
Abstract
Background:
Nursing work involves significant emotional, cognitive, and physical demands, making peer support an essential resource for sustaining well-being and resilience. Peer support among nurses is a collaborative process where nurses provide assistance to each other. Although formal peer support programmes are available in some organisations, the informal, everyday support that underpins clinical practice remains less understood.
Aims:
This study explored clinical nurses’ experiences of informal peer support in an acute hospital in Singapore.
Methods:
Twelve registered nurses were recruited through convenience sampling, and semi-structured interviews were conducted between June and December 2024. Interviews were audio-recorded, transcribed verbatim, and analysed thematically using Braun and Clarke’s six-phase approach.
Results:
Four themes were identified: (1) peer support requires effort and intentionality, (2) boundaries shape how support is negotiated, (3) leadership shapes the culture of support, and (4) peer support promotes resilience and retention. Informal support was experienced as psychologically complex yet critical for resilience, job satisfaction, and sustainability of practice.
Conclusions:
These results highlight the need for healthcare organisations to foster psychological safety and strengthen informal support mechanisms to protect nurses’ well-being and promote retention.
Keywords
Introduction
In hospitals, nurses often have to provide immediate and complex nursing care to patients with severe injuries, illness, or urgent medical conditions. They are routinely exposed to a wide range of occupational stressors that can compromise professional performance and personal well-being (Tamata and Mohammadnezhad, 2023). High patient acuity, chronic disease complexity, inadequate staffing, poor skill mix, time pressures, limited resources, and frequent exposure to workplace violence place sustained emotional and operational demands on the workforce (Figueroa et al., 2019). These conditions contribute to stress and burnout, with well-documented consequences for nurses’ mental health, job satisfaction, and quality of care (Khamisa et al., 2015). Stress and burnout have also been consistently linked to nurses’ intention to leave both their organisations and the profession, thereby exacerbating workforce shortages (Hämmig, 2018). The COVID-19 pandemic amplified these long-standing issues, with evidence indicating unprecedented workloads, high psychological strain, and attrition reported during the pandemic. Synthesised findings suggest that approximately 48% of nurses experienced burnout during the pandemic, with burnout associated with a four-fold increase in turnover intention (Liang et al., 2025). Post-COVID-19, these intensified demands and residual workforce pressures continue to shape nurses’ working conditions and worsen attrition (International Council of Nurses, 2002). In the context of a global nursing shortage and escalating psychological strain, mitigating these risks is essential to workforce retention and the delivery of safe, effective care.
Social support is widely recognised as a protective workplace resource that buffers the psychological effects of job stress, enhances well-being and promotes sustained engagement in the profession (Jolly et al., 2021). It encompasses the emotional, informational and practical assistance received from interpersonal relationships, including supervisors, family or other professionals (Donovan and Greenwell, 2021).
Under the broad framework of social support, peer support has emerged as an important resource in clinical nursing for nurses’ mental well-being and job satisfaction (Barry et al., 2025). Peer support among nurses involves the exchange of emotional, practical, and informational support between colleagues who have similar work experiences (Raqueno et al., 2025). This form of support fosters psychological safety for clinical decision-making, promotes collaborative communication, and strengthens interpersonal relationships grounded in shared goals (Kristoffersen, 2021). Supportive workplace relationships enhance resilience, strengthen belonging, and promote professional development (Noguchi-Watanabe et al., 2016).
Background
Research distinguishes between informal peer support, which arises spontaneously through everyday workplace interactions, and formal peer support such as structured mentoring programmes and support groups (Watson et al., 2025). Informal peer support is often more accessible than formal support, but its availability is shaped by contextual barriers such as organisational hierarchy, time pressures, cultural norms, and competition (Hofmann et al., 2009; Wall et al., 2022). Inadequate peer support has been linked to missed nursing care, interpersonal conflict, and burnout (Anusiewicz et al., 2020; Göktepe et al., 2020). Conversely, strong peer relationships mitigate distress following adverse events, facilitate emotional recovery, promote a sense of belonging, and sustain long-term work engagement, which are all protective factors against mental health decline (Singh et al., 2020).
Most studies conceptualise support broadly, or focus on formal support interventions, with little attention to the informal, everyday peer support that occurs in the context of the ward environment (Cohen et al., 2023). Understanding how informal peer support functions in high-pressure clinical settings is important because it protects nurses’ mental health and wellbeing by mitigating burnout, moral distress, and compassion fatigue, which are critical to workforce sustainability, retention, and safe practice. Examining informal peer support practices also reveals informal coping mechanisms that are already embedded in ward culture, which are often unrecognised and unsupported at the organisational level. This understanding can guide the development of context-appropriate strategies grounded in frontline realities that are practical and sustainable. In summary, understanding informal peer support allows organisations to strengthen nurses’ resilience in areas that formal support systems do not adequately address.
As the specific practices, psychological processes, and leadership dynamics that sustain informal peer support is underexplored, this study sought to uncover how nurses negotiate psychological demands, boundaries, and support structures in their everyday work. Understanding these dynamics is crucial to promote peer support. This gap highlights the need for qualitative inquiry into how nurses negotiate these interactions and how informal peer support contributes to resilience, retention, and quality of care. This study therefore explores how registered nurses experience informal peer support in their everyday practice, and how such interactions shape professional functioning, resilience, and retention.
Methodology
A qualitative descriptive design (Sandelowski, 2000) was employed to obtain a comprehensive account of how nurses at Woodlands Hospital, an acute hospital in the metropolitan city-state of Singapore, understood and experienced peer support. This design was appropriate for a phenomenon that is contextually specific and insufficiently described in existing literature. It enables low-inference representation of participants’ perspectives in language close to their own, producing findings that are readily applicable to practice. The aim was to describe the forms and meanings of peer support as they occur within a newly established organisation. The qualitative descriptive approach therefore provided the methodological fit needed to produce credible, contextually grounded insights for workforce development. The study was reported according to the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Tong et al., 2007). Participants were registered nurses employed full-time in general medical wards at an acute hospital in Singapore. Eligible nurses had at least 6 months of independent clinical practice and direct patient care responsibilities; those in non-clinical or administrative roles were excluded.
Twelve participants were recruited by convenience sampling across general medical wards between June and December 2024 through ward roll calls and institutional email circulars. Informed consent was obtained after emphasising the study’s purpose, voluntary nature of participation, confidentiality, and the use of audio-recording. One-to-one in-person interviews were then conducted by the principal investigator or the co-investigator in private hospital rooms. Interviews lasted between 45 and 75 minutes. The interviews were conducted in English as English is the common and official language in Singapore and is spoken by all nurses who are licensed to practise in the country. The researchers employed probing techniques to elicit elaboration and clarification to ensure that participants’ perspectives were accurately represented.
The semi-structured interview guide was developed by the principal investigator and co-investigator and refined by the supervising researcher who was then pursuing a Doctor of Philosophy in Nursing. The principal investigator and co-investigator, both female inpatient ward nurses who graduated with Bachelor of Nursing with Honours, pilot tested the interview guide with the supervising researcher. No changes were made to the guide following the pilot test. Both the principal investigator and co-investigator had completed interview training with the supervising researcher.
The interview guide was designed to elicit reflections on the meaning, practice, barriers and motivations surrounding peer support. Questions were:
What does peer support mean to you?
What does an ideal peer support culture look like in your workplace?
Can you describe your experience with peer support on a typical workday?
How do you personally practise or offer peer support at work?
If you have not experienced support, why do you think that is so?
Interviews were transcribed verbatim and returned to participants for verification. Data were analysed using Braun and Clarke’s (2006) six-phase reflexive thematic analysis to allow an understanding of experiences and identification of shared meaning among different participants. Data were managed within Microsoft Excel. The principal investigator and co-investigator independently coded the transcripts and refined them into themes. Themes were then reviewed collaboratively with the supervising researcher. Data collection and inductive thematic analysis occurred concurrently, allowing the researchers to regularly review coded data and discuss emerging themes. Data saturation was considered achieved by the tenth interview during iterative analysis meetings with the two researchers and supervisor, as only repetitive codes and themes were identified, with no new codes emerging (Saunders et al., 2018). Two additional interviews were then conducted to confirm saturation.
The trustworthiness of the study was guided by the criteria established by Lincoln and Guba (1985). Credibility was ensured by reinforcing that participation was entirely voluntary and could be withdrawn anytime. Measures were also implemented to mitigate potential undue influence from any existing relationship between the researchers and the participants. This includes having the interviews conducted, where possible, by a researcher with no prior relationship with the participant and reinforcing confidentiality. Transcripts were returned to participants for comment or correction. Triangulation was achieved by recruiting participants from different wards, and through independent data analysis by two researchers from different wards, followed by discussion with the supervising researcher. Transferability was addressed by providing detailed information of the research process. Dependability and confirmability were maintained through adherence to the COREQ checklist, a code–recode process with at least 2 weeks between coding sessions, regular discussions to challenge assumptions, and reflexive notes.
This study was approved by the institution’s ethical board on 14 February 2024. All participants received a Study Information Sheet detailing the study’s purpose with an emphasis on the voluntary and confidential nature of their participation. All participants gave written consent before starting interviews. All participants were assigned a number and data securely stored to ensure anonymity.
Results
The findings revealed that informal peer support plays a central role in shaping nurses’ professional experiences in hospital wards. Four key themes were identified from the analysis: 1. Peer support requires effort and intentionality; 2. Boundaries shape how support is negotiated; 3. Leadership shapes the culture of support and, 4. Peer support promotes resilience and retention. As illustrated in the conceptual diagram (Figure 1), peer support is depicted as an active and effortful process, represented by one hand supporting and lifting another hand. This symbolises the link between the intentional and effortful act of peer support and its outcomes in resilience and retention. These two hands are encircled to reflect the broader contextual influences of boundaries and leadership, which shape how peer support is enacted within the ward.

Conceptual diagram.
Characteristics of participants
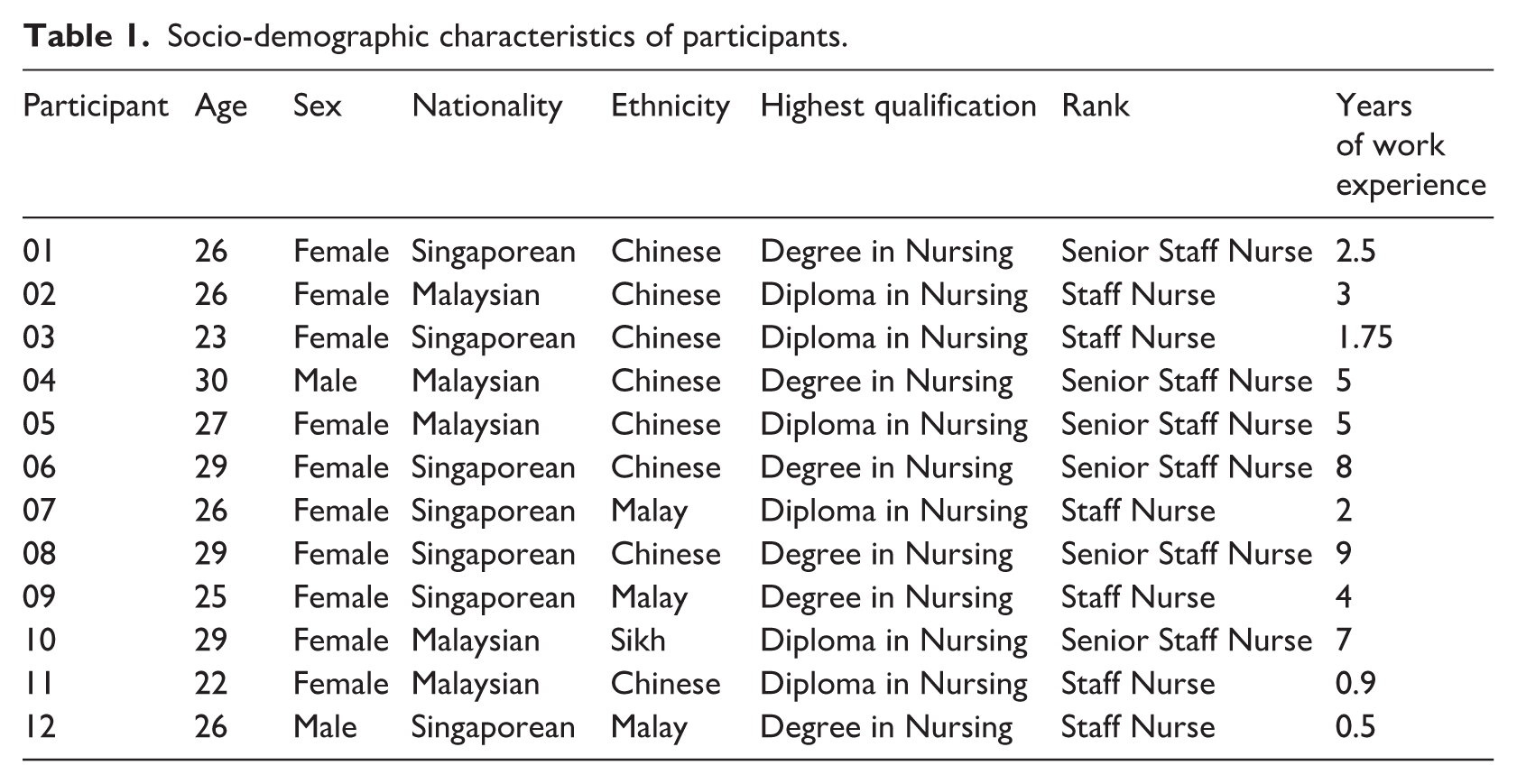
The socio-demographic characteristics of participants are delineated in Table 1. Participants had a mean age of 26.5 years. Nursing experience ranged from 0.5 to 9 years, with a median of 3.5 years. Participants were staff nurses or senior staff nurses with diploma or degree qualifications in nursing.
Socio-demographic characteristics of participants.
Theme 1: Peer support requires effort and intentionality
This theme captures how peer support was experienced by nurses as an intentional act that required emotional and cognitive labour. Participants consistently described the need to regulate their own emotions, manage interpersonal risks, anticipate others’ needs, and weigh competing priorities.
Although most participants valued the reassurance and safety net provided by supportive peers, they often hesitated to seek help because of fears of judgement or negative repercussions: ‘When you ask a question, you don’t want to feel judged or inferior’ (P11). They have to overcome their reluctance to seek support by prioritising their professional responsibility to uphold patient safety: ‘But I will ask when it concerns patient safety, although I will have to mentally prepare myself for any backlash’ (P01). Supporting others could also be burdensome when layered onto personal responsibilities, with one nurse noting, ‘It gets overwhelming . . . it becomes a burden’ (P10). Nurses have to put aside their frustrations and judgements about their peers’ competence to maintain teamwork: ‘I know I shouldn’t judge them . . . but I still help, just not fully’ (P03). At the same time, participants recognised the importance of actively interpreting situational cues, inferring needs that are not verbally expressed by their peers and offering assistance proactively: ‘They said “nothing”, but I realised they needed equipment’ (P02). However, nurses emphasised the cognitive effort needed to strategically prioritise their own responsibilities before helping others and managing the competing demands for time and attention: ‘I have to make sure I’m settled before helping, otherwise I may give the wrong advice’ (P03). These accounts highlight the complexities of seeking and providing support, illustrating that peer support is an intentional and effortful practice rather than an automatic exchange.
Theme 2: Boundaries shape how support is negotiated
This theme highlights how peer support was not freely or uniformly exchanged, but instead negotiated within relational boundaries shaped by trust, hierarchy, ward culture, and expectations of reciprocity. Rather than being automatically available, support was influenced by interpersonal relationships and implicit norms that shaped why and who nurses sought or offered help to.
Nurses reported seeking help first from close colleagues and then competent colleagues, instead of escalating indiscriminately: ‘My closest colleagues are the first people I ask, the more knowledgeable ones are the next’ (P12). Hierarchical dynamics sometimes prevented open communication, as seniors felt offended when corrected by juniors: ‘The seniors feel stepped upon when I correct them’ (P04). Senior nurses also reported feeling overlooked when they were not offered help by the others: ‘At the end of the day, seniors are still human. . . sometimes we do have our down days’ (P10). Participants also reflected on a prevailing culture of self-reliance and independence, which could be either developmental or harmful: ‘When you are young, you should be supported to learn and not thrown into a sea of sharks’ (P08) and ‘They should do it themselves . . . otherwise, there’s no way for them to manage their own job’ (P10). Reciprocity was described as both motivating and limiting: ‘Show them what you can help with and they will help you the next time’ (P12) and ‘It’s a transaction. . . what can you offer in their eyes?’ (P07).
These findings reveal how relational boundaries can both enable and constrain the exchange of peer support. Understanding these constraints provides important context for how peer support requires intentional effort and underscores the importance of leadership in shaping how these boundaries are navigated.
Theme 3: Leadership shapes the culture of support
This theme illustrates how leadership practices influenced whether peer support was encouraged, normalised, and sustained within the ward. Participants described leaders as shaping the conditions under which peer support could occur through authority, role modelling, and visible engagement with front-line work.
Managers were viewed as responsible for resolving tensions among nurses and setting expectations of professional conduct: ‘They’re the ones with oversight of the ward’ (P01). Even small symbolic acts, such as assisting briefly on the ward, were meaningful because they reduced hierarchical distance and conveyed leaders’ investment in staff wellbeing: ‘Just showing your face. . . makes us feel appreciated’ (P06). By modelling supportive behaviours, leaders were perceived to soften hierarchical barriers that might otherwise inhibit peer support and legitimise collaboration into everyday practice: ‘If someone in a superior position is doing that, people would just do the same’ (P08).
These findings reveal how leadership shapes the cultural context in which peer support is enacted by influencing ward norms and how hierarchical boundaries are navigated. When leaders actively normalised peer support, nurses described feeling more able to sustain supportive practices over time, which then promote outcomes of resilience and retention as described in the following theme.
Theme 4: Peer support promotes resilience and retention
This theme captures the outcomes of sustained peer support on nurses’ professional well-being, with participants describing its role in fostering work engagement, motivation, resilience, and retention.
When emotionally supported by peers, nurses reported greater confidence to take on responsibilities and support others: ‘I was very expressive with my ideas as compared to the times I had no confidence when colleagues were so critical with me. I was motivated to work and help others’. (P01). Supportive environments fostered camaraderie and made demanding shifts more manageable: ‘Even if you finish late, you don’t mind, because you have a good team’ (P03). Strong peer relationships anchored nurses to their workplaces: ‘A lot of people will stay because of their colleagues . . . you’ll be happier at work’ (P05). In contrast, unsupportive environments, often characterised by incivility among peers, had an opposite effect: ‘That person did not help me and was backbiting me. I feel sad and did not want to work’ (P09).
These findings suggest that motivation and resilience are not simply individual attributes, but emerge from the intentional and sustained practice of peer support within ward environments. When peer support is limited, its protective effects on nurses were diminished. Conversely, when peer support is actively practised, it not only enhances resilience and retention, but also generates a positive feedback loop, in which experiencing support motivate nurses to support others, thereby sustaining collaborative ward cultures over time.
Discussion
The findings of this study highlight the central role of informal peer support in shaping nurses’ professional experiences. Four themes captured how nurses engaged with and made sense of peer support in their everyday practice by collectively illustrating how informal peer support operates as both a protective resource and a source of strain, depending on the ward environment in which it is enacted.
Theme 1: Peer support requires effort and intentionality
Our study found that peer support is fraught with psychological complexity as many participants shared their fears about seeking support. This may reflect a workplace culture with limited psychological safety, which is the belief that it is safe to take interpersonal risks such as speaking up (Edmondson, 1999). When nurses feel safe, they are more likely to speak up and seek support (Cho et al., 2023). When nurses feel unsafe, they engage in avoidant behaviours, including withholding questions and support-seeking. This avoidant behaviour was evident in our study and is consistent with findings from other healthcare contexts. Tedone and Lanz (2024) described similar reluctance among nurses to seek help for fear of being judged as incompetent. These cross-contextual parallels suggest that fears about judgement and repercussions in peer interactions are not unique to Singaporean nursing settings. However, our study adds to this discussion by highlighting how nurses actively negotiated when and how to seek support, balancing the need for assistance with concerns about patient safety and maintaining professionalism.
O’Donovan and McAuliffe’s (2020) systematic review identified cultural safety and learning promoted by leadership, support from peers and leaders, and hierarchy as key enablers of psychological safety in healthcare teams. Our findings resonate with these enablers, in demonstrating how trust, hierarchy, and leadership modelling shape peer support dynamics. The review also identified familiarity among team members as critical for psychological safety as frequent turnover impedes the development of trusting interpersonal relationships. This is especially pertinent in our study as data collection coincided with a period of organisational transition where nurses were being reassigned across multiple wards. This reshuffling of manpower may have disrupted the formation of a stable core team, thereby impeding the development of psychological safety necessary for support-seeking.
We also found that when nurses in our study do not feel safe to seek support, their professional duty to prioritise patient safety contradicts their desire to protect their own emotional well-being. This tension reflects moral distress, which occurs when nurses are unable to act according to their professional responsibilities (Salari et al., 2022). Navigating these challenges require moral resilience, which is the ability to uphold moral integrity despite emotional and ethical dilemmas (Young and Rushton, 2017). Nurses with strong moral resilience maintain quality patient care by drawing onto their ethical and professional values, even in the face of workplace challenges (Morley et al., 2022). Our findings support this: participants described prioritising their professional obligations and commitment to patient care over their own emotional needs. Without sufficient moral resilience to manage their distress, nurses may inadvertently compromise patient care.
Theme 2: Boundaries shape how support is negotiated
Participants reported a preference for seeking help from close peers, which emphasises the importance of interpersonal relationships. When close peers were unavailable, they sought out assistance from trusted and knowledgeable peers rather than those of higher rank. This underscores the role of informal leaders, who are highly competent nurses often sought out by others due to their expertise and influence, despite lacking formal leadership positions (Lawson et al., 2019). Our study aligns with existing research, showing that nurses seek support based on trust, familiarity, and perceived competence, rather than hierarchical status.
Some participants shared that hierarchy created barriers to constructive feedback and caused tension within the nursing team. This aligns with Essex et al. (2023), whose scoping review highlights how healthcare hierarchical structures often impede open communication and discourage feedback. Similarly, Sahay and Willis (2022) found that junior nurses frequently experienced anxiety and fear when interacting with senior nurses. In both studies, as in ours, hierarchy not only hindered support-seeking behaviours but also reinforced traditional patterns of deference and silence, limiting opportunities for reflective practice and collaborative learning.
Additionally, there is an implicit assumption that senior nurses require minimal support, which can contribute to unaddressed stress and affect their well-being. Existing literature primarily focuses on the challenges faced by junior nurses during transition to practice. Notably, research on supporting senior nurses in their roles remains a little-studied area and this lack of emphasis may stem from the assumption that experienced nurses are self-sufficient and need less support (Bry and Wigert, 2022). However, senior nurses encounter unique challenges, including increased responsibilities, emotional strain, and evolving workplace dynamics. These factors are identified as pertinent to nursing attrition in a systematic review by Lessi et al. (2025).
Our study found that some nurses provide support selectively based on perceived necessity, reflecting a culture that values self-reliance while also expecting mutual support. This dual expectation creates ambiguity around when it is appropriate to seek or provide support. Padgett (2013) identified a similar tension between autonomy and peer support, in which nurses provided support only when explicitly requested and refrained from offering unsolicited assistance to avoid encroaching on their peers’ autonomy. In contrast, the tension in this study lay between self-reliance and peer support: nurses felt obliged to manage tasks independently to avoid burdening their peers or being judged, yet still proactively offered help to maintain patient safety and reciprocity. Although both studies show that professional norms shape peer support, the motivations differ, reflecting variations in organisational and cultural contexts. Padgett’s study was conducted in a Western hospital operating under a total patient care model, where responsibility was individualised, professional autonomy highly valued, and collective accountability limited. In our study, team nursing was practised within a Confucian-influenced context, where collaboration was essential and interpersonal interactions were guided by values of collective responsibility, reciprocity, and relational harmony (Chang et al., 2025). Self-reliance was further reinforced by professional norms, including the expectation that early career nurses demonstrate competence through independent practice before passing probation. Although independence and teamwork are typically examined in isolation, our findings show that nurses must navigate this duality daily by deciding when to work independently and when to engage in peer support. The paradox functions as a core mechanism that organises and shapes the everyday of peer support. This study advances existing scholarship by identifying the independence–peer support paradox as a feature of contemporary nursing practice in our local context. By conceptualising peer support as a socially mediated practice structured by this paradox, our study provides a framework that recognises how cultural, structural, and professional factors converge in practice.
Theme 3: Leadership shapes the culture of support
Participants recognised the pivotal role of leaders in shaping peer support within nursing teams. This aligns with previous studies that show how nursing leaders’ influence extends beyond policies and procedures to shaping the daily interpersonal dynamics that define the work environment (Hayward et al., 2016).
Although leaders do not always engage in direct peer support at the bedside, their presence ‘on the floor’ serves as a powerful symbol of solidarity and legitimises peer support as a shared endeavour rather than a bottom-up responsibility (Liao et al., 2023). Conversely, leaders who are absent from clinical settings risk being perceived as unsympathetic to frontline challenges, which can diminish respect and morale (Taylor, 2016). Leaders who are overburdened by bureaucracy and are less present at the bedside may unintentionally undermine their own authority, as nurses may view their initiatives as out of touch. Our findings align with existing research demonstrating that leadership visibility positively impacts team morale and collaboration (Morsiani et al., 2017).
Theme 4: Peer support promotes resilience and retention
Some participants reported experiences of being intentionally excluded, reflecting elements of bullying and incivility, though they did not explicitly label them as such. Bullying involves repeated behaviours directed towards an intended target with an intent to harm (Shoorideh et al., 2021). In contrast, incivilities are disrespectful behaviours with an ambiguous intention to harm and are typically not in the scope of legal sanctions despite their negative effects (Keller et al., 2020). Participants’ inability to identify these experiences as bullying and incivilities suggest that such behaviours are normalised. This lack of recognition, widely noted in the literature, allows unhealthy workplace dynamics to persist, undermining team cohesion, and increasing turnover. Even when recognised, such behaviour often goes unreported due to fears of retaliation, perpetuating its presence in nursing (Taylor, 2016).
To integrate all themes into a cohesive conceptual understanding, we drew upon Wenger’s theory of Communities of Practice (CoP) as the overarching framework. A CoP is a group of individuals who engage in collective learning within a shared domain of human endeavour. Wenger (2000) identified three essential elements: the domain, the community, and the practice. The domain represents the shared interest that gives the group its identity. The community encompasses the relationships and mutual engagement among members. The practice refers to the shared repertoire of knowledge, experiences and ways of doing things that the members develop and refine over time. In this study, informal peer support can be conceptualised as a CoP. The domain is grounded in a collective commitment to patient safety, professional standards, and the well-being of the nursing workforce. This is reflected in Theme 1, where nurses deliberately sought to seek and provide support despite the complexities of doing so, demonstrating commitment and engagement in the shared enterprise. The community is enacted through routine workplace interactions, such as through conversations and shift handovers, where relationships are established and sustained. However, participation is shaped by trust, hierarchy, cultural norms, and reciprocity (Theme 2), which influence who engages and how support is negotiated. The practice is embodied in the collective knowledge that nurses share, such as specific work routines, shared language, and coping strategies. Leadership (Theme 3) plays a crucial role here by mediating conflicts, performing symbolic acts, and modelling supportive behaviours, to embed peer support within the community’s shared repertoire. The outcomes of active participation in this CoP (Theme 4) show that engagement in peer support enhances nurses’ professional identity, resilience and motivation. These outcomes align individual actions towards sustaining a supportive and learning oriented workplace community. Through the CoP lens, it becomes evident that nurses develop and adapt through shared social and professional interactions rather than through formal training alone. Peer support functions not merely as a social process but as a central mechanism of professional learning. Knowledge and expertise are co-constructed through everyday interactions in nursing practice. As such, spontaneous peer support among nurses is a living example of community practice, where collective learning and shared resources drive both personal and organisational improvement.
Strengths and limitations
The study’s strengths include its in-depth qualitative approach, which allowed participants to provide rich, detailed accounts of their experiences, and the use of rigorous methods such as thematic saturation, triangulation, and reflexive practices to enhance trustworthiness.
Social desirability bias may have influenced how openly participants discussed sensitive issues of vulnerability and support-seeking. This study was conducted in a newly established acute hospital in Singapore, where the nursing workforce was predominantly young Singaporean and Malaysian nurses early in their careers. This specific organisational and cultural context may have influenced how peer support was experienced and described. In newer institutions with a younger workforce, hierarchy may be less entrenched and peer support may manifest more collaboratively. Conversely, in older and more established hospitals with intergenerational teams, hierarchies, and longstanding leadership, cultures may exert a different influence on peer support. Additionally, within Singapore’s collectivist and high-power distance culture, deference to senior staff may subtly shape how nurses seek and provide support, particularly in interactions involving authority. Those contextual factors likely shaped the themes that were identified, especially those related to leadership and hierarchy. Although the findings cannot be transferable to all nursing contexts, they offer insights that may be transferable to other hospital settings with similar cultural characteristics or organisational structures. Readers are encouraged to consider how factors such as workforce composition and cultural norms may affect the applicability of these results in their own settings.
Recommendations
Integrating moral resilience training, as well as anti-bullying and civility education into nursing curricula and workplace programmes, can equip nurses with the skills to navigate ethical challenge, foster collaboration, and prevent workplace incivility (Crawford et al., 2019; Han et al., 2023).
Nursing leaders should be enabled to balance administrative responsibilities with visible frontline engagement to model supportive behaviours and foster collaboration (Phillips et al., 2023; Rosengren and Friberg, 2024). Relational leadership, which prioritises interpersonal engagement, is recommended to strengthen peer support and cultivate a positive ward culture (Cummings et al., 2018; Kaiser, 2017).
Interventions aimed at promoting nurses’ wellbeing should target informal peer support, as the peer support that occurs spontaneously between nurses in daily practice reinforces collaboration in ways that formal programmes alone cannot achieve. These interventions should be implemented with organisational stability in mind, as stable team structures are critical for fostering psychological safety.
Organisations should recognise and empower informal nurse leaders through mentorship and leadership development programmes, as these individuals exert significant influence through earned trust and competence rather than formal hierarchy. Nurses who are frequently overlooked by others as potential sources of support may benefit from target skill-building initiatives. Nursing competence should be conceptualised not only as individual ability but also as the capacity to collaborate effectively with others (Sebok-Syer et al., 2018; Shinners and Franqueiro, 2017).
Further research is needed to explore how nurses reconcile dual expectations of self-reliance and teamwork. Given that the departure of senior nurses can be particularly disruptive, examining how their support needs differ from those of junior nurses may ensure that support systems address the needs of all nurses, regardless of experience level.
Conclusion
This study highlights that informal peer support among hospital nurses is a multifaceted and complex process shaped by individual initiative, relational boundaries, workplace culture, and leadership practices. Rather than a spontaneous or automatic exchange, peer support was described as effortful and deliberate, often constrained by hierarchy and expectations of reciprocity, but sustained when leaders modelled collaboration and maintained visibility on the ward.
Although organisational policies can set expectations for teamwork, the findings suggest that ward-level culture particularly peer dynamics and frontline leadership has a more enduring influence on how support is enacted in daily practice. Informal peer relationships offered nurses immediate emotional reassurance and a sense of belonging, however, the responsibility for initiating and sustaining these connections frequently rested on individual nurses. This created variable access to informal peer support, shaped by nurses’ level of social embeddedness within the ward community.
To strengthen peer support, healthcare organisations should focus on cultivating psychological safety, addressing hierarchical barriers, and empowering visible, relational leadership that embeds collaboration into everyday practice. When these conditions are met, peer support can serve not only as a buffer against occupational stress but also as a driver of resilience, job satisfaction, and workforce retention.
Importantly, fostering a culture of peer supports may function as a preventative mental health strategy, helping nurses manage emotional demands and sustain psychological well-being in stressful clinical settings. These findings contribute to the growing evidence that relational workplace practices are essential to the mental health and sustainability of the nursing workforce.
Key point for policy, practice and/or research
The findings highlight the importance of nursing leadership to promote informal peer support.
Addressing hierarchical barriers and modelling of collaborative behaviours by leadership are essential to embed informal peer support in everyday nursing practice.
Fostering psychological safety, adressing incivility and promoting respectful communication should be organisational priorities.
Integrating moral resilience into nursing education and professional development may equip nurses to manage ethical tensions.
Investigating the support needs of senior nurses may ensure that support systems address the needs of nurses across all experience levels.
Research to explore how nurses reconcile dual expectations of self-reliance and teamwork may help to strike a balance that fosters both individual competence and a collaborative work environment.
Footnotes
Acknowledgements
The authors would like to thank Ms Poh Chee Lien and Dr Dong Li Juan for their thoughtful feedback on previous versions of this work, as well as the registered nurses who generously volunteered their time to participate in this study. The authors also extend their appreciation to the three anonymous reviewers for their constructive comments, and to Ms Sheena Nishanti D/o Ramasamy for her assistance with manuscript editing for submission.
Author contributions
Data availability
The data that support the findings of this study are available from the corresponding author (BM) upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the National Healthcare Group Domain Specific Review Board (2023/00791) on 14 February 2024. Respondents gave written consent before starting interviews.