
Abstract
Background:
Children with complex chronic conditions (CCCs) frequently revisit emergency departments (EDs), increasing demand on acute services and challenging care coordination.
Aims:
To identify clinical and family factors associated with higher ED utilisation in children with CCCs and to characterise frequent service use (FSU).
Methods:
Retrospective longitudinal cohort at a tertiary hospital in Spain (2015–2021). We included 248 children <18 years with CCCs (Feudtner v2), regardless of ED use. Recurrent ED visits were modelled using a Cox Andersen–Gill approach from discharge of the index ED visit. Global FSU was described as ⩾8 ED visits during 2015–2021.
Results:
Overall, 240/248 (96.8%) children attended the ED (mean 13.0 visits; median 8, IQR 4–18). Higher hazards of ED revisits were associated with non-malignant CCC macro-groups, rehabilitation enrolment, higher urgent and scheduled hospitalisation counts and any PICU admission (C-index ≈ 0.71).
Conclusion:
Routinely recorded factors may support risk stratification and coordinated follow-up for children with CCCs. Contribution to nursing: This study strengthens nursing knowledge on continuity and family-centred complex care by identifying clinically relevant risk profiles in a tertiary-care cohort. Multicentre validation and prospective evaluation are needed before specific service models can be recommended.
Keywords
Introduction
Paediatric emergency care for children with complex chronic conditions (CCCs) has received increasing attention because these children account for high resource use and costs and experience substantial impacts on health and quality of life (Agrawal et al., 2016). Children with CCCs typically share four core features: chronic multisystem disease, functional limitations, high healthcare utilisation and substantial caregiving needs (Berry et al., 2013).
CCCs are associated with prolonged hospitalisations (Cohen et al., 2018), paediatric intensive care unit (PICU) admissions and frequent emergency department (ED) visits (Hudson et al., 2014). In the United States, 9%–14% of children meet definitions of frequent service use (FSU), commonly operationalised as 4–6 ED visits per year (Giannouchos et al., 2021).
From a nursing and health policy perspective, frequent ED use is a priority because it may signal unmet needs in continuity of care and care coordination across hospital and community services. The decision of when and where to seek emergency care reflects not only illness instability but also system and family context. Key influences include access to timely, high-quality outpatient care (Montalbano et al., 2017), caregiver self-efficacy, community and family resources (Berry et al., 2017; O’Mahony et al., 2013) and socio-demographic factors that shape care-seeking directly or indirectly (e.g. via access barriers and parents’ perceived severity; Pehlivanturk-Kizilkan et al., 2022). Accordingly, patterns of FSU may reflect not only clinical severity but also gaps in outpatient management and coordination, contributing to potentially avoidable use of urgent services (Giannouchos et al., 2021; Montalbano et al., 2017). These mechanisms are directly relevant to nursing practice because discharge preparation, caregiver education, anticipatory guidance (including device troubleshooting and symptom action plans) and post-discharge follow-up are nurse-sensitive processes that can be designed and evaluated to reduce preventable revisits.
Identifying children at higher risk of FSU is therefore essential to inform targeted, nurse-led interventions and service planning that optimise ED care and strengthen post-discharge coordination for children with CCCs (Joseph et al., 2022). However, although age, chronic illness burden and comorbidities have been associated with frequent ED use (Thind et al., 2022; Vrijlandt et al., 2022), few externally validated prediction models are available to identify children with CCCs at risk of FSU. Moreover, much of the evidence comes from health systems without universal access or strong primary-care gatekeeping, or from social and cultural contexts that differ from Spain (Samuels-Kalow et al., 2020; Thind et al., 2022). Evidence from tax-funded systems with universal coverage is needed to support nursing pathways and policy decisions that aim to improve continuity and reduce potentially avoidable ED utilisation.
Aim
The aim of this study was to identify clinical and socio-demographic factors associated with higher ED utilisation among children with CCCs and to describe profiles of FSU.
Methods
Study design
We conducted a retrospective longitudinal cohort study at a tertiary referral hospital in Spain (tax-funded national health system) from 2015 to 2021, reported in accordance with Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (von Elm et al., 2007). This study builds on prior cross-sectional work describing healthcare utilisation in children with CCCs (Pérez-Ardanaz et al., 2019).
Study setting and sampling
Eligible participants were children <18 years with CCCs classified using Feudtner’s CCC v2 system (Feudtner et al., 2014). This retrospective cohort included all eligible children receiving care at the study hospital during 2015–2021 and therefore reflects a consecutive real-world tertiary-care sample rather than a sample selected to detect a single prespecified effect size.
Inclusion and exclusion criteria
We included children with CCCs who received care at the hospital between 2015 and 2021, regardless of ED utilisation. Because follow-up spanned multiple years, some participants were older than 18 years during observation; they were retained if they continued to receive paediatric or shared-care services. The selection flowchart is provided in Supplemental File 1.
Data collection
Data were retrospectively extracted from electronic medical records by a single investigator using prespecified study definitions and coding rules based on the study protocol. Variables included CCC category, comorbidities, technology dependence, inpatient admissions, paediatric intensive care unit (PICU) admissions, outpatient visits, surgical procedures, length of stay, therapeutic effort limitation (TEL; treatment-limitation orders), mortality, time since diagnosis, transplantation and SARS-CoV-2 infection. Participation in rehabilitation and paediatric palliative care (PPC; implemented locally in 2018) was also recorded. Healthcare utilisation metrics were derived both annually and across the full observation window.
For analytic parsimony, Feudtner categories were collapsed a priori into three mutually exclusive macro-groups reflecting clinical similarity: (1) congenital–genetic–neurologic, (2) malignancy and (3) acquired/other organ-system CCCs (e.g. cardiac, respiratory, gastrointestinal/hepatic, renal/urologic, endocrine/metabolic and haematologic/immunologic). When a child mapped to more than one Feudtner category, a single macro-group was assigned using a prespecified hierarchy (malignancy > congenital–genetic–neurologic > acquired/other) for person-level analyses.
Outcome definitions
Global FSU was defined as ⩾8 total ED visits during 2015–2021 (vs 0–7), corresponding to the cohort median. For descriptive sensitivity summaries, alternative global cut-offs (⩾6 and ⩾10 total ED visits) were examined (Furia et al., 2023; Giannouchos et al., 2021; Greenfield et al., 2021). For year-specific summaries only, annual ED use was categorized as 0–1 versus ⩾2 visits per calendar year; this annual categorization was not used in time-to-event models.
Ethical considerations
This study used data from clinical records and did not involve direct data collection from children or their families. The ethics committee of Granada considered it exempt from the need for additional informed consent and confirmed the validity of the previous study approval (No. 0655-N-16). Data were handled in de-identified form in accordance with applicable data-protection regulations.
Data analysis
Descriptive statistics were used to summarise the sample. Continuous variables are reported as mean (Standard Deviation [SD]) or median (Interquartile Range [IQR]), as appropriate.
FSU (global) comparisons: Patients were classified by global FSU status based on total ED visits accumulated over 2015–2021 (0–7 vs ⩾8). Clinical, socio-demographic and utilisation variables were compared between FSU groups using independent-samples t-tests for continuous variables (with Levene’s correction when appropriate) and χ2 tests for categorical variables. When assumptions were not met, Mann–Whitney U-test and Fisher’s exact test were used. Effect sizes (Cramér’s V; standardised mean differences/Hedges’ g) and denominators are reported in table footnotes. Where applicable, p-values were adjusted for multiple comparisons using the Benjamini–Hochberg false discovery rate (FDR) within prespecified test families.
Figure analyses: Year-specific utilisation patterns were summarised using repeated-measures General Linear Models (GLMs) with Greenhouse–Geisser correction when needed. Prespecified contrasts versus 2015 were reported for each outcome. Associations between global FSU status and continuous/count variables were explored using point-biserial Pearson and Spearman correlations, respectively (two-sided α = 0.05; FDR-adjusted, where applicable).
Recurrent-event analysis: Recurrent ED visits were modelled using a Cox proportional hazards model in the counting-process (Andersen–Gill) formulation. The event was any ED visit, and the time scale was days since discharge from the index ED visit. Risk intervals restarted after each ED visit and ended at the earliest of 365 days, death, transfer outside the care network or loss to follow-up. Hazard ratios (HRs) are reported with 95% confidence intervals (CIs) and the C-index; ties were handled using the Efron method. Proportional-hazards assumptions were assessed using Schoenfeld residuals and log–log plots. For descriptive, unadjusted contrasts, time to first ED revisit was compared across baseline groups using log-rank tests. Robust (sandwich) standard errors clustered by patients were used to account for within-child correlation of recurrent events.
No post hoc power analyses were conducted. Exact two-sided p-values and 95% CIs are reported where appropriate. For the recurrent-event Cox model, performance is summarised using the C-index, likelihood-ratio χ2 and a likelihood-ratio-based pseudo-R2. All tests were two-sided with α = 0.05. Analyses were conducted in IBM SPSS Statistics, Version 25.0. (SPSS Inc, 2017)
Results
Sample characteristics
The cohort included 248 children; 56.0% (n = 139) of them were female, and the median age was 13 years (Interquartile Range: IQR 9.3–17.0). The most common CCC categories were congenital/genetic (39.5%, n = 98), neurologic (20.2%, n = 50) and malignancy (15.7%, n = 39).
The median number of comorbidities was 2 (IQR 1.0–3.0). The mean time since diagnosis was 8 years; the median was 7 years (IQR 6.0–13.0).
ED visits
During follow-up, 96.8% (n = 240) of children attended the ED, with a mean of 13.0 visits (SD 13.34) and a median of 8.0 visits (IQR 4.0–18.0). The annual mean number of ED visits decreased from 2.5 (SD 3.5) in 2015 to 1.1 (SD 2.1) in 2021. Table 1 presents the clinical and socio-demographic factors between the group with 0–7 emergency visits (42.3%, n = 105) and the group with 8 or more visits (57.7%, n = 143).
Baseline characteristics by global frequent service use (FSU) (⩾8 vs 0–7 ED visits, 2015–2021).
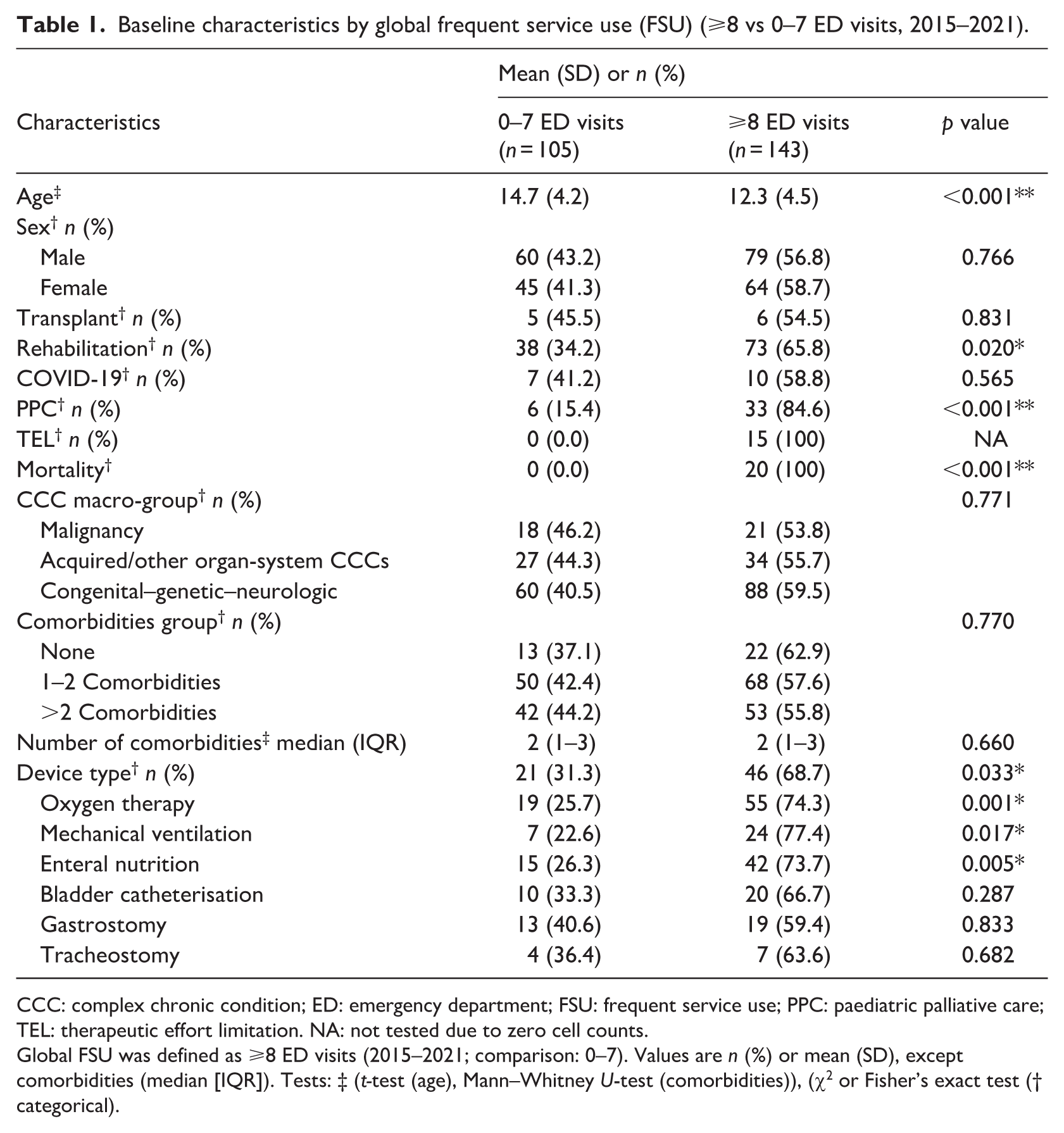
CCC: complex chronic condition; ED: emergency department; FSU: frequent service use; PPC: paediatric palliative care; TEL: therapeutic effort limitation. NA: not tested due to zero cell counts.
Global FSU was defined as ⩾8 ED visits (2015–2021; comparison: 0–7). Values are n (%) or mean (SD), except comorbidities (median [IQR]). Tests: ‡ (t-test (age), Mann–Whitney U-test (comorbidities)), (χ2 or Fisher’s exact test († categorical).
Children with fewer ED visits had a longer time since diagnosis (mean difference 1.9 years; 95% CI 0.8–3.0; t (219.7) = 3.51; p ⩽ .001). The number of comorbidities was not significantly associated with global FSU (Spearman ρ = 0.088; p = 0.203), whereas child age was inversely correlated with FSU status (point-biserial (r = −0.30; p < 0.001) see Table 1).
Parental socio-demographic factors
Parents of children with ⩾8 ED visits were younger (fathers: mean difference 2.3 years, 95% CI 0.3–4.3, p = 0.025; mothers: mean difference 2.2 years, 95% CI 0.4–4.1, p = 0.017). There were no significant between-group differences in parental occupational status or educational level (fathers: χ2 = 3.10, p = 0.377; mothers: χ2 = 3.42, p = 0.332).
Healthcare utilisation
During 2015–2021, year-specific comparisons by global FSU group (0–7 vs ⩾8 total ED visits over the observation window) showed significant differences in several years, most consistently for urgent hospitalisations, outpatient visits, hospital days and total healthcare contacts. By contrast, day-hospital use and PICU days showed small and inconsistent differences over time and scheduled (elective) hospitalisations rarely differed by FSU group. For selected categorical outcomes (e.g. PICU admission within a given year), differences emerged in some years but did not show a stable pattern. Full estimates with 95% CIs and exact p-values (FDR-adjusted where applicable) are reported in Supplemental Table S1.
Urgent hospitalisations were more frequent in the ⩾8-visit group (mean difference −0.3; 95% CI −0.5 to −0.2; p < 0.001; overall year effect F (42, 877.9) = 33.70; p < 0.001). Scheduled hospitalisations were slightly higher in the 0–7 group (mean difference 0.1; 95% CI −0.0 to 0.3; p = 0.143). During 2015–2021, global tests indicated significant variation over time (F (3, 469.4) = 10.45; p < 0.001).
Outpatient visits, hospital days, PICU days and total healthcare contacts were higher in the ⩾8-visit group, with statistically significant differences (consultations: mean difference −2.6; 95% CI −4.7 to −0.5; p = 0.016; F (4, 840.1) = 9.32; p < 0.001; hospital days: mean difference −2.0; 95% CI −3.5 to −0.4; p = 0.012; F (2.5, 514.1) = 27.10; p < 0.001; PICU days: mean difference −0.5; 95% CI −0.9 to −0.1; p = 0.015; F (3, 647.4) = 6.19; p < 0.001; total contacts: mean difference −4.4; 95% CI −7.1 to −1.8; p = 0.001; F (3.6, 726.7) = 23.57; p < 0.001).
Clinical factors
ED visit frequency was higher among children in the congenital–genetic–neurologic macro-group than among those with malignancy (mean difference 1.0; 95% CI 0.0–2.0; p = 0.039). At the global level, the overall between-year comparison (2015–2021) did not reach statistical significance (omnibus p ⩾ 0.05). However, in prespecified pairwise contrasts versus 2015, lower values were observed in 2020 and 2021 within the congenital–genetic–neurologic group, and similar decreases were seen in the acquired/other group. Panel-wise p-values are shown in Figure 1; pairwise contrasts should be interpreted as exploratory given the non-significant omnibus test and multiple testing.
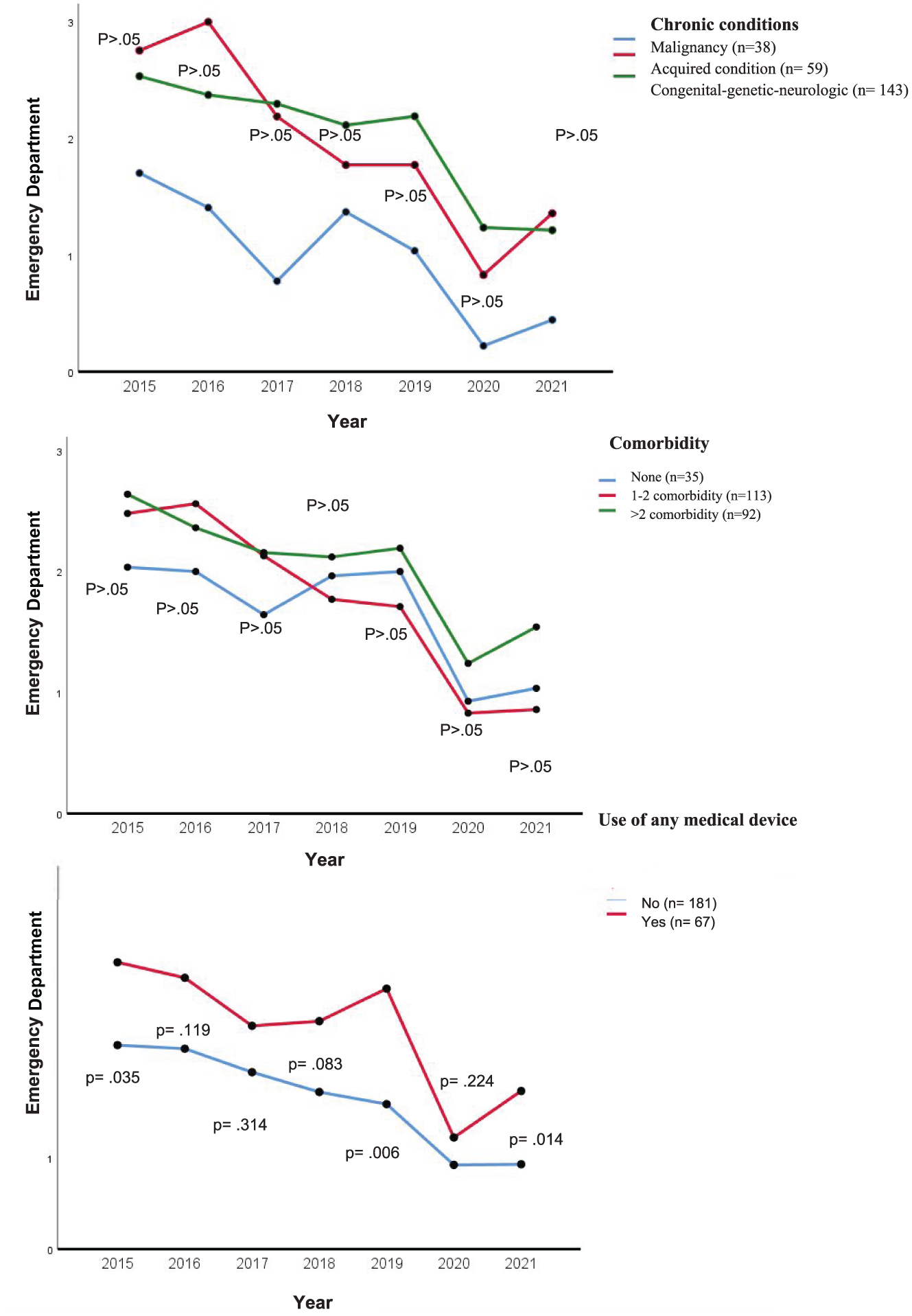
Emergency visits according to clinical factors during 2015–2021.
Regarding comorbidity burden, the mean number of ED visits was 1.68 (95% CI 0.9–2.3) for children with no comorbidities, 1.76 (95% CI 1.4–2.1) for those with 1–2 comorbidities and 2.00 (95% CI 1.62–2.40) for those with >2 comorbidities. Differences over the follow-up period were statistically significant (F(9, 934.3) = 9.55; p < 0.001). The largest decreases occurred in 2020 and 2021 compared with 2016 within the 1–2 comorbidity group (Figure 1).
Children with any medical device had more ED visits than those without device dependence (mean difference 0.7; 95% CI 0.1–1.32; p = 0.009), with a significant year effect (F(4.5, 933.7) = 13.20; p < 0.001). The largest decreases were observed in 2020 versus 2015 and 2016 (Figure 1).
Device-specific panels showed a similar pattern (Figure 2). Children receiving oxygen therapy had more ED visits than those without oxygen therapy (mean difference 0.9; 95% CI 0.3–1.5; p = 0.002; year effect F(4.5, 936.0) = 12.66; p < 0.001). Mechanical ventilation was also associated with higher utilisation (mean difference 1.88; 95% CI 0.2–1.9; p = 0.011; F(4.5, 933.5) = 7.52; p < 0.001), as was enteral nutrition (mean difference 1.1; 95% CI 0.5–1.7; p = 0.003; F(4.5, 934.2) = 12.58; p < 0.001). For bladder catheterisation, gastrostomy and tracheostomy, between-group differences were not statistically significant (all p ⩾ 0.05), although year effects were detected. Panel-wise exact p-values (FDR-adjusted) are shown in Figure 2 and refer to within-panel comparisons only.
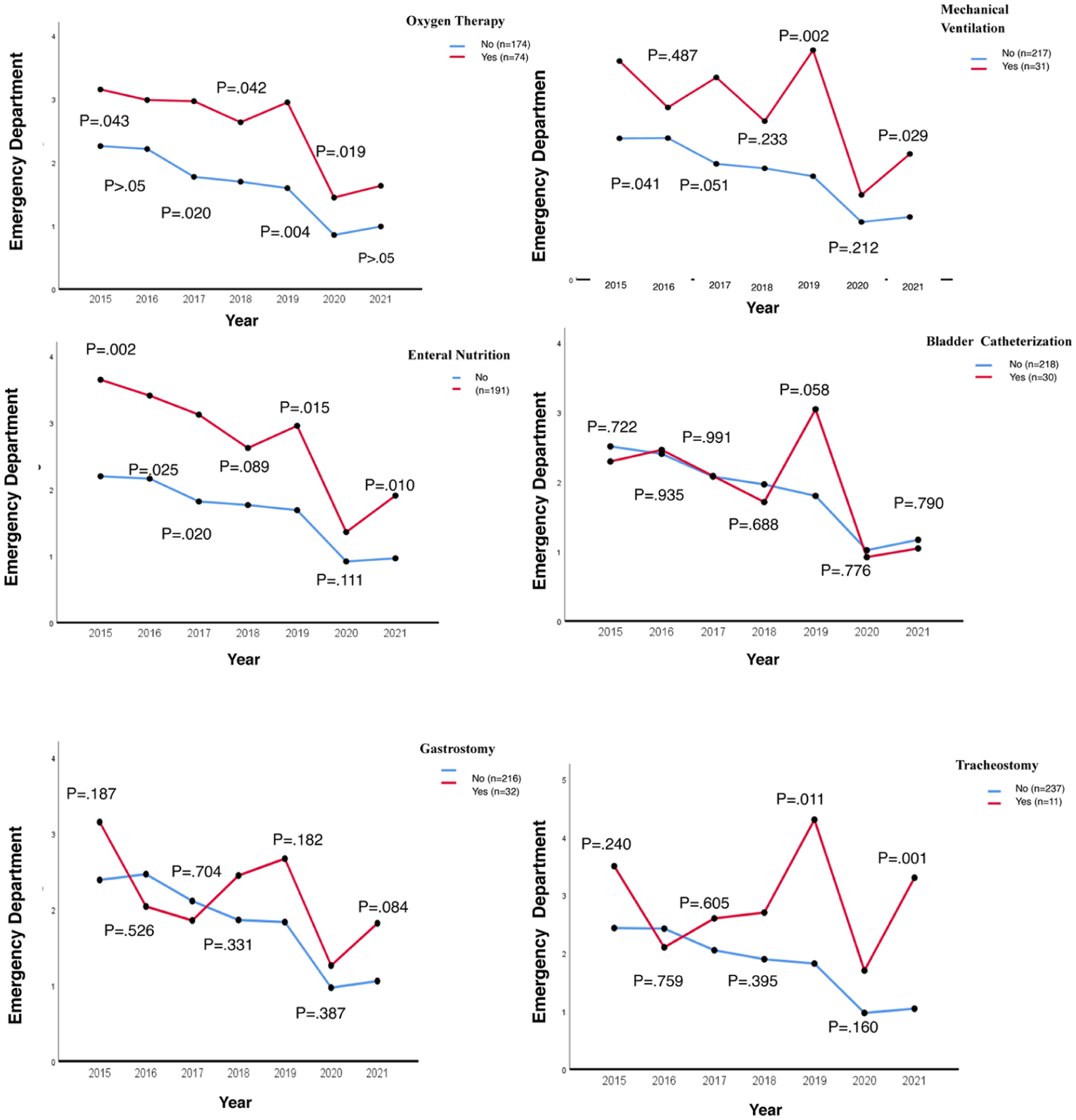
Legend: Y-axis: annual mean ED visits per patient (visits per patient-year), linear scale. Points/bars show the mean with 95% CIs. Per-panel n indicates the number of unique patients contributing to that year/group. Panel tests derive from a repeated-measures GLM (Year 2015–2021 as the within-subject factor; device status for the panel—yes/no—as the between-subject factor), with Greenhouse–Geisser correction when sphericity was violated and estimated marginal means for prespecified pairwise contrasts vs 2015. Exact p-values (FDR-adjusted) are shown within panels and refer to within-panel comparisons only; no cross-panel inference is implied.
Multivariate analysis
In the recurrent-event Cox model (Andersen–Gill), the event was any ED visit. Overall, 919 ED visits were observed. In the Andersen–Gill model, compared with malignancy, the hazard of an ED revisit was higher for acquired/other CCCs (adjusted HR 1.75; p < 0.001) and for the congenital–genetic–neurologic macro-group (adjusted HR 1.51; p < 0.001). Additional factors associated with a higher hazard of ED revisits included rehabilitation enrolment (adjusted HR 1.50; p < 0.001), higher counts of urgent (adjusted HR 1.40; p < 0.001) and scheduled hospitalisations (adjusted HR 1.06; p = 0.002) and any PICU admission (adjusted HR 4.52; p < 0.001). Model discrimination was acceptable (C-index 0.71; SE 0.010; Table 2).
Recurrent-event Cox model (Andersen–Gill): univariable and multivariable HRs.
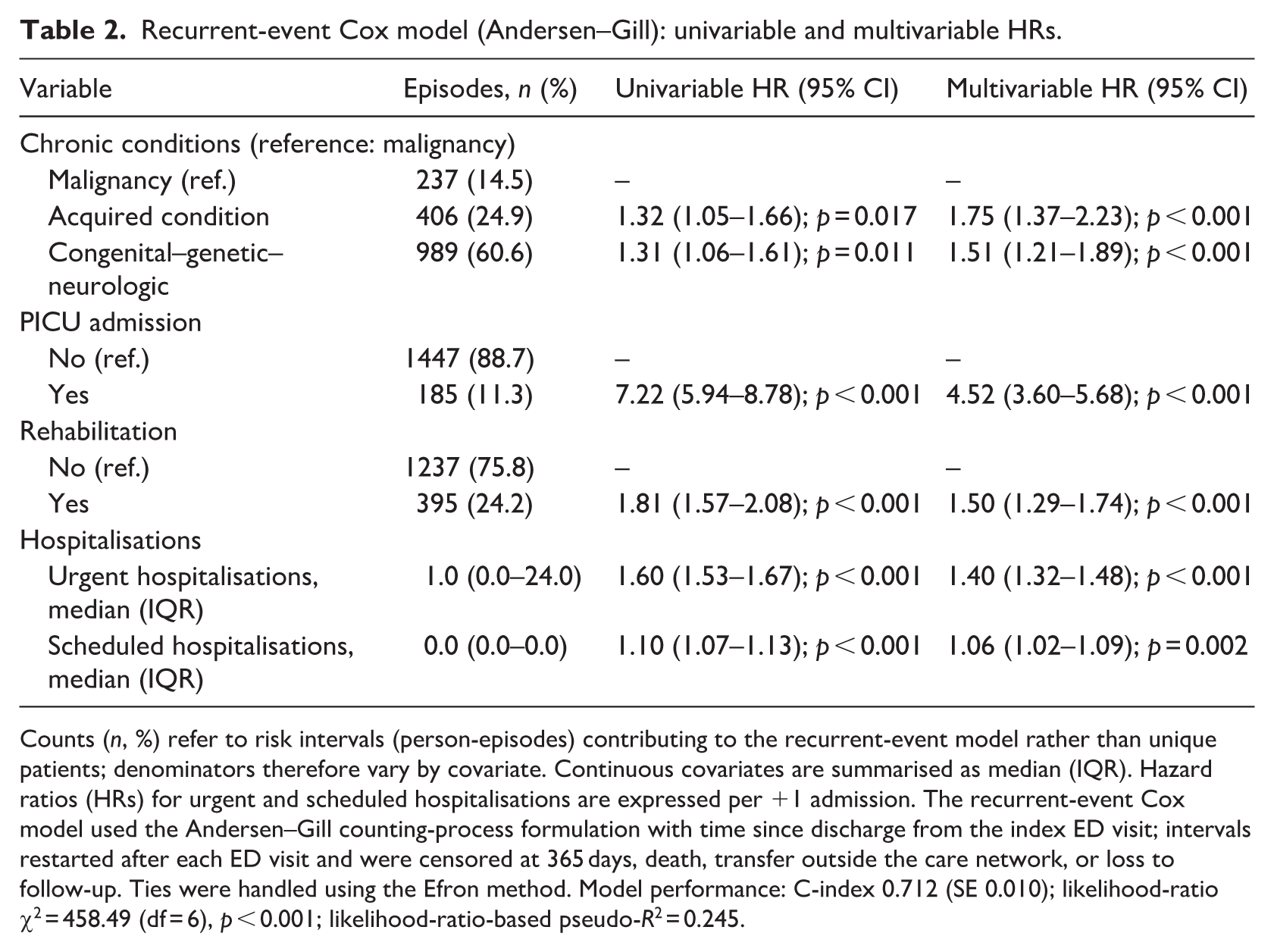
Counts (n, %) refer to risk intervals (person-episodes) contributing to the recurrent-event model rather than unique patients; denominators therefore vary by covariate. Continuous covariates are summarised as median (IQR). Hazard ratios (HRs) for urgent and scheduled hospitalisations are expressed per +1 admission. The recurrent-event Cox model used the Andersen–Gill counting-process formulation with time since discharge from the index ED visit; intervals restarted after each ED visit and were censored at 365 days, death, transfer outside the care network, or loss to follow-up. Ties were handled using the Efron method. Model performance: C-index 0.712 (SE 0.010); likelihood-ratio χ2 = 458.49 (df = 6), p < 0.001; likelihood-ratio-based pseudo-R2 = 0.245.
Discussion
In this single-centre cohort of children with CCCs, ED utilisation clustered into recognisable clinical profiles. Children in non-malignant macro-groups – particularly the congenital–genetic–neurologic group – and those with prior PICU admission, rehabilitation enrolment, or a higher hospitalisation burden had a consistently higher risk of ED revisits. These patterns highlight opportunities for individualised risk identification and follow-up pathways and were robust across prespecified sensitivity analyses.
These findings suggest that children with congenital/genetic or neurologic conditions may experience recurrent ED use partly because of multisystem complexity and extensive care needs, as described in earlier studies (Berry et al., 2017; Fortin et al., 2021). Rather than implying care failure, these patterns may reflect underlying clinical instability, high caregiving burden and the challenges of coordinating care across services. Consistent with this, parents of children with complex conditions have emphasised the importance of being recognised as experts in their child’s care and of maintaining continuity with clinicians (Bogetz et al., 2021).
Our socio-demographic analyses suggested that younger parents relied more on the ED. This finding aligns with studies indicating that younger parents may have fewer resources and less experience managing CCCs, which may increase reliance on emergency care (Hudson et al., 2014; Lozano and Houtrow, 2018). These results underscore the importance of supporting self-management skills in children with CCCs and their caregivers to improve the capacity to manage acute episodes and complications (Lozano and Houtrow, 2018).
Although we did not observe statistically significant differences by socio-economic indicators, prior studies have reported meaningful socio-economic gradients in frequent ED use among children with chronic conditions (Chang et al., 2022; Seguin et al., 2018). Lower socio-economic status may limit access to primary or specialty care, reduce health literacy and delay symptom recognition and home management, thereby increasing reliance on the ED. Families with fewer economic or social resources may also face barriers related to transportation, caregiving flexibility and access to prescribed treatments, which can further complicate timely management. These considerations highlight the importance of accounting for family context when designing future support strategies. Time since diagnosis was longer among children with fewer ED visits, which may indicate more stable disease trajectories and fewer acute episodes requiring urgent care. Prior studies have documented high ED utilisation among children with CCCs (Cianci et al., 2020; McKenzie et al., 2021). In our cohort, recurrent ED use appeared to cluster in children with greater clinical and functional complexity, reinforcing the need for careful follow-up and coordinated care.
The inverse association between child age and FSU may reflect the greater vulnerability of younger children to acute episodes, including higher rates of infectious illness (Vrijlandt et al., 2022). It may also reflect time-dependent factors such as improved clinical management, increasing caregiver experience and changing referral patterns as children age. Future studies should examine these temporal dynamics to better understand how utilisation trajectories evolve over childhood.
Higher ED utilisation and broader healthcare use among children with global FSU highlight the substantial demand that children with CCCs place on health systems (Passone et al., 2020) and the need for more effective management and follow-up strategies to reduce urgent care use and improve outcomes (Parker et al., 2020). The decline in annual ED visit frequency over time may reflect caregiver learning, improved coping strategies or evolving care plans. Early after diagnosis, prognostic uncertainty, limited information and inexperience managing symptoms may prompt caregivers to seek acute care more readily (Marshall et al., 2022). In addition, our follow-up overlapped with the COVID-19 pandemic (March 2020–December 2021), during which care pathways and resource allocation were reconfigured across the public health system. These system-level changes may have influenced ED utilisation in this cohort; we therefore present year-specific summaries (2015–2021) to contextualise trends (Barbiellini Amidei et al., 2021).
We also observed higher ED utilisation among children receiving PPC, those enrolled in rehabilitation and those who died during follow-up. Prior work indicates that children receiving PPC may attend the ED more frequently because of disease severity and acute exacerbations (Neugarten et al., 2024). These findings underscore the need for better integration and coordination of PPC and rehabilitation services to support families and potentially reduce avoidable ED visits while maintaining quality of life (Neugarten et al., 2024).
The multivariable model identified independent predictors of higher ED revisit risk in children with CCCs. Several factors were consistent with prior studies, including non-malignant clinical profiles (Peltz, et al., 2017), PICU admission (Cianci et al., 2020; O’Mahony et al., 2013) and higher hospitalisation burden (Coller et al., 2019). We additionally identified rehabilitation enrolment as a marker of functional and clinical complexity. This association may reflect multisystem morbidity and rehabilitation needs rather than a direct causal effect on ED use.
This study was conducted in a tertiary referral hospital within a tax-funded national health system in Southern Spain. Patterns of ED access, primary-care gatekeeping, referral thresholds and availability of paediatric subspecialty services (rehabilitation, PICU and PPC implemented locally in 2018) may differ across regions and health systems. Accordingly, although the direction of associations may be relevant to similar referral settings, effect sizes may vary with local care pathways, case mix, socio-demographic context and service capacity. The pandemic years (2020–2021) may also have influenced care-seeking. Multicentre validation across community and rural hospitals and in systems with different financing and resources is warranted to confirm generalisability and, if needed, recalibrate estimates and prospectively evaluate nurse-led follow-up and care-coordination strategies.
Strengths and limitations
This study has several strengths. It used a real-world longitudinal cohort of children with CCCs in a tertiary referral hospital within a tax-funded health system, included all eligible children regardless of ED utilisation, and examined clinically interpretable risk profiles using routinely recorded variables relevant to continuity and care coordination.
Information bias may arise from electronic medical record coding and from retrospective extraction by a single investigator using routine clinical documentation; some variables may therefore remain vulnerable to documentation errors or misclassification. In addition, encounters outside our network may not have been fully captured, despite the use of explicit denominators and complete-case analyses. Loss to follow-up and administrative 365-day censoring may introduce informative censoring, and death was not modelled as a competing risk. Although robust standard errors clustered by patient were used to account for within-child correlation of recurrent events, alternative recurrent-event approaches, such as frailty or joint models, may capture individual heterogeneity differently and should be explored in future studies.
Implications
These findings have implications for nursing education, practice, healthcare systems and policy and further research. For nursing education, they support training in continuity of care, discharge preparation, caregiver education, anticipatory guidance and coordination across services for children with CCCs. For nursing practice, routinely recorded indicators such as prior PICU admission, hospitalisation burden and rehabilitation enrolment may help identify children who could benefit from enhanced follow-up and care coordination after ED discharge. At the healthcare systems and policy level, the findings support strengthening integrated pathways across ED, inpatient, rehabilitation, palliative care, primary care and community services to improve continuity for high-risk children and families. Because this was an observational study, the results should be interpreted as informing risk stratification and service planning rather than as evidence of effectiveness. Further multicentre and prospective studies are needed to validate these findings and evaluate nurse-led continuity strategies.
Conclusions
We identified a clinically interpretable risk profile for higher ED utilisation among children with CCCs in this tertiary-care cohort, spanning clinical complexity, prior PICU admission, rehabilitation enrolment and hospitalisation burden. These findings may support risk stratification and inform nurse-led continuity and care coordination strategies. However, multicentre validation and prospective intervention studies are needed before specific models of care can be recommended.
Key points for policy, practice and research
Children with CCCs showed high ED utilisation during 2015–2021, with a median of eight visits per child.
Prior PICU admission and higher hospitalisation burden were strong markers of recurrent ED revisits.
Rehabilitation enrolment may help identify children with functional complexity who warrant closer follow-up and care coordination.
Routinely recorded factors may support nursing risk stratification and continuity planning across ED, inpatient and community settings.
The findings can inform the future design and evaluation of integrated ED–PICU–community continuity models for high-risk children and families.
Supplemental Material
sj-docx-1-jrn-10.1177_17449871261439013 – Supplemental material for Predictors of emergency department utilisation in children with complex chronic conditions: a retrospective longitudinal cohort study
Supplemental material, sj-docx-1-jrn-10.1177_17449871261439013 for Predictors of emergency department utilisation in children with complex chronic conditions: a retrospective longitudinal cohort study by Bibiana Pérez-Ardanaz, Laura Gutiérrez-Rodríguez, Celia Martí-García, Patricia Jiménez-Cuenca and José Miguel Morales-Asencio in Journal of Research in Nursing
Supplemental Material
sj-docx-2-jrn-10.1177_17449871261439013 – Supplemental material for Predictors of emergency department utilisation in children with complex chronic conditions: a retrospective longitudinal cohort study
Supplemental material, sj-docx-2-jrn-10.1177_17449871261439013 for Predictors of emergency department utilisation in children with complex chronic conditions: a retrospective longitudinal cohort study by Bibiana Pérez-Ardanaz, Laura Gutiérrez-Rodríguez, Celia Martí-García, Patricia Jiménez-Cuenca and José Miguel Morales-Asencio in Journal of Research in Nursing
Supplemental Material
sj-docx-3-jrn-10.1177_17449871261439013 – Supplemental material for Predictors of emergency department utilisation in children with complex chronic conditions: a retrospective longitudinal cohort study
Supplemental material, sj-docx-3-jrn-10.1177_17449871261439013 for Predictors of emergency department utilisation in children with complex chronic conditions: a retrospective longitudinal cohort study by Bibiana Pérez-Ardanaz, Laura Gutiérrez-Rodríguez, Celia Martí-García, Patricia Jiménez-Cuenca and José Miguel Morales-Asencio in Journal of Research in Nursing
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The institutional ethics committee determined that this study was exempt from new approval and confirmed that it was covered under the prior approval (No. 0655-N-16).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.