
Abstract
Background:
Early ambulation (EA) supports recovery in cardiovascular patients. Its effects on haemodynamic stability and clinical outcomes in non-ST elevation myocardial infarction (NSTEMI) patients before coronary angioplasty are unexplored.
Aims:
To evaluate EA’s impact on haemodynamic stability and clinical outcomes in NSTEMI patients before coronary angioplasty.
Methods:
A quasi-experimental study was conducted in two cardiac wards with 154 NSTEMI patients, assigned to EA (n = 77) or complete rest in bed (CRIB) (n = 77). Haemodynamic parameters, telemetry events (non-sustained ventricular tachycardia) and cardiac events (angina, reinfarction, dyspnoea and syncope) were monitored. Logistic regression assessed associations between EA and clinical outcomes.
Results:
Demographic and clinical characteristics were similar between groups (p > 0.05). Haemodynamic parameters remained stable in both groups (p > 0.05). EA was associated with a 79% reduction in cardiac events (OR = 0.21, 95% confidence interval (CI) (0.07, 0.60), p = 0.003) and a trend towards fewer telemetry events (OR = 0.27, 95% CI (0.07, 1.03), p = 0.06). EA also shortened hospitalisation by a mean of 49.56 hours (p = 0.02).
Conclusion:
EA before coronary angioplasty is safe, reduces cardiac events and shortens hospital stay. These findings support structured nursing-led EA as part of routine acute cardiology care and highlight its role in promoting patient-centred recovery, efficient resource utilisation and potential cost savings for healthcare providers.
Keywords
Introduction
Non-ST segment elevation myocardial infarction (NSTEMI) is a prevalent form of acute coronary syndrome. According to the Singapore Myocardial Infarction Registry (2023), NSTEMI accounted for 73.5% of all acute myocardial infarction cases in 2021, with approximately 9121 recorded incidences, forming a significant proportion of hospital admissions in cardiac wards. Given the high prevalence, optimising the management of NSTEMI patients is crucial to improving outcomes and reducing healthcare burdens.
Traditionally, NSTEMI patients are prescribed with complete rest in bed (CRIB) to reduce myocardial workload and prevent further perfusion impairment (Cortes et al., 2015). Despite variations in hospital practices globally, CRIB remains a standard practice in many settings for patients awaiting coronary angioplasty (Cortes et al., 2015). However, current international guidelines do not endorse CRIB for NSTEMI population. Instead, leading organisations such as the European Society of Cardiology and the American Heart Association advocate for early ambulation (EA) following coronary angioplasty, citing benefits such as improved patient outcomes and shorter hospital stays (Amsterdam et al., 2014; Byrne et al., 2023; Rao et al., 2025). In Singapore, there is no national policy dictating the mobility management of NSTEMI patients prior to intervention, highlighting the need for evidence-based practice.
Although EA is widely practiced and established post-angioplasty, its role in stabilising NSTEMI patients before intervention remains inadequately studied, leaving a critical evidence gap in pre-angioplasty ambulation (Amsterdam et al., 2014; Cortes et al., 2009; Munir et al., 2020). Meta-analyses have shown that EA after myocardial infarction can improve cardiovascular outcomes (Hama et al., 2021; Johnson et al., 2023; Kanejima et al., 2020; Munir et al., 2020; Nakamura et al., 2021), reduce mortality rates (Cortes et al., 2015; Okada et al., 2019) and shorten hospital stays (Fleming et al., 2018; Johnson et al., 2023; Munir et al., 2020). However, no studies to date have investigated the impact of EA in NSTEMI patients awaiting coronary interventions.
From a physiological perspective, prolonged bedrest is associated with cardiovascular deconditioning, including impaired endothelial function and altered autonomic regulation, all of which may increase vulnerability to arrhythmias and adverse cardiac events (Lavie et al., 2019; Mastrandrea et al., 2024). In contrast, light to moderate ambulation enhances endothelial function through increased blood flow and shear stress, resulting in increased nitric oxide production and bioavailability (Man et al., 2020).
Beyond these immediate cardiovascular effects, prolonged immobilisation during hospitalisation is associated with adverse outcomes such as muscle atrophy, venous thromboembolism, delayed recovery and hospital-acquired deconditioning, which can begin within 24 hours of inpatient stay (Al-Dorzi et al., 2023; Cortes et al., 2015; Gordon et al., 2019; Hama et al., 2021; Lau et al., 2020; Wegiel et al., 2018). Evidence from post-angioplasty populations suggests that EA can improve physical function, psychological well-being and autonomy (Wegiel et al., 2018; Zhang et al., 2018).
Additionally, introducing EA before coronary intervention aligns with the principles of prehabilitation, a growing concept in cardiac care that aims to enhance functional capacity and reduce complications before major procedures (Steinmetz et al., 2023). Prehabilitation strategies have been linked to improved surgical and procedural outcomes, further supporting the potential benefits of EA in NSTEMI patients awaiting intervention. From a nursing perspective, EA aligns with Orem’s self-care deficit theory which emphasises the nurse’s role in supporting patients to regain independence through education and empowerment (Orem, 2001; Yip, 2021). By integrating EA into NSTEMI care, nursing can directly contribute to safer, faster recovery, lower resource utilisation and improve patient-centred outcomes. Hence, this study aims to investigate the safety and efficacy of EA in NSTEMI patients prior to coronary angioplasty, focusing on cardiovascular outcomes, telemetry events and length of hospital stay. The research hypothesises that EA is as safe as CRIB in maintaining haemodynamic stability while enabling patients to achieve mobility and functional milestones required for safe discharge, thereby potentially reducing cardiac events, telemetry abnormalities and overall hospital stay.
Methodology
Study design
A two-armed quasi-experimental, nonrandomised study compared the effects of EA versus CRIB on haemodynamic stability and cardiac events in NSTEMI patients before coronary angioplasty. The study was conducted over 10 months in two cardiac general wards of an academic tertiary hospital in Singapore.
Ward-based allocation was implemented to avoid cross-contamination of mobility protocols within the same unit, ensuring consistency in care delivery. Individual randomisation was not feasible because nursing workflow, telemetry resources and ambulation pathways were organised at the ward-level. Randomising patients within the same ward risked protocol cross-over, inconsistent implementation and safety concerns. Ward A implemented the EA protocol, whereas Ward B adhered to standard CRIB practices. Standardised mobility protocols and staff training were applied across both wards to minimise variability in care delivery.
Potential cluster level bias was addressed by including ward as a covariate in regression models and adjusting for baseline characteristics. This covariate adjustment mitigates confounding arising from differences in ward cultures or nursing practices. Blinding of participants and staff was not possible due to the nature of the intervention requiring active participation. However, the potential bias in outcome monitoring was minimised through strict protocol adherence and standardised monitoring by the primary investigator.
Setting and participants
The study was conducted from November 2022 to September 2023 in two cardiac general wards, each with a 45-bed capacity, at a tertiary hospital in Singapore. Adult cardiology patients admitted with NSTEMI were recruited consecutively according to predefined inclusion and exclusion criteria, constituting a purposive sampling approach appropriate for intervention studies requiring participants to meet specific clinical characteristics (Campbell et al., 2020).
Inclusion criteria were patients aged 21 years or above, diagnosed with NSTEMI and under standard continuous telemetry monitoring. Exclusion criteria were defined to ensure patient safety and minimise confounding clinical instability. Patients with markedly elevated cardiac troponin level ⩾10,000 ng/L or ST-segment elevation myocardial infarction were excluded due to higher infarct burden and the need for urgent invasive management. Suspected left main disease and advanced heart failure (Killip III and IV) was excluded because of the increased risk of haemodynamic deterioration with mobilisation. Patients with symptomatic unstable arrhythmias or ongoing angina were excluded to avoid precipitating adverse cardiac events. Those with haemodynamic instability (systolic blood pressure <90 mmHg or ⩾180 mmHg) were excluded due to the risk of compromised perfusion or hypertensive complications during ambulation. Patients with existing thromboembolism complications (i.e. deep vein thrombosis and pulmonary embolism) were excluded because mobilisation may increase embolic risk. Individuals with diagnosed psychiatric or cognitive impairment (abbreviated mental test score <7 in patients aged ⩾ 65 years old, as assessed using the Abbreviated Mental Test (AMT)) were excluded due to concerns regarding capacity to follow safety instructions. Patients demonstrating non-compliant behaviour, assessed by the nursing staff during the initial admission based on refusal to follow medical advice, frequent disregard for hospital protocols or a history of leaving the hospital against medical advice, were excluded to ensure adherence to the ambulation protocol and to minimise safety risks during mobilisation. These exclusion criteria were based on established guidelines from the European Society of Cardiology acute coronary syndromes (Byrne et al., 2023), the hospital’s trigger protocol guidelines and the Ministry of Health Singapore AMT tool (Sahadevan et al., 2008).
The AMT was applied as a standardised cognitive screening tool for patients aged ⩾65 years. It is routinely administered in general wards upon admission or when a patient’s condition changes. Ward nurses conducted the AMT as part of standard care, and patients scoring below seven were identified as having significant cognitive impairment and were excluded to ensure they could provide informed consent, safely follow mobility protocols and to minimise the risk of falls, protocol deviation and unreliable symptom reporting during EA.
Sample size calculation
The sample size calculation followed Cohen’s recommendation for comparing two independent groups (Cohen, 1992). Although studies on EA in cardiac populations exist, they do not report effect size. As EA is a novel intervention in this specific NSTEMI population, a medium effect size was considered a conservative and reasonable estimate. For studies comparing two groups using an independent sample t-test, a medium effect size requires a minimum sample size of 64 participants per group to achieve a statistical power of 0.80 at an alpha level of 0.05 (Brydges, 2019). Accounting for a20% attrition rate, 154 participants were recruited.
Participant flow
A total of 168 patients were screened for eligibility. Of these, 154 patients were enrolled, with 77 participants in each group. Fourteen patients did not proceed with enrolment: five were excluded based on predefined medical criteria, whereas nine declined participations (see Figure 1). No loss to follow-up or patient dropout occurred throughout the study period.
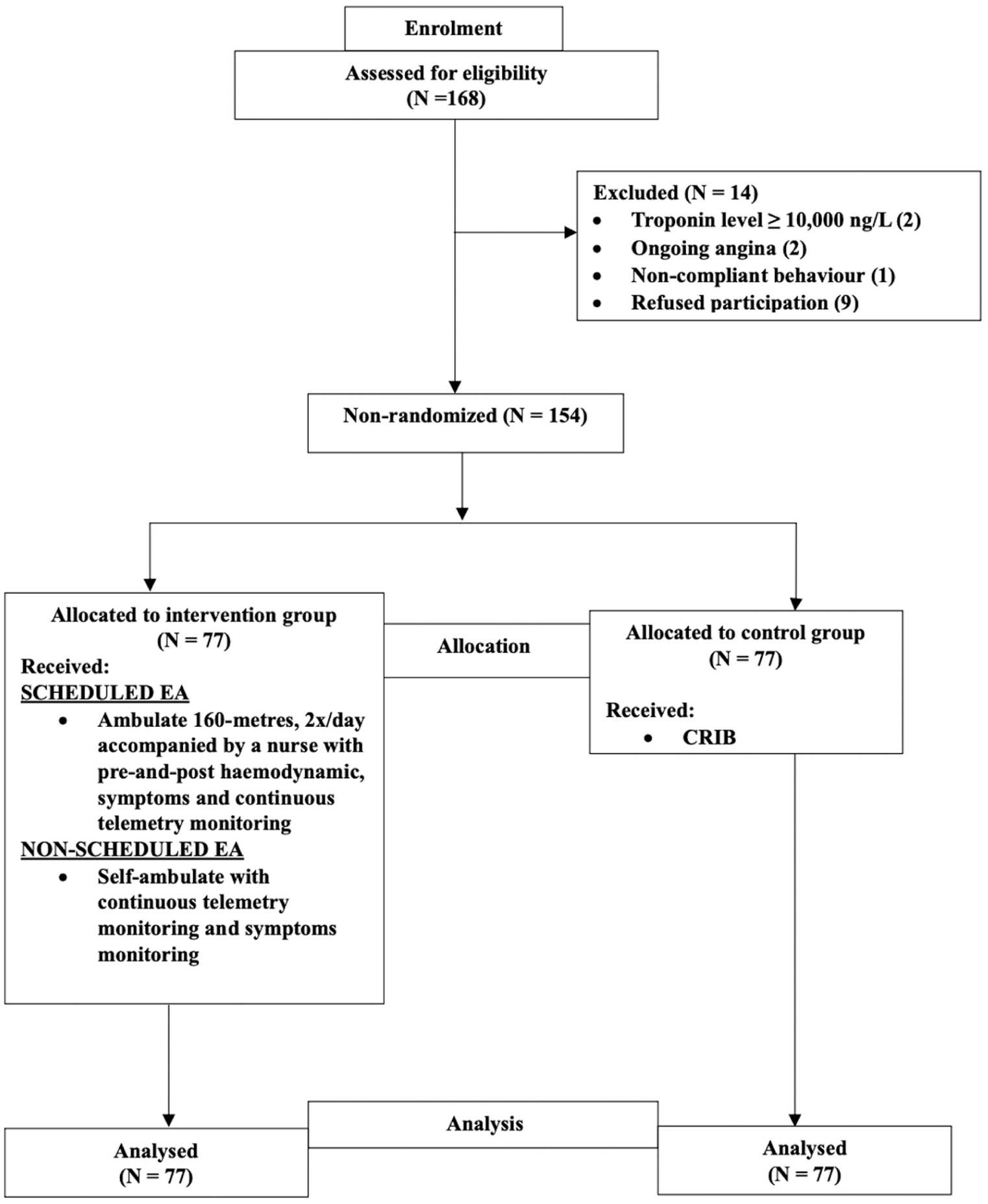
Enrolment process.
Intervention group
The intervention group consisted of 77 patients from Ward A who engaged in scheduled and non-scheduled ambulation sessions. Ambulation was initiated within the first 24 hours of admission if clinical stability criteria were met.
Scheduled ambulation sessions were conducted twice daily, with participants ambulating approximately 160-metres in 10 minutes. This distance was equivalent to walking twice the length of the ward corridor. The ambulation protocol was designed to correspond to light-to-moderate intensity activity, based on established metabolic equivalent of task (MET) ranges for walking and common ward-based activities (American College of Sports Medicine, 2022; Mendes et al., 2018), depending on patient tolerance and clinical condition.
Pre-ambulation vital signs were measured to ensure clinical stability. Ambulation was withheld if contraindications were present, including: (1) new onset or worsening angina, (2) systolic blood pressure <90 mmHg or ⩾180 mmHg, (3) heart rate (HR) >110 beats per minute, (4) oxygen saturation <94% and (5) signs of breathlessness, dizziness, syncope or new arrhythmias.
During ambulation, participants were accompanied by a nurse and continuously monitored via telemetry to detect any adverse events. Rest intervals were allowed as needed to help patients manage fatigue, optimise comfort and ensure safety. Nurses documented vital signs and symptoms in a standardised ambulation checklist, and telemetry data were reviewed post-session to detect any arrhythmias. To enhance engagement, participants were encouraged to partake in light activities of daily living (ADLs) such as bathing, dressing and toileting, which are classified as light intensity activities based on established MET ranges reported in standard compendia (American College of Sports Medicine, 2022; Thompson et al., 2024). Adherence to the EA protocol was recorded using a standardised ambulation diary. For each participant, the number of prescribed and completed sessions were logged by nursing staff.
Nursing staff received comprehensive training on trigger parameters and symptom escalation. In cases of patient-reported angina, serum troponin levels and electrocardiograms were checked to assess for potential ST-segment elevation myocardial infarction, with re-evaluation by the physician. Nurses were expected to respond promptly to haemodynamic instability, arrhythmias, syncope or falls, following routine care protocols. In the event of adverse events, activity was immediately ceased, and a physician triggered to administer appropriate rescue treatments.
Control group
The control group consisted of 77 patients from Ward B who followed standard CRIB practices. Participants remained in bed with only minimal repositioning for personal care, bedside sitting for meals and necessary hygiene activities under nursing supervision. Vital signs were monitored at the same intervals as in the intervention group, and continuous telemetry monitoring was conducted to observe cardiac events.
Data collection
Consecutive sampling was employed to ensure that all eligible patients admitted during the study period were screened and considered for inclusion. Ward nurses monitored patient recruitment daily and the primary investigator conducted weekly reviews to ensure consistency and reduce selection bias.
Baseline demographic and clinical data, including age, sex, ethnicity, functional status, cardiovascular risk factors, peak troponin levels, beta-blockers use and thrombolysis in myocardial infarction (TIMI) predictive risk score, were collected. The TIMI risk score, a validated risk stratification tool for predicting death, myocardial infarction, or urgent revascularisation within 14 days in patients with NSTEMI, was used to stratify baseline risk. This score is based on seven clinical variables – age, the presence of at least three coronary risk factors (e.g. hypertension, diabetes, hyperlipidaemia, smoking or family history of coronary artery disease), known coronary stenosis (>50%), aspirin use in the prior 7 days, severe angina (two or more episodes within the preceding 24 hours), elevated cardiac biomarkers and ST-segment deviation on the electrocardiogram. Higher scores indicate a greater risk of adverse cardiac events (Kumar et al., 2021; Namazi et al., 2022).
Data from both groups were collected over a maximum of 72 hours prior to coronary angioplasty. Data for the intervention group were logged in the Ambulation Diary, whereas data for the control group were documented in the CRIB Events Record. Haemodynamic parameters (blood pressure (BP), HR and oxygen saturation (SPO2)) were measured pre- and post-session and averaged per participant to provide a representative measure for analysis. Telemetry events and ambulation sessions were recorded individually for each participant and analysed as discrete events. Weekly reviews by the primary investigator ensured data accuracy and completeness. Exercise intensity was standardised at the protocol level using established MET classifications for walking and ADLs. Individual MET values were not calculated. The total number of ambulation sessions per day was calculated for each participant to assess adherence to the EA protocol.
Measurement of primary and secondary outcomes
Primary outcomes included haemodynamic stability, non-sustained ventricular tachycardia (NSVT) and cardiac events. Haemodynamic stability was measured by monitoring BP, HR and SPO2 before each ambulation session and again after a 3-minute rest period following the session for every participant to ensure accuracy (Unger et al., 2020). Telemetry monitoring prioritised NSVT due to its clinical relevance in NSTEMI patients, as it can progress to more serious ventricular arrhythmias and is associated with increased risk of mortality (Bui et al., 2016). The five cardiac events assessed were: (1) angina: self-reported chest pain; (2) reinfarction: a rise in cardiac biomarkers (troponin I levels) above patient baseline with new ischaemic changes on electrocardiogram or telemetry; (3) dyspnoea: self-reported difficulty breathing with corresponding oxygen desaturation; (4) syncope: documented based on patient reports and nurse observations; (5) falls: documented falls related to cardiac instability and secondary outcomes included length of hospital stay.
Data analysis
Statistical analysis was performed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics including means, standard deviations (SDs) and frequencies were used to characterise the participants’ profile. For the primary efficacy analysis, the pre-session values between the EA and CRIB groups were compared using independent sample t-tests. The post-session values were analysed in the same way. No repeated-measures or mixed-effects models were employed at predefined analytic time points. Therefore, the reported results reflect between group comparisons only. In addition to p-values, Cohen’s d was calculated for all independent sample t-test comparing haemodynamic parameters between the EA and CRIB groups. Cohen’s d quantifies the magnitude of the between group differences, with values 0.2, 0.5 and 0.8 representing small, medium and large effects, respectively (Cohen, 1988). Independent sample t-test was also used to compare the length of hospitalisation between groups. Logistic regression evaluated telemetry events and cardiac events, with results reported as odds ratio (OR) with 95% confidence intervals (CIs). Multiple linear regression assessed EA’s association with length of stay, adjusting for confounders (age, sex, ethnicity and cardiovascular risk factors, including smoker, diabetes, hyperlipidaemia, hypertension, arrhythmias, heart failure, TIMI predictive risk score, coronary artery disease severity and beta-blocker use). All statistical tests were two-sided with a significance level set at p < 0.05.
Ethical consideration
Ethical approval was obtained from the National Healthcare Group Domain Specific Review Board (DSRB No: 2022/00529). Participation was voluntary, with anonymity and confidentiality ensured. Written informed consent was obtained from all participants before enrolment. Approval from the head of Cardiology Department ensured alignment with institutional standards and protocols. The study is reported in accordance with the Transparent Reporting of Evaluations with Non-randomized Design (TREND) statement for nonrandomised evaluations (Des Jarlais et al., 2004). The completed TREND checklist is provided as Supplemental Material.
Results
Participants characteristics
A total of 154 participants were recruited and divided into two groups, EA (n = 77) and CRIB (n = 77). Socio-demographic and clinical characteristics of the participants are presented in Table 1. No significant differences were found between the EA and CRIB groups in terms of age, sex, ethnicity, functional status, TIMI predictive risk score, arrhythmias, heart failure severity, beta-blocker usage or coronary angioplasty outcomes (all p-values >0.05).
Comparison of socio-demographic and clinical data between the EA and CRIB groups.
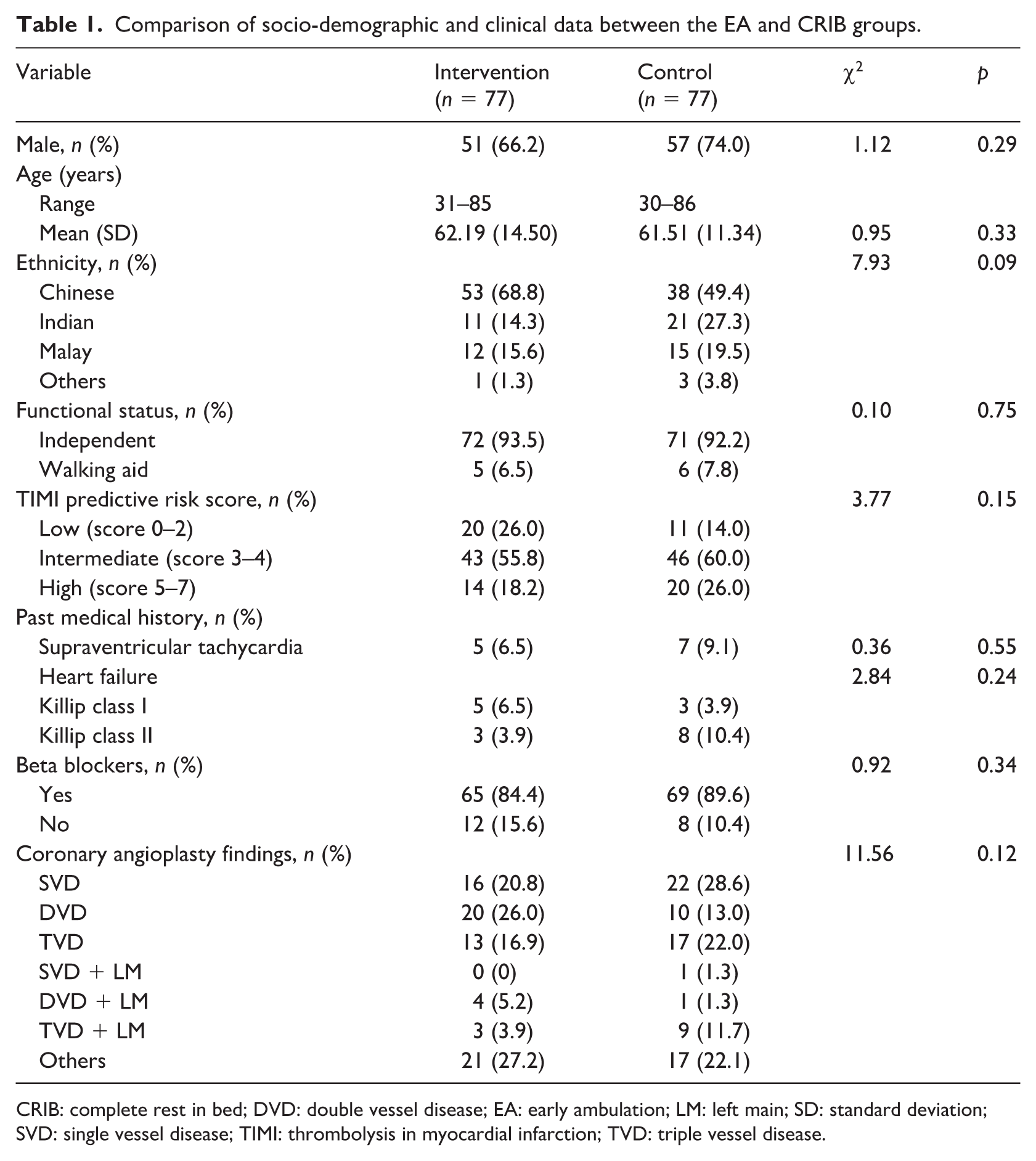
CRIB: complete rest in bed; DVD: double vessel disease; EA: early ambulation; LM: left main; SD: standard deviation; SVD: single vessel disease; TIMI: thrombolysis in myocardial infarction; TVD: triple vessel disease.
Intervention adherence and safety
A total of 207 ambulation sessions were completed by participants in the EA group over the 3-day intervention period. Participants completed a mean of 0.90 ± 0.54 ambulation sessions per day (Table 2). Although the protocol allowed for up to two scheduled ambulation sessions daily, session delivery was guided by clinical stability, procedural timing and patient tolerance, reflecting routine acute NSTEMI ward practice.
Adherence and safety outcomes in EA group (n = 77) a .
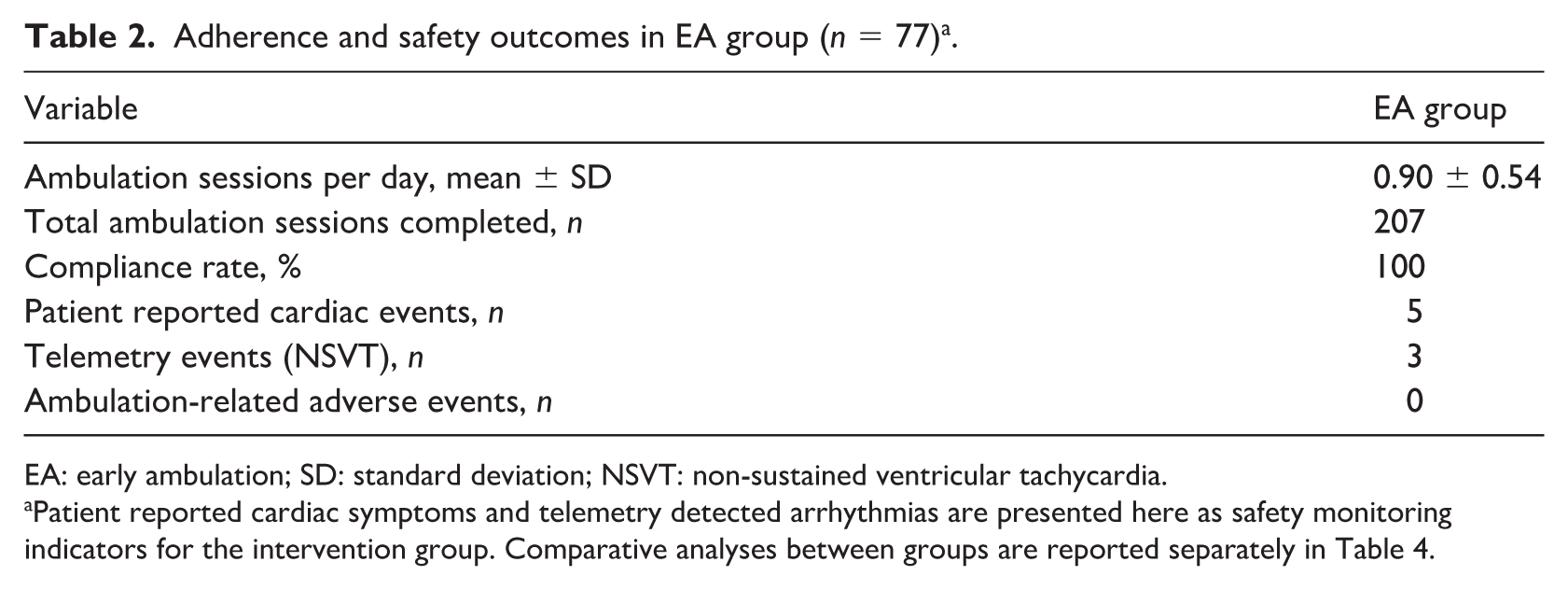
EA: early ambulation; SD: standard deviation; NSVT: non-sustained ventricular tachycardia.
Patient reported cardiac symptoms and telemetry detected arrhythmias are presented here as safety monitoring indicators for the intervention group. Comparative analyses between groups are reported separately in Table 4.
Nursing compliance with the ambulation protocol was 100%, with all prescribed sessions delivered when patients met predefined safety criteria. No participants withdrew from the intervention, and no ambulation sessions were terminated prematurely due to safety concerns.
Regarding safety monitoring, five participants experienced patient-reported cardiac symptoms and three participants had NSVT detected on telemetry during the study period. These events were monitored according to institutional protocols and did not necessitate cessation of the intervention. Importantly, no events met the predefined criteria for ambulation-related adverse events, including falls, syncope, sustained arrhythmias or haemodynamic compromise.
Haemodynamic status
There were no statistically significant differences between the EA and CRIB groups in systolic blood pressure (SBP), HR or SPO2 at any time point (all p-values >0.05; Table 3). Both groups maintained stable haemodynamic parameters before and after ambulation sessions. Effect sizes were trivial to small (Cohen’s d ⩽ 0.26), supporting that the magnitude of between group differences in haemodynamic parameters was clinically negligible. Within subject pre- or post-session changes were examined descriptively and were not subjected to formal repeated measures testing.
Comparison of pre-and-post haemodynamic parameters between both groups.
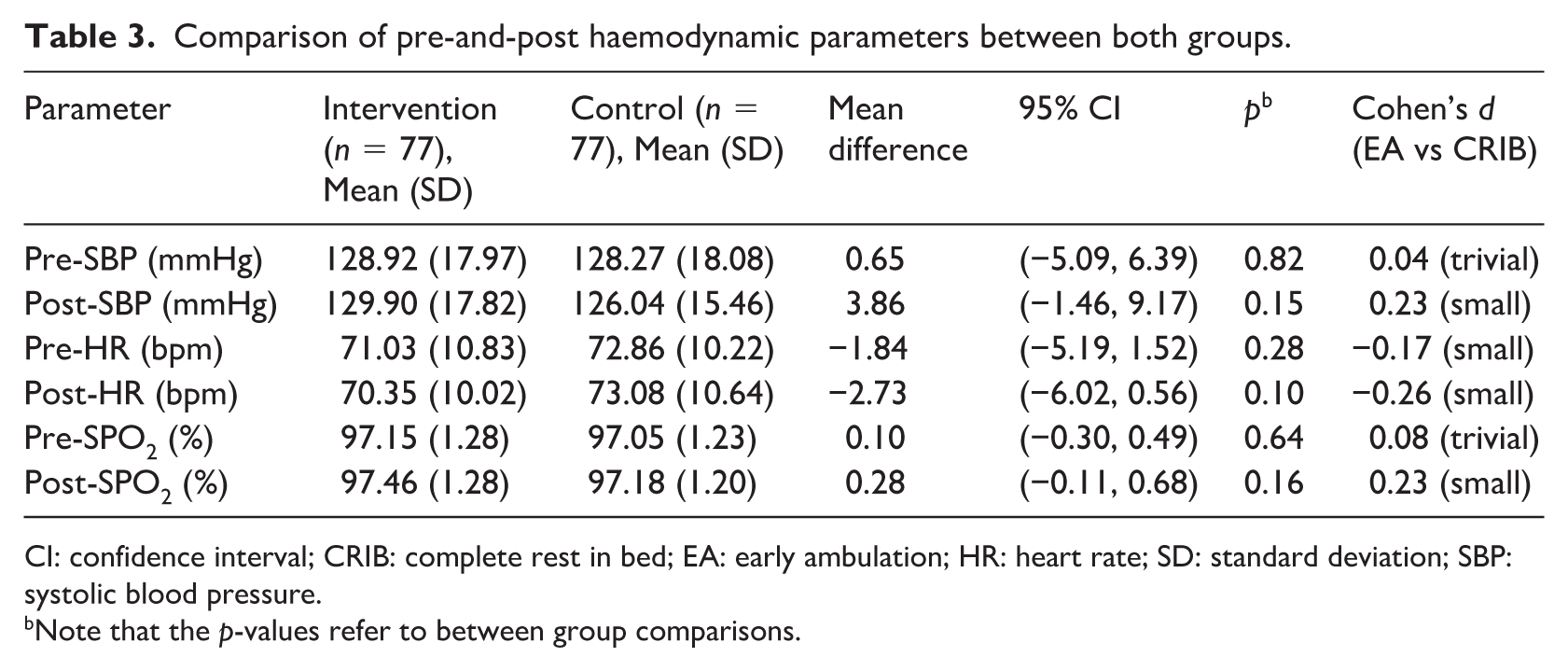
CI: confidence interval; CRIB: complete rest in bed; EA: early ambulation; HR: heart rate; SD: standard deviation; SBP: systolic blood pressure.
Note that the p-values refer to between group comparisons.
Telemetry events
A total of 10 telemetry events occurred in the CRIB group (12.99%), compared to 3 events in the EA group (3.9%). The odds of experiencing a telemetry event were significantly lower in the EA group (OR = 0.27, 95% CI (0.07, 1.03), p = 0.06). Although this difference did not reach statistical significance, the intervention group showed a trend towards fewer events (Table 4).
Comparison of telemetry and cardiac events between both groups.
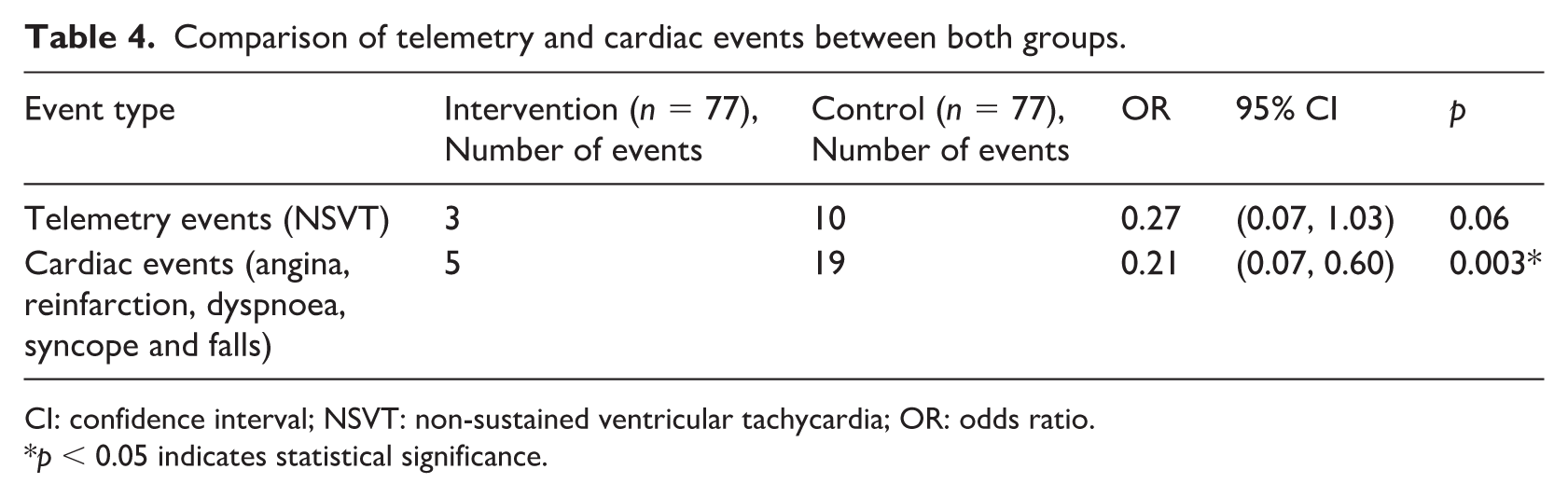
CI: confidence interval; NSVT: non-sustained ventricular tachycardia; OR: odds ratio.
p < 0.05 indicates statistical significance.
Cardiac events
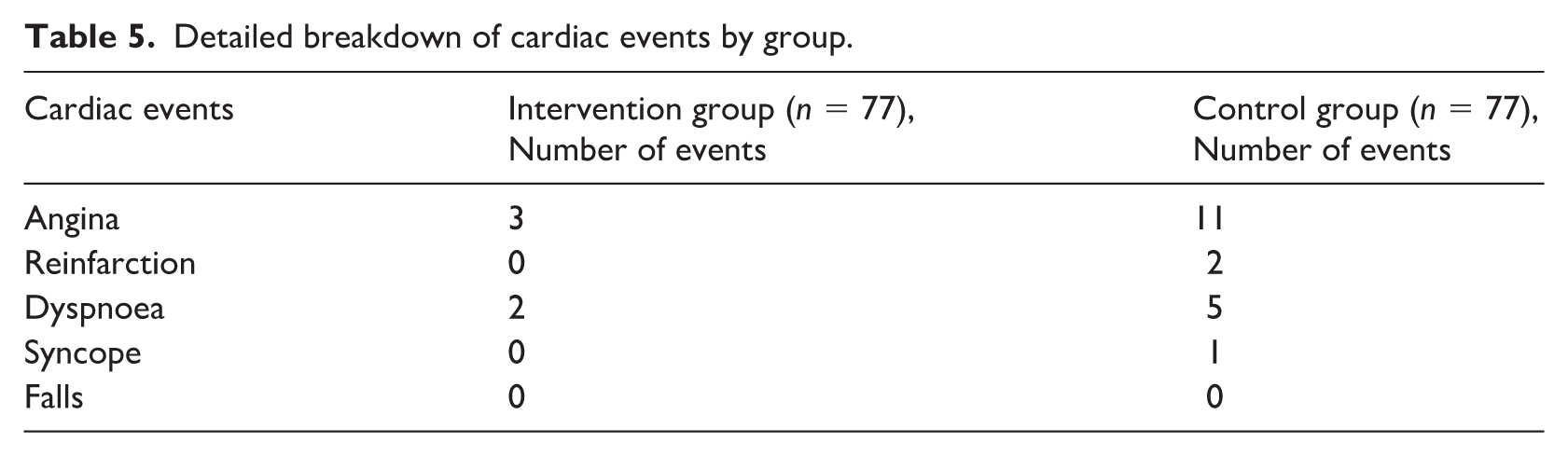
For cardiac events, 5 patients (6.49%) in the EA group experienced events, compared to 19 patients (24.68%) in the CRIB group. The odds of experiencing a cardiac event were significantly lower in the EA group (OR = 0.21, 95% CI (0.07, 0.60), p = 0.003; Table 4). This result highlights a clinically meaningful reduction in cardiac events associated with EA (Table 5; further breaks down the occurrences of each of the events by group).
Detailed breakdown of cardiac events by group.
Length of hospitalisation
No significant differences were observed between both groups regarding beta-blockers initiation or time to coronary angioplasty (all p-values >0.05). Current cardiovascular guidelines recommend coronary angioplasty within 24 hours of NSTEMI presentation (Lawton et al., 2022). However, in clinically stable patients with complicating comorbidities, angioplasty may be appropriately delayed for up to 72 hours due to staffing, procedural prioritisation or optimisation of comorbid conditions (Batchelor et al., 2020; Lawton et al., 2022). In this study, time to angioplasty did not differ between groups, reflecting routine clinical decision-making rather than differences in patient recovery.
The EA group had a significantly shorter length of hospitalisation (100.08 hours, SD = 77.53) compared to the CRIB group (149.64 hours, SD = 158.75), with a mean difference of 49.56 hours (95% CI (9.66, 89.45), p = 0.02; Table 6). After adjusting for key confounders in a multiple linear regression model, EA remained significantly associated with a reduced length of hospitalisation (B = −3625.87, 95% CI (−6366.04, −885.70), p = 0.01), suggesting an average reduction of approximately 60.43 hours compared to the CRIB group.
Treatment trajectory time frame (in hours) from admission.
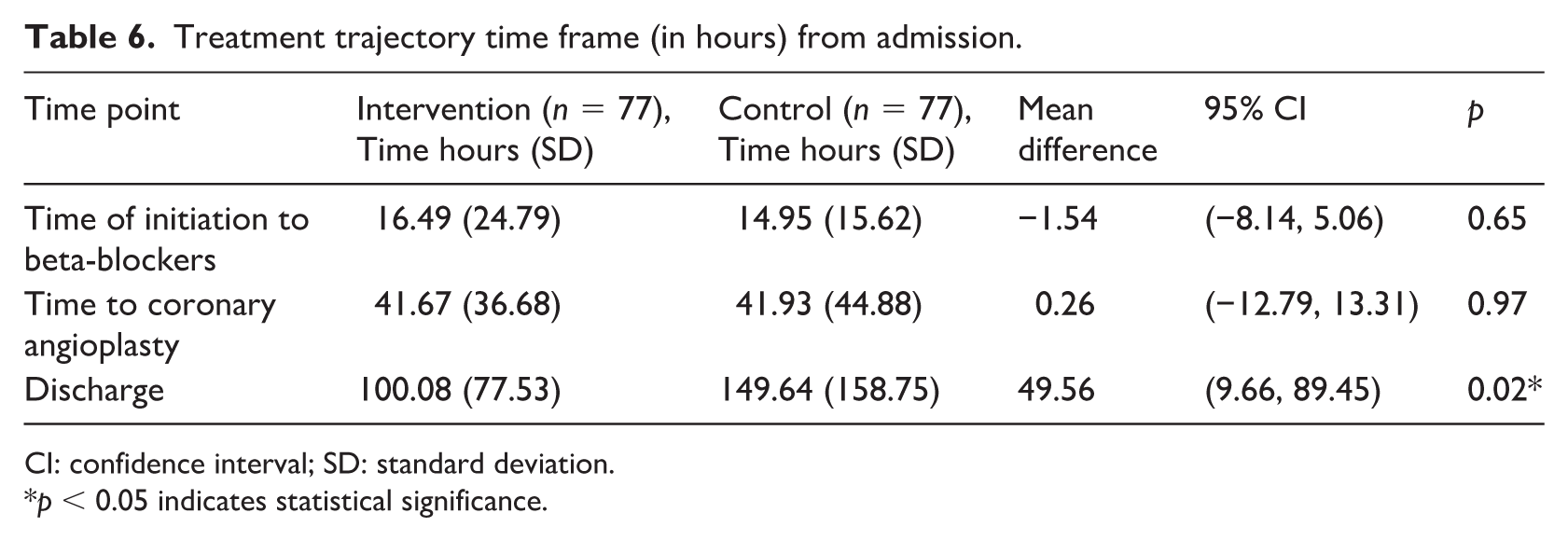
CI: confidence interval; SD: standard deviation.
p < 0.05 indicates statistical significance.
Beta-blocker use was also independently associated with shorter hospitalisation (B = −6247.11, 95% CI (−10182.25, −2311.96), p = 0.002). Other variables including age, sex, ethnicity and cardiovascular risk factors including: smoker, diabetes, hyperlipidaemia, hypertension, arrhythmias, heart failure, TIMI predictive risk score and coronary artery disease severity did not significantly affect length of stay (p > 0.05). Importantly, procedural timing did not differ between groups, indicating that the reduction in hospitalisation can be reasonably attributed to EA rather than differences in patient characteristics, medication use or procedural scheduling (Table 7).
Adjusted regression analysis for length of stay (in minutes).
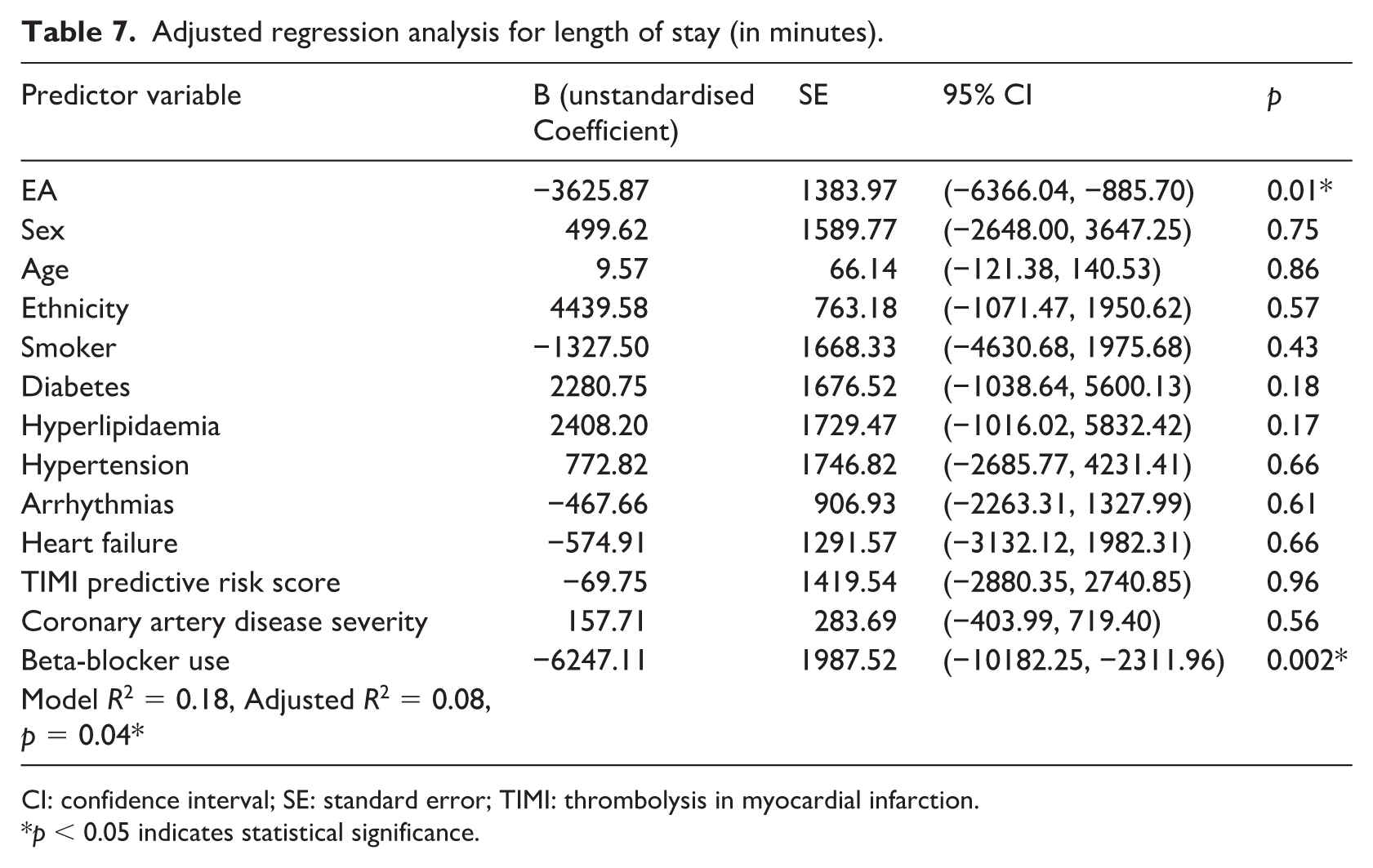
CI: confidence interval; SE: standard error; TIMI: thrombolysis in myocardial infarction.
p < 0.05 indicates statistical significance.
Discussion
This study provides strong evidence supporting the safety and efficacy of EA in NSTEMI patient pre-angioplasty. The findings demonstrate that EA does not compromise haemodynamic stability while significantly reducing cardiac events and shortening hospital stays. These results reinforce EA as a viable, evidence-based intervention that can be integrated into pre-procedural NSTEMI care.
Safety of early ambulation in NSTEMI patients
An important concern in mobilising NSTEMI patients before coronary angioplasty is the potential risk of haemodynamic instability. The between group analysis in this study demonstrates that EA does not compromise haemodynamic stability. The absence of statistically significant differences between groups, together with trivial to small effect sizes (Cohen’s d ⩽ 0.26), suggests that any observed variations in SBP, HR or SPO2 were minimal and clinically negligible. These findings support the safety of implementing structured EA protocols in this patient population.
While previous research has established the safety of EA in post-angioplasty patients (Zhang et al., 2018) and other cardiac populations (Nydahl et al., 2017), the safety of EA in NSTEMI patients awaiting intervention has remained inadequately studied (Munir et al., 2020; Zhang et al., 2018). This study addresses that evidence gap by demonstrating that structured, guided mobility can be safely implemented in the pre-procedural setting. The findings suggest that traditional bedrest protocols should be re-evaluated in favour of structured, guided mobility programmes for haemodynamically stable NSTEMI patients awaiting coronary angioplasty (Munir et al., 2020; Nydahl et al., 2017).
Reduction in cardiac events and impact of sedentary behaviour
A key outcome of the study was the statistically significant reduction in cardiac events in the EA group compared to the CRIB group (OR = 0.21, p = 0.003). This contrasts with previous literature, where no association was found between ambulation and reduced cardiac events (Herkner et al., 2007; Munir et al., 2020). Differences in ambulation protocols or patient characteristics may explain this discrepancy. Although previous studies focused on post-procedure ambulation, this study highlights the importance of EA even before coronary angioplasty.
Importantly, the CRIB group remained in bed for prolonged periods, effectively meeting the definition of sedentary behaviour. Sedentary behaviour is characterised by an energy expenditure of less than or equal to 1.5 METs while sitting, reclining or lying down (Tremblay et al., 2017). Studies indicate that sedentary behaviour exceeding 6 to 8 hours/day significantly increases the risk of cardiovascular deconditioning, heightened sympathetic activity and endothelial dysfunction, which predispose patients to arrhythmias and adverse cardiac events (Lavie et al., 2019). Patients in the EA group actively counteracted these detrimental effects, leading to a clinically meaningful reduction in cardiac events.
This finding is consistent with the understanding that prolonged inactivity, such as sedentary behaviour exacerbates the risk of cardiovascular events, whereas EA helps mitigate these risks by promoting circulatory and metabolic stability.
The CI for the association between EA and reduced cardiac events (OR = 0.21, 95% CI (0.07, 0.60)) is relatively narrow, suggesting a more precise estimate of the effect. Variability in effect size due to sample size constraints may still be present, and a larger cohort could provide more precise estimates. Although the reduction in telemetry events in the EA group did not reach statistical significance (p = 0.06), the observed odds ratio (OR = 0.27, 95% CI (0.07, 1.03)) suggests a clinically relevant trend. The confidence interval for telemetry events, spanning from 0.07 to 1.03 indicates some uncertainty in the estimates, which could be attributed to the smaller number of events. Future studies with larger sample sizes are warranted to further investigate this association.
Physiological mechanisms and the role of prehabilitation
The observed reduction in cardiac events in the EA group may be partially explained by underlying physiological mechanisms that support cardiovascular stability and functional reserve. Traditional post-MI mobilisation strategies typically focus on activity initiation after coronary intervention, once haemodynamic stability is established (Amsterdam et al., 2014; Byrne et al., 2023). In contrast, EA in this study was implemented pre-procedurally, positioning mobility not merely as rehabilitation, but as prehabilitation aimed at preserving physiological reserve before coronary angioplasty (Steinmetz et al., 2023).
Prolonged bedrest in acute cardiac patients is associated with heightened sympathetic nervous system activity, reduced parasympathetic tone, endothelial dysfunction and rapid cardiovascular deconditioning. Even short durations of sedentary behaviour can exacerbate catecholamine release, impair baroreflex sensitivity and reduce endothelial shear stress, increasing susceptibility to arrhythmias and adverse cardiac events (Lavie et al., 2019; Mastrandrea et al., 2024). By contrast, light-to-moderate ambulation promotes autonomic balance by attenuating sympathetic overactivity and enhancing vagal tone, which may contribute to improved haemodynamic stability and lower cardiac event burden (Man et al., 2020; Munir et al., 2020
EA may also benefit vascular endothelial function. Mobilisation increases pulsatile blood flow and shear stress, stimulating nitric oxide release and improving endothelial responsiveness (Man et al., 2020). This effect is particularly relevant in NSTEMI patients awaiting coronary angioplasty, where endothelial dysfunction and plaque instability are central to ongoing myocardial risk.
From a prehabilitation perspective, EA supports maintenance of functional capacity and counters rapid inpatient deconditioning. Even low intensity ambulation preserves skeletal muscle activation, optimises metabolic efficiency and maintains cardiopulmonary reserve. Enhancing functional reserve prior to coronary intervention may facilitate faster post-procedural recovery, earlier discharge readiness and improved tolerance of subsequent rehabilitation phases (Steinmetz et al., 2023).
Taken together, these mechanisms provide a biologically plausible explanation for the reduced cardiac events and shorter hospitalisation observed in the EA group. Although causal pathways cannot be definitively established within the current study design, these findings support EA as a nursing-led prehabilitation strategy that counteracts sedentary-induced deconditioning and enhances cardiovascular stability in the pre-procedural setting.
Reduction in hospitalisation duration and role of beta-blockers
Building on the physiological benefits of EA including improved autonomic balance, preserved endothelial function and maintained functional reserve, EA may have facilitated faster recovery and earlier readiness for discharge. Consistent with this, the EA group experienced a significantly shorter hospital stay (100.08 hours vs 149.64 hours, mean difference = 49.56 hours, p = 0.02). This reduction highlights the clinical advantages of integrating EA into NSTEMI care as shorter hospitalisations can improve haemodynamic recovery, enhance functional capacity, reduce hospital-associated complications and enhance long-term cardiovascular outcomes (Asgari et al., 2015; Semsar-Kazerooni et al., 2021; Zhang et al., 2018).
As part of guideline-directed medical therapy for NSTEMI, beta-blockers are recommended to improve cardiovascular stability by reducing HR, lowering myocardial oxygen consumption and enhancing cardiac contractility. They are also associated with reduced mortality and recurrent ischaemia (Amsterdam et al., 2014; Byrne et al., 2023; Kennedy, 2018). In this study, beta-blockers were routinely administered, reflecting standard of care, and were independently associated with shorter hospital stay (B = −6247.11, p = 0.002).
Beta-blocker use and EA were analysed as independent contributors in the regression model. EA may complement recovery alongside pharmacological therapy by promoting circulation, preserving muscle strength (Okada et al., 2019) and supporting functional recovery (Asgari et al., 2015; Semsar-Kazerooni et al., 2021; Zhang et al., 2018). Synergistic effects between EA and beta-blockers were not formally evaluated, and no conclusions regarding interaction can be drawn. Combined with standard pharmacotherapy, EA likely complements treatment to optimise both functional and cardiovascular stability, contributing to improved patient outcomes (Amsterdam et al., 2014; Kennedy, 2018).
Although the regression model explained 18% of the variance in length of stay (Adjusted R2 = 8%), these results underscore EA’s potential to shorten recovery time and complement standard pharmacotherapy in NSTEMI management.
Clinical and healthcare implications
The combination of EA’s physiological benefits and its association with shorter hospitalisation highlights its potential to optimise NSTEMI care at both the patient and system levels. Implementing structured EA protocols could alleviate strain on hospital resources by enabling earlier discharge, reducing demands on continuous monitoring, medical interventions and bed utilisation (Johnson et al., 2023; Stone et al., 2022). The nearly 2 days (49.56 hours) reduction observed highlights improved hospital capacity utilisation, with potential downstream cost savings for healthcare providers, particularly in high-volume acute cardiac units (Johnson et al., 2023; Stone et al., 2022).
Beyond clinical efficiency, EA provides important psychosocial benefits. Prolonged hospitalisation is associated with increased psychological stress, anxiety and loss of independence. EA fosters a sense of normalcy and self-efficacy, which are essential for mental well-being and recovery (Asgari et al., 2015; Zhang et al., 2018). Maintaining mobility also reduces the risk of hospital-acquired infections and complications, enhancing overall patient outcomes. By preserving functional independence and supporting engagement in ADLs, EA contributes to smoother transitions to post-discharge care and subsequent rehabilitation phases (Asgari et al., 2015; Semsar-Kazerooni et al., 2021; Zhang et al., 2018).
From a system perspective, EA demonstrates that nursing-led, structured interventions can achieve tangible improvements in both patient recovery and healthcare efficiency. Successful integration relies on structured delivery processes, ward-wide training, pre-ambulation assessments and adherence to standardised checklists, which ensure patient safety and protocol fidelity. These findings highlight the capacity of nurses to drive evidence-based change and establish scalable models of care that enhance both clinical outcomes and operational efficiency.
Feasibility and integration into routine care
The study demonstrates that EA can be reliably operationalised within routine ward practice. Nurses successfully integrated the intervention into standard workflows through structured delivery processes. Pre-ambulation vital sign assessments, application of trigger criteria and documentation using a standardised checklist ensured consistent and accountable implementation of the mobility protocol. Ambulation sessions were delivered at the protocol-defined light-to-moderate intensity level. Nursing compliance exceeded 99% of prescribed ambulation sessions, and no ambulation-related adverse events occurred across 77 participants.
Brief ward-wide training on trigger parameters and escalation pathways further facilitated successful adoption and supported a shift away from traditional CRIB practices towards a mobility-promoting ward culture. The observed reduction in cardiac events and hospital length of stay reflects downstream benefits directly linked to consistent nursing delivery of EA, effectively closing the theory to practice loop.
The beneficial effects of EA may also be understood through a broader theoretical lens that recognises how supportive interventions can paradoxically become stressors when poorly structured or insufficiently monitored. Analogous findings from high stress environments suggest that well-intentioned support may heightened physiological or psychological strain when underlying stressors remain unresolved (Aqtam et al., 2025). In the context of NSTEMI care, this framework helps explain why protocol-driven, nurse-monitored EA provides controlled physiological loading that mitigates cardiovascular stress, whereas unstructured activity or prolonged immobilisation may exacerbate sympathetic activation and deconditioning. The structured implementation approach used in this study–characterised by clear trigger criteria, continuous monitoring and standardised documentation–ensured that EA functioned as therapeutic support rather than an additional stressor.
Strengths and limitations
This study achieved strong participation across two cardiac wards, with an adequate sample size that met the required statistical power. The nurse-led design ensured strong protocol adherence and reflects real-world clinical practice, enhancing its clinical relevance.
However, several limitations should be acknowledged. The absence of long-term follow-up data, including readmissions and mortality, limits the ability to determine the durability of benefits. Outcome assessors were unblinded, introducing potential measurement bias. Conducting the study within a single institution may limit generalisability. Additionally, because EA was delivered alongside existing ward-based care bundles, there is a possibility of intervention conflation, making it difficult to isolate the independent effect of EA from background practices.
Implications
Targeted nurse education should enhance knowledge and confidence in EA protocols, whereas integration of EA into routine nursing practice can promote patient safety and recovery. At the service and policy level, standardised protocols and institutional support can facilitate consistent delivery across wards. Future research is recommended through multicentre randomised controlled trial with larger samples, long-term clinical and patient-reported outcomes and cost-effectiveness analyses to guide wider implementation and evidence-based policy.
Conclusion
This study provides robust evidence supporting the efficacy and safety of EA in NSTEMI patients before coronary angioplasty. By reducing cardiac events and hospitalisation duration without compromising haemodynamic stability, EA offers a promising strategy for improving patient outcomes and advancing acute cardiac care. These findings align with the study’s objectives to evaluate the feasibility and benefits of EA, addressing a critical gap in EA practices in NSTEMI patients.
As nursing plays a pivotal role in ambulation protocols, this research reinforces the profession’s contribution to evidence-based cardiovascular care. Implementing structured ambulation protocols could enhance nursing-led interventions and optimise resource utilisation. It also offers the potential for meaningful cost savings through reduced length of stay and more efficient use of inpatient resources, while improving patient recovery trajectories. Future studies should focus on refining ambulation guidelines, addressing implementation barriers and evaluating long-term clinical, patient-reported and economic outcomes to ensure that EA can be sustainably integrated into routine clinical practice.
Key points for policy, practice and research
EA is safe and effective: This study provides strong evidence that EA before coronary angioplasty significantly reduces cardiac events and hospital length of stay without compromising haemodynamic stability in NSTEMI patients.
Enhancing nursing-led ambulation protocols: The findings reinforce the critical role of nursing in promoting EA in acute cardiac settings. Structured EA protocols should be incorporated into standard nursing practice to improve patient recovery outcomes.
Potential for policy integration: Given the benefits observed, EA should be considered for broader implementation in hospital protocols, aligning with international trends emphasising EA in cardiac care.
Need for further research: Future studies should explore the long-term effects of EA including its impact on rehospitalisation rates, quality of life and cost-effectiveness to strengthen its justification for widespread adoption.
Supplemental Material
sj-pdf-1-jrn-10.1177_17449871261421460 – Supplemental material for Early ambulation before percutaneous coronary intervention in patients with non-ST elevation myocardial infarction: a quasi-experimental study of haemodynamics and clinical outcomes
Supplemental material, sj-pdf-1-jrn-10.1177_17449871261421460 for Early ambulation before percutaneous coronary intervention in patients with non-ST elevation myocardial infarction: a quasi-experimental study of haemodynamics and clinical outcomes by Jolyn Si Ying Chin, Choy Yee Lee, Tee Joo Yeo, Poh Chi Tho, Wilson Wai San Tam and Wenru Wang in Journal of Research in Nursing
Footnotes
Acknowledgements
The authors gratefully acknowledge the support and contributions of Dr Siti Zubaidah, ADON Doreen Chew Mei Leng, Dr Goh Mien Li, SNC Oon Siow Eng, NM Thangam Thomas, Physiotherapist Candice Wee and the nurses of Ward A and Ward B. The authors also acknowledge the Nursing innovation, Clinical inquiry, Enabling Research (NiCER) award for enabling and supporting the conduct of this study. RN Liew Qian Wen and RN Phua Jueying are acknowledged for their active involvement in data collection.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the National Healthcare Group Domain Specific Review Board (DSRB No: 2022/00529).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.