose work provided foundational support for this manuscript.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
All data supporting the findings of this study are included within the manuscript.
Ethics approval
Ethical approval was obtained from the Health Research Ethics Committee, DELSUTH, Oghara, Delta State, Nigeria (Reference No. HRE/PAN/2023/031/0564). Written and verbal informed consents were obtained from all participants prior to their participation.