
Abstract
Background:
There is limited evidence comparing differences in pain experienced during ventrogluteal (VG) muscular injections between the standing and lying-down positions. This study aims to compare pain and complications during VG injection (VGI) in standing versus lying positions in women.
Methods:
The study utilised a quasi-experimental design, a sample size (n = 48), a crossover design and a 2-week interval between injections. The first VG intramuscular injection (IMI) site was administered according to the patient’s preference for position. After the IMIs, the patients’ pain and complication levels were assessed. Descriptive statistics and odds were used to evaluate the data. The level of significance was set at p < 0.05.
Results:
A paired design was used to compute the difference in visual analogue scale (VAS) scores in standing and lying positions. The difference between the mean pain in the standing position and lying position was −0.76 with CI = (−1.24, −0.27) and p-value = 0.0012, indicating a significant pain decrease in the standing position with odds = 3.67 and 95% CI (1.64, 8.25). The mean VAS scores (standing: 1.10; lying: 1.86) were obtained for the clinical context.
Conclusions:
This research suggests that the standing position may be a method for administering VGIs to reduce patient-perceived pain.
Introduction
Healthcare professionals worldwide administer approximately 12 billion intramuscular injections (IMIs) each year, making it one of the most common methods of drug administration (Polania Gutierrez and Munakomi, 2025). This is a fundamental nursing skill used to deliver medication deeply into the muscle (Strohfus, 2025). IMI is often preferred when the drug’s absorption rate is too slow via subcutaneous administration or too rapid via the intravenous (IV) route (Erstad and Barletta, 2022). It can also be employed when the absorption of oral medication is poor (Baish et al., 2022) to help ensure treatment adherence (Baryakova et al., 2023). For instance, older adults are at risk of B vitamin deficiency due to age-related changes in the gastrointestinal tract and insufficient dietary intake (Mouchaileh, 2023). The standard treatment for vitamin B deficiency involves administering B-complex vitamins via IMI (Sarwar and Sarwar, 2022). However, these injections can be painful, and there are potential injection-related side effects such as sciatic nerve injury, infections, bruising, abscesses, necrosis, hematoma, ecchymosis, pain and injuries to blood vessels and nerves (Gokkus et al., 2024). Leakage of the injection solution (drug leakage) and/or bleeding (blood leakage) from the injection site onto the skin occurs. Injection side effects lead to noncompliance with many treatment modalities (Kim et al., 2022).
Several studies have examined the factors that influence successful IMI outcomes. Physical characteristics such as the patient’s sex, subcutaneous fat and muscle thickness (Lau, 2024), body mass index (BMI), body shape, nurse’s skills and the size of syringes and needles appear to be impact factors (Kim et al., 2022). The risk of IMI failure was high in obese and underweight individuals; for those underweight, there was a risk of bone contact with the IMI (Kaya et al., 2023). In such cases, the patient might face complications such as fractures, breaks, infection and tissue damage (Pettyjohn et al., 2022). Nurses often prefer the ventrogluteal (VG) site for injections due to its safety, low risk of sciatic nerve injury, accessibility and lower pain levels (Lau, 2024).
Patients can be positioned in supine, prone, lateral or standing positions (Nicoll and Hesby, 2002). Nurses should consider the selection of a patient’s position based on factors such as muscle relaxation, individual patient needs, medical conditions and specific procedural requirements(Abdelkhalek, 2019). Research has shown that patients in the prone position during ventrogluteal intramuscular injection (VGIMI) experience less pain and discomfort compared to those in the lateral position (Potter et al., 2025).
Nurses have limited evidence on pain levels and patient compliance when VGIMI is administered in a standing position, whereas there has been an increase in requests for standing injections in clinical outpatient settings during the COVID-19 pandemic. Patients have learned from health education on social media that there is a lower risk of infection if their contact with the bed, sheets and other clinical devices decreases. This helps break the chain of transmission (Open Resources for and Reuter-Sandquist, 2022).
This complicates the decision-making process for both nurses and patients regarding the VGIMI site. Despite nurses frequently receiving requests for upright injections, no studies have directly compared pain and complications between standing and lying positions for VGI. Therefore, conducting a study to compare pain levels and complications associated with VGIMI in standing versus lying-down positions can offer valuable scientific evidence to assist clinical nurses in making informed decisions during the injection process.
Objective
This study aims to compare the pain and complications associated with VGIMI in the standing versus lying-down positions.
Methods
Study design and participants
The study utilised a quasi-experimental design. The participants were selected through convenience sampling from the outpatient clinic at a Comprehensive Health Care Centre. The research population consisted of clients referred to the Comprehensive Health Services Centre between August 2020 and September 2023 who had a physician’s order for two doses of IMIs of the B-complex, comprising 48 females. The first VGIMI was performed according to the patient’s preference for position (either a standing position or lying down, to reduce their anxiety and build patient trust). The second injection is administered to alternate legs. This study was not blinded and was a single-group procedure. Two injection positions were performed in a self-controlled manner, eliminating differences that may arise from individuals.
The patients were required to meet the following inclusion criteria: (1) female, aged between 49 to 60 years, (2) having no cognitive-perceptive problem, (3) having a physician’s prescription for only a B-complex ampule by the IM route, (4) being at the beginning of treatment, (5) having no inconvenience for applying different lying or standing positions, (6) having a BMI of normal weight based on the World Health Organization classification, (8) having had no IMI at the Dorso–Gluteal (DG) or VG site in the last 6 months and (9) having no scar, buttock pain, no musculoskeletal imbalances, etc.(for diagnosis and to reduce flowing complication of current injection).
The sample size was calculated using the formula: n = 2(z1 − α/2 + z1 − β)2 σ2/d2 to detect a 20% difference in pain scores with 80% power and a 5% significance level, factoring in a potential 10% dropout rate. Here, d = 1 and σ = 1.66 and n = 55. Initially, 55 patients were recruited for the study. The data were analysed using R programming, with the significance level set at p < 0.05 (Nicoll and Hesby, 2002).
Two individuals were excluded for not meeting the inclusion criteria (n = 2). One person declined to participate (n = 1), and two were lost to follow-up (n = 2), with one of them not answering the phone (n = 1). Another patient chose to seek treatment at a closer clinic instead. During the second phase, one participant believed that a single dose of B-complex was enough (n = 1), whereas another thought that B-complex was ineffective (n = 1). In the end, 48 patients completed the study (Figure 1).
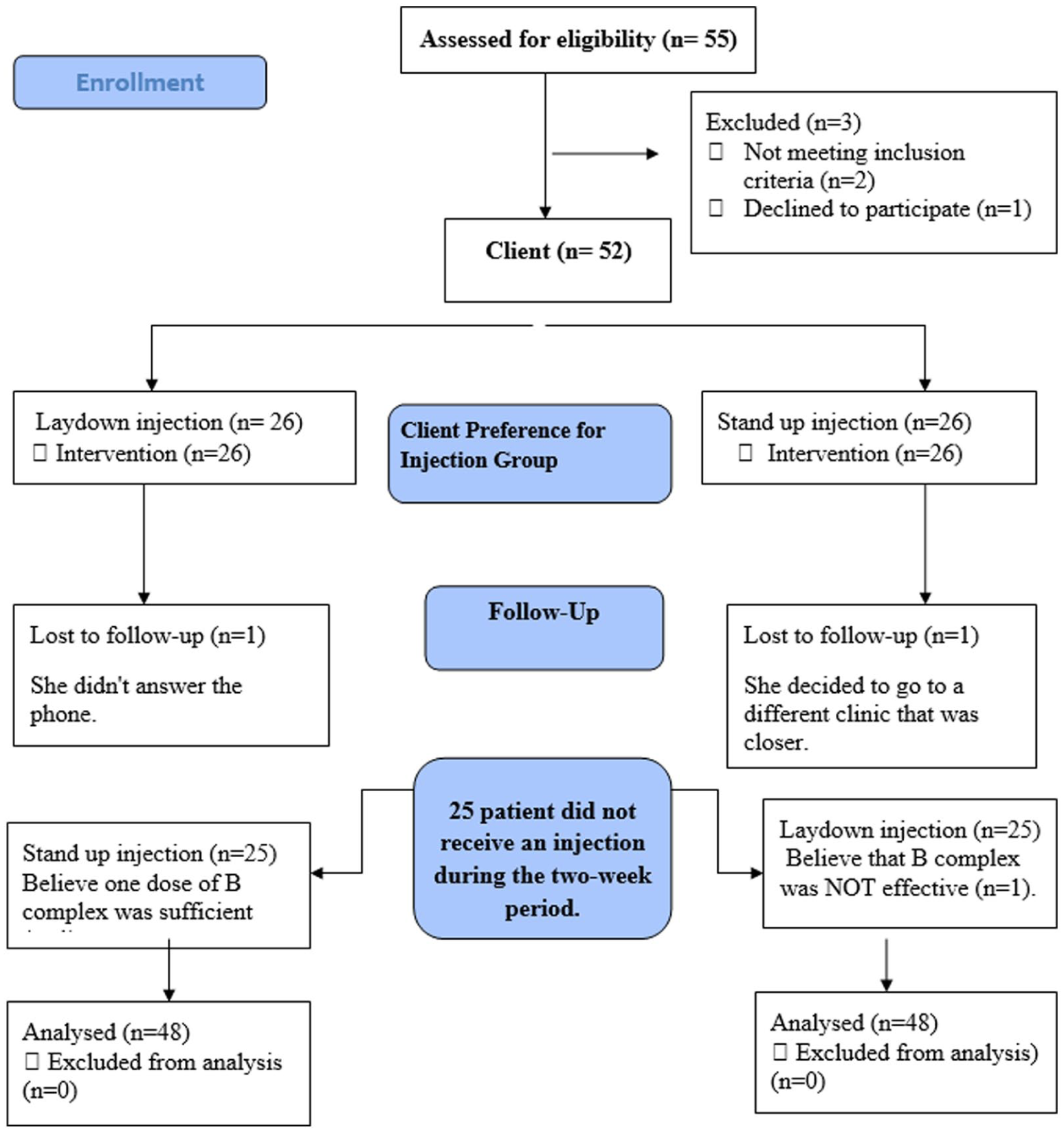
Flowchart of the study design.
Software and implementation
All analyses were conducted using R, a widely used open-source software in biostatistics and medical research (R Core Team, 2023). The confidence intervals and p-values were computed using the Bootstrap method since sample sizes are relatively small and the Visual Analogue Scale (VAS) distribution is skewed.
VG injection
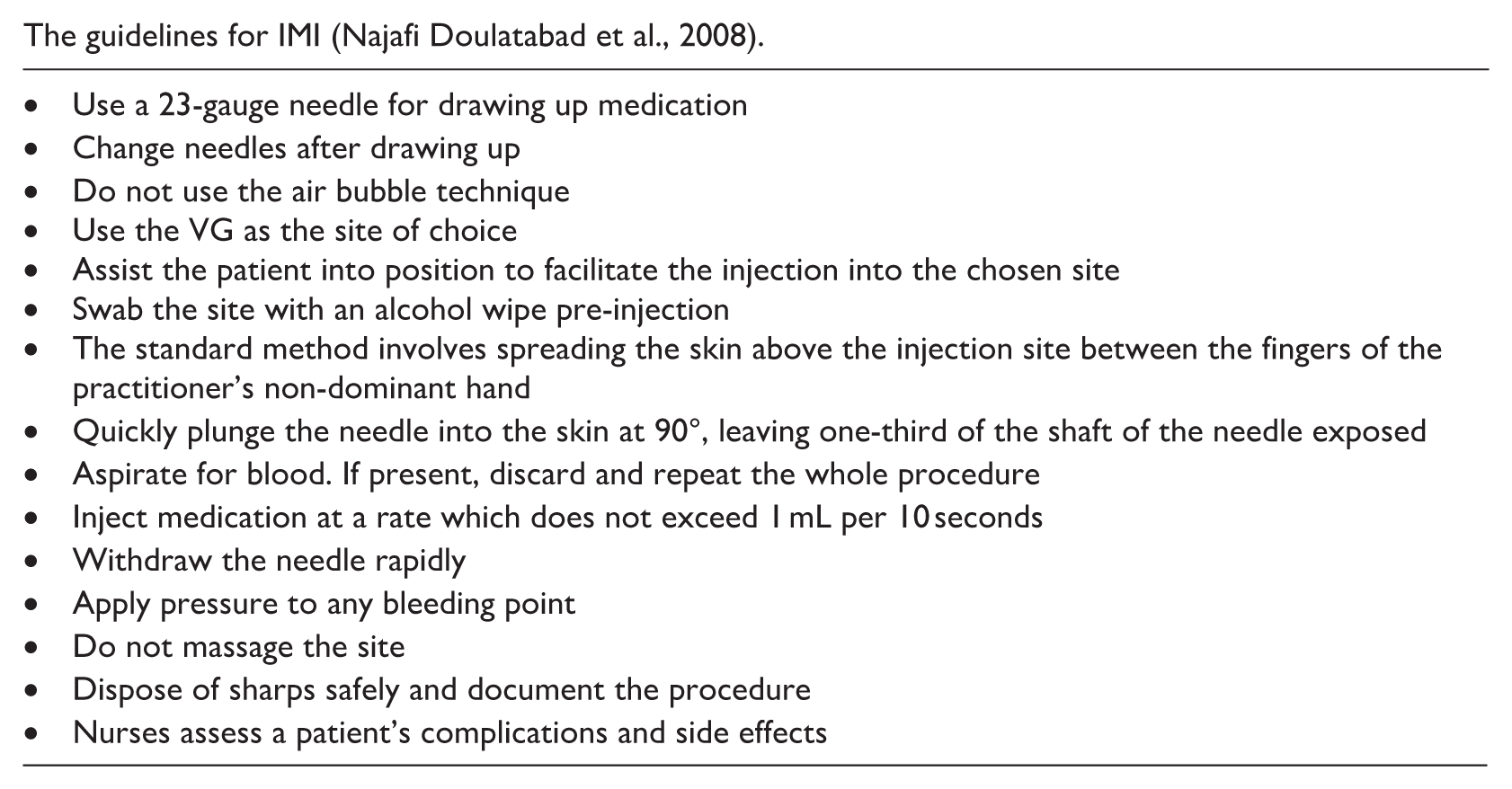
The nursing staff administered both standing and lateral (lying down) injections to each client at a 2-week interval in the same room, using standard methods. The room was equipped with an emergency trolley, and a doctor was present and informed about the research being conducted. One section of the room was designated for IMIs, featuring a handle mounted on the wall 1 m above the ground for patients to hold on to. The nurse positioned the patient vertically for IMIs, with a soft mat on the floor and a nearby chair for the patient to sit in if needed. When administering injections in a lying-down position, the patient was positioned on their lateral side with the knee bent for the injection (Nicoll and Hesby, 2002). Table 1 provides comprehensive technical details of the injection procedure, including the needle gauge (23) and length (25 mm), as well as the drug volume (2cc; Najafi Doulatabad et al., 2008). The injection technique followed standard protocols, and the needle was replaced after drawing up the medication. All injections were administered by a nurse with 3 years of professional experience. She directly follows up on adverse events through phone calls to effectively address any complications.
The guidelines for IMI (Najafi Doulatabad et al., 2008).
Data collection
The VG site was utilised for all injections. Each client received two B-complex injections, with a 2-week interval.
Study instruments
The data were collected using a self-administered questionnaire and a checklist. The questionnaire included sections on age, sex and BMI, as well as a 10 cm VAS to measure perceived pain intensity during VGIMI. The VAS score ranged from 0 (no pain) to 10 cm (extreme pain). After each injection, the subjects rated the pain intensity at the injection site by marking a point on the VAS. Researchers designed a checklist based on the method proposed by Burian et al. (2018) to assess injection complications of VG. The checklist includes a straightforward YES or NO scoring system: Test–retest reliability, standard error of measurement (SEM), minimal detectable change (MDC) for the VAS. After each injection, another investigator immediately assessed pain intensity using the VAS.
The intraclass correlation coefficient (ICC) reliably measures reproducibility, but it is affected by sample heterogeneity. Conversely, the SEM provides a more practical and reliable indicator, assisting in calculating the MDC (Alghadir et al., 2018). However, there are no studies examining the SEM and MDC for the VAS in relation to injection pain. Alghadir et al. (2018) researched the test–retest reliability, validity and minimum detectable change of VAS for assessing osteoarthritic knee pain. Their results indicated minimal measurement error (SEM = 0.03) and (MDC = 0.08), with an ICC of 0.97. The significance level was set at p < 0.05, with a 95% confidence interval (Alghadir et al., 2018). In the current study, we assessed the ICC = 0.93, minimal measurement error (SEM = 0.021) and (MDC = 0.05 cm).
Published MCID values for VAS in hip osteoarthritis range from 0.3 to 1.1 cm (Olaiya et al., 2025).
Ethical considerations
Participants were provided with written information about the study requirements and gave their consent before participating, following approval from the Review Board of the University of Medical Sciences. This study is reported in line with The Transparent Reporting of Evaluations with Non-randomised Designs reporting guidelines (TREND) (Des Jarlais et al., 2004).
Results
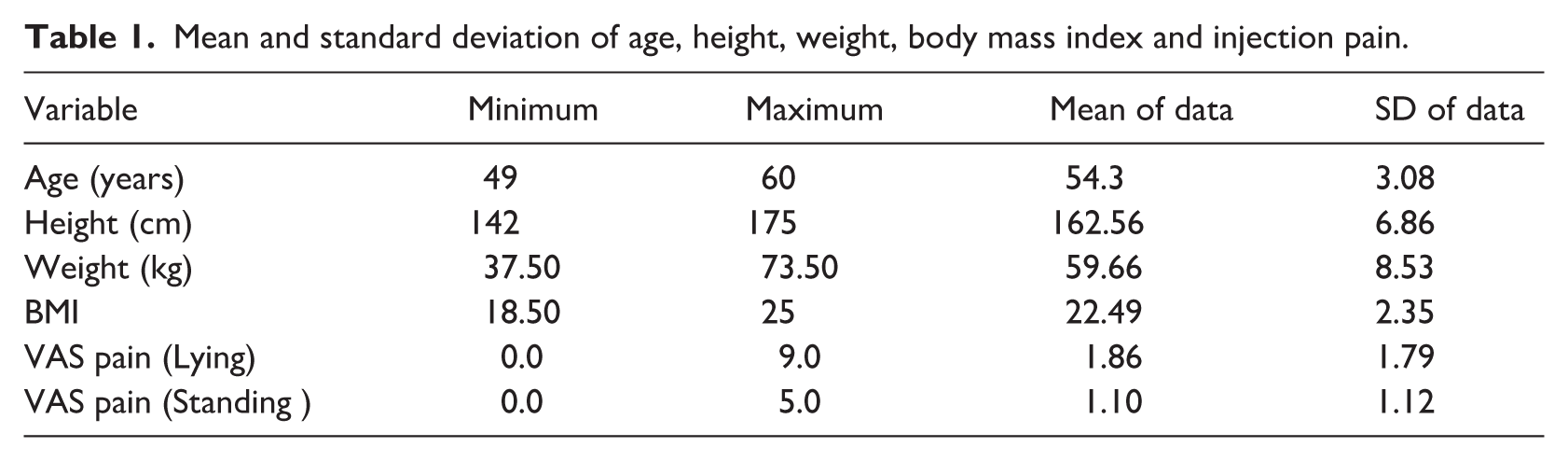
In total, 48 female clients were included in the study, 43 (89%) of them were married and 5 (11%) were single. Three (6.2%) were illiterate, 14 (29.1%) had an under diploma degree, 17 (35.4%) had a diploma, 1 (2%) had a post-diploma, 9 (18.7%) had a bachelor’s degree and 4 (8.3%) had a master’s degree. In terms of occupation, 5 (10.4%) were employees, 8 (16.6%) were self-employed and 35 (72.9%) were stay-at-home mothers. The minimum, maximum and average age, height, weight, BMI and injection pain in the standing and lying-down positions are displayed in Table 1.
Mean and standard deviation of age, height, weight, body mass index and injection pain.
The results show that the frequency of blood leakage complications after IMI in the standing position was six patients versus six patients in the lying-down position. Use of McNamar’s test shows that there was no significant difference in the frequency of drug leakage complications between the standing position (two patients) and the lying-down position (two patients; Table 2). No fainting, bruising, abscess or nerve damage was observed in any of the samples when assessing other injection complications.
Comparison of the frequency of side effects of VGI (blood leakage and drug leakage) in standing and lying-down positions in the study samples.
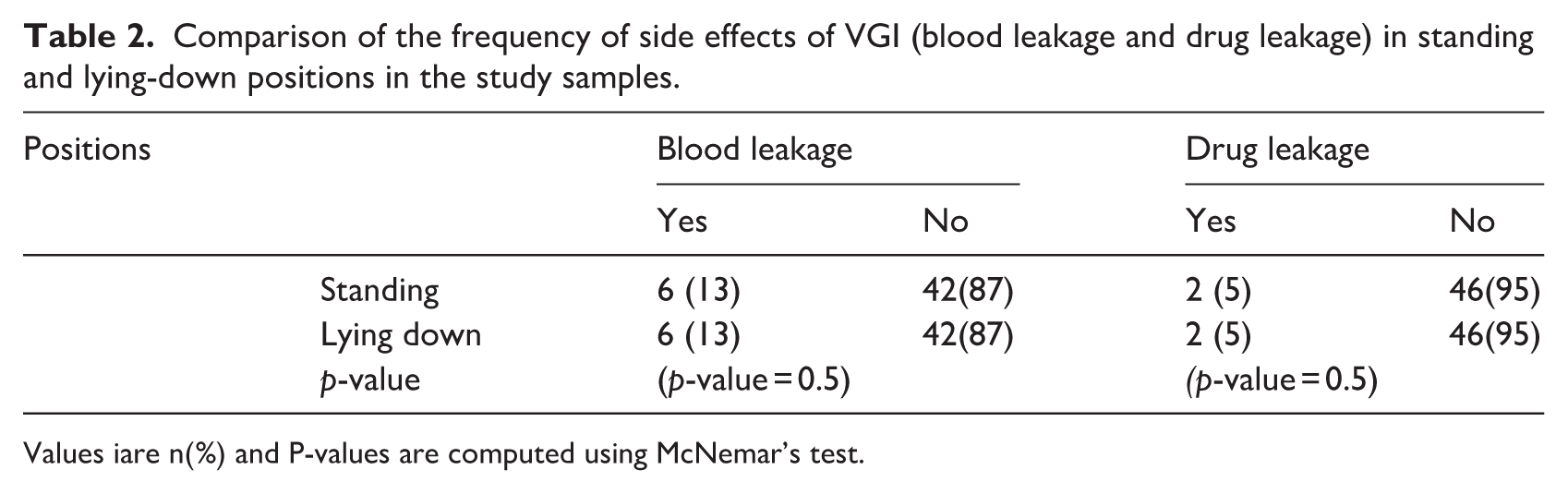
Values iare n(%) and P-values are computed using McNemar’s test.
This study compares VAS pain scores for injections administered in standing versus lying positions using a dataset of 48 patients with 2 observations each (standing and lying). Boxplots and bar plots revealed a median VAS difference of −1, indicating lower pain in the standing position for most patients (Figure 2).
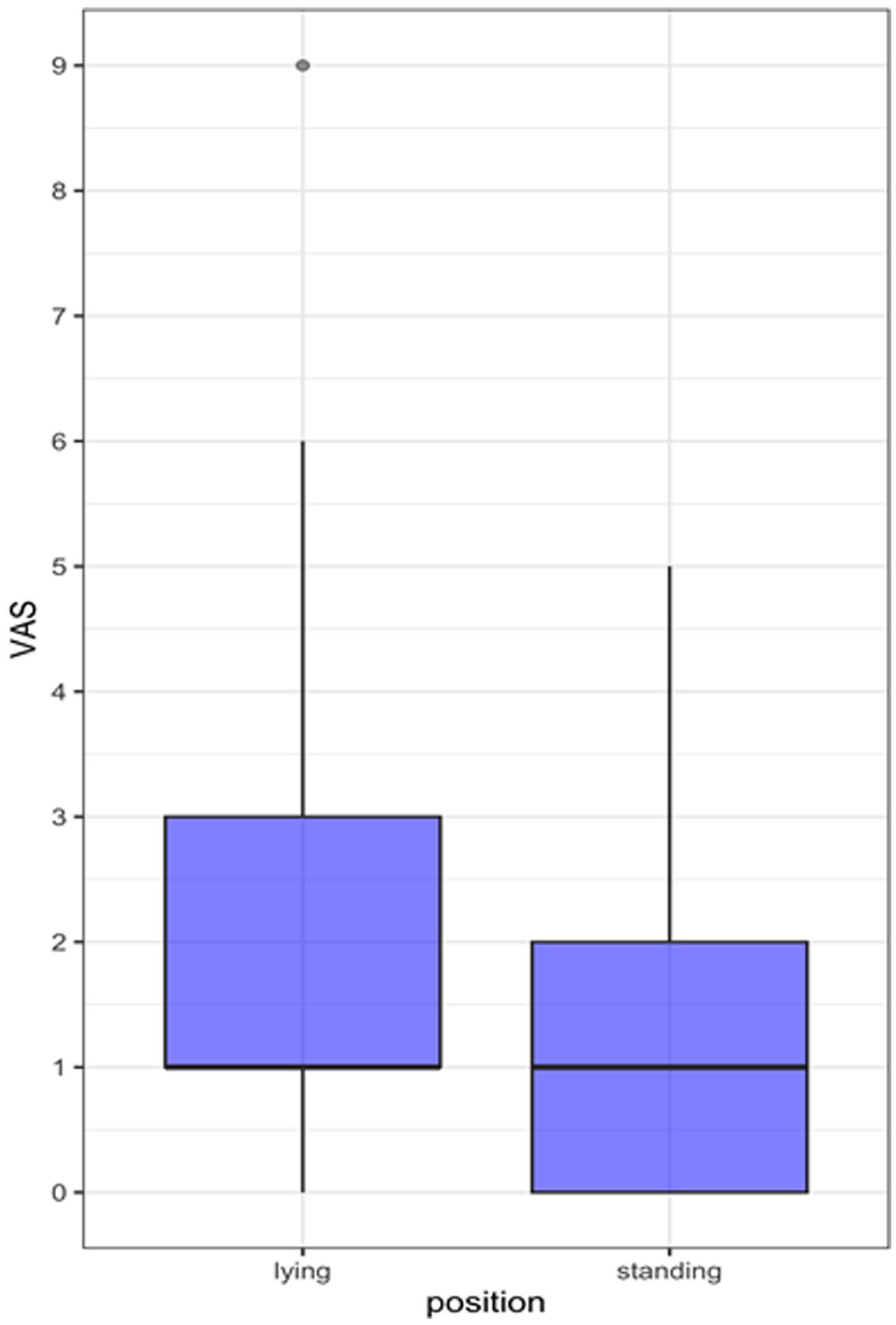
The pain intensity of VGI in the standing and lying-down positions is shown.
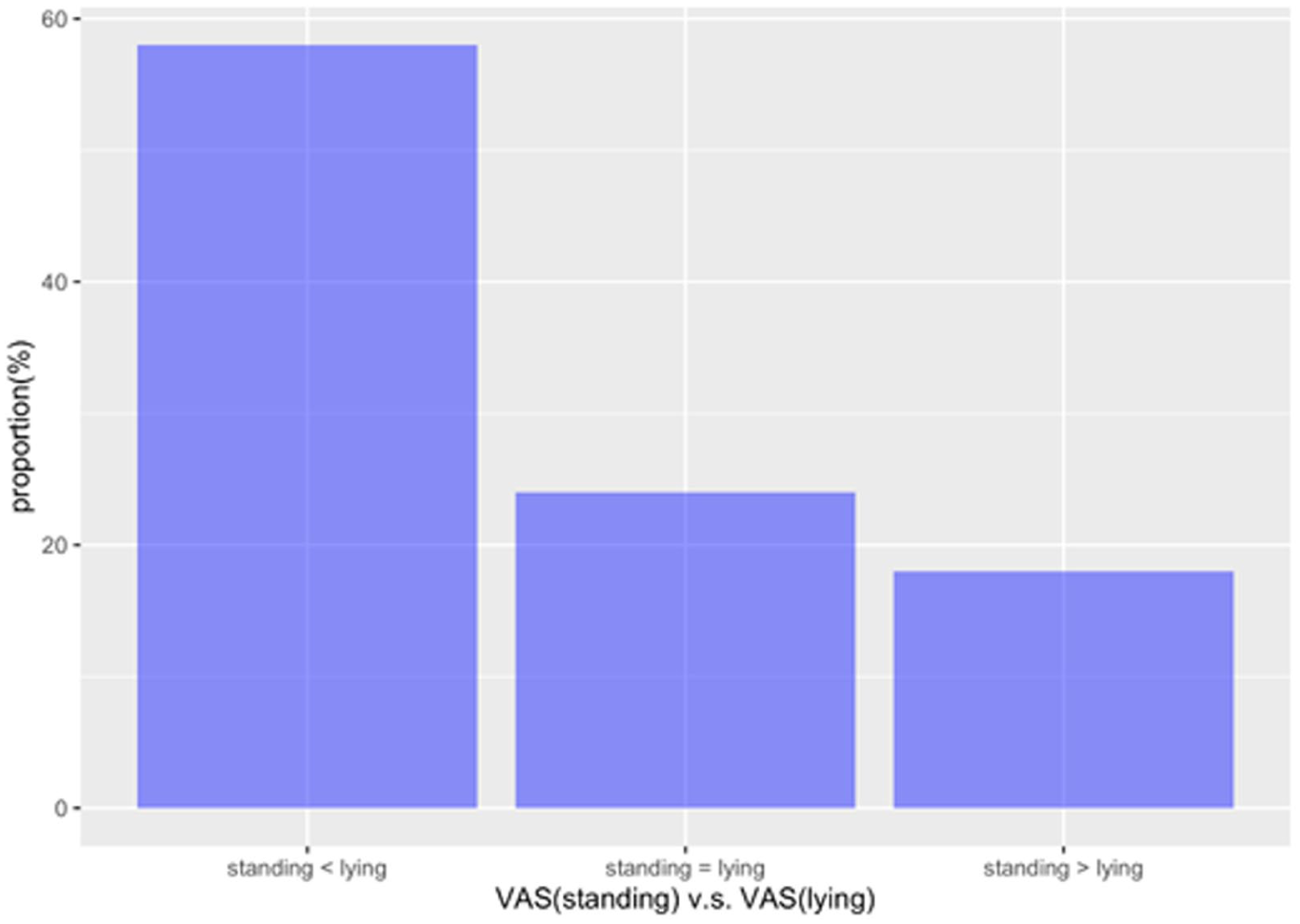
There are three probabilities: P1, the pain of standing is equal to lying; P2, pain of standing is less than lying; P3, pain of standing is greater than lying. We are interested in: – Odds of (standing pain is less) on (standing pain is greater) = P2/P3.
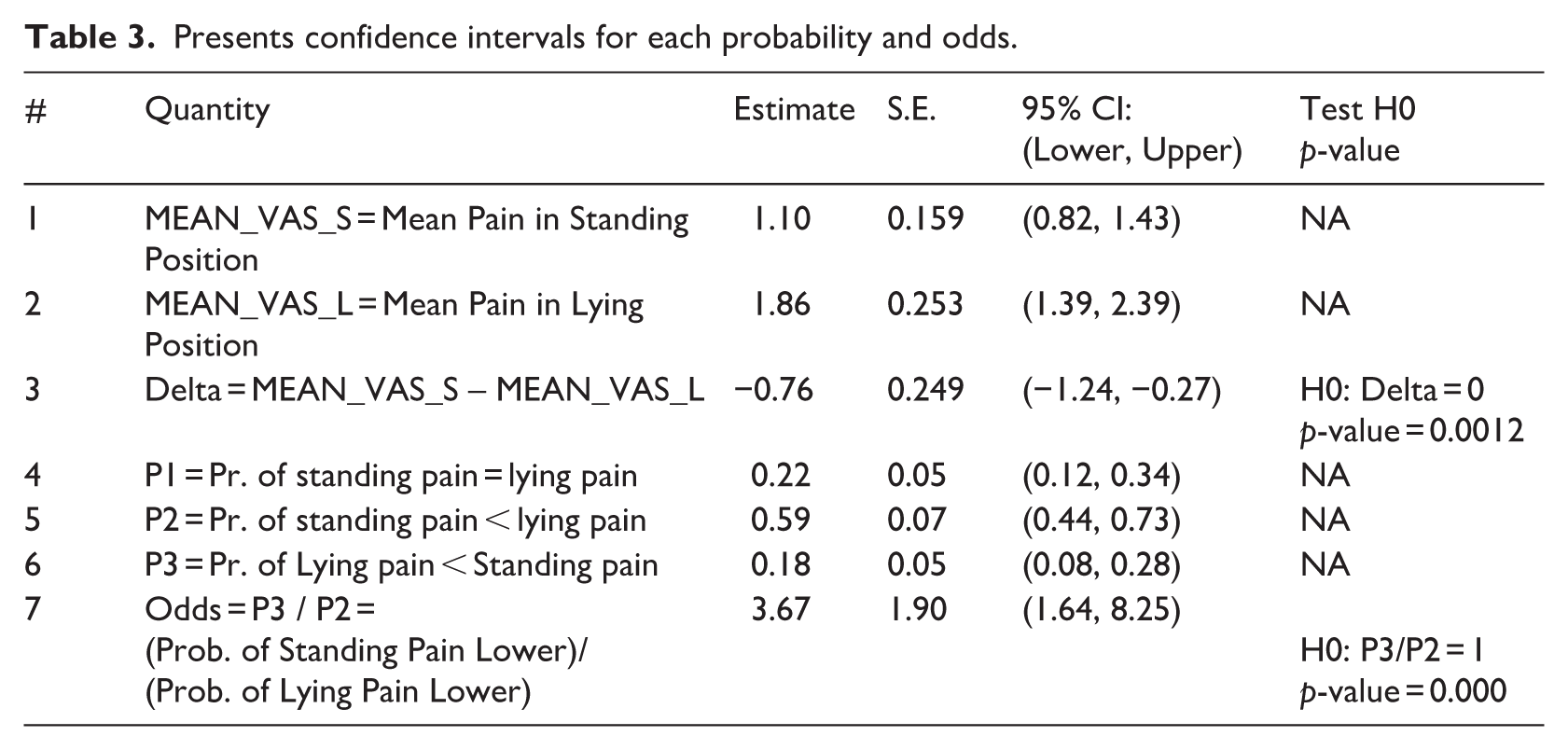
The difference between the mean pain in the standing position and lying position was −0.76 with CI = (−1.24, −0.27) and p-value = 0.0012, indicating a significant pain decrease in the standing position (see Table 3). Moreover, to better help nurses and patients in decision-making, we studied three probabilistic outcomes (Figure 3): Probability of standing pain < lying pain (58%), Probability standing pain = lying pain (24%) or Probability of standing pain > lying pain (18%). This study suggests that the probability of patient pain during the standing position is lower than during the lying position for VGI, with odds = 3.67 and 95% CI = (1.64, 8.25) with p-value of 0.0003 as shown in Table 3.
Presents confidence intervals for each probability and odds.
Discussion
This is a quasi-experimental study comparing pain levels and complications related to VGIMI in standing versus lying positions among women attending comprehensive health services for IMIs.
Nurses are responsible for administering painless IMIs in the Comprehensive Health Service. The proper technique, selection of equipment (including needle size and syringe), patient characteristics and injection skill and method are important to minimise pain and complications. These variables were controlled in this research to ensure the validity and reliability of the study. Some research has indicated that the position of the injection site is important in the level of the patient’s pain.
In this study, all participants were women. Research suggests that there is a difference in subcutaneous tissue thickness between males and females, with a greater thickness suggesting that women may experience greater pain because they have more fatty tissue in their hips, whereas males have thicker fatty tissue in their abdominal area (Strohfus et al., 2022).
Menopausal females aged were chosen as participants in this study for two reasons. Firstly, physicians had prescribed B-complex to alleviate their specific menopausal symptoms by supporting nervous system function (Guan et al., 2025). Second, a study by Tuğrul and Khorshid (2014) found a statistically significant negative relationship between age and pain intensity after an IMI (Tuğrul and Khorshıd, 2014). In this study, participants ranged in age from 49 to 60. No significant relation was found between their average age and reported pain levels. Since the sample was homogeneous in terms of age, it appears that age does not significantly influence the results. However, it is important to recognise that age could still be a potential limitation when analysing the findings.
Our findings showed that the mean pain intensity in clients during VGI in the standing position was 1.10 with CI = (0.82, 1.43). The mean pain intensity associated with lying down was 1.86 with CI = (1.39, 2.39). The difference between the mean pain in the standing position and lying position was −0.76 with CI = (−1.24, −0.27) and p-value = 0.0012, indicating a significant pain decrease in the standing position. This outcome is similar to the results of Sarıkaynak and Büyükyilmaz (2023) study. They assessed how different lying positions (prone and lateral) affect regional pain and comfort during IM drug administration. The findings showed that the average pain intensity after IMI in the prone position was lower than in the lateral position (4.12 ± 1.67 vs 5.22 ± 1.91, a difference of 1.1 ± 0.24 units), with very high statistical significance (p < 0.01).
The difference observed in Sarıkaynak et al.’s study (1.1 units) between the prone and lateral positions was greater than in the current study, which compared the standing and lateral positions (0.76 units). According to Olaiya et al. (2025), previous studies have also indicated that the Minimal Clinically Important Difference (MCID) is 0.3 cm for long-term nonspecific pain populations (Olaiya et al., 2025). Therefore, it can be concluded that, in this study, 0.76 units for acute and specific pain are acceptable. And the standing position results in less pain than the prone position.
The study by Kara and Yapucu Güneş (2016) showed that injection position is more effective than injection technique in reducing pain during VGI (Kara and Yapucu Güneş, 2016). According to a 2015 review, children reported decreased fear of receiving vaccines when standing compared to when lying down (Taddio et al., 2015).
Standing may lead to central hypovolemia and increase activity in the hypothalamic–pituitary–adrenal axis (HPA), resulting in elevated levels of hormones such as endorphins and cortisol (Hennig et al., 2000). Endorphins, known as natural happiness hormones, are effective in diminishing pain perception. Additionally, cortisol plays a role in reducing inflammation, further contributing to a decrease in pain perception while standing(Chaudhry and Rahimi, 2025).
In addition, the study showed that some patients experienced complications, such as drug leakage and blood leakage, after VGI. However, there were no statistically significant differences in complications between the standing and lying positions in this study. Najafi Dolatabad et al. (2010) demonstrated that the air-locking technique produced less drug leakage and ecchymosis than the Z-track injection technique. The injection technique modifications impact the frequency of bruising and drug leakage at the injection site (Kara and Yapucu Güneş, 2016), focused on blood leakage, drug leakage and bruising after changes in the injection technique and area of injection, rather than the patient’s position (Ayinde et al., 2021). The injection technique used in this study was consistent across all the samples. However, a comparison with the findings of other studies suggested that the injection technique can affect drug and blood leakage rates and the probability of bruising. Despite changing positions, the rates of drug leakage, blood leakage and bruising remain unaffected. It is essential to keep this in mind as a successful research outcome.
The hypothesis is that larger volumes in VGIMI cause more pain at the injection site. This pain likely comes from increased tissue pressure, stretching or irritation from the large volume (St Clair-Jones et al., 2020). When the injection is administered while the patient is standing, the solution tends to move downward through the muscle under the influence of gravity (Woodley et al., 2022). Gravity can have dramatic effects on the fluid balance in the limb (Baish et al., 2022). As a result, the area under the needle has a lower volume of solution, which leads to decreased pressure and less pain perception, and the rates of drug leakage, blood leakage and bruising remain unaffected.
Strengths and limitations
The strengths of this study include an appropriate design, rigorous analysis, practical results and a low dropout rate. However, this study has certain demographic limitations, such as age, sex, occupation (specifically, stay-at-home women) and BMI, which may not accurately represent a diverse population. We determined the order of positions based on patient preference rather than through randomisation, which raises concerns about potential selection bias. Therefore, caution is needed when generalising these findings.
Implications
This study provides evidence supporting the administration of VGIMI to patients in a standing position in nursing curriculum and practice. Administering injections while standing can reduce pain and enhance the quality of care. This method also saves time and reduces costs by eliminating the need to change bed sheets for each patient and minimising patient exposure to contaminated air in medical facilities. The standing VGIMI technique is especially beneficial in emergencies such as floods, earthquakes or conflicts, where resources are limited, and many individuals require urgent attention. Further research is needed to compare pain and complication rates associated with VGIMI across positions, including standing, prone and lateral. This research should include a diverse population, encompassing both men and individuals from various age groups.
Moreover, this study did not evaluate patient satisfaction or preferences after the injection. Therefore, it is recommended to conduct a post-procedure study to assess these factors. This study suggests that larger randomised controlled trials are needed to bolster the evidence for the use of VGIMI in routine practice. Further investigation is also essential to fully comprehend hormonal changes and the impact of gravity on perceived pain.
Conclusions
The data indicated that patients experienced less pain during IMIs when standing compared to lying down. Additionally, no significant differences in injection complications were observed between the standing and lying-down positions. Nurses may consider allowing patients to stand for VGIMI upon request or when circumstances warrant. Furthermore, nurses can enhance their understanding of this subject by conducting further research and integrating the use of standing positions for IMI into standard nursing practices.
Key points for policy, practice and research
Nurses commonly employ IMI for drug administration.
Traditionally, this procedure has been performed with the patient in a lying-down position.
Research indicates that there is no significant difference in pain experienced during VGIs when administered in a standing position versus lying down.
This study presents evidence for nurses to consider administering injections while the patient is standing in clinical settings.
The findings demonstrate that this approach results in lower pain levels and similar complication rates compared to the lying-down position.
Footnotes
Acknowledgements
The authors would like to express their special thanks and gratitude to all the people who cooperated in performing this research and the relevant officials.
Author contributions
Data availability
The datasets used and analysed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The ethics committees approved the study (IR.RUMS.REC.1399.233). All participants received an explanation of the study before participating. Informed consent was obtained from all participants. Patients were informed about voluntary participation and the right to withdraw from the study at any time. To ensure confidentiality, any identifying information of the participants was removed and numbered identifiers were used. It was emphasised to enrolees in the practicum course that there were no disadvantages in withdrawing from the study.
Consent for publication
By submitting this document, the authors declare consent for the final accepted version of the manuscript to be considered for publication.